Cellular Phone Use and Risk of Tumors: Systematic Review and Meta-Analysis

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Selection Criteria
2.3. Selection of Relevant Studies
2.4. Assessment of Methodological Quality
2.5. Main and Subgroup Analyses
2.6. Statistical Analysis
3. Results
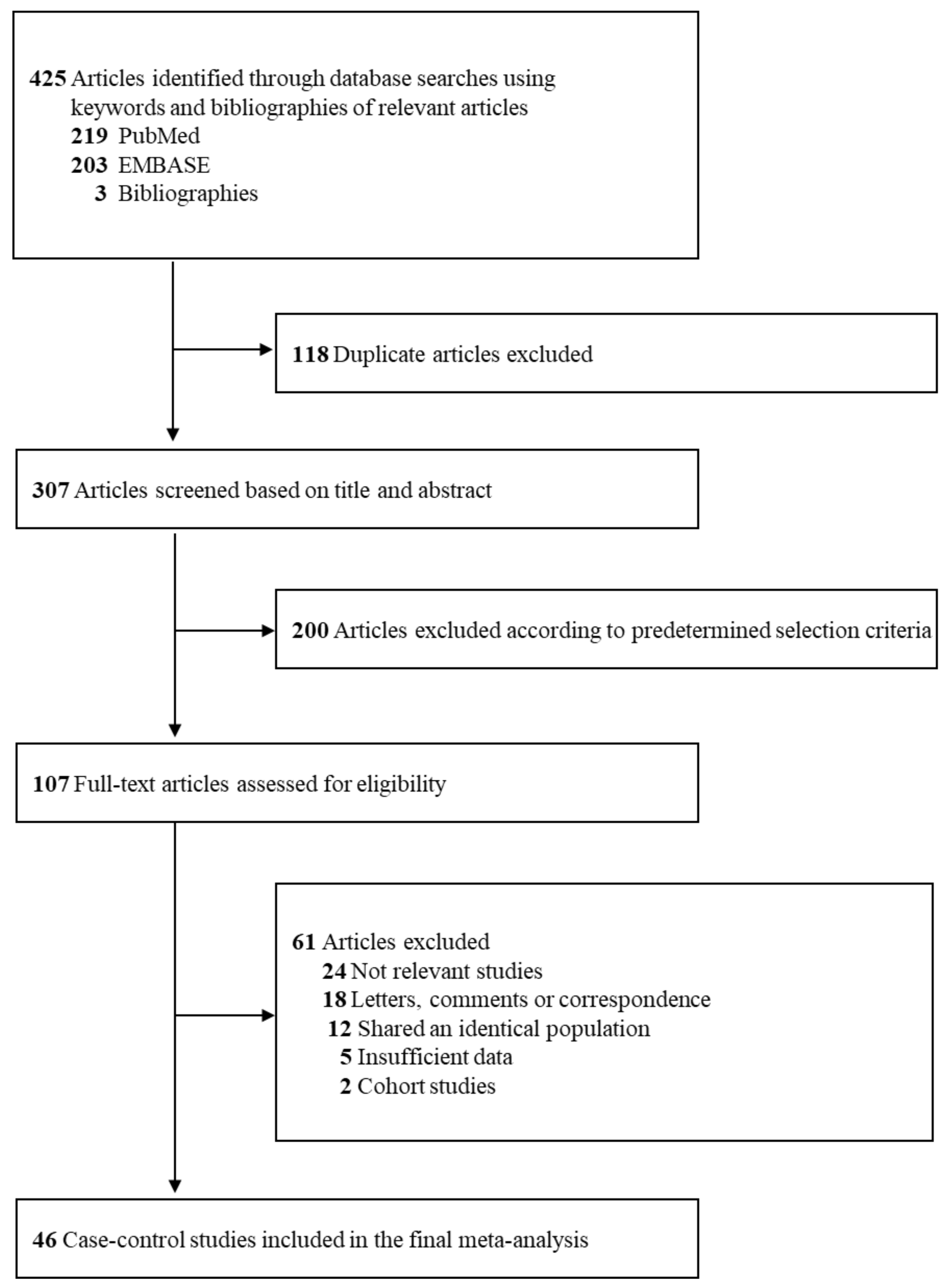
3.1. Study Selection
3.2. General Characteristics of Studies and Participants
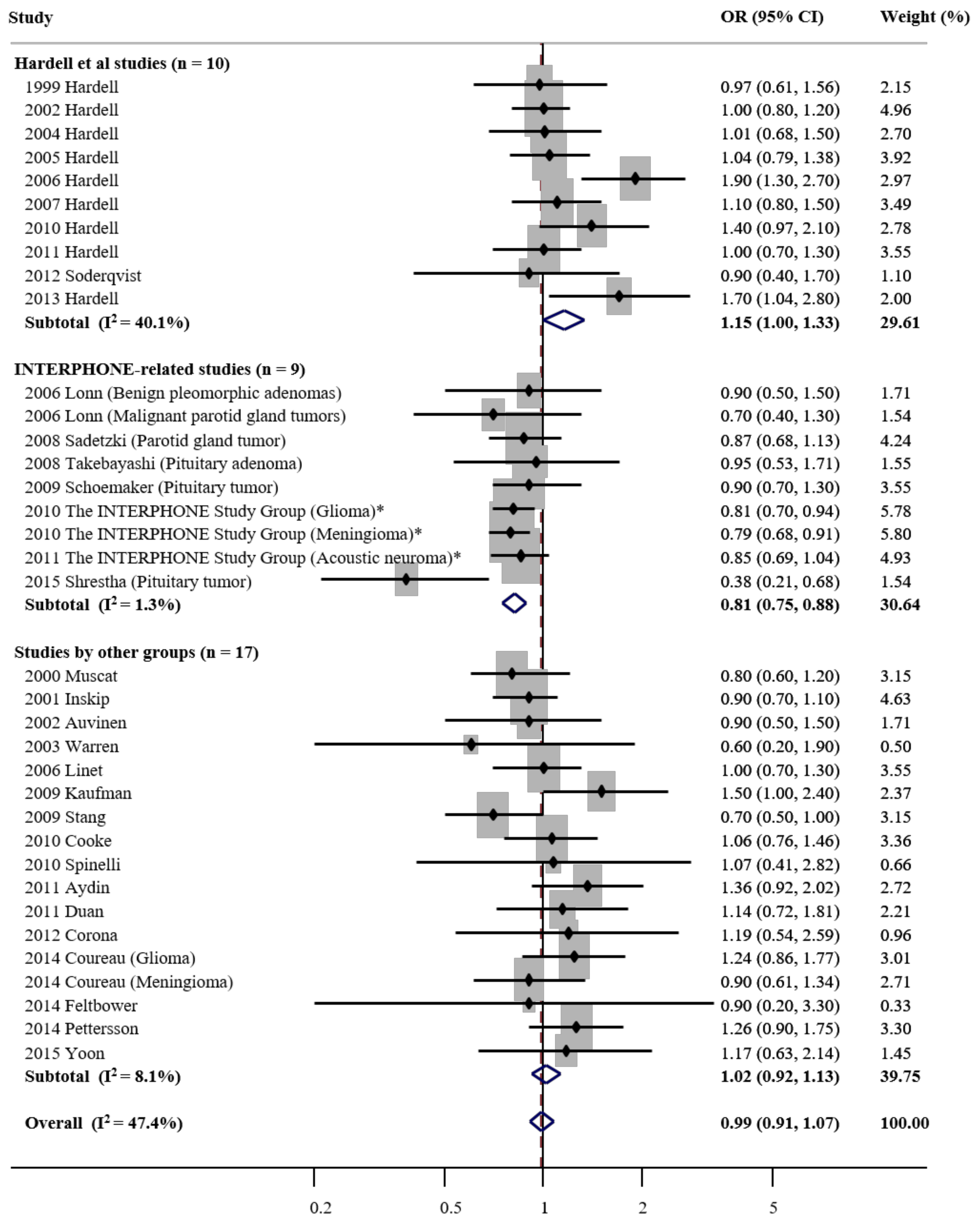
3.3. Overall Use of Cellular Phone and Risk of Tumors
3.4. Use of Cellular Phones and Risk of Tumors in Subgroup Meta-analysis By Various Factors
3.5. Exposure–Response Relationship Between Use of Cellular Phones and Risk of Tumors
3.6. Use of Cellular Phones and Risk of Tumors in Subgroup Meta-analysis By Type of Tumor
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- International Telecommunication Union. ICT Statistics. Available online: https://www.itu.int/en/ITU-D/Statistics/Pages/stat/default.aspx (accessed on 22 January 2020).
