Epidemiology of Rotavirus Gastroenteritis and Rotavirus-Associated Benign Convulsions with Mild Gastroenteritis after the Introduction of Rotavirus Vaccines in South Korea: Nationwide Data from the Health Insurance Review and Assessment Service


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Study Population
2.3. Demographics and Annual Prevalence of RVGE and RaCwG
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Patients with RVGE, Patients with RaCwG, and the MYP
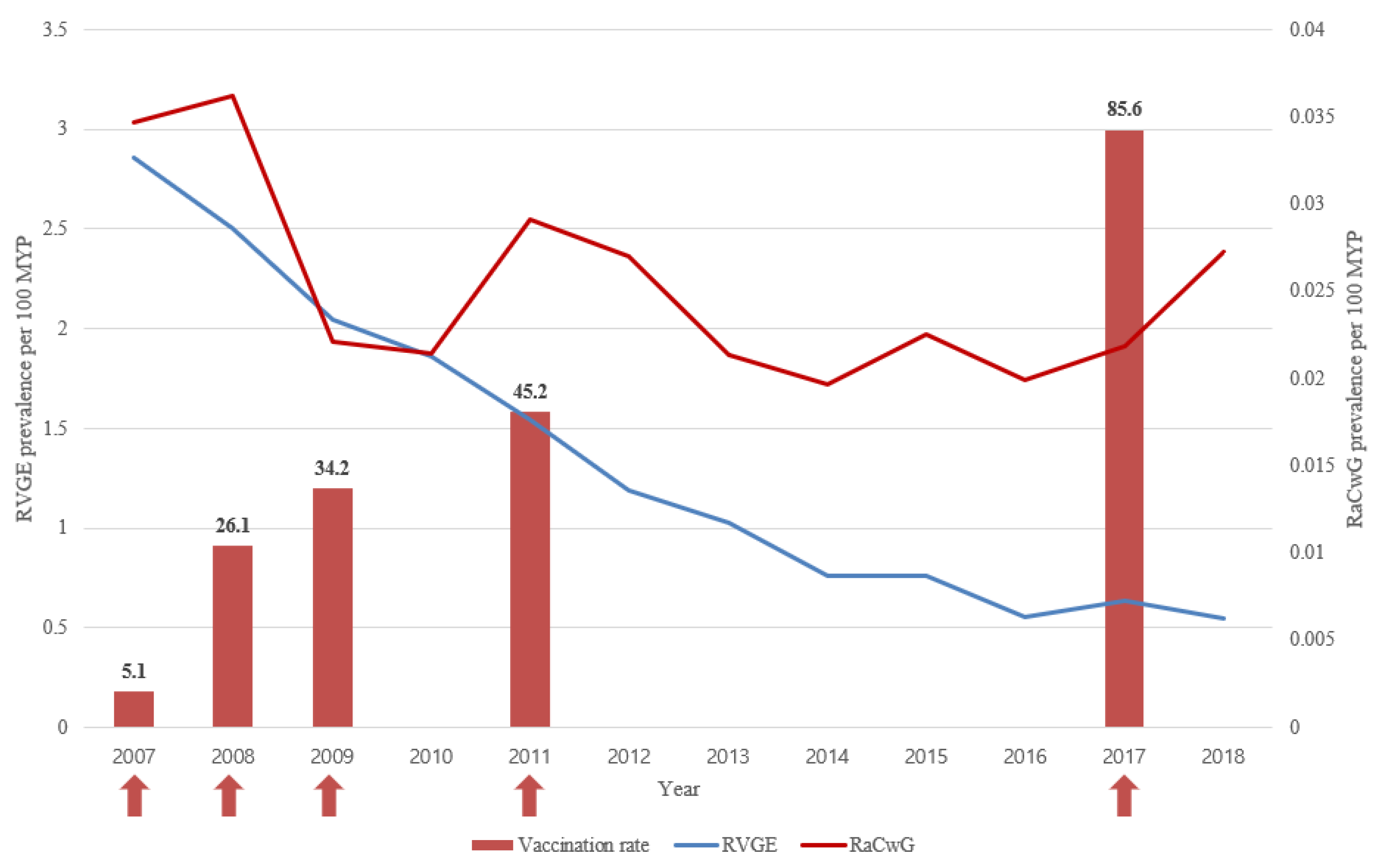
3.2. Annual Prevalence of RVGE, Annual Prevalence of RaCwG, and Ratio of RaCwG to RVGE
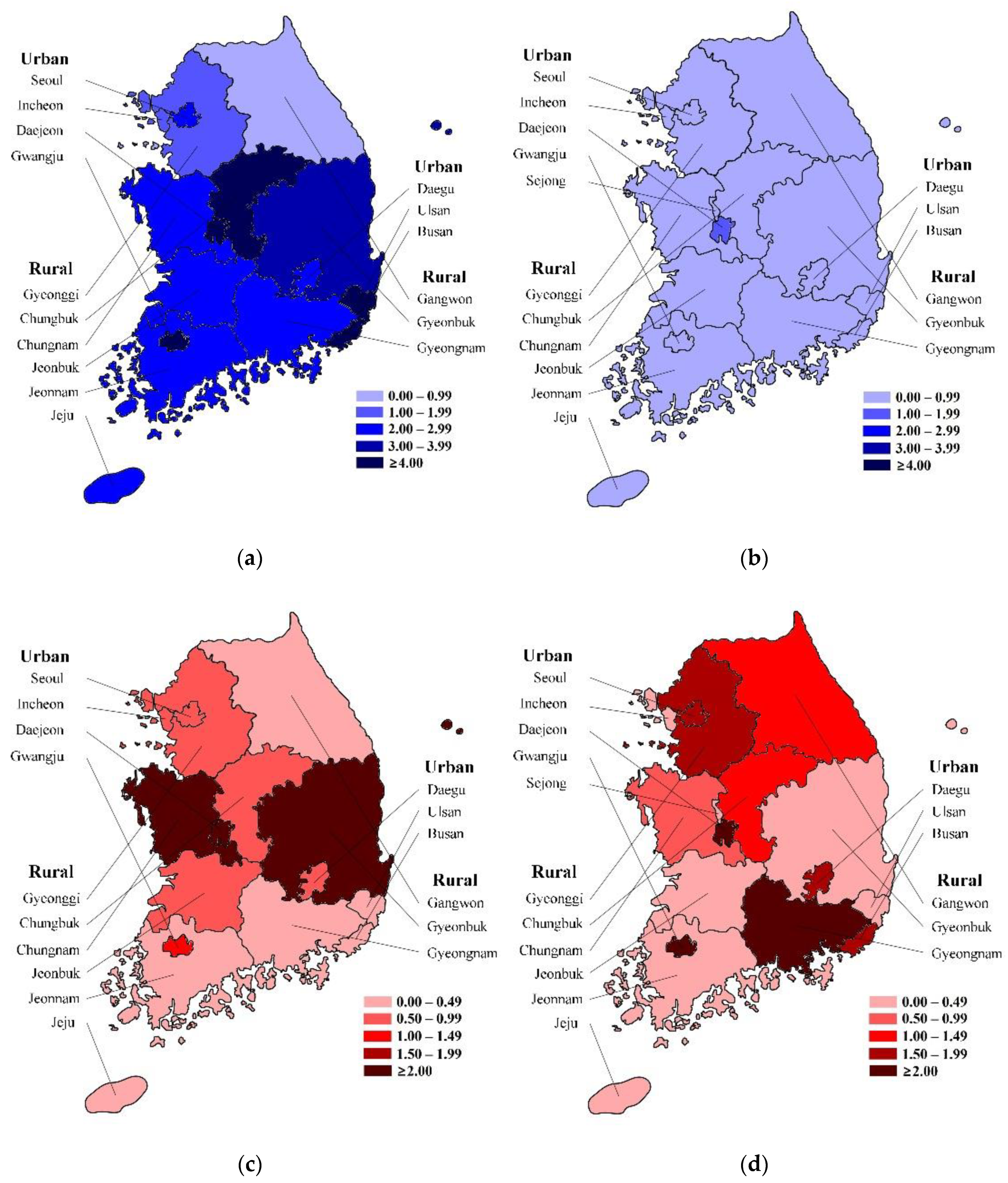
3.3. Associated Factors with RVGE and RaCwG
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Abubakar, I.I.; Tillmann, T.; Banerjee, A. Global Burden of Disease 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [Google Scholar]
- Lanata, C.F.; Fischer-Walker, C.L.; Olascoaga, A.C.; Torres, C.X.; Aryee, M.J.; Black, R.E. Child Health Epidemiology Reference Group of the World Health Organization and UNICEF. Global causes of diarrheal disease mortality in children <5 years of age: A systematic review. PLoS ONE 2013, 8, e72788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tate, J.E.; Burton, A.H.; Boschi-Pinto, C.; Parashar, U.D. World Health Organization-Coordinated Global Rotavirus Surveillance Network. Global, regional, and national estimates of rotavirus mortality in children <5 years of age, 2000–2013. Clin. Infect. Dis. 2016, 62, S96–S105. [Google Scholar] [CrossRef] [Green Version]
- Tate, J.E.; Burton, A.H.; Boschi-Pinto, C.; Steele, A.D.; Duque, J.; Parashar, U.D. WHO-coordinated Global Rotavirus Surveillance Network. 2008 estimate of worldwide rotavirus-associated mortality in children younger than 5 years before the introduction of universal rotavirus vaccination programmes: A systematic review and meta-analysis. Lancet Infect. Dis. 2012, 12, 136–141. [Google Scholar] [CrossRef] [Green Version]
- Wong, C.J.; Price, Z.; Bruckner, D.A. Aseptic meningitis in an infant with rotavirus gastroenteritis. Pediatr. Infect. Dis. 1984, 3, 244–246. [Google Scholar] [CrossRef]
- Wong, V. Acute gastroenteritis-related encephalopathy. J. Child Neurol. 2001, 16, 906–910. [Google Scholar] [CrossRef]
