Prevalence of Type 2 Diabetes and Its Association with Added Sugar Intake in Citizens and Refugees Aged 40 or Older in the Gaza Strip, Palestine







Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Sampling Approach
2.3. Data Collection
2.4. Outcome Definitions
2.5. Statistical Analysis
3. Results
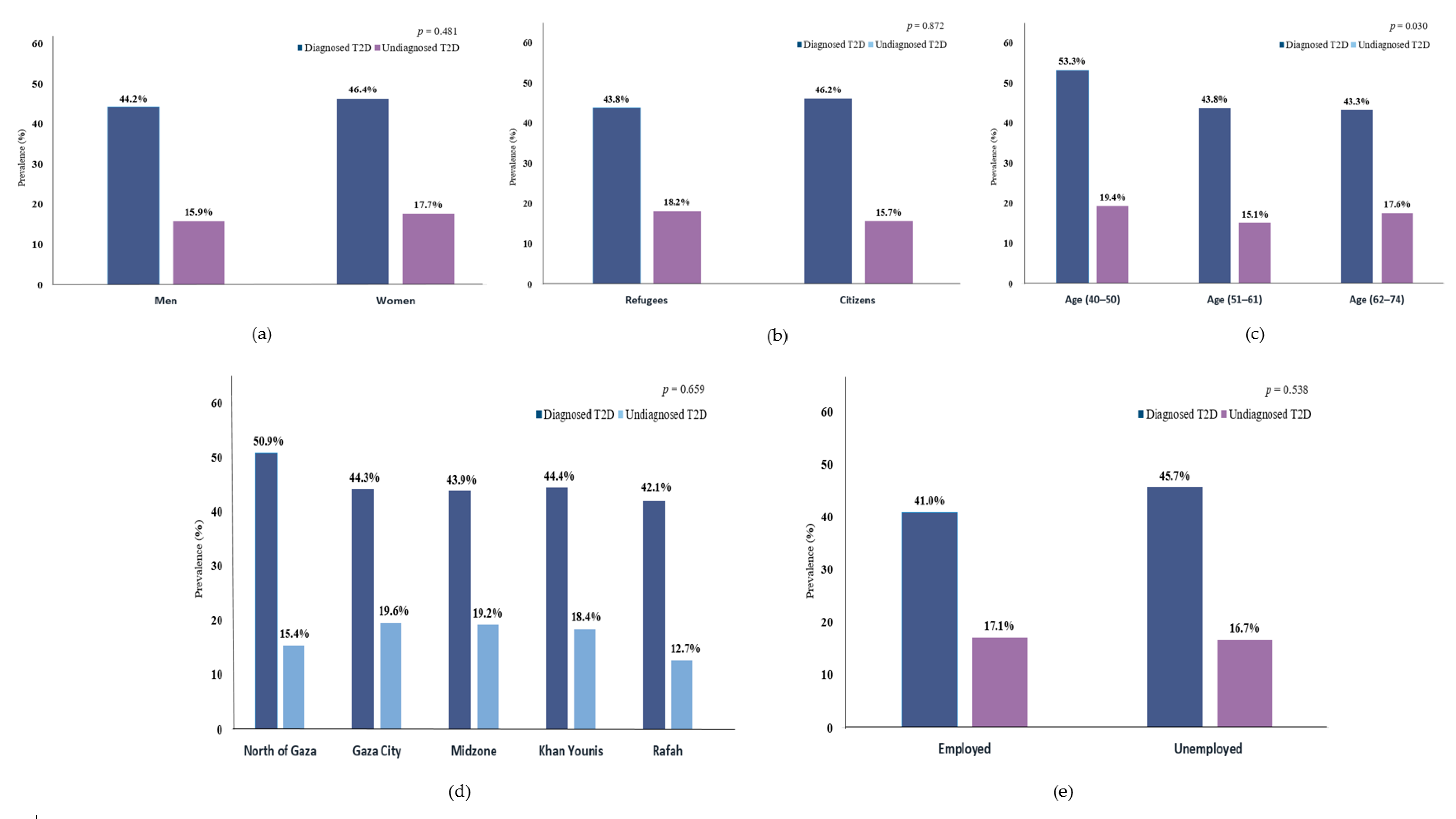
3.1. Prevalence of T2D and Characteristics of the Participants
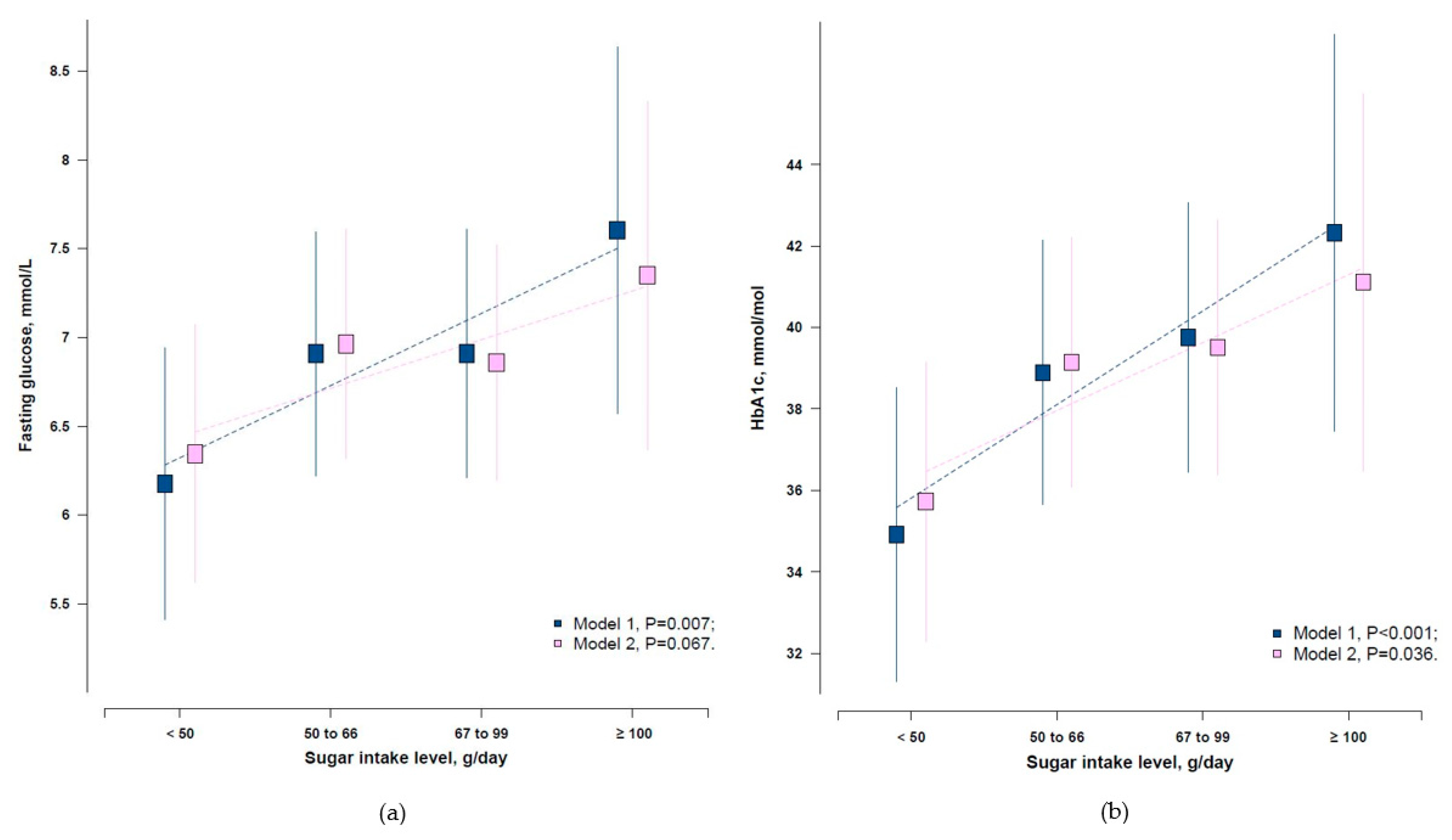
3.2. Associations between Added Sugar Intake Level and Glycaemic Parameters
3.3. Associations between Added Sugar Intake and the Risk of Undiagnosed T2D
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Van der Berg, J.D.; Stehouwer, C.D.; Bosma, H.; van der Velde, J.H.; Willems, P.J.; Savelberg, H.H.; Schram, M.T.; Sep, S.J.; van der Kallen, C.J.; Henry, R.M. Associations of total amount and patterns of sedentary behaviour with type 2 diabetes and the metabolic syndrome: The maastricht study. Diabetologia 2016, 59, 709–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Rev. Endo. 2018, 14, 88. [Google Scholar] [CrossRef] [PubMed]
- Zimmet, P.Z.; Magliano, D.J.; Herman, W.H.; Shaw, J.E. Diabetes: A 21st century challenge. Lancet Diab. Endo. 2014, 2, 56–64. [Google Scholar] [CrossRef]
- Farmanfarma, K.K.; Ansari-Moghaddam, A.; Zareban, I.; Adineh, H. Prevalence of type 2 diabetes in middle–east: Systematic review& meta-analysis. Primary Care Diabetes 2020, 14. [Google Scholar] [CrossRef]
