Depressive Disorders and Sleeping Disturbances—Surveys Study of 923 Participants on the Pol’and’Rock Festival, Kostrzyn, Poland 2019

 ,
,  , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling and Data Collection
2.2. Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Study Group
3.2. Prevalence of Depressive Symptoms
3.3. Presence of Insomnia
3.4. Relationship between Insomnia and Depressive Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Solomon, A.; Haaga, D.A.F.; Arnow, B.A. Is clinical depression distinct from subthreshold depressive symptoms? A review of the continuity issue in depression research. J. Nerv. Ment. Dis. 2001, 189, 498–506. [Google Scholar] [PubMed]
- Toledano-Toledano, F.; Contreras-Valdez, J.A. Validity and reliability of the Beck Depression Inventory II (BDI-II) in family caregivers of children with chronic diseases. PLoS ONE 2018, 13, e0206917. [Google Scholar] [CrossRef]
- Vos, T.; Abajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abate, K.H.; Abd-Allah, F.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; Aboyans, V.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- O’Callaghan, G.; Stringaris, A. Reward processing in adolescent depression across neuroimaging modalities. Z. Kinder Jugendpsychiatr. Psychother. 2019, 47, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Gururajan, A.; Naughton, M.E.; Scott, K.A.; O’Connor, R.M.; Moloney, G.; Clarke, G.; Dowling, J.; Walsh, A.; Ismail, M.F.; Shorten, G.; et al. MicroRNAs as biomarkers for major depression: A role for let-7b and let-7c. Transl. Psychiatry 2016, 6, e862. [Google Scholar] [CrossRef] [Green Version]
- Arnone, D.; Job, D.; Selvaraj, S.; Abe, O.; Amico, F.; Cheng, Y.; Colloby, S.J.; O’Brien, J.T.; Frodl, T.; Gotlib, I.H.; et al. Computational meta-analysis of statistical parametric maps in major depression. Hum. Brain Mapp. 2016, 37, 1393–1404. [Google Scholar] [CrossRef]
- Hansen, R.; Gaynes, B.; Thieda, P.; Gartlehner, G.; Deveaugh-Geiss, A.; Krebs, E.; Lohr, K. Meta-analysis of major depressive disorder relapse and recurrence with second-generation antidepressants. Psychiatr. Serv. 2008, 59, 1121–1130. [Google Scholar] [CrossRef] [Green Version]
- Koopman, M.; Daniels, J.K.; Spitzer, C.; Lampe, A.; El Aidy, S. Depressed gut? The microbiota-diet-inflammation trialogue in depression. Curr. Opin. Psychiatry 2017, 30, 369–377. [Google Scholar]
- Winter, G.; Hart, R.A.; Charlesworth, R.P.G.; Sharpley, C.F. Gut microbiome and depression: What we know and what we need to know. Rev. Neurosci. 2018, 29, 629–643. [Google Scholar] [PubMed]
- Ohayon, M.M. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Med. Rev. 2002, 6, 97–111. [Google Scholar] [PubMed]
- Ontario, H.Q. Psychotherapy for major depressive disorder and generalized anxiety disorder: A health technology assessment. Ont. Health Technol. Assess. Ser. 2017, 17, 1–167. [Google Scholar]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders: Diagnostic & Coding Manual, 2nd ed.; AASM: Westchester, NY, USA, 2005. [Google Scholar]
- Patel, D.; Steinberg, J.; Patel, P. Insomnia in the elderly: A review. J. Clin. Sleep Med. 2018, 14, 1017–1024. [Google Scholar]
