Preparedness and Responses Faced during the COVID-19 Pandemic in Belgium: An Observational Study and Using the National Open Data

Abstract
:1. Introduction
2. Materials and Methods
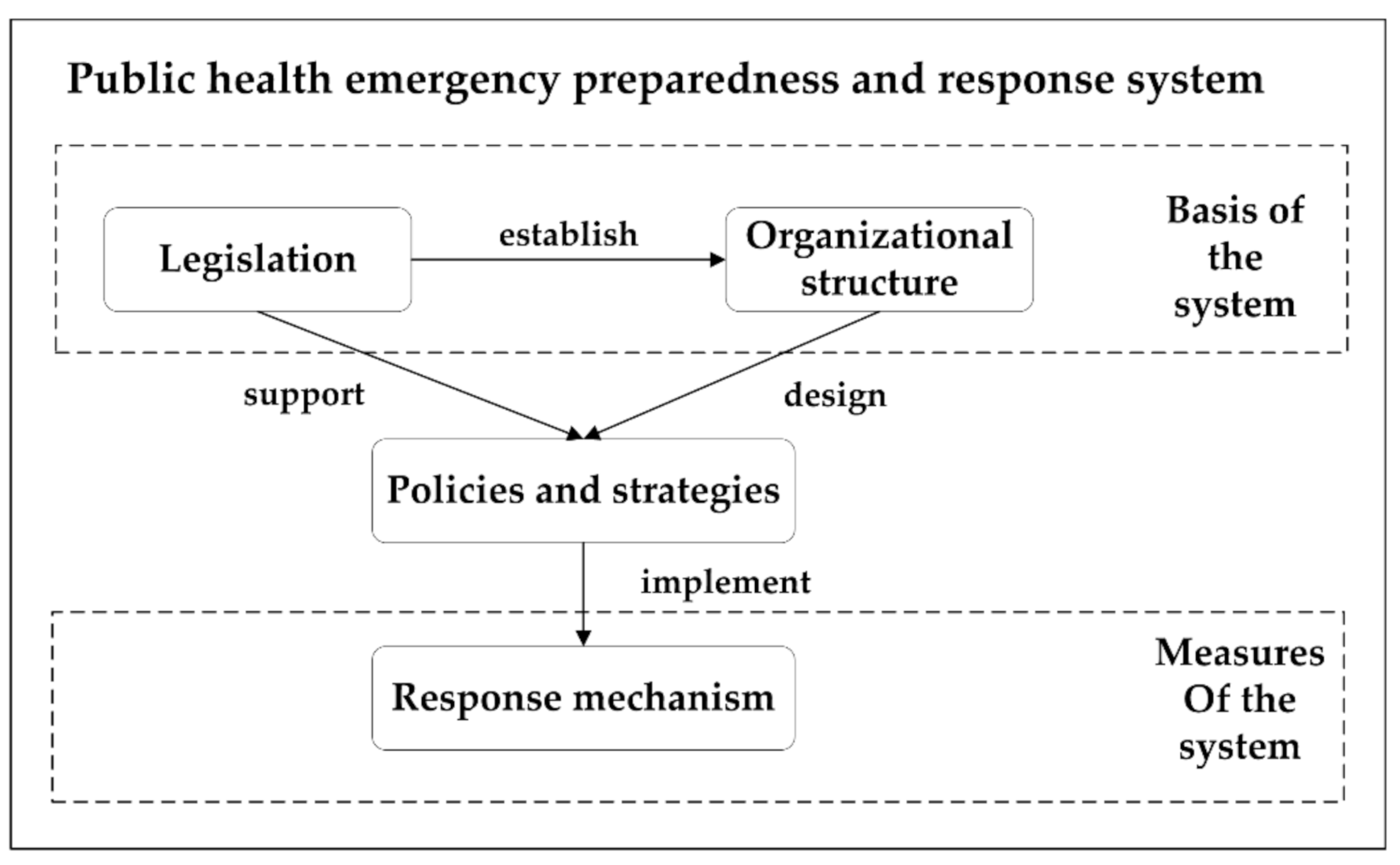
2.1. Analysis Framework
2.2. Data Resource
3. Result
3.1. Preparedness to the COVID-19 Epidemic
3.1.1. Legislation
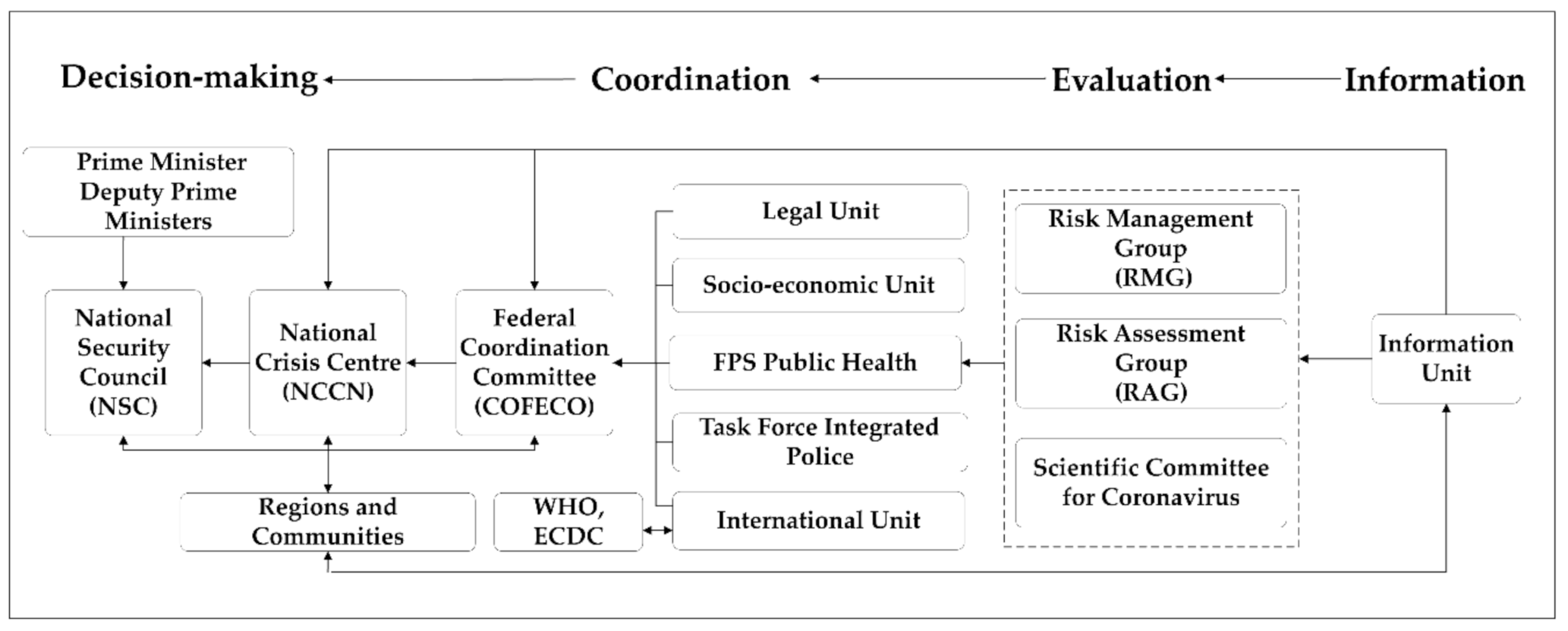
3.1.2. Organizational Structure
3.2. Response to the COVID-19 Epidemic
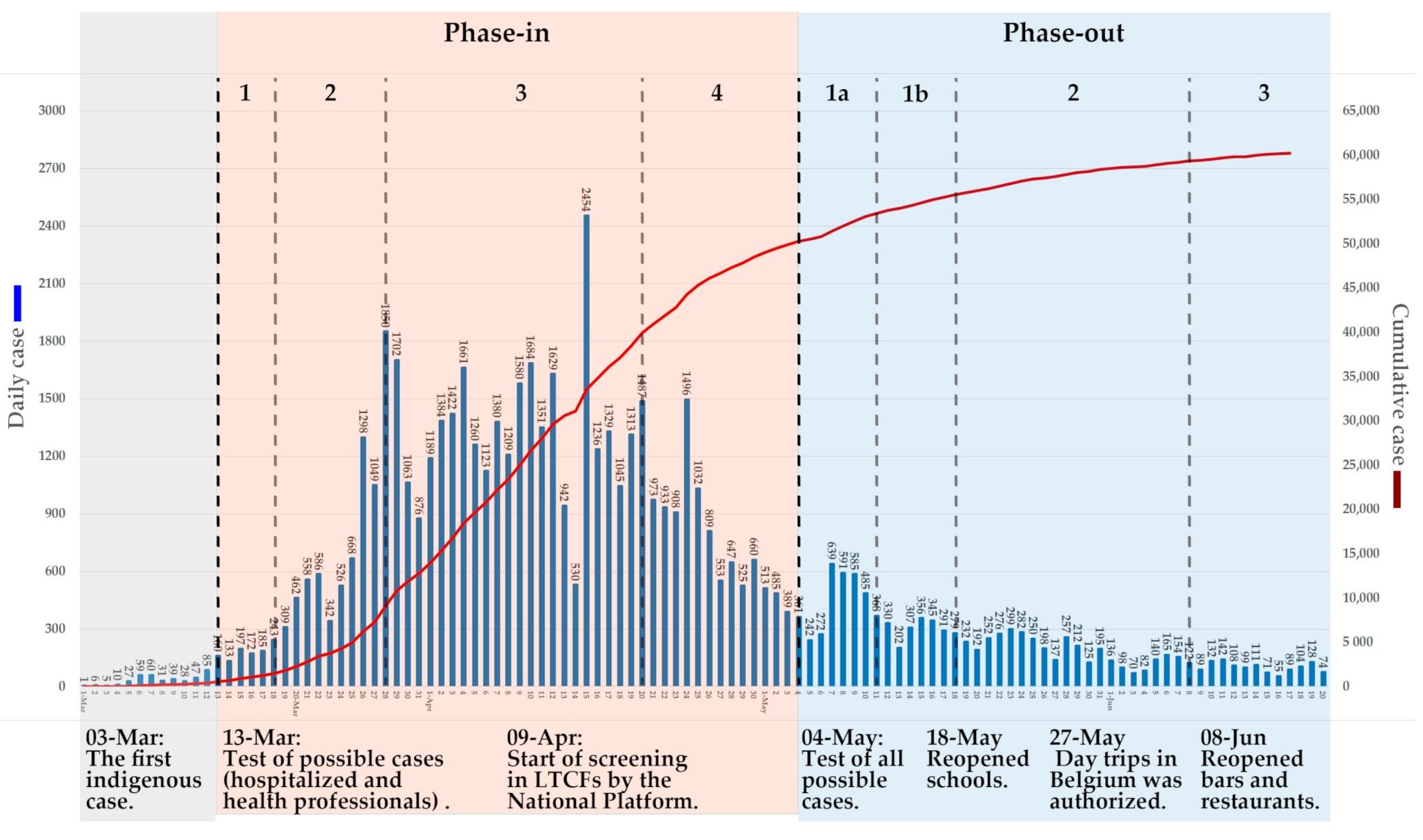
3.2.1. Timeline
Before the Lockdown
During the Lockdown
Lifting the Lockdown
3.2.2. Control Strategy
