Role of qSOFA and SOFA Scoring Systems for Predicting In-Hospital Risk of Deterioration in the Emergency Department

 ,
,  , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Setting
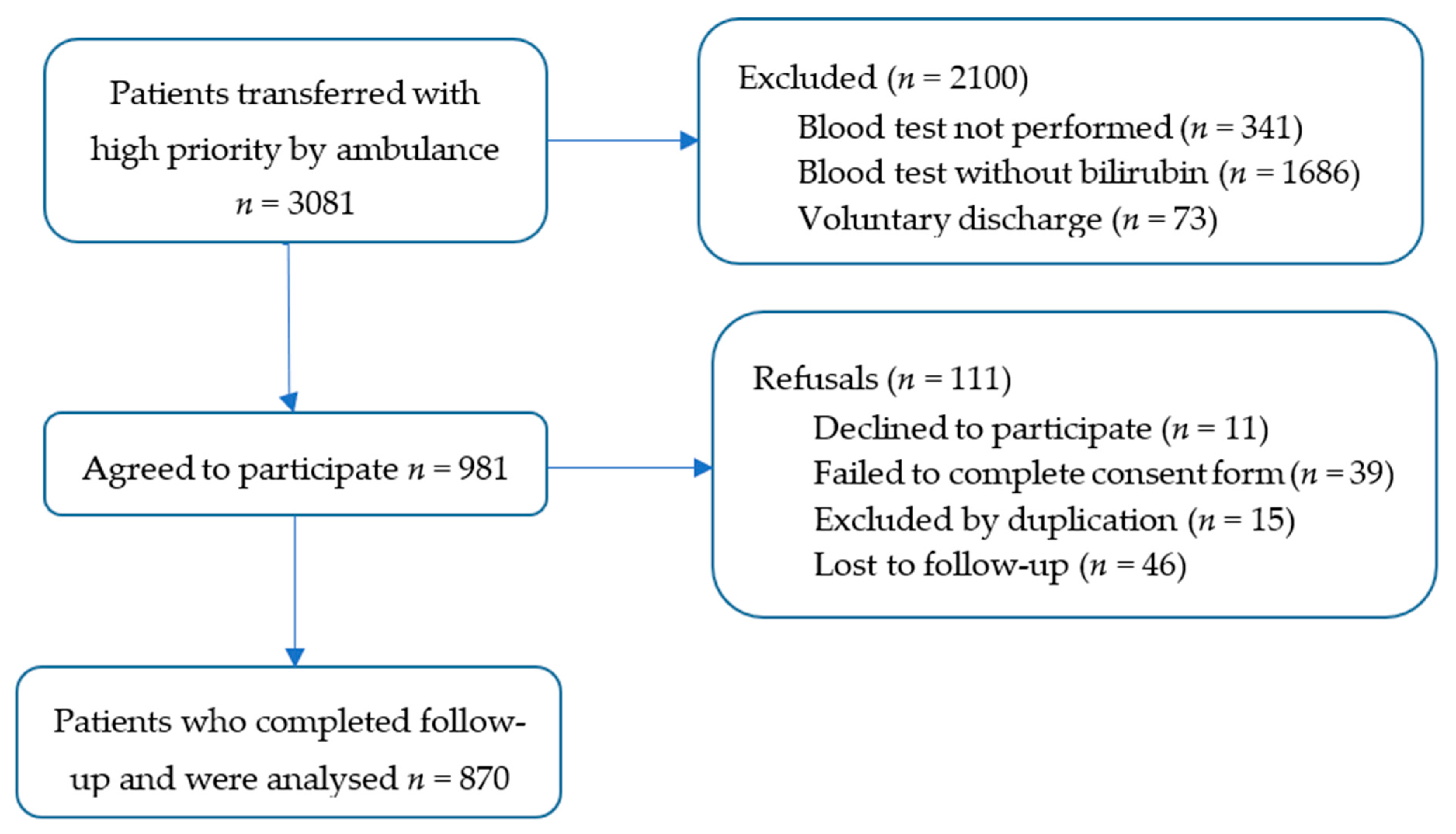
2.2. Population
2.3. Study Protocol and Data Abstraction
2.4. Data Analysis
3. Results
3.1. Patient Baseline
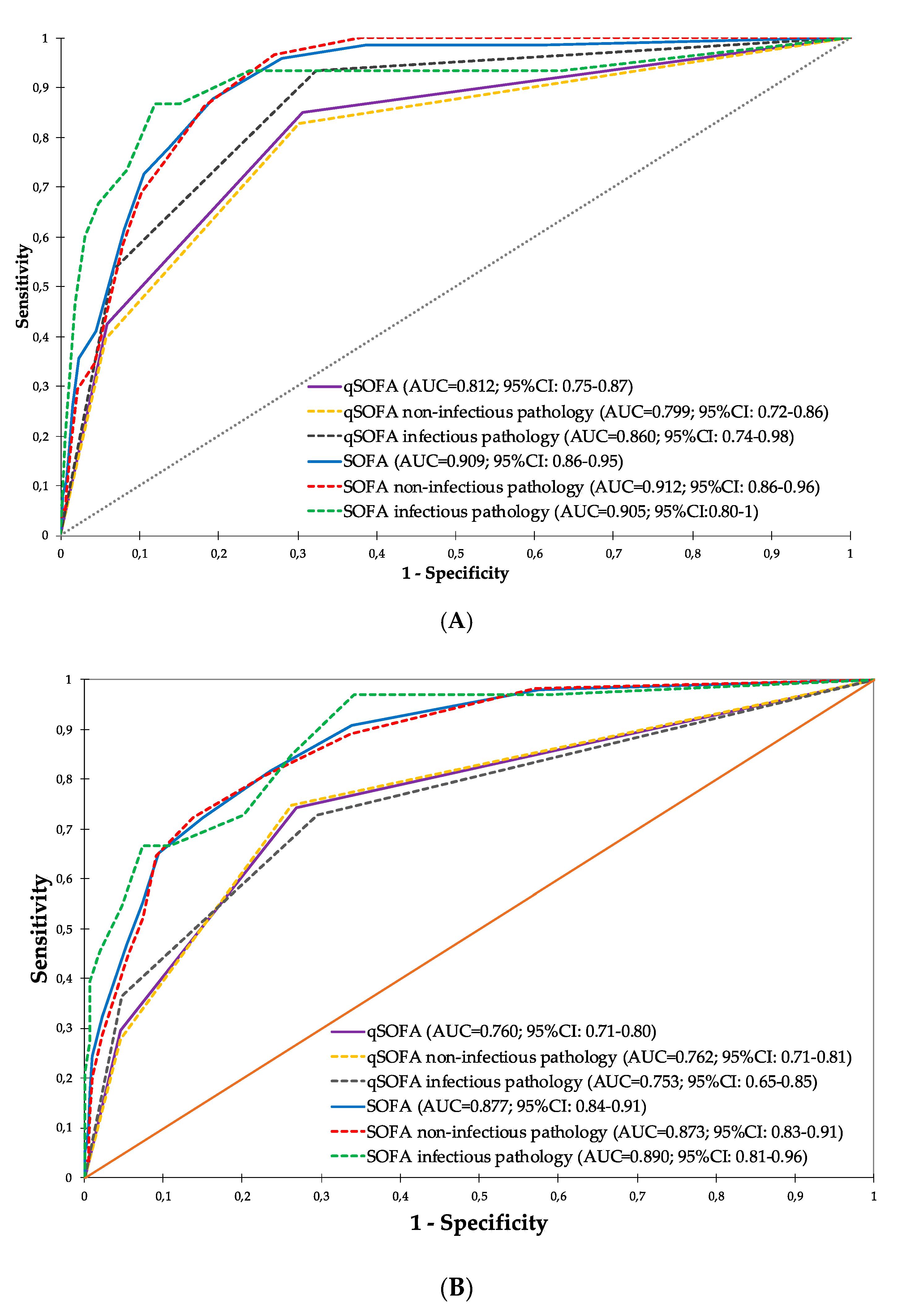
3.2. Prognostic Accuracy of the Scores
3.3. Cut-Off Points for qSOFA and SOFA
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siddiqui, S.; Chua, M.; Kumaresh, V.; Choo, R. A comparison of pre ICU admission SIRS, EWS and q SOFA scores for predicting mortality and length of stay in ICU. J. Crit. Care 2017, 41, 191–193. [Google Scholar] [CrossRef]
- Rahmatinejad, Z.; Tohidinezhad, F.; Reihani, H.; Rahmatinejad, F.; Pourmand, A.; Abu-Hanna, A.; Eslami, S. Prognostic utilization of models based on the APACHE II, APACHE IV, and SAPS II scores for predicting in-hospital mortality in emergency department. Am. J. Emerg. Med. 2020, 38, 1841–1846. [Google Scholar] [CrossRef]
- Lambden, S.; Laterre, P.F.; Levy, M.M.; François, B. The SOFA score—Development, utility and challenges of accurate assessment in clinical trials. Crit. Care 2019, 23, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raith, E.P.; Udy, A.A.; Bailey, M.; McGloughlin, S.; MacIsaac, C.; Bellomo, R.; Pilcher, D.V.; Australian and New Zealand Intensive Care Society (ANZICS); Centre for Outcomes and Resource Evaluation (CORE). Prognostic Accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for In-Hospital Mortality Among Adults With Suspected Infection Admitted to the Intensive Care Unit. JAMA 2017, 317, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Langlais, E.; Nesseler, N.; Le Pabic, E.; Frasca, D.; Launey, Y.; Seguin, P. Does the clinical frailty score improve the accuracy of the SOFA score in predicting hospital mortality in elderly critically ill patients? A prospective observational study. J. Crit. Care 2018, 46, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Serafim, R.; Gomes, J.A.; Salluh, J.; Póvoa, P. A Comparison of the Quick-SOFA and Systemic Inflammatory Response Syndrome Criteria for the Diagnosis of Sepsis and Prediction of Mortality. Chest 2018, 153, 646–655. [Google Scholar] [CrossRef]