- Suh, S.; Cho, N.; Zhang, J. Sex differences in Insomnia: From Epidemiology and etiology to intervention. Curr. Psychiatry Rep. 2018, 20, 69. [Google Scholar]
- Everitt, H.; Baldwin, D.S.; Stuart, B.; Lipinska, G.; Mayers, A.; Malizia, A.L.; Manson, C.C.F.; Wilson, S. Antidepressants for insomnia in adults. Cochrane Database Syst. Rev. 2018, 5, CD010753. [Google Scholar]
- Pasierb, N.; Filipczyk, K.; Kunert, Ł.; Piegza, M.; Pudlo, R. Insomnia in shift workers of a zinc smelter. Med. Pr. 2019, 70, 611–616. [Google Scholar] [CrossRef]
- Gebara, M.A.; Siripong, N.; DiNapoli, E.A.; Maree, R.D.; Germain, A.; Reynolds, C.F.; Kasckow, J.W.; Weiss, P.M.; Karp, J.F. Effect of insomnia treatments on depression: A systematic review and meta-analysis. Depress. Anxiety 2018, 35, 717–731. [Google Scholar]
- Franzen, P.L.; Buysse, D.J. Sleep disturbances and depression: Risk relationships for subsequent depression and therapeutic implications. Dialogues Clin. Neurosci. 2008, 10, 473–481. [Google Scholar]
- Baglioni, C.; Riemann, D. Is chronic insomnia a precursor to major depression? Epidemiological and biological findings. Curr. Psychiatry Rep. 2012, 14, 511–518. [Google Scholar] [CrossRef]
- Baglioni, C.; Battagliese, G.; Feige, B.; Spiegelhalder, K.; Nissen, C.; Voderholzer, U.; Lombardo, C.; Riemann, D. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect. Disord. 2011, 135, 10–19. [Google Scholar]
- Ohayon, M.M.; Shapiro, C.M.; Kennedy, S.H. Differentiating DSM-IV anxiety and depressive disorders in the general population: Comorbidity and treatment consequences. Can. J. Psychiatry 2000, 45, 166–172. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An Inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Basker, M.; Moses, P.D.; Russell, S.; Russell, P.S.S. The psychometric properties of beck depression Inventory for adolescent depression in a primary-care paediatric setting in India. Child Adolesc. Psychiatry Ment. Health 2007, 1, 8. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.P.; Gorenstein, C. Psychometric properties of the Beck Depression Inventory-II: A comprehensive review. Rev. Bras. Psiquiatr. 2013, 35, 416–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smarr, K.L.; Keefer, A.L. Measures of depression and depressive symptoms: Beck Depression Inventory-II (BDI-II), Center for Epidemiologic Studies Depression Scale (CES-D), Geriatric Depression Scale (GDS), Hospital Anxiety and Depression Scale (HADS), and Patient Health Questionnaire-9 (PHQ-9). Arthritis Care Res. 2011, 63, S454–S466. [Google Scholar] [CrossRef]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale: Validation of an instrument based on ICD-10 criteria. J. Psychosom. Res. 2000, 48, 555–560. [Google Scholar] [CrossRef]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. The diagnostic validity of the Athens Insomnia Scale. J. Psychosom. Res. 2003, 55, 263–267. [Google Scholar] [CrossRef]
- Depression. Available online: https://www.who.int/en/news-room/fact-sheets/detail/depression (accessed on 26 May 2020).
