Clinical Use of Acid Suppressants and Risk of Dementia in the Elderly: A Pharmaco-Epidemiological Cohort Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
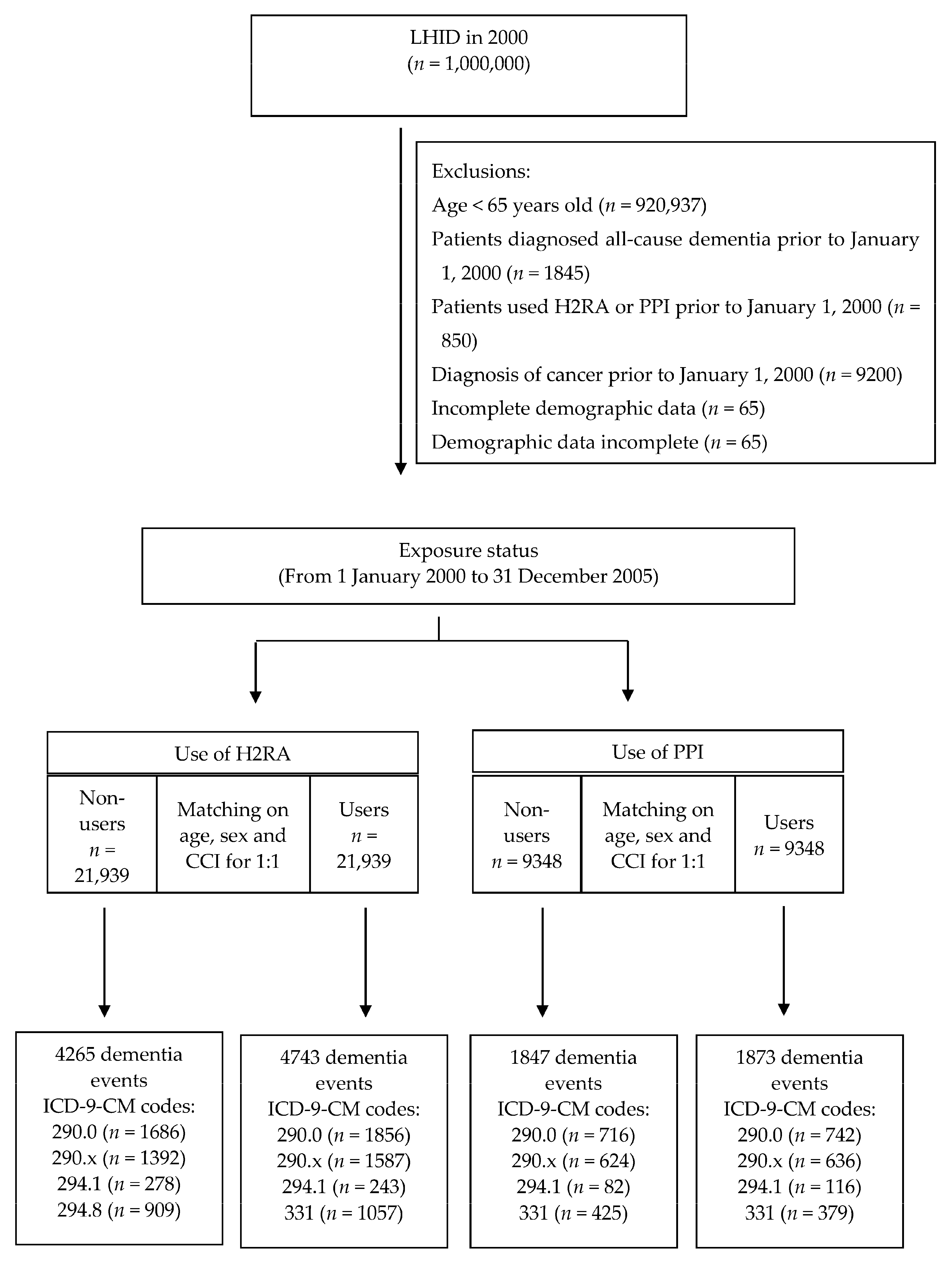
2.2. Participants
2.3. Exposure Measurement of Studied Medications
2.4. Ascertainment of Dementia
2.5. Covariate Ascertainment and Adjustment
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mannucci, P.M.; REPOSI Investigators; Nobili, A. Multimorbidity and polypharmacy in the elderly: Lessons from REPOSI. Intern. Emerg. Med. 2014, 9, 723–734. [Google Scholar] [CrossRef] [PubMed]
- Aoki, T.; Yamamoto, Y.; Ikenoue, T.; Onishi, Y.; Fukuhara, S. Multimorbidity patterns in relation to polypharmacy and dosage frequency: A nationwide, cross-sectional study in a Japanese population. Sci. Rep. 2018, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Fox, C.; Richardson, K.; Maidment, I.D.; Savva, G.M.; Matthews, F.E.; Smithard, D.; Coulton, S.; Katona, C.; Boustani, M.; Brayne, C. Anticholinergic Medication Use and Cognitive Impairment in the Older Population: The Medical Research Council Cognitive Function and Ageing Study. J. Am. Geriatr. Soc. 2011, 59, 1477–1483. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.; Patel, T.; Molnar, F.; Seitz, D. Optimizing medications in older adults with cognitive impairment: Considerations for primary care clinicians. Can. Fam. Physician 2018, 64, 646–652. [Google Scholar] [PubMed]
- GBD 2016 Dementia Collaborators. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990-2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 88–106. [Google Scholar] [CrossRef] [Green Version]
- Ponjoan, A.; Garre-Olmo, J.; Blanch, J.; Fages, E.; Alves-Cabratosa, L.; Martí-Lluch, R.; Comas-Cufí, M.; Parramon, D.; Garcia-Gil, M.; Ramos, R. Epidemiology of dementia: Prevalence and incidence estimates using validated electronic health records from primary care. Clin. Epidemiol. 2019, 11, 217–228. [Google Scholar] [CrossRef] [Green Version]
- Lam, J.R.; Schneider, J.L.; Zhao, W.; Corley, D.A. Proton Pump Inhibitor and Histamine 2 Receptor Antagonist Use and Vitamin B12Deficiency. JAMA 2013, 310, 2435–2442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scally, B.; Emberson, J.R.; Spata, E.; Reith, C.; Davies, K.; Halls, H.; Holland, L.; Wilson, K.; Bhala, N.; Hawkey, C.; et al. Effects of gastroprotectant drugs for the prevention and treatment of peptic ulcer disease and its complications: A meta-analysis of randomised trials. Lancet Gastroenterol. Hepatol. 2018, 3, 231–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haas, H.L.; Sergeeva, O.A.; Selbach, O. Histamine in the Nervous System. Physiol. Rev. 2008, 88, 1183–1241. [Google Scholar] [CrossRef]