- Seymour, C.W.; Liu, V.X.; Iwashyna, T.J.; Brunkhorst, F.M.; Rea, T.D.; Scherag, A.; Rubenfeld, G.; Kahn, J.M.; Shankar-Hari, M.; Singer, M.; et al. Assessment of Clinical Criteria for Sepsis. JAMA 2016, 315, 762–774. [Google Scholar] [CrossRef] [Green Version]
- Shankar-Hari, M.; Phillips, G.S.; Levy, M.L.; Seymour, C.W.; Liu, V.X.; Deutschman, C.S.; Angus, D.C.; Rubenfeld, G.D.; Singer, M.; Force, F.T.S.D.T. Developing a New Definition and Assessing New Clinical Criteria for Septic Shock. JAMA 2016, 315, 775–787. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.C.; Shankar-Hari, M.M.; Annane, D.; Bauer, M.M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.J.; Coopersmith, C.C.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- De Grooth, H.J.H.; Geenen, I.I.; Girbes, A.R.J.A.; Vincent, J.-L.; Parienti, J.J.J.; Straaten, H.M.H.H.O.-V. SOFA and mortality endpoints in randomized controlled trials: a systematic review and meta-regression analysis. Crit. Care 2017, 21, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Klimpel, J.; Weidhase, L.; Bernhard, M.; Gries, A.; Petros, S. The impact of the Sepsis-3 definition on ICU admission of patients with infection. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 98. [Google Scholar] [CrossRef] [PubMed]
- Khwannimit, B.; Bhurayanontachai, R.; Vattanavanit, V. Comparison of the performance of SOFA, qSOFA and SIRS for predicting mortality and organ failure among sepsis patients admitted to the intensive care unit in a middle-income country. J. Crit. Care 2018, 44, 156–160. [Google Scholar] [CrossRef] [PubMed]
- García-Gigorro, R.; La Fuente, I.S.-D.; Mateos, H.M.; Andrés-Esteban, E.M.; Sanchez-Izquierdo, J.A.; Montejo-González, J.C. Utility of SOFA and Δ-SOFA scores for predicting outcome in critically ill patients from the emergency department. Eur. J. Emerg. Med. 2018, 25, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Rahmatinejad, Z.; Reihani, H.; Tohidinezhad, F.; Rahmatinejad, F.; Peyravi, S.; Pourmand, A.; Abu-Hanna, A.; Eslami, S. Predictive performance of the SOFA and mSOFA scoring systems for predicting in-hospital mortality in the emergency department. Am. J. Emerg. Med. 2019, 37, 1237–1241. [Google Scholar] [CrossRef] [PubMed]
- Askim, Å.; Moser, F.; Gustad, L.T.; Stene, H.; Gundersen, M.; Åsvold, B.O.; Dale, J.; Bjørnsen, L.P.; Damås, J.K.; Solligård, E. Poor performance of quick-SOFA (qSOFA) score in predicting severe sepsis and mortality—A prospective study of patients admitted with infection to the emergency department. Scand. J. Trauma Resusc. Emerg. Med. 2017, 25, 1–9. [Google Scholar] [CrossRef]