- Kużel, A.; Krajewska-Kułak, E.; Śmigielska-Kuzia, J. Perception of depression in selected social groups. Med. Ogólna Nauk. Zdrowiu 2015, 21, 295–302. [Google Scholar] [CrossRef]
- Dróżdż, W.; Wojnar, M.; Araszkiewicz, A.; Nawacka-Pawlaczyk, D.; Urbański, R.; Cwiklińska-Jurkowska, M.; Rybakowski, J. The study of the prevalence of depressive disorders in primary care patients in Poland. Wiad. Lek. 2007, 60, 109–113. [Google Scholar]
- Bjelland, I.; Krokstad, S.; Mykletun, A.; Dahl, A.A.; Tell, G.S.; Tambs, K. Does a higher educational level protect against anxiety and depression? The HUNT study. Soc. Sci. Med. 2008, 66, 1334–1345. [Google Scholar] [CrossRef]
- Gan, Z.; Li, Y.; Xie, D.; Shao, C.; Yang, F.; Shen, Y.; Zhang, N.; Zhang, G.; Tian, T.; Yin, A.; et al. The impact of educational status on the clinical features of major depressive disorder among Chinese women. J. Affect. Disord. 2012, 136, 988–992. [Google Scholar] [CrossRef] [Green Version]
- Akhtar-Danesh, N.; Landeen, J. Relation between depression and sociodemographic factors. Int. J. Ment. Health Syst. 2007, 1, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Lorant, V.; Deliège, D.; Eaton, W.; Robert, A.; Philippot, P.; Ansseau, M. Socioeconomic inequalities in depression: A meta-analysis. Am. J. Epidemiol. 2003, 157, 98–112. [Google Scholar] [CrossRef] [Green Version]
- Kate, J.T.; de Koster, W.; van der Waal, J. Why are depressive symptoms more prevalent among the less educated? The relevance of low cultural capital and cultural entitlement. Sociol. Spectr. 2017, 37, 63–76. [Google Scholar] [CrossRef] [Green Version]
- Farabaugh, A.; Bitran, S.; Nyer, M.; Holt, D.J.; Pedrelli, P.; Shyu, I.; Hollon, S.D.; Zisook, S.; Baer, L.; Busse, W.; et al. Depression and suicidal ideation in college students. Psychopathology 2012, 45, 228–234. [Google Scholar] [CrossRef]
- Orth, U.; Robins, R.W.; Widaman, K.F.; Conger, R.D. Is low self-esteem a risk factor for depression? Findings from a longitudinal study of mexican-origin youth. Dev. Psychol. 2014, 50, 622–633. [Google Scholar] [CrossRef] [Green Version]
- Yun, J.Y.; Choi, Y.; Kwon, Y.; Lee, H.Y.; Choi, S.H.; Jang, J.H. Hubness of strategic planning and sociality influences depressive mood and anxiety in College Population. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kiejna, A.; Wojtyniak, B.; Rymaszewska, J.; Stokwiszewski, J. Prevalence of insomnia in Poland-Results of the National Health Interview Survey. Acta Neuropsychiatr. 2003, 15, 68–73. [Google Scholar] [CrossRef]
- Li, R.H.Y.; Wing, Y.K.; Ho, S.C.; Fong, S.Y.Y. Gender differences in insomnia—A study in the Hong Kong Chinese population. J. Psychosom. Res. 2002, 53, 601–609. [Google Scholar] [CrossRef]
- Bixler, E.; Kales, A.; Soldatos, C.; Kales, J.; Healey, S. Prevalence of sleep disorders in the Los Angeles metropolitan area. Am. J. Psychiatry 1979, 136, 1257–1262. [Google Scholar] [PubMed]
- Hohagen, F.; Rink, K.; Kappler, C.; Schramm, E.; Riemann, D.; Weyerer, S.; Berger, M. Prevalence and treatment of insomnia in general practice. A longitudinal study. Eur. Arch. Psychiatry Clin. Neurosci. 1993, 242, 329–336. [Google Scholar] [CrossRef]
- Zhang, B.; Wing, Y.K. Sex differences in insomnia: A meta-analysis. Sleep 2006, 29, 85–93. [Google Scholar] [CrossRef]
- Reyner, A.; Horne, J. Gender- and age-related differences in sleep determined by home-recorded sleep logs and actimetry from 400 adult. Sleep 1995, 18, 127–134. [Google Scholar]
- Lindberg, E.; Janson, C.; Gislason, T.; Björnsson, E.; Hetta, J.; Boman, G. Sleep disturbances in a young adult population: Can gender differences be explained by differences in psychological status? Sleep 1997, 20, 381–387. [Google Scholar] [CrossRef] [Green Version]
- Medicines used in generalized anxiety and sleep disorders. In Pharmacological Treatment of Mental Disorders in Primary Health Care; World Health Organization: Geneva, Switzerland, 2009; pp. 37–44.