- Al-Halaweh, A.A.; Davidovitch, N.; Almdal, T.P.; Cowan, A.; Khatib, S.; Nasser-Eddin, L.; Baradia, Z. Prevalence of type 2 diabetes mellitus complications among palestinians with t2dm. Diabetes Metab. Syndr. 2017, 11, 783–787. [Google Scholar] [CrossRef]
- Mataria, A.; Khatib, R.; Donaldson, C.; Bossert, T.; Hunter, D.J.; Alsayed, F.; Moatti, J.P. The health-care system: An assessment and reform agenda. Lancet 2009, 373, 1207–1217. [Google Scholar] [CrossRef]
- UNRWA. Annual Report of United Nations Relief and Works Agency; United Nations Relief and Works Agency for Palestine Refugees in the Near East: Amman, Jordan, 2018; p. 77. [Google Scholar]
- El Sharif, N.; Samara, I.; Titi, I.; Awartani, A. Compliance with and knowledge about diabetes guidelines among physicians and nurses in palestine. East Mediterr. Health J. 2011, 21, 791–802. [Google Scholar] [CrossRef]
- Feldman, I. Difficult distinctions: Refugee law, humanitarian practice, and political identification in gaza. Cult. Anthropol. 2007, 22, 129–169. [Google Scholar] [CrossRef]
- De Jong, A. The gaza freedom flotilla: Human rights, activism and academic neutrality. Soc. Mov. Stud. 2012, 11, 193–209. [Google Scholar] [CrossRef]
- PCBS. The international day of refugees 2019. Available online: http://www.badil.org/phocadownloadpap/Statistics/(PCBS)The-International-Day-of-Refugees-2019-eng.pdf (accessed on 28 May 2019).