- Ortega, R.N.; Rosin, C.; Bingisser, R.; Nickel, C.H. Clinical Scores and Formal Triage for Screening of Sepsis and Adverse Outcomes on Arrival in an Emergency Department All-Comer Cohort. J. Emerg. Med. 2019, 57, 453–460.e2. [Google Scholar] [CrossRef]
- Zhang, Y.; Luo, H.; Wang, H.; Zheng, Z.; Ooi, O.C. Validation of prognostic accuracy of the SOFA score, SIRS criteria, and qSOFA score for in-hospital mortality among cardiac-, thoracic-, and vascular-surgery patients admitted to a cardiothoracic intensive care unit. J. Card. Surg. 2019, 35, 118–127. [Google Scholar] [CrossRef]
- Singer, A.J.; Ng, J.; Thode, H.C.; Spiegel, R.; Weingart, S. Quick SOFA Scores Predict Mortality in Adult Emergency Department Patients With and Without Suspected Infection. Ann. Emerg. Med. 2017, 69, 475–479. [Google Scholar] [CrossRef] [Green Version]
- Prasad, A.; Thode, H.C.; Singer, A.J. Predictive value of quick SOFA and revised Baux scores in burn patients. Burns 2020, 46, 347–351. [Google Scholar] [CrossRef]
- Falcão, A.L.E.; Barros, A.G.D.A.; Bezerra, A.A.M.; Ferreira, N.L.; Logato, C.M.; Silva, F.P.; Monte, A.B.F.O.D.; Tonella, R.M.; De Figueiredo, L.C.; Moreno, R.; et al. The prognostic accuracy evaluation of SAPS 3, SOFA and APACHE II scores for mortality prediction in the surgical ICU: An external validation study and decision-making analysis. Ann. Intensive Care 2019, 9, 1–10. [Google Scholar] [CrossRef]
- Buhler, H.; Stanley, A.; Hobbs, B.; Kornelsen, J.; Lamont, S.; Kaus, R.; Grant, K.; Grzybowski, S. Standardised early warning scores in rural interfacility transfers: A pilot study into their potential as a decision-making aid. Can. J. Rural. Med. 2019, 24, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Hung, S.-K.; Ng, C.-J.; Kuo, C.-F.; Goh, Z.N.L.; Huang, L.-H.; Li, C.-H.; Chan, Y.-L.; Weng, Y.-M.; Seak, J.C.-Y.; Seak, C.-J. Comparison of the Mortality in Emergency Department Sepsis Score, Modified Early Warning Score, Rapid Emergency Medicine Score and Rapid Acute Physiology Score for predicting the outcomes of adult splenic abscess patients in the emergency department. PLoS ONE 2017, 12, e0187495. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.E.; Trzeciak, S.; Kline, J.A. The Sequential Organ Failure Assessment score for predicting outcome in patients with severe sepsis and evidence of hypoperfusion at the time of emergency department presentation*. Crit. Care Med. 2009, 37, 1649–1654. [Google Scholar] [CrossRef] [Green Version]