- Hanlon, J.T.; Landerman, L.R.; Artz, M.B.; Gray, S.L.; Fillenbaum, G.G.; Schmader, K.E. Histamine2 receptor antagonist use and decline in cognitive function among community dwelling elderly. Pharmacoepidemiol. Drug Saf. 2004, 13, 781–787. [Google Scholar] [CrossRef]
- Breitner, J.C.; Welsh, K.A.; Helms, M.J.; Gaskell, P.C.; Gau, B.A.; Roses, A.D.; Pericak-Vance, M.A.; Saunders, A.M. Delayed onset of Alzheimer’s disease with nonsteroidal anti-inflammatory and histamine H2 blocking drugs. Neurobiol. Aging 1995, 16, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Anthony, J.C.; Breitner, J.C.S.; Zandi, P.P.; Meyer, M.R.; Jurasova, I.; Norton, M.C.; Stone, S.V. Reduced prevalence of AD in users of NSAIDs and H2 receptor antagonists: The Cache County study. Neurology 2000, 54, 2066–2071. [Google Scholar] [CrossRef] [PubMed]
- Launer, L.; Jama, J.; Ott, A.; Breteler, M.M.; Hoes, A.; Hofman, A. Histamine H2 Blocking Drugs and the Risk for Alzheimer’s Disease: The Rotterdam Study. Neurobiol. Aging 1997, 18, 257–259. [Google Scholar] [CrossRef]
- Zandi, P.P.; Anthony, J.C.; Hayden, K.M.; Mehta, K.; Mayer, L.; Breitner, J.C. Reduced incidence of AD with NSAID but not H2 receptor antagonists: The Cache County Study. Neurology 2002, 59, 880–886. [Google Scholar] [CrossRef]
- Gray, S.L.; Walker, R.; Dublin, S.; Haneuse, S.; Crane, P.K.; Breitner, J.C.S.; Bowen, J.; McCormick, W.; Larson, E.B. Histamine-2 Receptor Antagonist Use and Incident Dementia in an Older Cohort. J. Am. Geriatr. Soc. 2011, 59, 251–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boustani, M.; Hall, K.S.; Lane, K.A.; Aljadhey, H.; Gao, S.; Unverzagt, F.; Murray, M.D.; Ogunniyi, A.; Hendrie, H. The association between cognition and histamine-2 receptor antagonists in African Americans. J. Am. Geriatr. Soc. 2007, 55, 1248–1253. [Google Scholar] [CrossRef] [PubMed]
- Hwang, I.C.; Chang, J.; Park, S.M. A Nationwide Population-Based Cohort Study of Dementia Risk among Acid Suppressant Users. Am. J. Geriatr. Psychiatry 2018, 26, 1175–1183. [Google Scholar] [CrossRef]
- Forgacs, I.; Loganayagam, A. Overprescribing proton pump inhibitors. BMJ 2008, 336, 2–3. [Google Scholar] [CrossRef] [Green Version]