- Hardell, L.; Sage, C. Biological effects from electromagnetic field exposure and public exposure standards. Biomed. Pharmacother. 2008, 62, 104–109. [Google Scholar] [CrossRef]
- Kan, P.; Simonsen, S.E.; Lyon, J.L.; Kestle, J.R. Cellular phone use and brain tumor: A meta-analysis. J. Neurooncol. 2008, 86, 71–78. [Google Scholar] [CrossRef]
- Hardell, L.; Carlberg, M.; Soderqvist, F.; Hansson Mild, K. Meta-analysis of long-term mobile phone use and the association with brain tumours. Int. J. Oncol. 2008, 32, 1097–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myung, S.K.; Ju, W.; McDonnell, D.D.; Lee, Y.J.; Kazinets, G.; Cheng, C.-T.; Moskowitz, J.M. Mobile phone use and risk of tumors: A meta-analysis. J. Clin. Oncol. 2009, 27, 5565–5572. [Google Scholar] [CrossRef] [PubMed]
- Khurana, V.G.; Teo, C.; Kundi, M.; Hardell, L.; Carlberg, M. Cell phones and brain tumors: A review including the long-term epidemiologic data. Surg. Neurol. 2009, 72, 205–214. [Google Scholar] [CrossRef]
- The World Health Organization/International Agency for Research on Cancer. PRESS RELEASE N0 208. IARC Classifies Radiofrequency Electromagnetic Fields as Possibly Carcinogenic to Humans; The World Health Organization/International Agency for Research on Cancer: Lyon, France, 31 May 2011.
- IARC Monographs Priorities Group. Advisory Group recommendations on priorities for the IARC Monographs. Lancet Oncol. 2019, 20, 763–764. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/nosgen.pdf (accessed on 22 January 2020).
- National Heart, Lung, and Blood Institute, National Institutes of Health, U.S. Department of Health & Human Services. Quality Assessment Tool of Case-Control Studies. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 22 January 2020).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Hardell, L.; Näsman, A.; Påhlson, A.; Hallquist, A.; Hansson Mild, K. Use of cellular telephones and the risk for brain tumours: A case-control study. Int. J. Oncol. 1999, 15, 113–116. [Google Scholar] [CrossRef]
- Hardell, L.; Hallquist, A.; Hansson Mild, K.; Carlberg, M.; Påhlson, A.; Lilja, A. Cellular and cordless telephones and the risk for brain tumours. Eur. J. Cancer Prev. 2002, 11, 377–386. [Google Scholar] [CrossRef]
- Hardell, L.; Hansson Mild, K.; Sandström, M.; Carlberg, M.; Hallquist, A.; Påhlson, A. Vestibular schwannoma, tinnitus and cellular telephones. Neuroepidemiology 2003, 22, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Hardell, L.; Hallquist, A.; Hansson Mild, K.; Carlberg, M.; Gertzén, H.; Schildt, E.-B.; Dahlqvist, A. No association between the use of cellular or cordless telephones and salivary gland tumours. Occup. Environ. Med. 2004, 61, 675–679. [Google Scholar] [CrossRef] [Green Version]
- Hardell, L.; Eriksson, M.; Carlberg, M.; Sandström, C.; Mild, K.H. Use of cellular or cordless telephones and the risk for non-Hodgkin’s lymphoma. Int. Arch. Occup. Environ. Health 2005, 78, 625–632. [Google Scholar] [CrossRef]
- Hardell, L.; Carlberg, M.; Hansson Mild, K. Case-control study of the association between the use of cellular and cordless telephones and malignant brain tumors diagnosed during 2000–2003. Environ. Res. 2006, 100, 232–241. [Google Scholar] [CrossRef]
- Hardell, L.; Carlberg, M.; Ohlson, C.G.; Westberg, H.; Eriksson, M.; Hansson Mild, K. Use of cellular and cordless telephones and risk of testicular cancer. Int. J. Androl. 2007, 30, 115–122. [Google Scholar] [CrossRef]
- Hardell, L.; Carlberg, M.; Hansson Mild, K. Mobile phone use and the risk for malignant brain tumors: A case-control study on deceased cases and controls. Neuroepidemiology 2010, 35, 109–114. [Google Scholar] [CrossRef]
- Hardell, L.; Carlberg, M.; Hansson Mild, K.; Eriksson, M. Case-control study on the use of mobile and cordless phones and the risk for malignant melanoma in the head and neck region. Pathophysiology 2011, 18, 325–333. [Google Scholar] [CrossRef]
- Söderqvist, F.; Carlberg, M.; Hardell, L. Use of wireless phones and the risk of salivary gland tumours: A case-control study. Eur. J. Cancer Prev. 2012, 21, 576–579. [Google Scholar] [CrossRef]
- Hardell, L.; Carlberg, M.; Söderqvist, F.; Hansson Mild, K. Case-control study of the association between malignant brain tumours diagnosed between 2007 and 2009 and mobile and cordless phone use. Int. J. Oncol. 2013, 43, 1833–1845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christensen, H.C. Cellular Telephone Use and Risk of Acoustic Neuroma. Am. J. Epidemiol. 2004, 159, 277–283. [Google Scholar] [CrossRef]
- Lönn, S.; Ahlbom, A.; Hall, P.; Feychting, M. Mobile Phone Use and the Risk of Acoustic Neuroma. Epidemiology 2004, 15, 653–659. [Google Scholar] [CrossRef] [PubMed]
- Christensen, H.C.; Schuz, J.; Kosteljanetz, M.; Skovgaard Poulsen, H.; Boice, J.D., Jr.; McLaughlin, J.K.; Johansen, C. Cellular telephones and risk for brain tumors: A population-based, incident case-control study. Neurology 2005, 64, 1189–1195. [Google Scholar] [CrossRef] [PubMed]