- Nakagomi, T.; Nakagomi, O. Rotavirus antigenemia in children with encephalopathy accompanied by rotavirus gastroenteritis. Arch. Virol. 2005, 150, 1927–1931. [Google Scholar] [CrossRef]
- Ushijima, H.; Bosu, K.; Abe, T.; Shinozaki, T. Suspected rotavirus encephalitis. Arch. Dis. Child. 1986, 61, 692–694. [Google Scholar] [CrossRef] [Green Version]
- Morooka, K. Convulsions and mild diarrhea. Shonika 1982, 23, 131–137. [Google Scholar]
- Komori, H.; Wada, M.; Eto, M.; Oki, H.; Aida, K.; Fujimoto, T. Benign convulsions with mild gastroenteritis: A report of 10 recent cases detailing clinical varieties. Brain Dev. 1995, 17, 334–337. [Google Scholar] [CrossRef]
- Uemura, N.; Okumura, A.; Negoro, T.; Watanabe, K. Clinical features of benign convulsions with mild gastroenteritis. Brain Dev. 2002, 24, 745–749. [Google Scholar] [CrossRef]
- Okumura, A.; Tanabe, T.; Kato, T.; Hayakawa, F.; Watanabe, K. A pilot study on lidocaine tape therapy for convulsions with mild gastroenteritis. Brain Dev. 2004, 26, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Kawano, G.; Oshige, K.; Syutou, S.; Koteda, Y.; Yokoyama, T.; Kim, B.G.; Mizuochi, T.; Nagai, K.; Matsuda, K.; Ohbu, K.; et al. Benign infantile convulsions associated with mild gastroenteritis: A retrospective study of 39 cases including virological tests and efficacy of anticonvulsants. Brain Dev. 2007, 29, 617–622. [Google Scholar] [CrossRef]
- Tanabe, T.; Okumura, A.; Komatsu, M.; Kubota, T.; Nakajima, M.; Shimakawa, S. Clinical trial of minimal treatment for clustering seizures in cases of convulsions with mild gastroenteritis. Brain Dev. 2011, 33, 120–124. [Google Scholar] [CrossRef] [PubMed]
- Kang, B.; Kwon, Y.S. Benign convulsion with mild gastroenteritis. Korean J. Pediatr. 2014, 57, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Durá-Travé, T.; Yoldi-Petri, M.E.; Gallinas-Victoriano, F.; Molins-Castiella, T. Infantile convulsions with mild gastroenteritis: A retrospective study of 25 patients. Eur. J. Neurol. 2011, 18, 273–278. [Google Scholar] [CrossRef]
- Lloyd, M.B.; Lloyd, J.C.; Gesteland, P.H.; Bale, J.F., Jr. Rotavirus gastroenteritis and seizures in young children. Pediatr. Neurol. 2010, 42, 404–408. [Google Scholar] [CrossRef]
