Metabolic Syndrome and Colorectal Cancer Risk: Results of Propensity Score-Based Analyses in a Community-Based Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
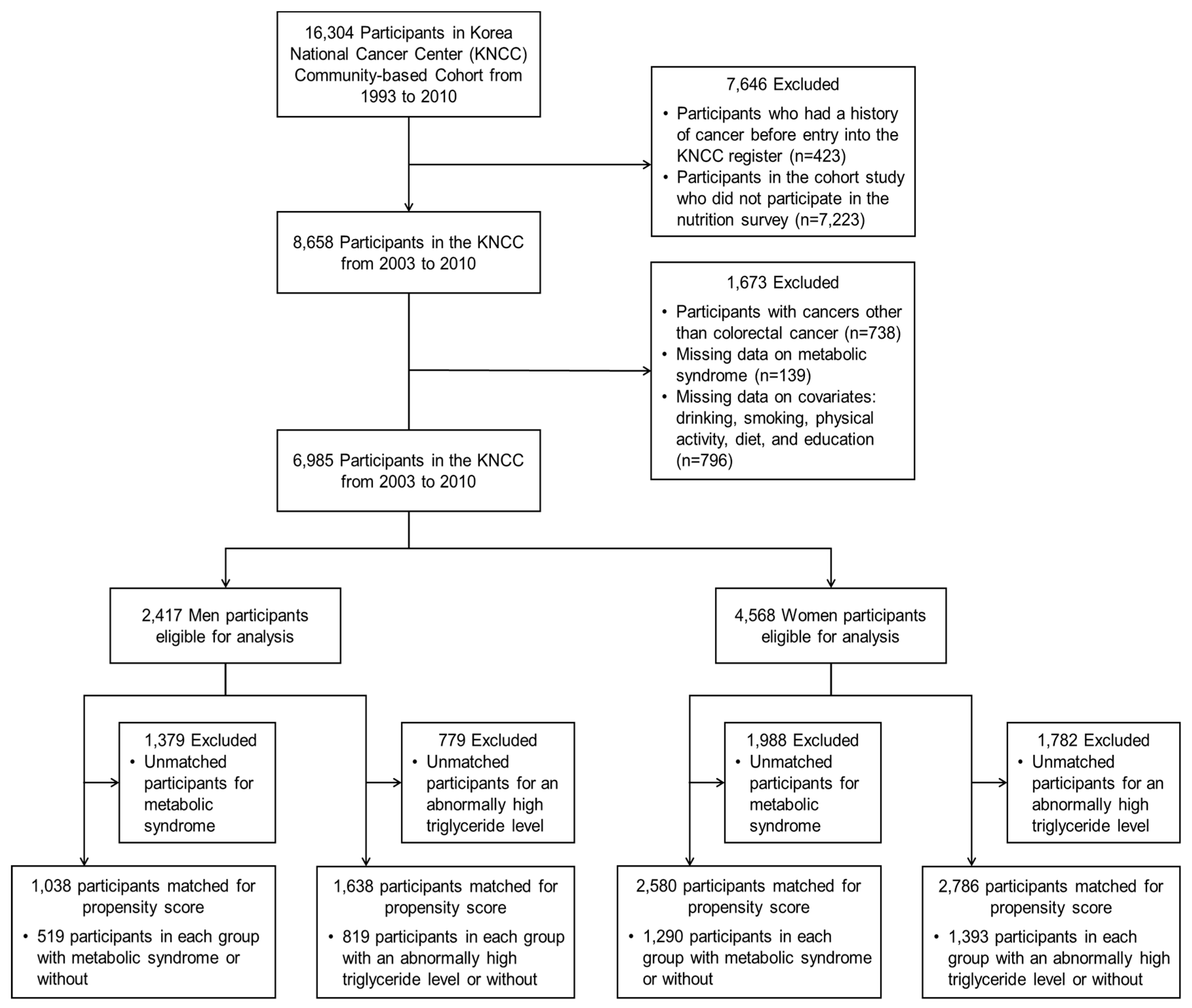
2.1. Data Source and Study Population
2.2. Definition of CRC and MetS
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esposito, K.; Chiodini, P.; Colao, A.; Lenzi, A.; Giugliano, D. Metabolic syndrome and risk of cancer: A systematic review and meta-analysis. Diabetes Care 2012, 35, 2402–2411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendonca, F.M.; De Sousa, F.R.; Barbosa, A.L.; Martins, S.C.; Araujo, R.L.; Soares, R.; Abreu, C. Metabolic syndrome and risk of cancer: Which link? Metab. Clin. Exp. 2015, 64, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Chiodini, P.; Capuano, A.; Bellastella, G.; Maiorino, M.I.; Rafaniello, C.; Panagiotakos, D.B.; Giugliano, D. Colorectal cancer association with metabolic syndrome and its components: A systematic review with meta-analysis. Endocrine 2013, 44, 634–647. [Google Scholar] [CrossRef]
- Ko, S.; Yoon, S.J.; Kim, D.; Kim, A.R.; Kim, E.J.; Seo, H.Y. Metabolic risk profile and cancer in Korean men and women. J. Prev. Med. Public Health Yebang Uihakhoe Chi. 2016, 49, 143–152. [Google Scholar] [CrossRef] [Green Version]
- Kim, N.H.; Park, J.H.; Park, D.I.; Sohn, C.I.; Choi, K.; Jung, Y.S. Metabolic syndrome is a risk factor for adenoma occurrence at surveillance colonoscopy: A single-center experience in Korea. Medicine 2016, 95, e4454. [Google Scholar] [CrossRef]
- Kim, M.C.; Kim, C.S.; Chung, T.H.; Park, H.O.; Yoo, C.I. Metabolic syndrome, lifestyle risk factors, and distal colon adenoma: A retrospective cohort study. World J. Gastroenterol. 2011, 17, 4031–4037. [Google Scholar] [CrossRef]
- Haukoos, J.S.; Lewis, R.J. The propensity score. JAMA 2015, 314, 1637–1638. [Google Scholar] [CrossRef]
- Austin, P.C. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [Green Version]
- Tak, Y.J.; Lee, S.Y.; Park, S.K.; Kim, Y.J.; Lee, J.G.; Jeong, D.W.; Kim, S.C.; Kim, I.J.; Yi, Y.H. Association between uterine leiomyoma and metabolic syndrome in parous premenopausal women: A case-control study. Medicine 2016, 95, e5325. [Google Scholar] [CrossRef]
- Won, K.B.; Chang, H.J.; Han, D.; Sung, J.; Choi, S.Y. Metabolic syndrome predicts long-term mortality in subjects without established diabetes mellitus in asymptomatic Korean population: A propensity score matching analysis from the Korea Initiatives on Coronary Artery Calcification (KOICA) registry. Medicine 2016, 95, e5421. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Kloor, M.; Pox, C.P. Colorectal cancer. Lancet 2014, 383, 1490–1502. [Google Scholar] [CrossRef] [PubMed]
- Liang, P.S.; Chen, T.Y.; Giovannucci, E. Cigarette smoking and colorectal cancer incidence and mortality: Systematic review and meta-analysis. Int. J. Cancer 2009, 124, 2406–2415. [Google Scholar] [CrossRef] [PubMed]
- Fedirko, V.; Tramacere, I.; Bagnardi, V.; Rota, M.; Scotti, L.; Islami, F.; Negri, E.; Straif, K.; Romieu, I.; La Vecchia, C.; et al. Alcohol drinking and colorectal cancer risk: An overall and dose-response meta-analysis of published studies. Ann. Oncol. 2011, 22, 1958–1972. [Google Scholar] [CrossRef]