- Lönn, S.; Ahlbom, A.; Hall, P.; Feychting, M.; Swedish Interphone Study Group. Long-term mobile phone use and brain tumor risk. Am. J. Epidemiol. 2005, 161, 526–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoemaker, M.J.; Swerdlow, A.J.; Ahlbom, A.; Auvinen, A.; Blaasaas, K.G.; Cardis, E.; Christensen, H.C.; Feychting, M.; Hepworth, S.J.; Johansen, C.; et al. Mobile phone use and risk of acoustic neuroma: Results of the Interphone case-control study in five North European countries. Br. J. Cancer 2005, 93, 842–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hepworth, S.J.; Schoemaker, M.J.; Muir, K.R.; Swerdlow, A.J.; van Tongeren, M.J.; McKinney, P.A. Mobile phone use and risk of glioma in adults: Case-control study. BMJ 2006, 332, 883–887. [Google Scholar] [CrossRef] [Green Version]
- Schuz, J.; Bohler, E.; Berg, G.; Schlehofer, B.; Hettinger, I.; Schlaefer, K.; Wahrendorf, J.; Kunna-Grass, K.; Blettner, M. Cellular phones, cordless phones, and the risks of glioma and meningioma (Interphone Study Group, Germany). Am. J. Epidemiol. 2006, 163, 512–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lönn, S.; Ahlbom, A.; Christensen, H.C.; Johansen, C.; Schüz, J.; Edström, S.; Henriksson, G.; Lundgren, G.; Wennerberg, J.; Feychting, M. Mobile phone use and risk of parotid gland tumor. Am. J. Epidemiol. 2006, 164, 637–643. [Google Scholar] [CrossRef]
- Takebayashi, T.; Akiba, S.; Kikuchi, Y.; Taki, M.; Wake, K.; Watanabe, S.; Yamaguchi, N. Mobile phone use and acoustic neuroma risk in Japan. Occup. Environ. Med. 2006, 63, 802–807. [Google Scholar] [CrossRef] [Green Version]
- Klaeboe, L.; Blaasaas, K.G.; Tynes, T. Use of mobile phones in Norway and risk of intracranial tumours. Eur. J. Cancer Prev. 2007, 16, 158–164. [Google Scholar] [CrossRef] [Green Version]
- Lahkola, A.; Auvinen, A.; Raitanen, J.; Schoemaker, M.J.; Christensen, H.C.; Feychting, M.; Johansen, C.; Klaeboe, L.; Lönn, S.; Swerdlow, A.J.; et al. Mobile phone use and risk of glioma in 5 North European countries. Int. J. Cancer 2007, 120, 1769–1775. [Google Scholar] [CrossRef]
- Schlehofer, B.; Schlaefer, K.; Blettner, M.; Berg, G.; Böhler, E.; Hettinger, I.; Kunna-Grass, K.; Wahrendorf, J.; Schüz, J.; Interphone Study Group. Environmental risk factors for sporadic acoustic neuroma (Interphone Study Group, Germany). Eur. J. Cancer 2007, 43, 1741–1747. [Google Scholar] [CrossRef] [PubMed]
- Lahkola, A.; Salminen, T.; Raitanen, J.; Heinävaara, S.; Schoemaker, M.J.; Collatz Christensen, H.; Feychting, M.; Johansen, C.; Klaeboe, L.; Lönn, S.; et al. Meningioma and mobile phone use--a collaborative case-control study in five North European countries. Int. J. Epidemiol. 2008, 37, 1304–1313. [Google Scholar] [CrossRef] [Green Version]
- Sadetzki, S.; Chetrit, A.; Jarus-Hakak, A.; Cardis, E.; Deutch, Y.; Duvdevani, S.; Zultan, A.; Novikov, I.; Freedman, L.; Wolf, M. Cellular phone use and risk of benign and malignant parotid gland tumors—A nationwide case-control study. Am. J. Epidemiol. 2008, 167, 457–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takebayashi, T.; Varsier, N.; Kikuchi, Y.; Wake, K.; Taki, M.; Watanabe, S.; Akiba, S.; Yamaguchi, N. Mobile phone use, exposure to radiofrequency electromagnetic field, and brain tumour: A case-control study. Br. J. Cancer 2008, 98, 652–659. [Google Scholar] [CrossRef] [Green Version]
- Schoemaker, M.J.; Swerdlow, A.J. Risk of pituitary tumors in cellular phone users: A case-control study. Epidemiology 2009, 20, 348–354. [Google Scholar] [CrossRef] [PubMed]
- The INTERPHONE Study Group. Brain tumour risk in relation to mobile telephone use: Results of the INTERPHONE international case-control study. Int. J. Epidemiol. 2010, 39, 675–694. [Google Scholar] [CrossRef] [Green Version]
- The INTERPHONE Study Group. Acoustic neuroma risk in relation to mobile telephone use: Results of the INTERPHONE international case-control study. Cancer Epidemiol. 2011, 35, 453–464. [Google Scholar] [CrossRef]
- Shrestha, M.; Raitanen, J.; Salminen, T.; Lahkola, A.; Auvinen, A. Pituitary tumor risk in relation to mobile phone use: A case-control study. Acta Oncol. 2015, 54, 1159–1165. [Google Scholar] [CrossRef] [Green Version]
- Muscat, J.E.; Malkin, M.G.; Thompson, S.; Shore, R.E.; Stellman, S.D.; McRee, D.; Neugut, A.I.; Wynder, E.L. Handheld cellular telephone use and risk of brain cancer. JAMA 2000, 284, 3001–3007. [Google Scholar] [CrossRef]
- Inskip, P.D.; Tarone, R.E.; Hatch, E.E.; Wilcosky, T.C.; Shapiro, W.R.; Selker, R.G.; Fine, H.A.; Black, P.M.; Loeffler, J.S.; Linet, M.S. Cellular-telephone use and brain tumors. N. Engl. J. Med. 2001, 344, 79–86. [Google Scholar] [CrossRef]
- Auvinen, A.; Hietanen, M.; Luukkonen, R.; Koskela, R.S. Brain tumors and salivary gland cancers among cellular telephone users. Epidemiology 2002, 13, 356–359. [Google Scholar] [CrossRef]