- Feldman, I. The humanitarian condition: Palestinian refugees and the politics of living. Int. Human. Rights. J. 2012, 3, 155–172. [Google Scholar] [CrossRef]
- Bank, W. Gaza strip. In Middle East Contemporary Survey; UK Border Security: London, UK, 2010. [Google Scholar]
- Ziadni, M.; Hammoudeh, W.; Rmeileh, N.M.A.; Hogan, D.; Shannon, H.; Giacaman, R. Sources of human insecurity in post-war situations: The case of gaza. J. Hum. Secur. 2011, 7. [Google Scholar] [CrossRef]
- Giacaman, R.; Khatib, R.; Shabaneh, L.; Ramlawi, A.; Sabri, B.; Sabatinelli, G.; Khawaja, M.; Laurance, T. Health status and health services in the occupied palestinian territory. Lancet 2009, 373, 837–849. [Google Scholar] [CrossRef]
- Murray, C.J.; Abraham, J.; Ali, M.K.; Alvarado, M.; Atkinson, C.; Baddour, L.M.; Bartels, D.H.; Benjamin, E.J.; Bhalla, K.; Birbeck, G. The state of us health, 1990–2010: Burden of diseases, injuries, and risk factors. JAMA 2013, 310, 591–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danaei, G.; Ding, E.L.; Mozaffarian, D.; Taylor, B.; Rehm, J.; Murray, C.J.; Ezzati, M. The preventable causes of death in the united states: Comparative risk assessment of dietary, lifestyle, and metabolic risk factors. PLoS Med 2009. [Google Scholar] [CrossRef]
- Abdeen, Z.; Greenough, G.; Shahin, M.; Tayback, M. Nutritional Assessment of the West Bank and Gaza Strip; Ministry of Health, Al Quds University, US Agency for International Development and Care International: Jerusalem, Israel, 2002.