3.2.3. Key Priority Areas and Related Activities
Intersectoral Collaboration
Testing
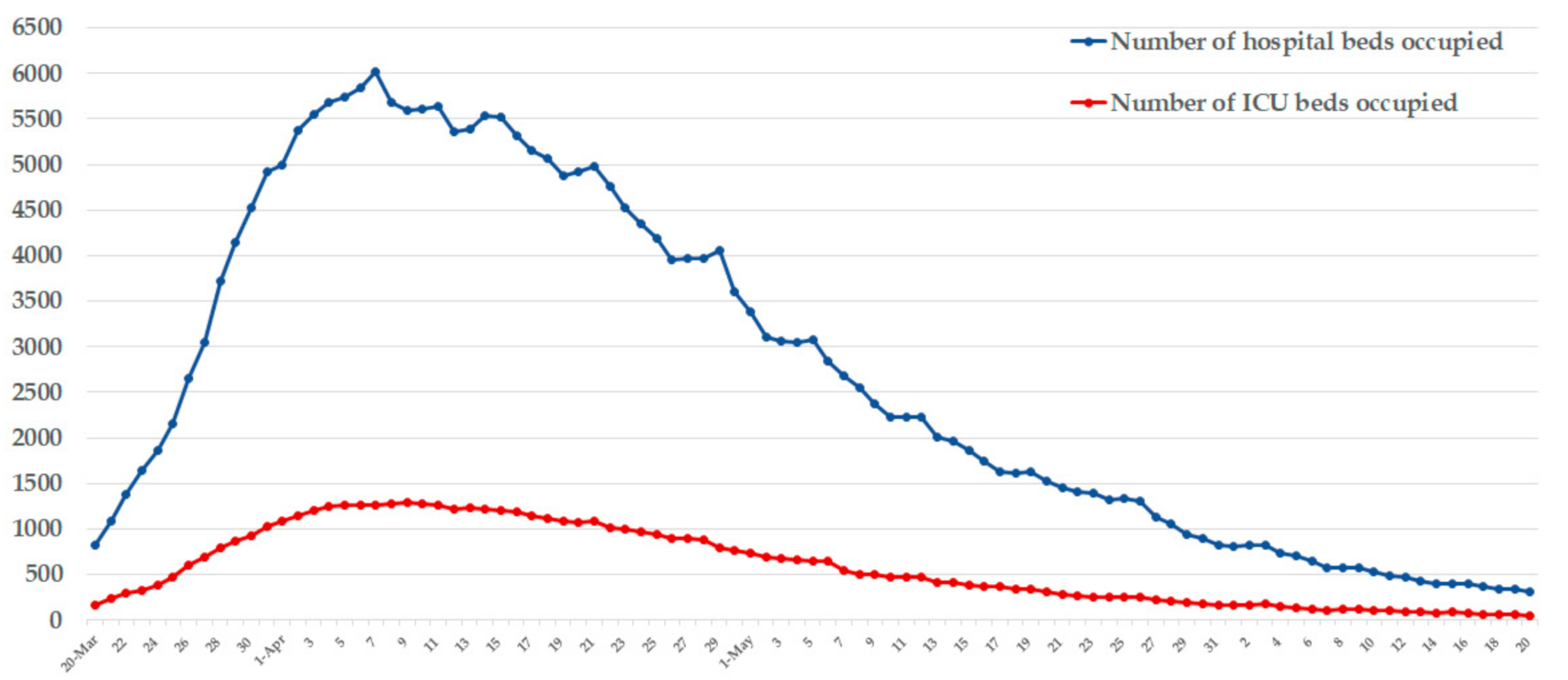
Emergency Resources
Risk Communication
The Vulnerable Populations
4. Discussion
4.1. Legislation and Organizational Structure
4.2. Response Mechanism
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| COVID-19 | Coronavirus Disease 2019 |
| WHO | World Health Organization |
| EDRM | Health Emergency and Disaster Risk Management |
| LTCF | Long term care facility |
| NSC | National Security Council |
| NCCN | National Crisis Centre |
| COFECO | Federal Coordination Committee |