- Warren, H.G.; Prevatt, A.A.; Daly, K.A.; Antonelli, P.J. Cellular telephone use and risk of intratemporal facial nerve tumor. Laryngoscope 2003, 113, 663–667. [Google Scholar] [CrossRef]
- Linet, M.S.; Taggart, T.; Severson, R.K.; Cerhan, J.R.; Cozen, W.; Hartge, P.; Colt, J. Cellular telephones and non-Hodgkin lymphoma. Int. J. Cancer 2006, 119, 2382–2388. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, D.W.; Anderson, T.E.; Issaragrisil, S. Risk factors for leukemia in Thailand. Ann. Hematol. 2009, 88, 1079–1088. [Google Scholar] [CrossRef]
- Stang, A.; Schmidt-Pokrzywniak, A.; Lash, T.L.; Lommatzsch, P.K.; Taubert, G.; Bornfeld, N.; Jöckel, K.-H. Mobile phone use and risk of uveal melanoma: Results of the risk factors for uveal melanoma case-control study. J. Natl. Cancer Inst. 2009, 101, 120–123. [Google Scholar] [CrossRef] [Green Version]
- Cooke, R.; Laing, S.; Swerdlow, A.J. A case-control study of risk of leukaemia in relation to mobile phone use. Br. J. Cancer 2010, 103, 1729–1735. [Google Scholar] [CrossRef]
- Spinelli, V.; Chinot, O.; Cabaniols, C.; Giorgi, R.; Alla, P.; Lehucher-Michel, M.P. Occupational and environmental risk factors for brain cancer: A pilot case-control study in France. Presse Med. 2010, 39, e35–e44. [Google Scholar] [CrossRef]
- Aydin, D.; Feychting, M.; Schuz, J.; Tynes, T.; Andersen, T.V.; Samso Schmidt, L.; Poulsen, A.H.; Johansen, C.; Prochazka, M.; Lannering, B.; et al. Mobile phone use and brain tumors in children and adolescents: A multicenter case-control study. J. Natl. Cancer Inst. 2011, 103, 1264–1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duan, Y.; Zhang, H.Z.; Bu, R.F. Correlation between cellular phone use and epithelial parotid gland malignancies. Int. J. Oral Maxillofac. Surg. 2011, 40, 966–972. [Google Scholar] [CrossRef]
- Corona, A.P.; Ferrite, S.; Lopes Mda, S.; Rego, M.A. Risk factors associated with vestibular nerve schwannomas. Otol. Neurotol. 2012, 33, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Coureau, G.; Bouvier, G.; Lebailly, P.; Fabbro-Peray, P.; Gruber, A.; Leffondre, K.; Guillamo, J.-S.; Loiseau, H.; Mathoulin-Pélissier, S.; Salamon, R.; et al. Mobile phone use and brain tumours in the CERENAT case-control study. Occup. Environ. Med. 2014, 71, 514–522. [Google Scholar] [CrossRef] [Green Version]
- Feltbower, R.G.; Fleming, S.J.; Picton, S.V.; Alston, R.D.; Morgan, D.; Achilles, J.; McKinney, P.A.; Birch, J.M. UK case control study of brain tumours in children, teenagers and young adults: A pilot study. BMC Res. Notes 2014, 7, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pettersson, D.; Mathiesen, T.; Prochazka, M.; Bergenheim, T.; Florentzson, R.; Harder, H.; Nyberg, G.; Siesjö, P.; Feychting, M. Long-term mobile phone use and acoustic neuroma risk. Epidemiology 2014, 25, 233–241. [Google Scholar] [CrossRef]
- Yoon, S.; Choi, J.W.; Lee, E.; An, H.; Choi, H.D.; Kim, N. Mobile phone use and risk of glioma: A case-control study in Korea for 2002–2007. Environ. Health Toxicol. 2015, 30, e2015015. [Google Scholar] [CrossRef] [Green Version]
- Luo, J.; Deziel, N.C.; Huang, H.; Chen, Y.; Ni, X.; Ma, S.; Udelsman, R.; Zhang, Y. Cell phone use and risk of thyroid cancer: A population-based case-control study in Connecticut. Ann. Epidemiol. 2019, 29, 39–45. [Google Scholar] [CrossRef]
- Karinen, A.; Heinavaara, S.; Nylund, R.; Leszczynski, D. Mobile phone radiation might alter protein expression in human skin. BMC Genom. 2008, 9, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Guo, X. Meta-analysis of association between mobile phone use and glioma risk. J. Cancer Res. Ther. 2016, 12 (Suppl. S4), C298–C300. [Google Scholar] [CrossRef] [PubMed]
- Bortkiewicz, A.; Gadzicka, E.; Szymczak, W. Mobile phone use and risk for intracranial tumors and salivary gland tumors—A meta-analysis. Int. J. Occup. Med. Environ. Health 2017, 30, 27–43. [Google Scholar] [CrossRef] [Green Version]
- De Siqueira, E.C.; de Souza, F.T.A.; Gomez, R.S.; Gomes, C.C.; de Souza, R.P. Does cell phone use increase the chances of parotid gland tumor development? A systematic review and meta-analysis. J. Oral Pathol. Med. 2017, 46, 480–483. [Google Scholar] [CrossRef]
- Yang, M.; Guo, W.; Yang, C.; Tang, J.; Huang, Q.; Feng, S.; Jiang, A.; Xu, X.; Jiang, G. Mobile phone use and glioma risk: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0175136. [Google Scholar] [CrossRef]
- Wang, P.; Hou, C.; Li, Y.; Zhou, D. Wireless Phone Use and Risk of Adult Glioma: Evidence from a Meta-Analysis. World Neurosurg. 2018, 115, e629–e636. [Google Scholar] [CrossRef] [PubMed]
- Prasad, M.; Kathuria, P.; Nair, P.; Kumar, A.; Prasad, K. Mobile phone use and risk of brain tumours: A systematic review of association between study quality, source of funding, and research outcomes. Neurol. Sci. 2017, 38, 797–810. [Google Scholar] [CrossRef] [PubMed]