- Junquera, C.G.; de Baranda, C.S.; Mialdea, O.G.; Serrano, E.B.; Sánchez-Fauquier, A. Prevalence and clinical characteristics of norovirus gastroenteritis among hospitalized children in Spain. Pediatr. Infect. Dis. J. 2009, 28, 604–607. [Google Scholar] [CrossRef]
- World Health Organization. Rotavirus vaccines: An update. Wkly Epidemiol. Rec. 2009, 84, 533–540. [Google Scholar]
- Lee, S.G.; Jeon, S.Y.; Park, K.S. Rotavirus vaccine coverage and related factors. J. Korean Soc. Matern. Child Health 2019, 23, 175–184. [Google Scholar] [CrossRef]
- Shim, J.O.; Chang, J.Y.; Shin, S.; Moon, J.S.; Ko, J.S. Changing distribution of age, clinical severity, and genotypes of rotavirus gastroenteritis in hospitalized children after the introduction of vaccination: A single center study in Seoul between 2011 and 2014. BMC Infect. Dis. 2016, 16, 287. [Google Scholar] [CrossRef] [Green Version]
- Park, D.K.; Chung, J.Y. The changes in the outbreak of rotavirus gastroenteritis in children after introduction of rotavirus vaccines: A retrospective study at a tertiary hospital. Korean J. Pediatr. Infect. Dis. 2014, 21, 167–173. [Google Scholar] [CrossRef] [Green Version]
- Payne, D.C.; Boom, J.A.; Staat, M.A.; Edwards, K.M.; Szilagyi, P.G.; Klein, E.J.; Selvarangan, R.; Azimi, R.H.; Harrison, C.; Moffatt, M.; et al. Effectiveness of pentavalent and monovalent rotavirus vaccines in concurrent use among US children <5 years of age, 2009–2011. Clin. Infect. Dis. 2013, 57, 13–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.S. Introduction: Health of the health care system in Korea. Soc. Work Public Health 2010, 25, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Kim, L.; Kim, J.A.; Kim, S. A guide for the utilization of health insurance review and assessment service national patient samples. Epidemiol. Health 2014, 36, e2014008. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.T.; Yoon, J.S.; Speedie, S.M.; Yoon, H.; Lee, J. Health insurance claim review using information technologies. Healthc. Inform. Res. 2012, 18, 215–224. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Rotavirus. In Epidemiology and Prevention of Vaccine-Preventable Diseases, 13th ed.; Hamborsky, J., Kroger, A., Wolfe, S., Eds.; Public Health Foundation: Washington, DC, USA, 2015; pp. 311–322. [Google Scholar]