| RAG | Risk Assessment Group |
| RMG | Risk Management Group |
| ICU | Intensive Care Unit |
| GEES | Group of Experts in charge of the Exit Strategy |
| ICMS | Incident & Crisis Management System |
References
- World Health Organization. Coronavirus Disease (COVID-19) Outbreak. Available online: https://www.who.int (accessed on 22 March 2020).
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 30 July 2020).
- Bressan, S.; Buonsenso, D.; Farrugia, R.; Parri, N.; Oostenbrink, R.; Titomanlio, L.; Roland, D.; Nijman, R.G.; Maconochie, I.; Da Dalt, L.; et al. Preparedness and response to Pediatric CoVID-19 in European Emergency Departments: A survey of the REPEM and PERUKI networks. Ann. Emerg. Med. 2020, 8, 1–13. [Google Scholar] [CrossRef]
- Eurostat. Population Density. Available online: https://ec.europa.eu/eurostat/tgm/table.do?tab=table&init=1&language=en&pcode=tps00003&plugin=1 (accessed on 30 July 2020).
- Federal Public Service (FPS) Health, Food Chain Safety and Environment. Coronavirus COVID-19. Available online: https://www.info-coronavirus.be/en/news/one-repatriated-belgian-has-tested-positive-for-the-novel-coronavirus/ (accessed on 2 February 2020).