- Hardell, L.; Carlberg, M. Mobile phone and cordless phone use and the risk for glioma—Analysisof pooled case-control studies in Sweden, 1997–2003 and 2007–2009. Pathophysiology 2015, 22, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Pandeya, N.; Williams, G.M.; Green, A.C.; Webb, P.M.; Whiteman, D.C. Do low control response rates always affect the findings? Assessments of smoking and obesity in two Australian case-control studies of cancer. Aust. N. Z. Public Health 2009, 33, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Morgan, L.L. Re: “Cellular phones, cordless phones, and the risks of glioma and meningioma (Interphone Study Group, Germany)”. Am. J. Epidemiol. 2006, 164, 294–295, author reply 295. [Google Scholar] [CrossRef] [Green Version]
- Hardell, L.; Carlberg, M. Health risks from radiofrequency radiation, including 5G, should be assessed by experts with no conflicts of interest. Oncol. Lett. 2020, 20, 15. [Google Scholar]
- Frei, P.; Poulsen, A.H.; Johansen, C.; Olsen, J.H.; Steding-Jessen, M.; Schüz, J. Use of mobile phones and risk of brain tumours: Update of Danish cohort study. BMJ 2011, 343, d6387. [Google Scholar] [CrossRef] [Green Version]
- Benson, V.S.; Pirie, K.; Schuz, J.; Reeves, G.K.; Beral, V.; Green, J.; Million Women Study Collaboratiors. Mobile phone use and risk of brain neoplasms and other cancers: Prospective study. Int. J. Epidemiol. 2013, 42, 792–802. [Google Scholar] [CrossRef] [Green Version]
- Toledano, M.B.; Auvinen, A.; Tettamanti, G.; Cao, Y.; Feychting, M.; Ahlbom, A.; Fremling, K.; Heinävaara, S.; Kojo, K.; Knowles, G.; et al. An international prospective cohort study of mobile phone users and health (COSMOS): Factors affecting validity of self-reported mobile phone use. Int. J. Hyg. Environ. Health 2018, 221, 1–8. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study a | Country | Study Design b | Study Period | Type of Tumor (Age Range, Years) | Type of Cellular Phone Used in Analysis | Exposure | OR (95% CI) | Adjusted Variables | No. (Response Rate) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Cases | Controls | |||||||||
| Hardell et al. studies (n = 11) | ||||||||||
| Hardell et al., 1999 [13] | Sweden | PCC | 1994–1996 | Brain tumor (20–80) | Digital | Use vs. no use (latency period >1 year) | 0.97 (0.61 to 1.56) | Age, sex, and study region (matched) | 209 (90%) | 425 (91%) |
| Hardell et al., 2002 [14] | Sweden | PCC | 1997–2000 | Brain tumor (20–80) | Digital | Use vs. no use (latency period >1 year) | 1.0 (0.8 to 1.2) | Use of different types of phones | 1429 (88%) | 1470 (91%) |
| Hardell et al., 2003 [15] | Sweden | PCC | 1997–2000 | Vestibular schwannoma (All ages) | Digital | Use vs. no use (latency period >1 year) | 1.21 (0.66 to 2.22) | Sex, age, and geographical area | 159 (89%) | 159 (89%) |
| Hardell et al., 2004 [16] | Sweden | PCC | 1994–2000 | Salivary gland tumors (21–80) | Digital | Use vs. no use (latency period >1 year) | 1.01 (0.68 to 1.50) | Age and sex | 267 (91%) | 1053 (90%) |
| Hardell et al., 2005 [17] | Sweden | PCC | 1999–2002 | Non-Hodgkin’s lymphoma (18–74) | Digital | Use vs. no use (latency period >1 year) | 1.04 (0.79 to 1.38) | Age, sex, and year of diagnosis (cases) or enrollment (controls) | 910 (91%) | 1016 (92%) |
| Hardell et al., 2006 [18] | Sweden | PCC | 2000–2003 | Malignant brain tumor (20–80) | Digital | Use vs. no use (latency period >1 year) | 1.9 (1.3 to 2.7) | Age, sex, socioeconomic index, and year of diagnosis | 317 (88%) | 692 (84%) |
| Hardell et al., 2007 [19] | Sweden | PCC | 1993–1997 | Testicular cancer (20–75) | Digital | Use vs. no use (latency period >1 year) | 1.1 (0.8 to 1.5) | Age, year of diagnosis, and cryptorchidism | 889 (91%) | 870 (89%) |
| Hardell et al., 2010 [20] | Sweden | PCC | 1997–2003 | Malignant brain tumor (20–80) | Digital | Use vs. no use (latency period >1 year) | 1.4 (0.97 to 2.1) | Age, sex, socio-economic index code, and year of diagnosis | 346 (75%) | 619 (67%) |
| Hardell et al., 2011 [21] | Sweden | PCC | 2000–2003 | Malignant melanoma (20–77) | Analog and digital | Use vs. no use (latency period >1 year) | 1.0 (0.7 to 1.3) | Age, gender, and year of diagnosis | 347 (82%) | 1184 (80%) |
| Söderqvist et al., 2012 [22] | Sweden | PCC | 2000–2003 | Salivary gland tumor (22–80) | Digital | Use vs. no use (latency period >1 year) | 0.9 (0.4 to 1.7) | Age, sex, year of diagnosis, and socio-economic index code | 69 (88%) | 262 (83%) |
| Hardell et al., 2013 [23] | Sweden | PCC | 2007–2009 | Malignant brain tumor (18–75) | Digital | Use vs. no use (latency period >1 year) | 1.7 (1.04 to 2.8) | Age, gender, socio-economic index code, and year of diagnosis | 593 (87%) | 1368 (85%) |
| INTERPHONE-related studies (n = 19) | ||||||||||
| Christensen et al., 2004 [24] | Denmark | PCC | 2000–2002 | Acoustic neuroma (20–69) | Cellular | Used regular vs. never or rarely used | 0.90 (0.51 to 1.57) | Education level, marital status, use of hands-free devices, and region | 107 (82%) | 214 (64%) |