- Sweileh, W.M.; Sawalha, A.F.; Al-Jabi, S.W.; Zyoud, S.H.; Abutaha, A.S. Global research trends of literature in sugar-sweetened beverages: 2000–2016. Indian J. Health. Sci. Biomed. Res. 2018, 11, 191–221. [Google Scholar]
- Stene, L.; Giacaman, R.; Abdul-Rahim, H.; Husseini, A.; Norum, K.; Holmboe-Ottesen, G. Food consumption patterns in a palestinian west bank population. Eur. J. Clin. Nutr. 1999, 53, 953–958. [Google Scholar] [CrossRef] [Green Version]
- Johnson, R.K.; Appel, L.J.; Brands, M.; Howard, B.V.; Lefevre, M.; Lustig, R.H.; Sacks, F.; Steffen, L.M.; Wylie-Rosett, J. Dietary sugars intake and cardiovascular health: A scientific statement from the american heart association. Circulation 2009, 120, 1011–1020. [Google Scholar] [CrossRef]
- WHO. Healthy Diet; World Health Organization, Regional Office for the Eastern Mediterranean: Geneva, Switzerland, 2019. [Google Scholar]
- Guideline, W. Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Winkley, K.; Stahl, D.; Chalder, T.; Edmonds, M.E.; Ismail, K. Risk factors associated with adverse outcomes in a population-based prospective cohort study of people with their first diabetic foot ulcer. J. Diabetes Complicat. 2007, 21, 341–349. [Google Scholar] [CrossRef]
- Navarro-Flores, E.; Morales-Asencio, J.M.; Cervera-Marín, J.A.; Labajos-Manzanares, M.T.; Gijon-Nogueron, G. Development, validation and psychometric analysis of the diabetic foot self-care questionnaire of the university of malaga, spain (dfsq-uma). J. Tissue Viability 2015, 24, 24–34. [Google Scholar] [CrossRef]
- Basiri, R.; Spicer, M.T.; Levenson, C.W.; Ormsbee, M.J.; Ledermann, T.; Arjmandi, B.H. Nutritional supplementation concurrent with nutrition education accelerates the wound healing process in patients with diabetic foot ulcers. Biomedicines 2020, 8, 263. [Google Scholar] [CrossRef]
- Ministry of Health, PHIC. The Annual Report of the Primary Healthcare Centers in Gaza Strip 2018; Ministry of Health: Gaza, Palestine, 2019.
- PCBS. Palestine in Figures; Palestinian Central Bureau of Statistics: Ramallah, Palestine, 2015. [Google Scholar]
- International Physical Activity Questionnaire: Long Last 7 Days Self-Administered Format. 2012. Available online: http://www.sdp.univ.fvg.it/sites/default/files/IPAQ_English_self-admin_long.pdf (accessed on 15 June 2019).
- C.K.B. Resurvey Data: 2nd Resurvey Questionnaire. Available online: https://www.ckbiobank.org/site/Data+Access (accessed on 11 June 2019).
- WHO. Diet, Nutrition and the Prevention of Chronic Diseases; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Ross, R.; Berentzen, T.; Bradshaw, A.J.; Janssen, I.; Kahn, H.S.; Katzmarzyk, P.T.; Kuk, J.; Seidell, J.; Snijder, M.; Sørensen, T. Does the relationship between waist circumference, morbidity and mortality depend on measurement protocol for waist circumference? Obesity Rev. 2008, 9, 312–325. [Google Scholar] [CrossRef] [PubMed]
- Association, A.D. Diagnosis and classification of diabetes mellitus. Diabet. Care 2014, 37, 81–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hazboun, N.N. The Resettlement of the Palestinian Refugees of the Gaza Strip. Ph.D. Thesis, University of Leeds, Leeds, UK, 1994. [Google Scholar]
- Kurz, A.; Dekel, U.; Berti, B. The Crisis of the Gaza Strip: A Way Out; Kurz, A., Dekel, U., Eds.; Institute for National Security Studies: Tel Aviv, Israel, 2018. [Google Scholar]