- Federal Public Service (FPS) Health, Food Chain Safety and Environment. Coronavirus COVID-19. Available online: https://www.info-coronavirus.be/en/news/6-new-cases-of-covid-19-by-the-end-of-the-spring-holidays/ (accessed on 3 March 2020).
- Sciensano. COVID-19—BULLETIN EPIDEMIOLOGIQUE DU 29 MARS 2020. Available online: https://covid-19.sciensano.be/sites/default/files/Covid19/COVID-19_Daily%20report_20200329%20-%20NL.pdf (accessed on 29 March 2020).
- The Health Consumer Powerhouse Ltd. (HCP). Euro Health Consumer Index 2018. Available online: https://healthpowerhouse.com/media/EHCI-2018/EHCI-2018-report.pdf (accessed on 1 March 2020).
- ECDC. Public Health Emergency Preparedness for Cases of Viral Haemorrhagic Fever (Ebola) in Belgium: A Peer Review; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2015; ISBN 9789291936724. [Google Scholar]
- Federal Public Service (FPS) Health, Food Chain Safety and Environment. Coronavirus COVID-19. Available online: https://www.info-coronavirus.be/en/news/nsc-0306/ (accessed on 3 June 2020).
- Gagliano, A.; Villani, P.G.; Cò, F.M.; Paglia, S.; Bisagni, P.A.G.; Perotti, G.M.; Storti, E.; Lombardo, M. 2019-ncov’s epidemic in middle province of northern Italy: Impact, logistic & strategy in the first line hospital. Disaster Med. Public Health Prep. 2020, 6, 1–5. [Google Scholar]
- For a Healthy Belgium: Health and Healthcare Indicators. Care for the Elderly. Available online: https://www.healthybelgium.be/en/health-system-performance-assessment/specific-domains/care-for-the-elderly (accessed on 3 March 2020).
- RESIDENTIAL CARE FOR OLDER PERSONS IN BELGIUM: PROJECTIONS 2011–2025. Available online: https://kce.fgov.be/sites/default/files/atoms/files/KCE_167C_residential_care_in_Belgium_synthesis.pdf (accessed on 3 June 2020).
- Sciensano. COVID-19–WEKELIJKS EPIDEMIOLOGISCH BULLETIN VAN 26 JUNI 2020. Available online: https://covid-19.sciensano.be/sites/default/files/Covid19/COVID-19_Weekly%20report_20200626%20-%20NL_0.pdf (accessed on 26 June 2020).
- Centre de Crise. AR 18/04/1988—Création du CGCCR. Available online: https://centredecrise.be/fr/legislation/ar-18041988-creation-du-cgccr (accessed on 13 June 2020).
- Centre de Crise. AR 16/02/2006-Plans d’urgence et d’intervention. Available online: https://centredecrise.be/fr/legislation/ar-16022006-plans-durgence-et-dintervention (accessed on 13 June 2020).
- Centre de Crise. CIRC MIN NPU2 30/03/2009-Plan Général d’Urgence et d’Intervention du Gouverneur du Province. Available online: https://centredecrise.be/fr/legislation/circ-min-npu2-30032009-plan-general-durgence-et-dintervention-du-gouverneur-du-province (accessed on 13 June 2020).
- Centre de Crise. Arrêté Royal du 22 mai 2019 Relatif à la Planification d’urgence Locale. Available online: https://centredecrise.be/fr/legislation/arrete-royal-du-22-mai-2019-relatif-la-planification-durgence-locale (accessed on 13 June 2020).
- Centre de Crise. Législation. Available online: https://centredecrise.be/fr/legislation (accessed on 13 June 2020).
- Federal Public Service (FPS) Health, Food Chain Safety and Environment. Coronavirus COVID-19. Available online: https://www.info-coronavirus.be/en/what-is-the-government-doing-about-it/ (accessed on 26 June 2020).
- Federal Public Service (FPS) Health, Food Chain Safety and Environment. Coronavirus COVID-19. Available online: https://www.info-coronavirus.be/en/news/10-new-patients-contaminated-by-the-covid-19-virus-in-our-country-out-of-495-tests-performed-in-the-reference-laboratory/ (accessed on 4 March 2020).