| Lönn et al., 2004 [25] | Sweden | PCC | 1999–2002 | Acoustic neuroma (20–69) | Digital | Regular use vs. Never or rarely | 0.9 (0.6 to 1.4) | Age, sex, residential area, and education | 148 (93%) | 604 (72%) |
| Christensen et al., 2005 [26] | Denmark | PCC | 2000–2002 | Low- grade glioma (20–69) | Cellular | Regular use vs. no regular use | 0.58 (0.37 to 0.90) | Sex, age, education, hands-free devices in cars, marital status, and region | 171 (74%) | 330 (64%) |
| High-grade glioma (20–69) | 1.08 (0.58 to 2.00) | 81 (74%) | 155 (64%) | |||||||
| Meningioma (20–69) | 0.83 (0.54 to 1.28) | 175 (74%) | 316 (64%) | |||||||
| Lönn et al., 2005 [27] | Sweden | PCC | 2000–2002 | Glioma (20–69) | Digital | Regular use vs. never or rarely use | 0.8 (0.6 to 1.0) | Age, gender, geographic region, and education | 371 (74%) | 674 (71%) |
| Meningioma (20–69) | 0.6 (0.5 to 0.9) | |||||||||
| Schoemaker et al., 2005 [28] | Denmark, Finland, Norway, Sweden, and UK | PCC | 1999–2004 | Acoustic neuroma (18–69) | Digital | Regular use vs. Never/non-regular use | 0.9 (0.7 to 1.1) | Highest educational level and combinations of interview year and interview lag time | 678 (83%) | 3553 (51%) |
| Hepworth et al., 2006 [29] | UK | PCC | 2000–2003 | Glioma (18–69) | Mobile | Regular use vs. never/non-regular | 0.94 (0.78 to 1.13) | Age, sex, region, Townsend deprivation category, and interview reference date category | 966 (51%) | 1716 (45%) |
| Schuz et al., 2006 [30] | Germany | PCC | 2000–2003 | Glioma (30–69) | Cellular | Ever use vs. never use | 0.98 (0.74 to 1.29) | Age, socioeconomic status, and living in a city | 366 (80%) | 732 (60%) |
| Meningioma (30–69) | 0.84 (0.62 to 1.13) | 381 (80%) | 762 (60%) | |||||||
| Lönn et al., 2006 [31] | Denmark and Sweden | PCC | 2000–2002 | Benign pleomorphic adenomas (20–69) | Mobile | Regular use vs. never or rarely use | 0.9 (0.5 to 1.5) | Age, gender, geographic region, and education | 112 (88%) | 321 (70%) |
| Malignant parotid gland tumors (20–69) | 0.7 (0.4 to 1.3) | 60 (85%) | 681 (70%) | |||||||
| Takebayashi et al., 2006 [32] | Japan | PCC | 2000–2004 | Acoustic neuroma (30–69) | Digital | Regular user vs. non-user | 0.68 (0.40 to 1.18) | Education and marital status | 101 (84%) | 339 (52%) |
| Klaeboe et al., 2007 [33] | Norway | PCC | 2001–2002 | Glioma (19–69) | Digital | Regular use vs. no or irregular use | 0.6 (0.4 to 0.8) | Age, sex, residential area, and education | 289 (77%) | 358 (69%) |
| Meningioma (19–69) | 0.6 (0.4 to 1.0) | |||||||||
| Lahkola et al., 2007 [34] | Denmark, Finland, Norway, Sweden, and UK | PCC | 2000–2004 | Glioma (20–69) | Digital | Regular use vs. never /non- regular use | 0.75 (0.65 to 0.87) | None (adjustment for education and family history of glioma did not affect the result) | 1521 (60%) | 3301 (50%) |
| Schlehofer et al., 2007 [35] | Germany | PCC | 2000–2003 | Acoustic neuroma (30–69) | Mobile | Ever use vs. never use | 0.67 (0.38 to 1.19) | SES, living area, age at diagnosis, and study center | 97 (89%) | 194 (55%) |
| Lahkola et al., 2008 [36] | Denmark, Finland, Norway, Sweden, and UK | PCC | 2000–2004 | Meningioma (18–69) | Digital | Regular use vs. never/non-regular | 0.74 (0.63 to 0.87) | Sex, five-year age group, region, and country | 1209 (74%) | 3299 (50%) |
| Sadetzki et al., 2008 [37] | Israel | PCC | 2001–2003 | Parotid gland tumors (≥18) | Cellular | Regular user vs. no regular user (<1 year) | 0.87 (0.68 to 1.13) | None (adjustment for cigarette smoking did not affect the result) | 460 (87%) | 1266 (66%) |
| Takebayashi et al., 2008 [38] | Japan | PCC | 2000–2004 | Glioma (30–69) | Digital | Regular user vs. non-user | 1.29 (0.66 to 2.53) | Education and marital status | 88 (59%) | 196 (53%) |
| Meningioma (30–69) | 0.67 (0.40 to 1.13) | 132 (78%) | 279 (52%) | |||||||
| Pituitary adenoma (30–69) | 0.95 (0.53 to 1.71) | 102 (76%) | 208 (49%) | |||||||
| Schoemaker et al., 2009 [39] | UK | PCC | 2001–2005 | Pituitary tumor (18–59) | Digital | Regular use vs. never/non-regular use | 0.9 (0.7 to 1.3) | Sex, age category, geographic area within study region, reference date, and Townsend deprivation score | 291 (63%) | 630 (43%) |
| The INTERPHONE Study Group, 2010 [40] | 13 c Countries | PCC | 2000–2004 | Glioma (30–59) | Mobile | Regular use vs. no regular use | 0.81 (0.70 to 0.94) | Sex, age, study center, ethnicity in Israel, and education | 2708 (64%) | 2972 (53%) |
| Meningioma (30–59) | 0.79 (0.68 to 0.91) | 2409 (78%) | 2662 (53%) | |||||||
| The INTERPHONE Study Group, 2011 [41] | 13 c Countries | PCC | 2000–2004 | Acoustic neuroma (30–59) | Mobile | Regular use vs. no regular use | 0.85 (0.69 to 1.04) | Sex, age, study center, ethnicity, and education | 1105 (85%) | 2145 (53%) |