- Chan, D.S.; Lau, R.; Aune, D.; Vieira, R.; Greenwood, D.C.; Kampman, E.; Norat, T. Red and processed meat and colorectal cancer incidence: Meta-analysis of prospective studies. PLoS ONE 2011, 6, e20456. [Google Scholar] [CrossRef] [Green Version]
- Boyle, T.; Keegel, T.; Bull, F.; Heyworth, J.; Fritschi, L. Physical activity and risks of proximal and distal colon cancers: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2012, 104, 1548–1561. [Google Scholar] [CrossRef]
- Aune, D.; Lau, R.; Chan, D.S.; Vieira, R.; Greenwood, D.C.; Kampman, E.; Norat, T. Nonlinear reduction in risk for colorectal cancer by fruit and vegetable intake based on meta-analysis of prospective studies. Gastroenterology 2011, 141, 106–118. [Google Scholar] [CrossRef] [Green Version]
- Hemminki, K.; Li, X. Level of education and the risk of cancer in Sweden. Cancer Epidemiol. Biomark. Prev. 2003, 12, 796–802. [Google Scholar]
- Perdue, D.G.; Perkins, C.; Jackson-Thompson, J.; Coughlin, S.S.; Ahmed, F.; Haverkamp, D.S.; Jim, M.A. Regional differences in colorectal cancer incidence, stage, and subsite among American Indians and Alaska Natives, 1999–2004. Cancer 2008, 113, 1179–1190. [Google Scholar] [CrossRef] [Green Version]
- Oh, J.K.; Lim, M.K.; Yun, E.H.; Choi, M.H.; Hong, S.T.; Chang, S.H.; Park, S.K.; Cho, S.I.; Kim, D.H.; Yoo, K.Y.; et al. Cohort profile: Community-based prospective cohort from the national cancer center, Korea. Int. J. Epidemiol. 2017, 46, e14. [Google Scholar] [CrossRef]
- Park, E.Y.; Lim, M.K.; Oh, J.K.; Cho, H.; Bae, M.J.; Yun, E.H.; Kim, D.I.; Shin, H.R. Independent and supra-additive effects of alcohol consumption, cigarette smoking, and metabolic syndrome on the elevation of serum liver enzyme levels. PLoS ONE 2013, 8, e63439. [Google Scholar] [CrossRef]
- Shin, A.; Lim, S.Y.; Sung, J.; Shin, H.R.; Kim, J. Dietary intake, eating habits, and metabolic syndrome in Korean men. J. Am. Diet. Assoc. 2009, 109, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Cleeman, J.I.; Merz, C.N.; Brewer, H.B., Jr.; Clark, L.T.; Hunninghake, D.B.; Pasternak, R.C.; Smith, S.C., Jr.; Stone, N.J. Implications of recent clinical trials for the national cholesterol education program adult treatment panel III guidelines. Circulation 2004, 110, 227–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, R.L.; Schmitz, K.H.; Anderson, K.E.; Rosamond, W.D.; Folsom, A.R. The metabolic syndrome and risk of incident colorectal cancer. Cancer 2006, 107, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Jinjuvadia, R.; Lohia, P.; Jinjuvadia, C.; Montoya, S.; Liangpunsakul, S. The association between metabolic syndrome and colorectal neoplasm: Systemic review and meta-analysis. J. Clin. Gastroenterol. 2013, 47, 33–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parsons, L. Performing a 1:N case-control match on propensity score. In Proceedings of the 29th Annual SAS Users Group International Conference; Available online: https://support.sas.com/resources/papers/proceedings/proceedings/sugi29/165-29.pdf (accessed on 4 April 2019).