- Raymond, N.J.; Nguyen, M.; Allmark, S.; Woods, L.; Peckler, B. Modified Sequential Organ Failure Assessment sepsis score in an emergency department setting: Retrospective assessment of prognostic value. Emerg. Med. Australas. 2019, 31, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Bossuyt, P.M.; Reitsma, J.B.; Bruns, D.E.; Gatsonis, C.A.; Glasziou, P.P.; Irwig, L.; Lijmer, J.G.; Moher, D.; Rennie, D.; de Vet, H.C.W.; et al. STARD 2015: An updated list of essential items for reporting diagnostic accuracy studies. BMJ 2015, 351, h5527. [Google Scholar] [CrossRef] [Green Version]
- Falsetti, L.; Martino, M.; Zaccone, V.; Viticchi, G.; Raponi, A.; Moroncini, G.; Fioranelli, A.; Di Pentima, C.; Martini, A.; Nitti, C.; et al. SOFA and qSOFA usefulness for in-hospital death prediction of elderly patients admitted for suspected infection in internal medicine. Infection 2020, 1–9. [Google Scholar] [CrossRef]
- Safari, S.; Shojaee, M.; Rahmati, F.; Barartloo, A.; Hahshemi, B.; Forouzanfar, M.M.; Mohammadi, E. Accuracy of SOFA score in prediction of 30-day outcome of critically ill patients. Turk. J. Emerg. Med. 2016, 16, 146–150. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.-Y.; Chen, Y.-X.; Guo, S.-B.; Mei, X.; Yang, P. Predictive performance of quick Sepsis-related Organ Failure Assessment for mortality and ICU admission in patients with infection at the ED. Am. J. Emerg. Med. 2016, 34, 1788–1793. [Google Scholar] [CrossRef]
- Flaatten, H.; De Lange, D.W.; Morandi, A.; Andersen, F.H.; Artigas, A.; Bertolini, G.; Boumendil, A.; Cecconi, M.; Christensen, S.; Faraldi, L.; et al. The impact of frailty on ICU and 30-day mortality and the level of care in very elderly patients (≥80 years). Intensive Care Med. 2017, 43, 1820–1828. [Google Scholar] [CrossRef]
- Innocenti, F.; Tozzi, C.; Donnini, C.; De Villa, E.; Conti, A.; Zanobetti, M.; Pini, R. SOFA score in septic patients: incremental prognostic value over age, comorbidities, and parameters of sepsis severity. Intern. Emerg. Med. 2017, 13, 405–412. [Google Scholar] [CrossRef] [Green Version]