- Devi, S. Gaza crisis continues to worsen as all eyes turn to lebanon. Lancet 2006, 368, 353–354. [Google Scholar] [CrossRef]
- Thabet, A.; Abu Tawahina, A.; El Sarraj, E.; Vostanis, P. Siege and quality of life of palestinians in the gaza strip. Arab. J. 2008, 20, 157–164. [Google Scholar]
- Filiu, J.P. The twelve wars on gaza. J. Palest. Stud. 2014, 44, 52–60. [Google Scholar] [CrossRef] [Green Version]
- El Sharif, N.; Imam, A. Current Status of Diabetes in Palestine: Epidemiology, Management, and Healthcare System. In Handbook of Healthcare in the Arab World; Laher, I., Ed.; Springer: Cham, Switzzerland, 2019. [Google Scholar]
- Oyola, M.G.; Handa, R.J. Hypothalamic–pituitary–adrenal and hypothalamic–pituitary–gonadal axes: Sex differences in regulation of stress responsivity. Stress 2017, 20, 476–494. [Google Scholar] [CrossRef]
- di Dalmazi, G.; Pagotto, U.; Pasquali, R.; Vicennati, V. Glucocorticoids and type 2 diabetes: From physiology to pathology. J. Nutr. Metab. 2012, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pitsavos, C.; Tampourlou, M.; Panagiotakos, D.B.; Skoumas, Y.; Chrysohoou, C.; Nomikos, T.; Stefanadis, C. Association between low-grade systemic inflammation and type 2 diabetes mellitus among men and women from the attica study. Rev. Diabet. Stud. 2007, 4, 98–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hackett, R.A.; Steptoe, A. Type 2 diabetes mellitus and psychological stress—a modifiable risk factor. Nat. Rev. Endocrinol. 2017, 13, 547–560. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.J.; Ismail, M. Stress and type 2 diabetes: A review of how stress contributes to the development of type 2 diabetes. Annu. Rev. Public Health 2015, 36, 441–462. [Google Scholar] [CrossRef] [Green Version]
- Ellulu, M.S. Obesity, hypertension, and type-2 diabetes mellitus: The interrelationships and the determinants among adults in Gaza city, Palestine. Osong. Pub. Health Res. Perspect. 2018, 9, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Baptista, L.C.; Dias, G.; Souza, N.R.; Veríssimo, M.T.; Martins, R.A. Effects of long-term multicomponent exercise on health-related quality of life in older adults with type 2 diabetes: Evidence from a cohort study. Qual. Life. Res. 2017, 26, 2117–2127. [Google Scholar] [CrossRef] [PubMed]
- Wändell, P.E.; Tovi, J. The quality of life of elderly diabetic patients. J. Diab. Complicat. 2000, 14, 25–30. [Google Scholar] [CrossRef]
- Weinger, K.; Beverly, E.A.; Smaldone, A. Diabetes self-care and the older adult. West. J. Nurs. Res. 2014, 36, 1272–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WTO. Making Tourism more Sustainable: A Guide for Policy Makers; World Tourism Organization Publications: Madrid, Spain, 2005. [Google Scholar]
- Abukashif, Y.J.; Riza, M. Urban development of conflict zones: The case of Gaza city. Open House Int. 2019, 2, 45–51. [Google Scholar]
- UNRWA. UNRWA Annual Operational Report 2019 for the Reporting Period 01 January–31 December 2019; United Nations Relief and Works Agency for Palestine refugees in the Near East (UNRWA): Amman, Jordan, 2019. [Google Scholar]
- Shahin, Y.; Kapur, A.; Seita, A. Diabetes care in refugee camps: The experience of unrwa. Diab. Res. Clin. Pract. 2015, 108, 1–6. [Google Scholar] [CrossRef]
- Radwan, M.; Elsous, A.; Al-Sharif, H.; Abu Mustafa, A. Glycemic control among primary care patients with type 2 diabetes mellitus in the gaza strip, palestine. Ther. Adv. Endocrinol. Metab. 2018, 9, 3–14. [Google Scholar] [CrossRef]