- Vogiatzoglou, A.; Smith, A.D.; Nurk, E.; Drevon, C.A.; Ueland, P.M.; Vollset, S.E.; Nygaard, H.A.; Engedal, K.; Tell, G.S.; Refsum, H. Cognitive Function in an Elderly Population. Psychosom. Med. 2013, 75, 20–29. [Google Scholar] [CrossRef] [Green Version]
- Haenisch, B.; Von Holt, K.; Wiese, B.; Prokein, J.; Lange, C.; Ernst, A.; Brettschneider, C.; König, H.-H.; Werle, J.; Weyerer, S.; et al. Risk of dementia in elderly patients with the use of proton pump inhibitors. Eur. Arch. Psychiatry Clin. Neurosci. 2015, 265, 419–428. [Google Scholar] [CrossRef]
- Gomm, W.; Von Holt, K.; Thomé, F.; Broich, K.; Maier, W.; Fink, A.; Doblhammer, G.; Haenisch, B. Association of Proton Pump Inhibitors with Risk of Dementia. JAMA Neurol. 2016, 73, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Wijarnpreecha, K.; Thongprayoon, C.; Panjawatanan, P.; Ungprasert, P. Proton pump inhibitors and risk of dementia. Ann. Transl. Med. 2016, 4, 240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tai, S.-Y.; Chien, C.-Y.; Wu, D.-C.; Lin, K.-D.; Ho, B.-L.; Chang, Y.-H.; Chang, Y.-P. Risk of dementia from proton pump inhibitor use in Asian population: A nationwide cohort study in Taiwan. PLoS ONE 2017, 12, e0171006. [Google Scholar] [CrossRef] [PubMed]
- Imfeld, P.; Bodmer, M.; Jick, S.S.; Meier, C.R. Proton Pump Inhibitor Use and Risk of Developing Alzheimer’s Disease or Vascular Dementia: A Case–Control Analysis. Drug Saf. 2018, 41, 1387–1396. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Luo, Z.; Yu, S.; Tang, Z. Proton pump inhibitor use and risk of dementia. Medicine 2019, 98, e14422. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, F.C.; Steenland, K.; Zhao, L.; Wharton, W.; Levey, A.I.; Hajjar, I. Proton Pump Inhibitors and Risk of Mild Cognitive Impairment and Dementia. J. Am. Geriatr. Soc. 2017, 65, 1969–1974. [Google Scholar] [CrossRef] [Green Version]
- Taipale, H.; Tolppanen, A.-M.; Tiihonen, M.; Tanskanen, A.; Tiihonen, J.; Hartikainen, S. No Association Between Proton Pump Inhibitor Use and Risk of Alzheimer’s Disease. Am. J. Gastroenterol. 2017, 112, 1802–1808. [Google Scholar] [CrossRef]
- Lochhead, P.; Hagan, K.; Joshi, A.D.; Khalili, H.; Grodstein, F.; Chan, A.T. Lack of Association Between Proton Pump Inhibitor Use and Cognitive Function in Women. Gastroenterology 2017, 152, S173. [Google Scholar] [CrossRef]