- Kim, J.S.; Kang, J.O.; Cho, S.C.; Jang, Y.T.; Min, S.A.; Park, T.H.; Nyambat, B.; Jo, D.S.; Gentsch, J.; Bresee, J.S.; et al. Epidemiological profile of rotavirus infection in the Republic of Korea: Results from prospective surveillance in the Jeongeub district, 1 July 2002 through 30 June 2004. J. Infect. Dis. 2005, 192, S49–S56. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.S.; Kim, D.Y.; Kim, J.A.; Choi, S.H. The epidemiological trend of rotavirus gastroenteritis in children in a single center from 2004 to 2012: A retrospective study. Korean J. Pediatr. Infect. Dis. 2014, 21, 181–190. [Google Scholar] [CrossRef]
- Chung, J.Y.; Kim, M.S.; Jung, T.W.; Kim, S.J.; Kang, J.H.; Han, S.B.; Kim, S.Y.; Rhim, J.W.; Kim, H.M.; Park, J.H.; et al. Detection of rotavirus genotypes in Korea 5 years after the introduction of rotavirus vaccines. J. Korean Med. Sci. 2015, 30, 1471–1475. [Google Scholar] [CrossRef] [Green Version]
- Kang, B.; Kim, D.H.; Hong, Y.J.; Son, B.K.; Kim, D.W.; Kwon, Y.S. Comparison between febrile and afebrile seizures associated with mild rotavirus gastroenteritis. Seizure 2013, 22, 560–564. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.J.; Chen, B.S.; Wang, S.F.; Lai, M.H. Rotavirus gastroenteritis in children: A clinical study of 125 patients in Hsin-Tien area. Zhonghua Min Guo Xiao Er Ke I Xue Hui Za Zhi 1991, 32, 73–78. [Google Scholar]
- Chen, S.Y.; Tsai, C.N.; Lai, M.W.; Chen, C.Y.; Lin, K.L.; Lin, T.Y.; Chiu, C.H. Norovirus infection as a cause of diarrhea-associated benign infantile seizures. Clin. Infect. Dis. 2009, 48, 849–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, C.C.; Chang, Y.C.; Wang, S.T. Acute symptomatic seizure disorders in young children—A population study in southern Taiwan. Epilepsia 1998, 39, 960–964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.H.; Kim, Y.O.; Kim, H.K.; Kim, H.S.; Kim, B.Y.; Cheon, K.R.; Kim, M.J.; Kim, S.H.; Chung, J.K.; Woo, Y.J. Incidence of benign convulsions with mild gastroenteritis after introduction of rotavirus vaccine. Brain Dev. 2015, 37, 625–630. [Google Scholar] [CrossRef]
- Yoo, S.Y.; Kim, D.H.; Lee, Y.; Lee, G.H.; Ha, D.J.; Kwon, Y.S. Serum uric acid as a predictive factor for rotaviral or noroviral benign convulsions with mild gastroenteritis. Ann. Child. Neurol. 2020, 28, 138–144. [Google Scholar] [CrossRef]