- Edelman, S.V.; Polonsky, W.H. Type 2 diabetes in the real world: The elusive nature of glycemic control. Diab. Care 2017, 40, 1425–1432. [Google Scholar] [CrossRef] [Green Version]
- Almadhoun, M.; Alagha, H. Assessment of medication adherence and its association with glycemic control among type-2 diabetes mellitus patients in gaza–palestine. Clin. Exp. Pharmacol. 2018, 3, 1–10. [Google Scholar]
- Horton, R. Offline: The health of palestinians is a global responsibility. Lancet 2018, 392, 1612. [Google Scholar] [CrossRef]
- Shabab, Q.S. The gaza health system. AMSA J. Glob. Health 2018, 12, 6–9. [Google Scholar]
- Weeratunga, P.; Jayasinghe, S.; Perera, Y.; Jayasena, G.; Jayasinghe, S. Per capita sugar consumption and prevalence of diabetes mellitus–global and regional associations. BMC Public Health 2014, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Millen, B.E.; Abrams, S.; Adams-Campbell, L.; Anderson, C.A.; Brenna, J.T.; Campbell, W.W.; Clinton, S.; Hu, F.; Nelson, M.; Neuhouser, M.L. The 2015 dietary guidelines advisory committee scientific report: Development and major conclusions. Adv. Nutr. 2016, 7, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Schulze, M.B.; Hu, F.B. Intake of sugar-sweetened beverages and weight gain: A systematic review. Am. J. Clin. Nutr. 2006, 84, 274–288. [Google Scholar] [CrossRef]
- Bray, G.A.; Popkin, B.M. Dietary sugar and body weight: Have we reached a crisis in the epidemic of obesity and diabetes?: Health be damned! Pour on the sugar. Diab. Care 2014, 37, 950–956. [Google Scholar] [CrossRef] [Green Version]
- Lapeyre, F.; Al Husseini, J.J.; Bocco, R.; Brunner, M.; Zureik, E. The living conditions of the palestine refugees registered with unrwa in jordan, lebanon, the syrian arab republic, the gaza strip and the west bank. Lebanon, the Syrian Arab Republic, the Gaza Strip and the West Bank. SSRN Electron. J. 2011, 16, 116. [Google Scholar]
- Williams, A. Unrwa and the occupied territories. J. Refug. Stud. 1989, 2, 156–162. [Google Scholar] [CrossRef]
- Riccardi, G.; Giacco, R.; Rivellese, A. Dietary fat, insulin sensitivity and the metabolic syndrome. Clin. Nutr. 2004, 23, 447–456. [Google Scholar] [CrossRef]
- Belfort, R.; Mandarino, L.; Kashyap, S.; Wirfel, K.; Pratipanawatr, T.; Berria, R.; DeFronzo, R.A.; Cusi, K. Dose-response effect of elevated plasma free fatty acid on insulin signaling. Diabetes 2005, 54, 1640–1648. [Google Scholar] [CrossRef] [Green Version]
- Boden, G.; Shulman, G. Free fatty acids in obesity and type 2 diabetes: Defining their role in the development of insulin resistance and β-cell dysfunction. Eur. J. Clin. Investig. 2002, 32, 14–23. [Google Scholar] [CrossRef]
- Paolisso, G.; Tataranni, P.; Foley, J.; Bogardus, C.; Howard, B.; Ravussin, E. A high concentration of fasting plasma non-esterified fatty acids is a risk factor for the development of niddm. Diabetologia 1995, 38, 1213–1217. [Google Scholar] [CrossRef] [PubMed]
- Item, F.; Konrad, D. Visceral fat and metabolic inflammation: The portal theory revisited. Obes. Rev. 2012, 13, 30–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergman, R.N.; Kim, S.P.; Catalano, K.J.; Hsu, I.R.; Chiu, J.D.; Kabir, M.; Hucking, K.; Ader, M. Why visceral fat is bad: Mechanisms of the metabolic syndrome. Obesity 2006, 14, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Cusi, K. The role of adipose tissue and lipotoxicity in the pathogenesis of type 2 diabetes. Curr. Diab. Rep. 2010, 10, 306–315. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | All n = 1000 | Diagnosed T2D n = 452 | Undiagnosed T2D n = 168 | Non-Cases n = 80 | p-Value |