- Staner, L. Sleep and anxiety disorders. Dialogues Clin. Neurosci. 2003, 5, 249–258. [Google Scholar]
- Mazzotti, D.R.; Guindalini, C.; Sosa, A.L.; Ferri, C.P.; Tufik, S. Prevalence and correlates for sleep complaints in older adults in low and middle income countries: A 10/66 Dementia Research Group study. Sleep Med. 2012, 13, 697–702. [Google Scholar] [CrossRef]
- Short, M.A.; Weber, N. Sleep duration and risk-taking in adolescents: A systematic review and meta-analysis. Sleep Med. Rev. 2018, 41, 185–196. [Google Scholar] [CrossRef] [Green Version]
- Hedin, G.; Norell-Clarke, A.; Hagell, P.; Tønnesen, H.; Westergren, A.; Garmy, P. Insomnia in relation to academic performance, self-reported health, physical activity, and substance use among adolescents. Int. J. Environ. Res. Public Health 2020, 17, 6433. [Google Scholar] [CrossRef]
- Bartel, K.A.; Gradisar, M.; Williamson, P. Protective and risk factors for adolescent sleep: A meta-analytic review. Sleep Med. Rev. 2015, 21, 72–85. [Google Scholar] [CrossRef]
- Mallampalli, M.P.; Carter, C.L. Exploring sex and gender differences in sleep health: A society for women’s health research report. J. Women’s Health 2014, 23, 553–562. [Google Scholar] [CrossRef] [Green Version]
- Tsuno, N.; Besset, A.; Ritchie, K. Sleep and depression. J. Clin. Psychiatry 2005, 66, 1254–1269. [Google Scholar] [CrossRef] [PubMed]
- Ford, D.E.; Cooper-Patrick, L. Sleep disturbances and mood disorders: An epidemiologic perspective. Depress. Anxiety 2001, 14, 3–6. [Google Scholar] [CrossRef]
- Thase, M.E. Depression and sleep: Pathophysiology and treatment. Dialogues Clin. Neurosci. 2006, 8, 217–226. [Google Scholar]