- Federal Public Service (FPS) Health, Food Chain Safety and Environment. Coronavirus COVID-19. Available online: https://www.info-coronavirus.be/fr/news/premier-deces-lies-au-covid-19/ (accessed on 12 March 2020).
- Federal Public Service (FPS) Health, Food Chain Safety and Environment. Coronavirus COVID-19. Available online: https://www.info-coronavirus.be/en/news/phase-2-maintained-transition-to-the-federal-phase-and-additional-measures/ (accessed on 12 March 2020).
- Centre de Crise. AM 24/03/2020—COVID-19. Available online: https://centredecrise.be/fr/legislation/am-24032020-covid-19 (accessed on 24 March 2020).
- Centre de Crise. AM 03/04/2020—COVID-19. Available online: https://centredecrise.be/fr/legislation/am-03042020-covid-19 (accessed on 3 April 2020).
- Federal Public Service (FPS) Health, Food Chain Safety and Environment. Coronavirus COVID-19. Available online: https://www.info-coronavirus.be/fr/news/tests-maisons-de-repos/ (accessed on 10 April 2020).
- Centre de Crise. AM 17/04/2020-Prolongation des Mesures Contre la Propagation du Covid-19. Available online: https://centredecrise.be/fr/legislation/am-17042020-prolongation-des-mesures-contre-la-propagation-du-covid-19 (accessed on 17 April 2020).
- Policy Responses for Belgium. Transition Measures: Governance. Available online: https://www.covid19healthsystem.org/countries/belgium/livinghit.aspx?Section=5.%20Governance&Type=Chapter (accessed on 24 June 2020).
- Federal Public Service (FPS) Health, Food Chain Safety and Environment. Coronavirus COVID-19. Available online: https://www.info-coronavirus.be/fr/news/cns-06-05/ (accessed on 6 May 2020).
- Federal Public Service (FPS) Health, Food Chain Safety and Environment. Coronavirus COVID-19. Available online: https://www.info-coronavirus.be/fr/news/cns-13-05/ (accessed on 13 May 2020).
- Belgium.be. Measures taken by the National Security Council of 3 June 2020. Available online: https://www.belgium.be/en/corona (accessed on 3 June 2020).
- To, K.K.W.; Tsang, O.T.Y.; Leung, W.S.; Tam, A.R.; Wu, T.C.; Lung, D.C.; Yip, C.C.Y.; Cai, J.P.; Chan, J.M.C.; Chik, T.S.H.; et al. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: An observational cohort study. Lancet Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Sciensano. COVID-19—Epidemiologische Situatie. Available online: https://covid-19.sciensano.be/nl/covid-19-epidemiologische-situatie (accessed on 20 June 2020).
- Federal Public Service (FPS) Health, Food Chain Safety and Environment. Coronavirus COVID-19. Available online: https://www.info-coronavirus.be/en/news/end-of-quarantine-for-eight-belgian-nationals-who-returned-from-wuhan/ (accessed on 16 February 2020).
- Federal Public Service (FPS) Health, Food Chain Safety and Environment. Coronavirus COVID-19. Available online: https://www.info-coronavirus.be/en/testing/ (accessed on 12 March 2020).
- Sciensano. COVID-19–COVID-19–WEKELIJKS EPIDEMIOLOGISCH BULLETIN VAN 19 JUNI 2020. Available online: https://covid-19.sciensano.be/sites/default/files/Covid19/COVID-19_Weekly%20report_20200619%20-%20NL.pdf (accessed on 19 June 2020).
- THE BRUSSELS TIMES. Belgium destroyed millions of mouth masks ahead of outbreak. Available online: https://www.brusselstimes.com/all-news/belgium-all-news/102302/belgium-destroyed-and-did-not-replace-millions-of-mouth-masks/ (accessed on 24 March 2020).
- Federal Public Service (FPS) Health, Food Chain Safety and Environment. Meertalige informatie. Available online: https://www.info-coronavirus.be/en/translation/ (accessed on 19 June 2020).
- Federal Public Service (FPS) Health, Food Chain Safety and Environment. Meertalige informatie. Available online: https://www.info-coronavirus.be/en/news/set-an-example-stop-the-virus/ (accessed on 9 April 2020).