|---|---|---|---|---|---|
| Age, years | 59.2 (7.5) | 59.1 (7.7) | 58.5 (7.3) | 59.4 (7.5) | 0.455 |
| Women | 468 (46.8%) | 217 (46.4%) | 83 (17.7%) | 168 (35.9%) | 0.034 |
| Study regions North | 220 (22.0%) | 101 (22.3%) | 32 (19.1%) | 87 (22.9%) | 0.286 |
| Gaza | 122 (12.2%) | 60 (13.3%) | 26 (15.5%) | 36 (9.5%) | |
| Midzone | 214 (21.4%) | 103 (22.8%) | 25 (14.8%) | 86 (22.6%) | |
| Khan Younis | 223 (22.3%) | 99 (21.9%) | 41 (24.4%) | 83 (21.8%) | |
| Rafah | 221 (22.1%) | 89 (19.7%) | 44 (26.2%) | 88 (23.2%) | |
| Refugees | 422 (42.2%) | 185 (40.9%) | 76 (45.2%) | 161 (42.4%) | 0.625 |
| Family size | 6.9 (1.5) | 6.9 (1.6) | 6.7 (1.5) | 6.9 (1.5) | 0.099 |
| Married | 844 (84.4%) | 373 (82.5%) | 147 (87.5%) | 324 (85.3%) | 0.386 |
| Education Low | 451 (45.1%) | 208 (46.0%) | 73 (43.4%) | 170 (44.7%) | 0.873 |
| Moderate | 295 (29.5%) | 134 (29.7%) | 47 (28.0%) | 114 (30.0%) | |
| High | 254 (25.4%) | 110 (24.3%) | 48 (28.6%) | 96 (25.3%) | |
| Employed | 117 (11.7%) | 48 (10.6%) | 20 (11.9%) | 49 (12.8%) | 0.594 |
| Household income (NIS) | 0.287 | ||||
| <500 | 51 (5.1%) | 26 (5.7%) | 11 (6.5%) | 14 (3.7%) | |
| 500–1000 | 41 (4.1%) | 23 (5.1%) | 9 (5.4%) | 9 (2.4%) | |
| 1000–1500 | 48 (4.8%) | 24 (5.3%) | 8 (4.8%) | 16 (4.2%) | |
| >1500 | 6 (0.6%) | 3 (0.7%) | 2 (1.2%) | 1 (0.3%) | |
| No constant income | 854 (85.4%) | 376 (83.2%) | 138 (82.1%) | 340 (89.4%) | |
| Having family history of NCDs b | 468 (46.8%) | 211 (46.7%) | 83 (49.4%) | 174 (45.8%) | 0.735 |
| Physical activity | 0.044 | ||||
| Low | 654 (65.4%) | 306 (67.7%) | 102 (60.7%) | 246 (64.7%) | |
| Moderate | 247 (24.7%) | 99 (21.9%) | 42 (25.0%) | 106 (27.9%) | |
| High | 99 (9.9%) | 47 (10.4%) | 24 (14.3%) | 28 (7.4%) | |
| T2D Medications | |||||
| Oral hypoglycaemic drugs | 225 (49.7%) | 225 (49.7%) | - | - | |
| Insulin | 171 (37.8%) | 171 (37.8%) | - | - | |
| Both | 56 (12.4%) | 56 (12.4%) | - | - | |
| Current cigarette’s smoking | 446 (44.6%) | 210 (46.5%) | 66 (39.3%) | 170 (44.7%) | 0.279 |
| BMI, kg/m2 | 28.1 (3.7) | 28.2 (3.7) | 28.5 (3.5) | 27.9 (3.7) | 0.189 |
| Waist circumference, cm | 105.0 (14.7) | 105.5 (14.8) | 105.2 (14.7) | 104.4 (14.6) | 0.547 |
| Fasting glucose, mmol/L | 9.4 (4.7) | 12.5 (4.6) | 10.0 (3.1) | 5.6 (1.0) | <0.001 |
| HbA1c, mmol/mol | 48.4 (18.8) | 60.5 (17.3) | 50.5 (14.4) | 32.9 (8.1) | <0.001 |
| HbA1c, % | 6.6 (1.7) | 7.7 (1.6) | 6.7 (1.3) | 5.2 (0.7) | <0.001 |
| Total cholesterol, mmol/L | 5.7 (1.6) | 6.2 (1.7) | 5.6 (1.3) | 5.1 (1.4) | <0.001 |
| Triglycerides, mmol/L | 2.1 (0.8) | 2.3 (0.8) | 2.0 (0.6) | 1.8 (0.7) | <0.001 |
| HDL, mmol/L | 1.1 (0.2) | 1.0 (0.2) | 1.1 (0.3) | 1.1 (0.2) | <0.001 |
| LDL, mmol/L | 4.4 (1.3) | 4.6 (1.3) | 4.2 (1.2) | 4.2 (1.2) | <0.001 |
| Systolic blood pressure, mmHg | 137.4 (21.4) | 137.7 (21.1) | 137.2 (20.9) | 137.1 (21.9) | 0.916 |
| Diastolic blood pressure, mmHg | 85.6 (7.2) | 85.7 (7.1) | 85.5 (7.4) | 85.8 (7.3) | 0.935 |
| Added sugar intake, g/day | 60.6 (22.4) | 60.1 (22.0) | 59.3 (23.4) | 61.8 (22.5) | 0.421 |
| Fruits consumption, g/day | 163.2 (49.3) | 161.4 (49.4) | 164.8 (48.2) | 164.5 (49.8) | 0.591 |