- Wod, M.; Hallas, J.; Andersen, K.; Rodríguez, L.A.G.; Christensen, K.; Gaist, D. Lack of Association Between Proton Pump Inhibitor Use and Cognitive Decline. Clin. Gastroenterol. Hepatol. 2018, 16, 681–689. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.Q.; Li, Y.; Zhang, S.L.; Gao, J.; Feng, S.Y. Proton pump inhibitor use does not increase dementia and Alzheimer’s disease risk: An updated meta-analysis of published studies involving 642305 patients. PLoS ONE 2019, 14, e0219213. [Google Scholar] [CrossRef] [PubMed]
- Booker, A.; Jacob, L.E.; Rapp, M.; Bohlken, J.; Kostev, K. Risk factors for dementia diagnosis in German primary care practices. Int. Psychogeriatr. 2016, 28, 1059–1065. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.-Y.; Chen, Y.-J.; Ho, H.J.; Hsu, Y.-C.; Kuo, K.N.; Wu, M.-S.; Lin, J.-T. Association between Nucleoside Analogues and Risk of Hepatitis B Virus–Related Hepatocellular Carcinoma Recurrence Following Liver Resection. JAMA 2012, 308, 1906–1913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, S.-H.; Chou, I.-J.; Yeh, Y.-H.; Chiou, M.-J.; Wen, M.-S.; Kuo, C.-T.; See, L.-C.; Kuo, C.-F. Association Between Use of Non–Vitamin K Oral Anticoagulants With and Without Concurrent Medications and Risk of Major Bleeding in Nonvalvular Atrial Fibrillation. JAMA 2017, 318, 1250–1259. [Google Scholar] [CrossRef] [PubMed]
- Chi, C.-C.; Tung, T.-H.; Wang, J.; Lin, Y.-S.; Chen, Y.-F.; Hsu, T.-K.; Wang, S.-H. Risk of Uveitis among People with Psoriasis. JAMA Ophthalmol. 2017, 135, 415–422. [Google Scholar] [CrossRef]
- Cheng, C.-L.; Kao, Y.-H.Y.; Lin, S.-J.; Lee, C.-H.; Lai, M.L. Validation of the national health insurance research database with ischemic stroke cases in Taiwan. Pharmacoepidemiol. Drug Saf. 2011, 20, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Kao, W.-H.; Hong, J.-H.; See, L.-C.; Yu, H.-P.; Hsu, J.-T.; Chou, I.-J.; Chou, W.-C.; Chiou, M.-J.; Wang, C.-C.; Kuo, C.-F. Validity of cancer diagnosis in the National Health Insurance database compared with the linked National Cancer Registry in Taiwan. Pharmacoepidemiol. Drug Saf. 2018, 27, 1060–1066. [Google Scholar] [CrossRef]
- Gau, C.-S.; Chang, I.-S.; Wu, F.-L.L.; Yu, H.-T.; Huang, Y.-W.; Chi, C.-L.; Chien, S.-Y.; Lin, K.-M.; Liu, M.-Y.; Wang, H.-P. Usage of the claim database of national health insurance programme for analysis of cisapride-erythromycin co-medication in Taiwan. Pharmacoepidemiol. Drug Saf. 2006, 16, 86–95. [Google Scholar] [CrossRef]
- Lin, L.-Y.; Warren-Gash, C.; Smeeth, L.; Chen, P.-C. Data resource profile: The National Health Insurance Research Database (NHIRD). Epidemiol. Health 2018, 40, e2018062. [Google Scholar] [CrossRef]