- Zhou, H.; Lan, T.; Guo, S. Stratified and prognostic value of admission lactate and severity scores in patients with community-acquired pneumonia in emergency department. Medicine 2019, 98, e17479. [Google Scholar] [CrossRef] [PubMed]
- Martín-Rodríguez, F.; Castro-Villamor, M.A.; Vegas, C.D.P.; Martín-Conty, J.L.; Mayo-Iscar, A.; Benito, J.F.D.; Ibañez, P.D.B.; Arnillas-Gómez, P.; Escudero-Cuadrillero, C.; López-Izquierdo, R. Analysis of the early warning score to detect critical or high-risk patients in the prehospital setting. Intern. Emerg. Med. 2019, 14, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Probst, M.A.; Gibson, T.; Weiss, R.E.; Yagapen, A.N.; Malveau, S.E.; Adler, D.H.; Bastani, A.; Baugh, C.W.; Caterino, J.M.; Clark, C.L.; et al. Risk Stratification of Older Adults Who Present to the Emergency Department With Syncope: The FAINT Score. Ann. Emerg. Med. 2020, 75, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Gaini, S.; Relster, M.M.; Pedersen, C.; Johansen, I.S. Prediction of 28-days mortality with sequential organ failure assessment (SOFA), quick SOFA (qSOFA) and systemic inflammatory response syndrome (SIRS)—A retrospective study of medical patients with acute infectious disease. Int. J. Infect. Dis. 2018, 78, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guirgis, F.W.; Brakenridge, S.; Sutchu, S.; Khadpe, J.D.; Robinson, T.; Westenbarger, R.; Topp, S.T.; Kalynych, C.J.; Reynolds, J.; Dodani, S.; et al. The long-term burden of severe sepsis and septic shock. J. Trauma Acute Care Surg. 2016, 81, 525–532. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Criteria | Points |
|---|---|
| Respiratory rate ≥ 22/minute | 1 |
| Systolic blood pressure ≤ 100 mmHg | 1 |
| Change in mental status (GCS < 15 points) | 1 |
| Variables | 0 | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|
| Respiratory | PaO2/FiO2 > 400 SpO2/FiO2 > 302 | PaO2/FiO2 < 400 SpO2/FiO2 < 302 | PaO2/FiO2 < 300 SpO2/FiO2 < 221 | PaO2/FiO2 < 200 SpO2/FiO2 < 142 | PaO2/FiO2 < 100 SpO2/FiO2 < 67 |
| Cardiovascular (doses in mcg/kg/min) | MAP ≥ 70 mmHg | MAP < 70 mmHg | Dopamine ≤ 5 or any Dobutamine | Dopamine > 5 Norepinephrine ≤ 0.1 | Dopamine > 15 Norepinephrine > 0.1 |
| Liver, bilirubin (mg/dL) | <1.2 | 1.2–1.9 | 2–5.9 | 6–11.9 | >12 |
| Renal, creatinine (mg/dL) | <1.2 | 1.2–1.9 | 2.0–3.4 | 3.5–4.9 | >5.0 |
| Coagulation (platelets × 103/mm3) | ≥150 | <150 | <100 | <50 | <20 |
| Neurologic (GCS, points) | 15 | 13–14 | 10–12 | 6–9 | <6 |