- Wichniak, A.; Wierzbicka, A.; Jernajczyk, W. Sleep and antidepressant treatment. Curr. Pharm. Des. 2012, 18, 5802–5817. [Google Scholar] [CrossRef] [PubMed]
- Janowsky, D.S.; Davis, J.M.; El-Yousef, M.K.; Sekerke, H.J. A cholinergic-adrenergic hypothesis of mania and depression. Lancet 1972, 300, 632–635. [Google Scholar] [CrossRef]
- Carneiro, L.S.F.; Mota, M.P.; Vieira-Coelho, M.A.; Alves, R.C.; Fonseca, A.M.; Vasconcelos-Raposo, J. Monoamines and cortisol as potential mediators of the relationship between exercise and depressive symptoms. Eur. Arch. Psychiatry Clin. Neurosci. 2017, 267, 117–121. [Google Scholar] [CrossRef]
- Holsboer, F. The corticosteroid receptor hypothesis of depression. Neuropsychopharmacology 2000, 23, 477–501. [Google Scholar] [CrossRef] [Green Version]
- Becker, N.B.; Jesus, S.N.; João, K.A.D.R.; Viseu, J.N.; Martins, R.I.S. Depression and sleep quality in older adults: A meta-analysis. Psychol. Health Med. 2017, 22, 889–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagai, M.; Hoshide, S.; Kario, K. Sleep duration as a risk factor for cardiovascular disease—A review of the recent literature. Curr. Cardiol. Rev. 2010, 6, 54–61. [Google Scholar] [CrossRef]
- Irwin, M.R.; Olmstead, R.; Carroll, J.E. Sleep disturbance, sleep duration, and inflammation: A systematic review and meta-analysis of cohort studies and experimental sleep deprivation. Biol. Psychiatry 2016, 80, 40–52. [Google Scholar] [CrossRef] [Green Version]
- Wirz-Justice, A. Chronobiology and mood disorders. Dialogues Clin. Neurosci. 2003, 5, 315–325. [Google Scholar] [PubMed]