- Deus, N.; João, E.; Cuamba, A.; Cassocera, M.; Luís, L.; Acácio, S.; Mandomando, I.; Augusto, O.; Page, N. Epidemiology of rotavirus infection in children from a rural and urban area, in Maputo, southern Mozambique, before vaccine introduction. J. Trop. Pediatr. 2018, 64, 141–145. [Google Scholar] [CrossRef]
- Parashar, U.D.; Hummelman, E.G.; Bresee, J.S.; Miler, M.A.; Glass, R.I. Global illness and deaths caused by rotavirus disease in children. Emerg. Infect. Dis. 2003, 9, 565–572. [Google Scholar] [CrossRef]
- Sohn, T.Y.; Lee, C.J.; Kim, Y.J.; Kang, M.J.; Kim, S.H.; Lee, S.Y.; Lee, D.H.; Lee, H.R.; Kim, K.N. Clinical and epidemiological study of 1165 hospitalized cases of rotaviral gastroenteritis before and after the introduction of rotavirus vaccine, 2006–2013. Korean J. Pediatr. Infect. Dis. 2014, 21, 174–180. [Google Scholar] [CrossRef]
- Choi, U.Y.; Lee, S.Y.; Ma, S.H.; Jang, Y.T.; Kim, J.Y.; Kim, H.M.; Kim, J.H.; Kim, D.S.; Kim, Y.S.; Kang, J.H. Epidemiological changes in rotavirus gastroenteritis in children under 5 years of age after the introduction of rotavirus vaccines in Korea. Eur. J. Pediatr. 2013, 172, 947–952. [Google Scholar] [CrossRef]
- Hung, J.J.; Wen, H.Y.; Yen, M.H.; Chen, H.W.; Yan, D.C.; Lin, K.L.; Lin, S.J.; Lin, T.Y.; Hsu, C.Y. Rotavirus gastroenteritis associated with afebrile convulsion in children: Clinical analysis of 40 cases. Chan Gung Med. J. 2003, 26, 654–659. [Google Scholar]
- Velazquez, F.R.; Matson, D.O.; Calva, J.J.; Guerrero, L.; Morrow, A.L.; Carter-Campbell, S.; Glass, R.I.; Estes, M.K.; Pickering, L.K.; Ruiz-Palacios, G.M. Rotavirus infections in infants as protection against subsequent infections. N. Engl. J. Med. 1996, 335, 1022–1028. [Google Scholar] [CrossRef] [PubMed]
- Gladstone, B.P.; Ramani, S.; Mukhopadhya, I.; Muliyil, J.; Sarkar, R.; Rehman, A.M.; Jaffar, S.; Gomara, M.I.; Gray, J.J.; Brown, D.W.G.; et al. Protective effect of natural rotavirus infection in an Indian birth cohort. N. Engl. J. Med. 2011, 365, 337–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, F.E.; Baram, T.Z. Developmental seizures induced by common early-life insults: Short- and long-term effects on seizure susceptibility. Ment. Retard. Dev. Disabil. Res. Rev. 2000, 6, 253–257. [Google Scholar] [CrossRef] [Green Version]