| Shrestha et al., 2015 [42] | Finland | PCC | 2000–2002 | Pituitary tumor (20–69) | Digital | Regular use vs. never /non-regular use | 0.38 (0.21 to 0.68) | Not described | 80 (42%) | 240 (77%) |
| Studies by other groups (n = 16) | ||||||||||
| Muscat et al., 2000 [43] | US | HCC | 1994–1998 | Brain cancer (18–80) | Cellular | Regular use vs. no use | 0.8 (0.6 to 1.2) | Age, education, sex, race, study center, proxy subject, and month and year of interview | 469 (82%) | 346 (90%) |
| Inskip et al., 2001 [44] | US | HCC | 1994–1998 | Brain tumor (≥18) | Cellular | Use vs. no use | 0.9 (0.7 to 1.1) | Age, sex, race, hospital, distance from patient’s residence to hospital, education, household income, date of interview, and interview respondent | 782 (80%) | 799 (86%) |
| Auvinen et al., 2002 [45] | Finland | PCC | 1996 | Brain tumor (20–69) | Digital | Ever use vs. never use | 0.9 (0.5 to 1.5) | Described that adjusted odds ratios were calculated, and potential confounding factors were urban residence, socioeconomic status, and occupation | 398 (n.a.) | 2160 (n.a.) |
| Warren et al., 2003 [46] | US | HCC | 1995–2000 | Infratemporal facial nerve tumor (mean 47) | Cellular | Use vs. no use | 0.6 (0.2 to 1.9) | Described that a multivariate model was used, but not presented | 18 (n.a.) | 141 (n.a.) |
| Linet et al., 2006 [47] | US | PCC | 1998–2000 | Non-Hodgkin’s lymphoma (20–74) | Cellular | Ever used vs. ever used | 1.0 (0.7 to 1.3) | Age, ethnic group, education, and geographic site | 551 (79%) | 462 (55%) |
| Kaufman et al., 2009 [48] | Thailand | HCC | 1997–2003 | Leukemia (≥18) | Cellular | Use vs. no use | 1.5 (1.0 to 2.4) | Age, sex, income, use of cellphones, benzene and other solvent exposure, occupational and non-occupational pesticide exposure, pesticides used near the home, working with power lines, and living near power lines | 180 (n.a.) | 756 (n.a.) |
| Stang et al., 2009 [49] | Germany | HCC | 2002–2004 | Uveal melanoma (20–74) | Mobile | Regular use vs. never | 0.7 (0.5 to 1.0) | Age, sex, and residence | 827 (94%) | 455 (57%) |
| Cooke et al., 2010 [50] | UK | PCC | 2003–2009 | Leukemia (18–59) | Mobile | Regular use vs. never/non-regular use | 1.06 (0.76 to 1.46) | Age, sex, socio-economic status, area of residence, ethnicity, smoking status, and interview lag time/period | 806 (50%) | 589 (75%) |
| Spinelli et al., 2010 [51] | France | HCC | 2005 | Brain cancer (20–87) | Cellular | >36 h-years vs. no use | 1.07 (0.41 to 2.82) | Age and sex | 116 (75%) | 116 (90%) |
| Aydin et al., 2011 [52] | Denmark, Norway, Sweden, and Switzerland | PCC | 2004–2008 | Brain tumors (7–19) | Mobile | Regular use vs. no regular use | 1.36 (0.92 to 2.02) | Unadjusted (SES, family history of cancer, past medical radiation exposure to the head, maternal smoking during pregnancy, past head injuries, and use of baby monitors did not change the results) | 352 (83%) | 646 (71%) |
| Duan et al., 2011 [53] | China | HCC | 1993–2000 | Epithelial parotid gland malignancies (7–80) | Cellular | Regular use vs. never or rarely use | 1.14 (0.72 to 1.81) | Gender, age, resident area, marital status, education background, monthly income, and smoking status | 136 (62%) | 2051 (78%) |
| Corona et al., 2012 [54] | Brazil | HCC | 2000–2010 | Vestibular schwannoma (mean 49 in cases, 53 in controls) | Cellular | Regular use vs. no use/irregular use | 1.19 (0.54 to 2.59) | Not described | 44 (52%) | 104 (57%) |
| Coureau et al., 2014 [55] | France | PCC | 2004–2006 | Glioma (≥16) | Mobile | Regular user vs. no regular user | 1.24 (0.86 to 1.77) | Education and ionizing radiation exposure | 253 (66%) | 504 (45%) |
| Meningioma (≥16) | 0.90 (0.61 to 1.34) | 194 (75%) | 388 (45%) | |||||||
| Feltbower et al., 2014 [56] | UK | PCC | 2007–2010 | Brain tumor (0–24) | Mobile | Spoken on a mobile phone more than 20 times vs. not | 0.9 (0.2 to 3.3) | Age, sex, and Townsend deprivation index | 49 (52%) | 78 (32%) |
| Pettersson et al., 2014 [57] | Sweden | PCC | 2002–2007 | Acoustic neuroma (20–69) | Digital | Regular use vs. never or rarely use | 1.26 (0.90 to 1.75) | Unadjusted (smoking, education, marital status, parity, and hands-free use did not affect the results) | 422 (83%) | 643 (65%) |
| Yoon et al., 2015 [58] | Korea | HCC | 2002–2007 | Glioma (15–69) | Mobile | User vs. non-user | 1.17 (0.63 to 2.14) | Age, sex, area, education, respondent type, hair coloring, alcohol drinking, computer use, and electro-blanket use | 285 (32%) | 285 (27%) |
| Factor | All | Hardell et al. Studies | INTERPHONE-Related Studies | Studies by Other Groups | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | OR (95% CI) | I2 (%) | No. | OR (95% CI) | I2 (%) | No. | OR (95% CI) | I2 (%) | No. | OR (95% CI) | I2 (%) | |||
| 36 | 0.99 (0.91 to 1.07) | 47.4 | 10 | 1.15 (1.00 to 1.33) * | 40.1 | 9 | 0.81 (0.75 to 0.88) | 1.3 | 17 | 1.02 (0.92 to 1.13) | 8.1 | |||