- Slavich, G.M.; Irwin, M.R. From stress to inflammation and major depressive disorder: A social signal transduction theory of depression. Psychol. Bull. 2014, 140, 774–815. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Points | Degree of Depressive Symptoms |
|---|---|
| 0–13 | Minimal range |
| 14–19 | Mild |
| 20–28 | Moderate |
| 29–63 | Severe |
| Parameter | Median | IQR |
|---|---|---|
| Body mass (kg) | 69 | 60.0 to 80.0 |
| Age (years) | 25 | 22.0 to 29.0 |
| Height (cm) | 172 | 165.0 to 180.0 |
| AIS questionnaire score | 4.0 | 2.0 to 8.0 |
| Beck questionnaire score | 7.0 | 3.0 to 14.0 |
| Degree of Depressive Phenotype | N (%) |
|---|---|
| Minimal range | 635 (68.8%) |
| Mild | 172 (18.6%) |
| Moderate | 54 (5.9%) |
| Severe | 62 (6.7%) |
| Variable | Minimal Depressive Symptoms | Mild Depressive Symptoms | Moderate Depressive Symptoms | Severe Depressive Symptoms | p |
|---|---|---|---|---|---|
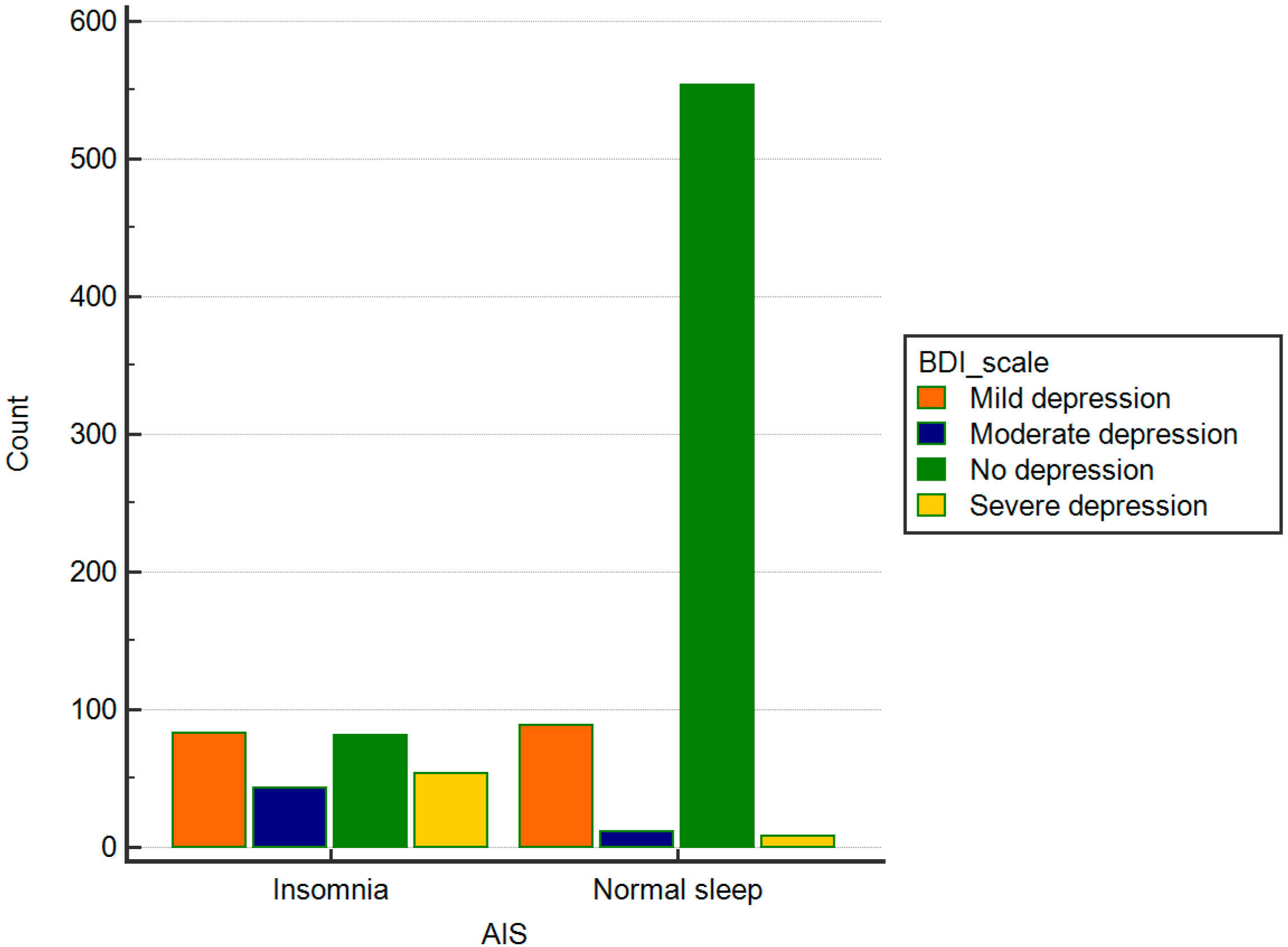
| Insomnia | 81 | 83 | 43 | 54 | |
| Normal sleep | 554 | 89 | 11 | 8 | <0.0001 |
| total | 635 68.8% | 172 18.6% | 54 5.9% | 62 6.7% |
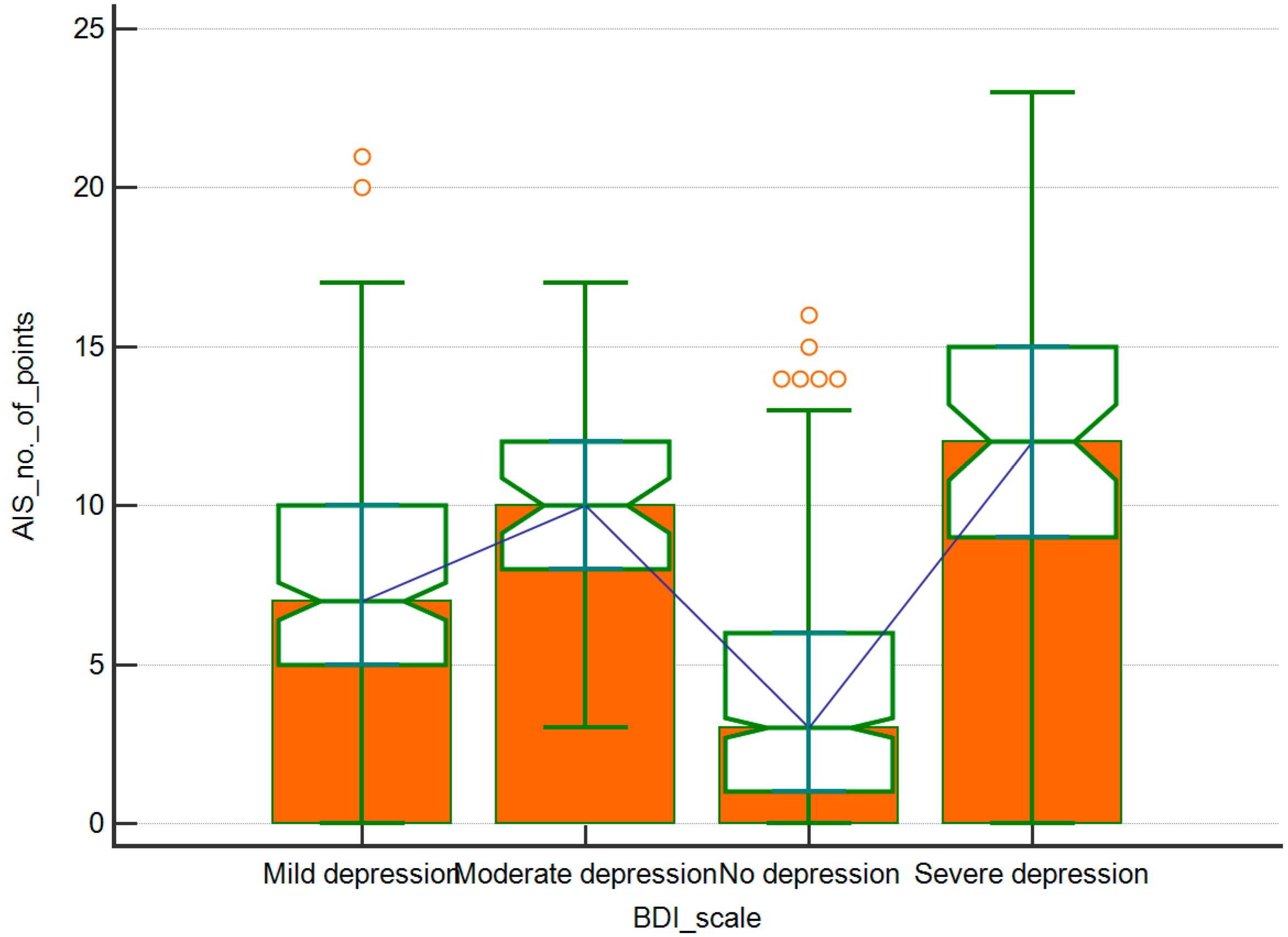
| Number of BDI-II Points vs.: | Correlation Coefficient | p |
|---|---|---|
| Number of AIS points | 0.65 | <0.0001 |
| Age | −0.124 | 0.0002 |
| Body weight | −0.061 | 0.0644 |
| Number of AIS Points vs.: | Correlation | p |
|---|---|---|
| Number of BDI-II points | 0.65 | <0.0001 |
| Age | −0.041 | 0.2169 |
| Body weight | −0.044 | 0.1817 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kałduńska, J.; Skonieczna-Żydecka, K.; Ryterska, K.; Palma, J.; Żwierełło, W.; Maciejewska-Markiewicz, D.; Czerwińska-Rogowska, M.; Wolska, A.; Stachowska, Z.; Budawski, R.; et al. Depressive Disorders and Sleeping Disturbances—Surveys Study of 923 Participants on the Pol’and’Rock Festival, Kostrzyn, Poland 2019. Int. J. Environ. Res. Public Health 2020, 17, 8092. https://doi.org/10.3390/ijerph17218092