- Prince, M. Epidemiology of dementia. Psychiatry 2007, 6, 488–490. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Prada-Ramallal, G.; Takkouche, B.; Figueiras, A. Bias in pharmacoepidemiologic studies using secondary health care databases: A scoping review. BMC Med. Res. Methodol. 2019, 19, 1–14. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. ATC Index with DDDs 2003. Guidelines for ATC Classification and DDD Assignment; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Klabunde, C.N.; Warren, J.L.; Legler, J.M. Assessing Comorbidity Using Claims Data. Med. Care 2002, 40, 26–35. [Google Scholar] [CrossRef]
- Chew, M.L.; Mulsant, B.H.; Pollock, B.G.; Lehman, M.E.; Greenspan, A.; Mahmoud, R.A.; Kirshner, M.A.; Sorisio, D.A.; Bies, R.R.; Gharabawi, G. Anticholinergic Activity of 107 Medications Commonly Used by Older Adults. J. Am. Geriatr. Soc. 2008, 56, 1333–1341. [Google Scholar] [CrossRef]
- De Graef, J.; Woussen-Colle, M.-C. Influence of the stimulation state of the parietal cells on the inhibitory effect of omeprazole on gastric acid secretion in dogs. Gastroenterology 1986, 91, 333–337. [Google Scholar] [CrossRef]
- Hyman, J. The limitations of using insurance data for research. J. Am. Dent. Assoc. 2015, 146, 283–285. [Google Scholar] [CrossRef] [PubMed]
- Hamzat, H.; Sun, H.; Ford, J.C.; Macleod, J.; Soiza, R.L.; Mangoni, A.A. Inappropriate prescribing of proton pump inhibitors in older patients: Effects of an educational strategy. Drugs Aging 2012, 29, 681–690. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | H2RA | PPI | ||||
|---|---|---|---|---|---|---|
| Users No. (%) | Non-Users No. (%) | p Value | Users No. (%) | Non-Users No. (%) | p Value | |
| No. of subjects | 21,939 | 21,939 | 9348 | 9348 | ||
| Sex | 1.000 | 1.000 | ||||
| Men | 10,770 (49.1) | 10,770 (49.1) | 5537 (59.2) | 5537 (59.2) | ||
| Women | 11,169 (50.9) | 11,169 (50.9) | 3811 (40.8) | 3811 (40.8) | ||
| Age (years) | 1.000 | 1.000 | ||||
| 65–69 | 7726 (35.2) | 7726 (35.2) | 2593 (27.7) | 2593 (27.7) | ||
| 70–79 | 10,822 (49.3) | 10,822 (49.3) | 4657 (49.8) | 4657 (49.8) | ||
| ≥80 | 3391 (15.5) | 3391 (15.5) | 2098 (22.4) | 2098 (22.4) | ||
| Main indications | ||||||
| Gastric ulcer | 4707 (21.5) | 1739 (7.9) | <0.001 | 3504 (37.5) | 737 (7.9) | <0.001 |
| Duodenal ulcer | 2672 (12.2) | 926 (4.2) | <0.001 | 2195 (23.5) | 398 (4.3) | <0.001 |