| Vegetable consumption, g/day | 282.3 (59.6) | 278.8 (59.9) | 285.1 (61.8) | 285.0 (58.4) | 0.267 |
| Added Sugar Intake Level g/day | No. of Participants n (%) | Model 1 | Model 2 | Model 3 | Model 4 |
|---|---|---|---|---|---|
| <50.0 g/day | 121 (22.1%) | 1.00 | 1.00 | 1.00 | 1.00 |
| 50.0–66.0 g/day | 183 (33.4%) | 2.13 (1.22–3.72) | 2.01 (1.13–3.59) | 2.01 (1.12–3.59) | 1.98 (1.09–3.60) |
| 67.0–99.0 g/day | 199 (36.3%) | 1.86 (1.06–3.25) | 1.59 (0.88–2.87) | 1.60 (0.89–2.88) | 1.54 (0.84–2.81) |
| ≥100.0 g/day | 45 (8.2%) | 3.52 (1.56–7.93) | 2.72 (1.15–6.39) | 2.72 (1.15–6.39) | 2.71 (1.12–6.54) |
| p for trend | <0.001 | <0.001 | <0.001 | <0.001 |
| Variable N (%) | <50.0 g/day OR (95% CI) n (%) | 50.0–66.0 g/day OR (95% CI) n (%) | ≥67.0 g/day OR (95% CI) n (%) | p-Value trend | p-Value interaction |
|---|---|---|---|---|---|
| Sex | 0.143 | ||||
| Men | 1.00 | 1.54 (0.67–3.55) | 2.04 (0.93–4.47) | 0.058 | |
| 310 (56.6%) | 60 (19.4%) | 104 (33.5%) | 146 (47.1%) | ||
| Women | 1.00 | 2.67 (1.19–6.02) | 1.42 (0.63–3.18) | 0.989 | |
| 238 (43.4%) | 61 (25.6%) | 79 (33.2%) | 98 (41.2%) | ||
| Age (Median) | 0.318 | ||||
| <59 years | 1.00 | 1.69 (0.71–4.03) | 1.64 (0.73–3.69) | 0.044 | |
| 259 (47.3 %) | 59 (22.8%) | 79 (30.5%) | 121 (46.7%) | ||
| ≥59 years | 1.00 | 1.41 (0.62–3.19) | 1.06 (0.46–2.40) | 0.679 | |
| 289 (52.7%) | 62 (21.4%) | 104 (36.0%) | 123 (42.6%) | ||
| BMI (Median) | 0.001 | ||||
| <26.7 kg/m2 | 1.00 | 1.94 (0.75–5.00) | 2.17 (0.84–5.34) | 0.808 | |
| 216 (39.4%) | 52 (24.1%) | 70 (32.4%) | 94 (43.5%) | ||
| ≥26.7 kg/m2 | 1.00 | 6.83 (2.69–17.36) | 4.72 (1.91–11.64) | 0.037 | |
| 332 (60.6%) | 69 (20.7%) | 113 (34.1%) | 150 (45.2%) | ||
| Population | 0.047 | ||||
| Refugees | 1.00 | 5.46 (1.75–17.08) | 5.09 (1.64–15.84) | 0.043 | |
| 237 (43.2%) | 52 (21.9%) | 77 (32.5%) | 108 (45.6%) | ||
| Citizens | 1.00 | 4.93 (1.61–12.26) | 3.98 (1.33–11.95) | 0.666 | |
| 311 (56.8%) | 69 (22.2%) | 106 (34.1%) | 136 (43.7%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jebril, M.; Liu, X.; Shi, Z.; Mazidi, M.; Altaher, A.; Wang, Y. Prevalence of Type 2 Diabetes and Its Association with Added Sugar Intake in Citizens and Refugees Aged 40 or Older in the Gaza Strip, Palestine. Int. J. Environ. Res. Public Health 2020, 17, 8594. https://doi.org/10.3390/ijerph17228594
Jebril M, Liu X, Shi Z, Mazidi M, Altaher A, Wang Y. Prevalence of Type 2 Diabetes and Its Association with Added Sugar Intake in Citizens and Refugees Aged 40 or Older in the Gaza Strip, Palestine. International Journal of Environmental Research and Public Health. 2020; 17(22):8594. https://doi.org/10.3390/ijerph17228594
Chicago/Turabian StyleJebril, Majed, Xin Liu, Zumin Shi, Mohsen Mazidi, Akram Altaher, and Youfa Wang. 2020. "Prevalence of Type 2 Diabetes and Its Association with Added Sugar Intake in Citizens and Refugees Aged 40 or Older in the Gaza Strip, Palestine" International Journal of Environmental Research and Public Health 17, no. 22: 8594. https://doi.org/10.3390/ijerph17228594
APA StyleJebril, M., Liu, X., Shi, Z., Mazidi, M., Altaher, A., & Wang, Y. (2020). Prevalence of Type 2 Diabetes and Its Association with Added Sugar Intake in Citizens and Refugees Aged 40 or Older in the Gaza Strip, Palestine. International Journal of Environmental Research and Public Health, 17(22), 8594. https://doi.org/10.3390/ijerph17228594