Kałduńska J, Skonieczna-Żydecka K, Ryterska K, Palma J, Żwierełło W, Maciejewska-Markiewicz D, Czerwińska-Rogowska M, Wolska A, Stachowska Z, Budawski R, et al. Depressive Disorders and Sleeping Disturbances—Surveys Study of 923 Participants on the Pol’and’Rock Festival, Kostrzyn, Poland 2019. International Journal of Environmental Research and Public Health. 2020; 17(21):8092. https://doi.org/10.3390/ijerph17218092
Chicago/Turabian StyleKałduńska, Justyna, Karolina Skonieczna-Żydecka, Karina Ryterska, Joanna Palma, Wojciech Żwierełło, Dominika Maciejewska-Markiewicz, Maja Czerwińska-Rogowska, Anna Wolska, Zofia Stachowska, Robert Budawski, and et al. 2020. "Depressive Disorders and Sleeping Disturbances—Surveys Study of 923 Participants on the Pol’and’Rock Festival, Kostrzyn, Poland 2019" International Journal of Environmental Research and Public Health 17, no. 21: 8092. https://doi.org/10.3390/ijerph17218092
APA StyleKałduńska, J., Skonieczna-Żydecka, K., Ryterska, K., Palma, J., Żwierełło, W., Maciejewska-Markiewicz, D., Czerwińska-Rogowska, M., Wolska, A., Stachowska, Z., Budawski, R., Mruk, H., Matyniak, D., Popik, M., Łoniewska, K., Czmielnik, M., Fryda, A., Wronski, M., & Stachowska, E. (2020). Depressive Disorders and Sleeping Disturbances—Surveys Study of 923 Participants on the Pol’and’Rock Festival, Kostrzyn, Poland 2019. International Journal of Environmental Research and Public Health, 17(21), 8092. https://doi.org/10.3390/ijerph17218092