- Jin, H.I.; Lee, Y.M.; Choi, Y.J.; Jeong, S.J. Recent viral pathogen in acute gastroenteritis: A retrospective study at a tertiary hospital for 1 year. Korean J. Pediatr. 2016, 59, 120–125. [Google Scholar] [CrossRef] [Green Version]
- Salim, H.; Karyana, I.P.G.; Sanjaya-Putra, I.G.N.; Budiarsa, S.; Soenarto, Y. Risk factors of rotavirus diarrhea in hospitalized children in Sanglah Hospital, Denpasar: A prospective cohort study. BMC Gastroenterol. 2014, 14, 54. [Google Scholar] [CrossRef] [Green Version]
- The Pediatric ROTavirus European CommitTee. The paediatric burden of rotavirus disease in Europe. Epidemiol. Infect. 2006, 134, 908–916. [Google Scholar] [CrossRef] [PubMed]
- Hsu, V.P.; Staat, M.A.; Roberts, N.; Thieman, C.; Bernstein, D.I.; Bresee, J.; Glass, R.I.; Parashar, U.D. Use of active surveillance to validate international classification of diseases code estimates of rotavirus hospitalizations in children. Pediatrics 2005, 115, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.M.; Jo, D.S.; Kim, Y.H.; Hong, J.M. The societal cost of rotavirus infection in South Korea. Korean J. Pediatr. 2008, 51, 977–986. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | RVGE | RaCwG | MYP |
|---|---|---|---|
| Subjects, number | 219,686 | 4032 | 15,960,271.5 |
| Sex | |||
| Male | 121,110 (55.1) | 2102 (52.1) | 8,209,580.5 (51.4) |
| Female | 98,576 (44.9) | 1930 (47.9) | 7,750,691 (48.6) |
| Age (years), median (IQR) | 1.0 (0.0–1.0) | 0.0 (0.0–1.0) | 1.0 (0.0–2.0) |
| Year | |||
| 2007 | 38,301 (17.4) | 465 (11.5) | 1,340,068 (8.4) |
| 2008 | 34,226 (15.6) | 495 (12.3) | 1,366,555 (8.6) |
| 2009 | 28,213 (12.8) | 305 (7.6) | 1,382,048 (8.7) |
| 2010 | 25,467 (11.6) | 293 (7.3) | 1,369,526.5 (8.6) |
| 2011 | 21,008 (9.6) | 397 (9.8) | 1,362,404 (8.5) |
| 2012 | 16,524 (7.5) | 374 (9.3) | 1,387,208 (8.7) |
| 2013 | 14,285 (6.5) | 298 (7.4) | 1,394,688.5 (8.7) |
| 2014 | 10,349 (4.7) | 268 (6.6) | 1,364,246 (8.5) |
| 2015 | 10,045 (4.6) | 298 (7.4) | 1,324,410 (8.3) |
| 2016 | 7147 (3.3) | 257 (6.4) | 1,288,368 (8.1) |
| 2017 | 7868 (3.6) | 270 (6.7) | 1,236,382.5 (7.7) |
| 2018 | 6253 (2.8) | 312 (7.7) | 1,144,367 (7.2) |
| Variable | RVGE/MYP | RaCwG/MYP | RaCwG/RVGE | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | Exp(B) | 95% CI | p Value | β | Exp(B) | 95% CI | p Value | β | Exp(B) | 95% CI | p Value | |