| Characteristic 1 | Total | 2-Days Mortality | p-Value | 30-Days Mortality | p-Value |
|---|---|---|---|---|---|
| Number [n (%)] | 870 (100) | 73 (8.3) | 152 (17.5) | ||
| Age (years) 2 | 70 (54–81) | 73 (62–82) | 0.007 | 73 (61–84) | <0.001 |
| Female 3 | 338 (38.8) | 26 (35.6) | 0.554 | 57 (37.5) | 0.707 |
| Quick sequential organ failure assessment score | |||||
| Breathing rate (bpm) 2 | 15 (12–19) | 17 (14–23) | 0.055 | 15 (13–20) | 0.362 |
| SAP (mmHg) 2 | 125 (109–144) | 116 (104–133) | 0.007 | 121 (107–140) | 0.107 |
| GCS (points) 2 | 15 (14–15) | 15 (13–15) | 0.970 | 15 (14–15) | 0.921 |
| qSOFA (points) 2 | 1 (1–2) | 2 (2–3) | <0.001 | 2 (1–3) | <0.001 |
| Sequential organ failure assessment score | |||||
| SpO2/FiO2 ratio 2 | 443 (266–462) | 443 (250–462) | 0.771 | 443 (279–462) | 0.843 |
| MAP (mmHg) 2 | 89 (78–101) | 82 (73–92) | <0.001 | 84 (76–98) | 0.094 |
| Inotropic agents 3 | 47 (5.4) | 4 (5.5) | 0.976 | 10 (6.6) | 0.481 |
| Bilirubin (mg/dL) 2 | 0.55 (0.38–0.85) | 0.97 (0.80–1.12) | 0.014 | 0.56 (0.43–0.82) | 0.065 |
| Creatinine (mg/dL) 2 | 0.99 (0.79–1.34) | 0.97 (0.80–1.12) | 0.046 | 0.99 (0.82–1.30) | 0.084 |
| Platelets (103/mm3) 2 | 212 (166–269) | 235 (183–285) | 0.120 | 211 (177–264) | 0.739 |
| SOFA (points) 2 | 1 (1–4) | 7 (5–10) | <0.001 | 6 (3–8) | <0.001 |
| Hospital outcomes | |||||
| Inpatients 3 | 590 (67.7) | 73 (100) | 0.003 | 152 (100) | 0.008 |
| ICU admissions 3 | 214 (24.6) | 32 (43.8) | <0.001 | 54 (35.5) | 0.001 |
| Infectious pathology 3 | 182 (20.9) | 23 (31.5) | <0.001 | 47 (30.9) | <0.001 |
| Non-infectious pathology 3 | 688 (79.0) | 50 (68.5) | 0.020 | 105 (69.1) | 0.001 |
| Scores | Statistics | All Patients 1 | Non-Infectious Pathology 1 | Infectious Pathology 1 |
|---|---|---|---|---|
| Prevalence | 0.084 | 0.084 | 0.082 | |
| qSOFA | Cut-off | 2 | 2 | 2 |
| Se | 84.9 (75.0–91.4) | 82.8 (71.1–90.4) | 93.3 (70.2–98.8) | |
| Sp% | 69.4 (66.1–72.5) | 69.8 (66.1–73.3) | 67.7 (60.2–74.3) | |
| PPV | 20.3 (16.1–25.1) | 20.2 (15.6–25.7) | 20.6 (12.7–31.6) | |
| NPV | 98.0 (96.5–98.9) | 97.8 (96.0–98.8) | 99.1 (95.2–99.8) | |
| LR(+) | 2.77 (2.41–3.20) | 2.74 (2.32–3.24) | 2.89 (2.23–3.74) | |
| LR(−) | 0.22 (0.13–0.38) | 0.25 (0.14–0.44) | 0.10 (0.01–0.66) | |
| OR | 12.77 (6.61–24.68) | 11.12 (5.51–22.43) | 29.30 (3.75–228.61) | |
| DA | 70.7 (67.6–73.6) | 70.9 (67.4–74.2) | 69.8 (62.8–76.0) | |