| Difference in response rates a | Smaller (<14.5%) | 16 | 1.07 (0.94 to 1.21) | 54.2 | 10 | 1.15 (1.00 to 1.33) * | 40.1 | 1 | 0.81 (0.70 to 0.94) | n.a. | 5 | 0.99 (0.81 to 1.2) | 21.1 | |
| Larger (>14.5%) | 17 | 0.91 (0.82 to 1.02) | 23.8 | n.a. | 8 | 0.81 (0.73 to 0.91) | 13.7 | 9 | 1.02 (0.90 to 1.17) | 0.0 | ||||
| Use of blinding at interview | Used | 10 | 1.16 (1.01to 1.34) * | 39.4 | 9 | 1.16 (1.00 to 1.35) * | 45.4 | n.a. | 1 | 1.19 (0.54 to 2.59) | n.a. | |||
| Not used | 26 | 0.91 (0.84 to 0.99) | 32.1 | 1 | 0.90 (0.44 to 1.70) | n.a. | 9 | 0.81 (0.75 to 0.88) | 1.3 | 16 | 1.02 (0.91 to 1.13) | 13.0 | ||
| Methodolog-ical quality b | High | NOS | 17 | 1.11 (1.00 to 1.22) * | 20.1 | 9 | 1.16 (1.00 to 1.35) * | 45.4 | 1 | 0.90 (0.66 to 1.23) | n.a. | 7 | 1.08 (0.92 to 1.27) | 0.0 |
| NHLBI | 20 | 1.09 (0.99 to 1.20) | 29.3 | 8 | 1.18 (1.00 to 1.40) | 50.7 | 2 | 0.80 (0.54 to 1.20) | 0.0 | 10 | 1.03 (0.91 to 1.15) | 0.0 | ||
| Low | NOS | 19 | 0.88 (0.80 to 0.97) | 33.9 | 1 | 0.90 (0.44 to 1.70) | n.a. | 8 | 0.81 (0.74 to 0.88) | 8.5 | 10 | 0.99 (0.85 to 1.16) | 30.5 | |
| NHLBI | 16 | 0.86 (0.78 to 0.95) | 27.2 | 2 | 0.95 (0.64 to 1.41) | 0.0 | 7 | 0.81 (0.74 to 0.90) | 22.4 | 7 | 0.99 (0.79 to 1.24) | 31.2 | ||
| Funding by cellular phone industry | Not funded | 28 | 1.07 (0.98 to 1.17) | 21.9 | 10 | 1.15 (1.00 to 1.33) * | 40.1 | 1 | 0.95 (0.53 to 1.71) | n.a. | 17 | 1.02 (0.92 to 1.13) | 8.1 | |
| Funded | 8 | 0.81 (0.74 to 0.89) | 10.6 | n.a. | 8 | 0.81 (0.74 to 0.89) | 10.6 | n.a. | ||||||
| Type of case-control study | HCC | 9 | 0.95 (0.80 to 1.12) | 22.4 | n.a. | n.a. | 9 | 0.95 (0.80 to 1.12) | 22.4 | |||||
| PCC | 27 | 1.00 (0.91 to 1.09) | 53.7 | 10 | 1.15 (1.00 to 1.33) * | 40.1 | 9 | 0.81 (0.75 to 0.88) | 1.3 | 8 | 1.10 (0.96 to 1.26) | 0.0 | ||
| Malignancy | Malignant | 21 | 1.08 (0.97 to 1.20) | 31.4 | 9 | 1.18 (1.02 to 1.37) | 38.5 | 2 | 0.84 (0.54 to 1.31) | 0.0 | 10 | 0.97 (0.84 to 1.12) | 8.8 | |
| Benign | 14 | 0.86 (0.77 to 0.95) | 21.9 | 3 | 0.92 (0.74 to 1.14) | 38.6 | 8 | 0.81 (0.72 to 0.90) | 14.6 | 3 | 1.07 (0.83 to 1.39) | 4.3 | ||
| Factor | All | Hardell et al.’s Studies | INTERPHONE-Related Studies | Other Groups | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | OR (95% CI) | I2 | No. | OR (95% CI) | I2 | No. | OR (95% CI) | I2 | No. | OR (95% CI) | I2 | ||
| Time since first use or latency (years) | <5 | 25 | 0.97 (0.86 to 1.09) | 39.0 | 10 | 1.05 (0.92 to 1.19) | 0.0 | 8 | 0.78 (0.64 to 0.94) | 36.2 | 8 | 1.10 (0.92 to 1.32) | 14.6 |
| 5–9 | 23 | 1.00 (0.86 to 1.16) | 51.0 | 10 | 1.20 (0.88 to 1.63) | 44.4 | 8 | 0.80 (0.70 to 0.92) | 13.7 | 5 | 1.19 (0.99 to 1.44) | 0.0 | |
| ≥10 | 18 | 1.29 (0.90 to 1.85) | 87.8 | 5 | 1.62 (1.03 to 2.57) * | 39.9 | 8 | 0.99 (0.79 to 1.24) | 25.3 | 5 | 1.57 (0.72 to 3.42) | 93.3 | |
| Cumulative or lifetime use (years) | <5 | 14 | 0.81 (0.74 to 0.90) | 19.6 | n.a. | 9 | 0.77 (0.69 to 0.86) | 15.8 | 5 | 0.99 (0.81 to 1.21) | 0.0 | ||
| 5–9 | 14 | 0.89 (0.78 to 1.01) | 22.9 | 9 | 0.83 (0.73 to 0.94) | 0.0 | 5 | 1.04 (0.75 to 1.46) | 54.4 | ||||
| ≥10 | 9 | 1.04 (0.69 to 1.59) | 36.9 | 5 | 0.92 (0.54 to 1.59) | 0.0 | 5 | 1.15 (0.61 to 2.18) | 77.1 | ||||
| Cumulative call time (hours) | <300 | 26 | 0.99 (0.90 to 1.08) | 0.0 | 9 | 1.08 (0.94 to 1.23) | 9.2 | 9 | 0.78 (0.66 to 0.93) | 0.0 | 8 | 1.05 (0.89 to 1.24) | 0.0 |
| 300–1000 | 7 | 1.14 (0.91 to 1.41) | 40.9 | 1 | 1.00 (0.40 to 2.60) | 2 | 1.07 (0.77 to 1.49) | 0.0 | 4 | 1.21 (0.79 to 1.84) | 40.9 | ||
| >1000 | 8 | 1.60 (1.12 to 2.30) * | 74.5 | 2 | 3.65 (1.69 to 7.85) * | 0.0 | 4 | 1.25 (0.96 to 1.62) | 23.7 | 2 | 1.73 (0.66 to 4.48) | 91.8 | |
| Cumulative number of calls | <1000 | 7 | 1.07 (0.87 to 1.32) | 9.6 | n.a. | 2 | 0.70 (0.38 to 1.29) | 0.0 | 5 | 1.13 (0.92 to 1.39) | 0.0 | ||
| 1000–7000 | 5 | 1.00 (0.69 to 1.43) | 51.6 | n.a. | n.a. | 5 | 1.00 (0.69 to 1.43) | 51.6 | |||||
| >7000 | 10 | 1.14 (0.39 to 3.32) | 98.6 | n.a. | 5 | 0.85 (0.56 to 1.29) | 55.1 | 5 | 1.68 (0.36 to 7.94) | 99.0 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.-J.; Moskowitz, J.M.; Myung, S.-K.; Lee, Y.-R.; Hong, Y.-C. Cellular Phone Use and Risk of Tumors: Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 8079. https://doi.org/10.3390/ijerph17218079
Choi Y-J, Moskowitz JM, Myung S-K, Lee Y-R, Hong Y-C. Cellular Phone Use and Risk of Tumors: Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(21):8079. https://doi.org/10.3390/ijerph17218079
Chicago/Turabian StyleChoi, Yoon-Jung, Joel M. Moskowitz, Seung-Kwon Myung, Yi-Ryoung Lee, and Yun-Chul Hong. 2020. "Cellular Phone Use and Risk of Tumors: Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 21: 8079. https://doi.org/10.3390/ijerph17218079
APA StyleChoi, Y. -J., Moskowitz, J. M., Myung, S. -K., Lee, Y. -R., & Hong, Y. -C. (2020). Cellular Phone Use and Risk of Tumors: Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 17(21), 8079. https://doi.org/10.3390/ijerph17218079