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, 1–12. [Google Scholar]
- Sciensano. COVID-19—BULLETIN EPIDEMIOLOGIQUE DU 30 JUIN 2020. Available online: https://covid-19.sciensano.be/sites/default/files/Covid19/COVID-19_Daily%20report_20200630%20-%20FR.pdf (accessed on 30 June 2020).
- Hoxha, A.; Wyndham-thomas, C.; Klamer, S.; Dubourg, D.; Vermeulen, M.; Hammami, N.; Cornelissen, L. Correspondence Asymptomatic Belgian long-term care. Lancet Infect. Dis. 2020, 3099, 30560. [Google Scholar]
- Policy Responses for Belgium. Paying for Services. Available online: https://www.covid19healthsystem.org/countries/belgium/livinghit.aspx?Section=4.1%20Health%20financing&Type=Section (accessed on 30 June 2020).
- InfoMigrants. Belgian Government Is Doing Nothing to Protect Migrants from Coronavirus, NGOs. Available online: https://www.infomigrants.net/en/post/23804/belgian-government-is-doing-nothing-to-protect-migrants-from-coronavirus-ngos (accessed on 1 April 2020).
- Federal Public Service (FPS) Health, Food Chain Safety and Environment. Coronavirus COVID-19. Available online: https://www.info-coronavirus.be/fr/news/avis-aux-voyageurs-de-retour-du-nord-italie-soyez-attentifs-a-votre-etat-de-sante-pendant-14-jours/ (accessed on 1 March 2020).
- Federal Public Service (FPS) Health, Food Chain Safety and Environment. Coronavirus COVID-19. Available online: https://www.info-coronavirus.be/fr/news/masques-qui-en-a-besoin/ (accessed on 26 March 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Date | Contents |
|---|---|
| 17 March 2020 | Royal decree concerning the prohibition of supply, putting into service and using rapid self-tests for the measurement or detection of antibodies of SARS-COV-2 virus. |
| 23 March 2020 24 March 2020 | Ministerial order carried out emergency measures to limit the spread of the COVID-19. |
| 3 April 2020 | Extension of measures to limit the spread of COVID-19 until April 19, 2020. |
| 6 April 2020 | Royal decree on the fight against non-compliance with emergency measures to limit the spread of the COVID-19 by the implementation of municipal administrative sanctions. |
| 17 April 2020 | Extension of measures to limit the spread of COVID-19. |
| 30 April 2020 | The ministerial decree of laying down emergency measures to limit the spread of the COVID-19. |
| 8 May 2020 | The ministerial decree updated. |
| 15 May 2020 | The ministerial decree updated. |
| 20 May 2020 | The ministerial decree updated. |
| 25 May 2020 | The ministerial decree updated. |
| 30 June 2020 | The ministerial decree updated. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, R.; Zhang, J.; Mao, Y.; Degomme, O.; Zhang, W.-H. Preparedness and Responses Faced during the COVID-19 Pandemic in Belgium: An Observational Study and Using the National Open Data. Int. J. Environ. Res. Public Health 2020, 17, 7985. https://doi.org/10.3390/ijerph17217985
He R, Zhang J, Mao Y, Degomme O, Zhang W-H. Preparedness and Responses Faced during the COVID-19 Pandemic in Belgium: An Observational Study and Using the National Open Data. International Journal of Environmental Research and Public Health. 2020; 17(21):7985. https://doi.org/10.3390/ijerph17217985
Chicago/Turabian StyleHe, Rongxin, Jun Zhang, Ying Mao, Olivier Degomme, and Wei-Hong Zhang. 2020. "Preparedness and Responses Faced during the COVID-19 Pandemic in Belgium: An Observational Study and Using the National Open Data" International Journal of Environmental Research and Public Health 17, no. 21: 7985. https://doi.org/10.3390/ijerph17217985
APA StyleHe, R., Zhang, J., Mao, Y., Degomme, O., & Zhang, W. -H. (2020). Preparedness and Responses Faced during the COVID-19 Pandemic in Belgium: An Observational Study and Using the National Open Data. International Journal of Environmental Research and Public Health, 17(21), 7985. https://doi.org/10.3390/ijerph17217985