| GERD | 232 (1.1) | 161 (0.7) | <0.001 | 115 (1.2) | 63 (0.7) | <0.001 |
| Comorbidities | ||||||
| Hypertension | 14,420 (65.7) | 13,296 (60.6) | <0.001 | 6047 (64.7) | 5642 (60.4) | <0.001 |
| Diabetes mellitus | 6134 (28.0) | 5483 (24.9) | <0.001 | 2879 (30.8) | 2547 (27.2) | <0.001 |
| Hyperlipidemia | 3169 (14.4) | 2919 (13.3) | 0.005 | 1215 (13.0) | 1022 (10.9) | <0.001 |
| CAD | 8752 (39.9) | 8139 (37.1) | <0.001 | 3840 (41.1) | 3631 (38.8) | <0.001 |
| Stroke | 8392 (38.3) | 7963 (36.3) | <0.001 | 3901 (41.7) | 3299 (35.3) | <0.001 |
| Depression | 1409 (6.4) | 1167 (5.3) | <0.001 | 590 (6.3) | 507 (5.4) | <0.001 |
| CCI score (Mean ± SD) | 2.26 ± 1.55 | 2.26 ± 1.55 | 1 | 2.33 ± 1.60 | 2.33 ± 1.60 | 1 |
| Co-medications | ||||||
| NSAIDs | 13,085 (59.6) | 11,095 (50.6) | <0.001 | 4519 (48.3) | 3979 (42.6) | <0.001 |
| Anti-hypertensives | 9577 (43.7) | 8248 (37.6) | <0.001 | 3439 (36.8) | 3012 (32.2) | <0.001 |
| Anti-diabetic agents | 5332 (24.3) | 5068 (23.1) | 0.005 | 2736 (29.3) | 2090 (22.4) | <0.001 |
| Statins | 2413 (10.9) | 1842 (8.4) | 0.003 | 919 (9.8) | 798 (8.5) | 0.025 |
| Aspirin | 5166 (23.5) | 4887 (22.3) | 0.002 | 2078 (22.2) | 1578 (16.9) | <0.001 |
| Anti-depressants | 1074 (4.9) | 775 (3.5) | <0.001 | 384 (4.1) | 294 (3.1) | 0.025 |
| No. annual outpatient visits (Mean ± SD) | 27.04 ± 18.78 | 20.87 ± 16.57 | <0.001 | 22.32 ± 18.70 | 20.35 ± 16.68 | <0.001 |
| Exposure to Acid Suppressants | No. of Subjects | Dementia Development | Adjusted HR * (95% CI) | |
|---|---|---|---|---|
| No. of Cases | Incidence Rate (per 1000) | |||
| H2RA non-users | 21,939 | 4265 | 19.69 | 1.00 (Reference) |
| H2RA users | 21,939 | 4743 | 22.71 | 1.84 (1.49–2.20) |
| cDDD (ref: H2RA non-users) | ||||
| Q1 (1–30) | 15,057 | 3116 | 22.11 | 1.69 (1.23–1.86) |
| Q2 (31–180) | 5834 | 1362 | 23.77 | 1.85 (1.46–2.24) |
| Q3 (181–365) | 735 | 175 | 23.63 | 1.82 (1.50–2.36) |
| Q4 (>365) | 313 | 90 | 28.62 | 1.96 (1.63–2.47) |
| ptrend < 0.001 | ||||
| PPIs non-users | 9348 | 1847 | 20.65 | 1.00 (Reference) |
| PPIs users | 9348 | 1873 | 24.28 | 1.42 (1.07–1.84) |
| cDDD (ref: PPI non-users) | ||||
| Q1 (1–30) | 4838 | 799 | 21.13 | 1.09 (0.91–1.37) |
| Q2 (31–180) | 3924 | 904 | 27.34 | 1.59 (1.19–1.89) |
| Q3 (181–365) | 438 | 119 | 30.54 | 1.82 (1.22–2.13) |
| Q4 (>365) | 148 | 51 | 38.44 | 2.02 (1.43–2.31) |
| ptrend < 0.001 | ||||
| Use of Acid Suppressants | No. of Subjects | Dementia Development | Adjusted HR * (95% CI) | |