| SOFA | Cut-off | 4 | 3 | 6 |
| Se | 87.7 (78.2–93.4) | 96.6 (88.3–99.0) | 86.7 (62.1–96.3) | |
| Sp% | 80.7 (77.4–83.3) | 73.0 (69.4–76.3) | 88.0 (82.2–92.1) | |
| PPV | 29.4 (23.7–35.7) | 24.8 (19.6–30.8) | 39.4 (24.7–56.3) | |
| NPV | 98.6 (97.4–99.3) | 99.6 (98.4–99.9) | 98.7 (95.2–99.6) | |
| LR(+) | 4.54 (3.84–5.36) | 3.58 (3.12–4.10) | 7.24 (4.58–11.42) | |
| LR(−) | 0.15 (0.08–0.28) | 0.05 (0.01–0.18) | 0.15 (0.04–0.55) | |
| OR | 29.69 (14.46–60.97) | 75.76 (18.29–313.88) | 47.78 (10.04–227.42) | |
| DA | 81.3 (78.5–83.7) | 75.0 (71.6–78.1) | 87.9 (82.4–91.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Izquierdo, R.; Brio-Ibañez, P.d.; Martín-Rodríguez, F.; Mohedano-Moriano, A.; Polonio-López, B.; Maestre-Miquel, C.; Viñuela, A.; Durantez-Fernández, C.; Villamor, M.Á.C.; Martín-Conty, J.L. Role of qSOFA and SOFA Scoring Systems for Predicting In-Hospital Risk of Deterioration in the Emergency Department. Int. J. Environ. Res. Public Health 2020, 17, 8367. https://doi.org/10.3390/ijerph17228367
López-Izquierdo R, Brio-Ibañez Pd, Martín-Rodríguez F, Mohedano-Moriano A, Polonio-López B, Maestre-Miquel C, Viñuela A, Durantez-Fernández C, Villamor MÁC, Martín-Conty JL. Role of qSOFA and SOFA Scoring Systems for Predicting In-Hospital Risk of Deterioration in the Emergency Department. International Journal of Environmental Research and Public Health. 2020; 17(22):8367. https://doi.org/10.3390/ijerph17228367
Chicago/Turabian StyleLópez-Izquierdo, Raúl, Pablo del Brio-Ibañez, Francisco Martín-Rodríguez, Alicia Mohedano-Moriano, Begoña Polonio-López, Clara Maestre-Miquel, Antonio Viñuela, Carlos Durantez-Fernández, Miguel Á. Castro Villamor, and José L. Martín-Conty. 2020. "Role of qSOFA and SOFA Scoring Systems for Predicting In-Hospital Risk of Deterioration in the Emergency Department" International Journal of Environmental Research and Public Health 17, no. 22: 8367. https://doi.org/10.3390/ijerph17228367
APA StyleLópez-Izquierdo, R., Brio-Ibañez, P. d., Martín-Rodríguez, F., Mohedano-Moriano, A., Polonio-López, B., Maestre-Miquel, C., Viñuela, A., Durantez-Fernández, C., Villamor, M. Á. C., & Martín-Conty, J. L. (2020). Role of qSOFA and SOFA Scoring Systems for Predicting In-Hospital Risk of Deterioration in the Emergency Department. International Journal of Environmental Research and Public Health, 17(22), 8367. https://doi.org/10.3390/ijerph17228367