| Age (≥2 year) | −1.091 | 0.336 | 0.151–0.748 | 0.008 * | −2.125 | 0.119 | 0.053–0.270 | <0.001 * | −1.008 | 0.365 | 0.162–0.821 | 0.015 * |
| Sex (female) | −0.136 | 0.873 | 0.496–1.538 | 0.639 | −0.031 | 0.969 | 0.548–1.715 | 0.915 | 0.100 | 1.105 | 0.624–1.956 | 0.732 |
| Area (rural) | −0.206 | 0.814 | 0.462–1.433 | 0.475 | −1.334 | 0.264 | 0.147–0.473 | <0.001 * | −1.109 | 0.330 | 0.185–0.589 | <0.001 * |
| Year | −0.161 | 0.852 | 0.786–0.923 | <0.001 * | −0.061 | 0.941 | 0.867–1.020 | 0.139 | 0.099 | 1.105 | 1.017–1.199 | 0.018 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.H.; Lee, Y.S.; Ha, D.J.; Chun, M.J.; Kwon, Y.S. Epidemiology of Rotavirus Gastroenteritis and Rotavirus-Associated Benign Convulsions with Mild Gastroenteritis after the Introduction of Rotavirus Vaccines in South Korea: Nationwide Data from the Health Insurance Review and Assessment Service. Int. J. Environ. Res. Public Health 2020, 17, 8374. https://doi.org/10.3390/ijerph17228374
Kim DH, Lee YS, Ha DJ, Chun MJ, Kwon YS. Epidemiology of Rotavirus Gastroenteritis and Rotavirus-Associated Benign Convulsions with Mild Gastroenteritis after the Introduction of Rotavirus Vaccines in South Korea: Nationwide Data from the Health Insurance Review and Assessment Service. International Journal of Environmental Research and Public Health. 2020; 17(22):8374. https://doi.org/10.3390/ijerph17228374
Chicago/Turabian StyleKim, Dong Hyun, Yeong Seok Lee, Dong Jun Ha, Min Jun Chun, and Young Se Kwon. 2020. "Epidemiology of Rotavirus Gastroenteritis and Rotavirus-Associated Benign Convulsions with Mild Gastroenteritis after the Introduction of Rotavirus Vaccines in South Korea: Nationwide Data from the Health Insurance Review and Assessment Service" International Journal of Environmental Research and Public Health 17, no. 22: 8374. https://doi.org/10.3390/ijerph17228374
APA StyleKim, D. H., Lee, Y. S., Ha, D. J., Chun, M. J., & Kwon, Y. S. (2020). Epidemiology of Rotavirus Gastroenteritis and Rotavirus-Associated Benign Convulsions with Mild Gastroenteritis after the Introduction of Rotavirus Vaccines in South Korea: Nationwide Data from the Health Insurance Review and Assessment Service. International Journal of Environmental Research and Public Health, 17(22), 8374. https://doi.org/10.3390/ijerph17228374