|---|---|---|---|---|
| No. of Cases (%) | Incidence Rate (per 1000) | |||
| PPI users | ||||
| H2RA non-users | 9036 | 1662 (18.4) | 21.40 | 1.00 (Reference) |
| H2RA users | 4994 | 865 (17.3) | 17.56 | 0.92 (0.85–1.06) |
| PPI non-users | ||||
| H2RA non-users | 23,277 | 4570 (19.6) | 19.99 | 1.00 (Reference) |
| H2RA users | 15,534 | 3531 (22.7) | 23.97 | 1.86 (1.37–2.02) |
| H2RA users | ||||
| PPI non-users | 15,534 | 3531 (22.7) | 23.97 | 1.00 (Reference) |
| PPI users | 4994 | 865 (17.3) | 17.56 | 0.76 (0.61–1.83) |
| H2RA non-users | ||||
| PPI non-users | 23,277 | 4570 (19.6) | 19.99 | 1.00 (Reference) |
| PPI users | 9036 | 1662 (18.4) | 21.40 | 1.23 (1.08–2.59) |
| Acid Suppressant Combination Use | No. of Subjects | Dementia Development | Adjusted HR * (95% CI) | |
|---|---|---|---|---|
| No. of Cases | Incidence Rate (per 1000) | |||
| Neither | 23,277 | 4570 | 19.99 | 1.00 (Reference) |
| H2RA only | 15,534 | 3531 | 23.97 | 1.85 (1.26–2.16) |
| PPI only | 9036 | 1662 | 21.40 | 1.64 (1.14–1.92) |
| Concurrent use | 4994 | 865 | 20.57 | 1.23 (1.07–1.98) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, L.-Y.; Lin, H.-J.; Wu, W.-T.; Chen, Y.-C.; Chen, C.-L.; Kao, J.; You, S.-L.; Chou, Y.-C.; Sun, C.-A. Clinical Use of Acid Suppressants and Risk of Dementia in the Elderly: A Pharmaco-Epidemiological Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 8271. https://doi.org/10.3390/ijerph17218271
Chen L-Y, Lin H-J, Wu W-T, Chen Y-C, Chen C-L, Kao J, You S-L, Chou Y-C, Sun C-A. Clinical Use of Acid Suppressants and Risk of Dementia in the Elderly: A Pharmaco-Epidemiological Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(21):8271. https://doi.org/10.3390/ijerph17218271
Chicago/Turabian StyleChen, Liang-Yu, Huey-Juan Lin, Wen-Tung Wu, Yong-Chen Chen, Cheng-Li Chen, Jing Kao, San-Lin You, Yu-Ching Chou, and Chien-An Sun. 2020. "Clinical Use of Acid Suppressants and Risk of Dementia in the Elderly: A Pharmaco-Epidemiological Cohort Study" International Journal of Environmental Research and Public Health 17, no. 21: 8271. https://doi.org/10.3390/ijerph17218271
APA StyleChen, L.-Y., Lin, H.-J., Wu, W.-T., Chen, Y.-C., Chen, C.-L., Kao, J., You, S.-L., Chou, Y.-C., & Sun, C.-A. (2020). Clinical Use of Acid Suppressants and Risk of Dementia in the Elderly: A Pharmaco-Epidemiological Cohort Study. International Journal of Environmental Research and Public Health, 17(21), 8271. https://doi.org/10.3390/ijerph17218271