- Desai, R.J.; Rothman, K.J.; Bateman, B.T.; Hernandez-Diaz, S.; Huybrechts, K.F. A propensity-score-based fine stratification approach for confounding adjustment when exposure is infrequent. Epidemiology 2017, 28, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Kurth, T.; Walker, A.M.; Glynn, R.J.; Chan, K.A.; Gaziano, J.M.; Berger, K.; Robins, J.M. Results of multivariable logistic regression, propensity matching, propensity adjustment, and propensity-based weighting under conditions of nonuniform effect. Am. J. Epidemiol. 2006, 163, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Bohn, J. Package ‘Tableone’ for R Statistical Programming Language. Available online: https://cran.r-project.org/web/packages/tableone/tableone.pdf (accessed on 4 April 2019).
- Elze, M.C.; Gregson, J.; Baber, U.; Williamson, E.; Sartori, S.; Mehran, R.; Nichols, M.; Stone, G.W.; Pocock, S.J. Comparison of propensity score methods and covariate adjustment: Evaluation in 4 cardiovascular studies. J. Am. Coll. Cardiol. 2017, 69, 345–357. [Google Scholar] [CrossRef]
- Kabat, G.C.; Kim, M.Y.; Peters, U.; Stefanick, M.; Hou, L.; Wactawski-Wende, J.; Messina, C.; Shikany, J.M.; Rohan, T.E. A longitudinal study of the metabolic syndrome and risk of colorectal cancer in postmenopausal women. Eur. J. Cancer Prev. 2012, 21, 326–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabat, G.C.; Kim, M.Y.; Stefanick, M.; Ho, G.Y.F.; Lane, D.S.; Odegaard, A.O.; Simon, M.S.; Bea, J.W.; Luo, J.; Wassertheil-Smoller, S.; et al. Metabolic obesity phenotypes and risk of colorectal cancer in postmenopausal women. Int. J. Cancer 2018, 143, 543–551. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.J.; Lee, D.H.; Han, K.D.; Shin, C.M.; Kim, N. Abdominal obesity, glucose intolerance and decreased high-density lipoprotein cholesterol as components of the metabolic syndrome are associated with the development of colorectal cancer. Eur. J. Epidemiol. 2018, 33, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- Inoue, M.; Noda, M.; Kurahashi, N.; Iwasaki, M.; Sasazuki, S.; Iso, H.; Tsugane, S. Impact of metabolic factors on subsequent cancer risk: Results from a large-scale population-based cohort study in Japan. Eur. J. Cancer Prev. 2009, 18, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, A.; Leipsic, J.; Feuchtner, G.; Gransar, H.; Kalra, D.; Heo, R.; Achenbach, S.; Andreini, D.; Al-Mallah, M.; Berman, D.S.; et al. Is metabolic syndrome predictive of prevalence, extent, and risk of coronary artery disease beyond its components? Results from the multinational coronary CT angiography evaluation for clinical outcome: An international multicenter registry (CONFIRM). PLoS ONE 2015, 10, e0118998. [Google Scholar] [CrossRef] [Green Version]
- Kheterpal, E.; Sammon, J.D.; Diaz, M.; Bhandari, A.; Trinh, Q.D.; Pokala, N.; Sharma, P.; Menon, M.; Agarwal, P.K. Effect of metabolic syndrome on pathologic features of prostate cancer. Urol. Oncol. 2013, 31, 1054–1059. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Men | Women | ||||
|---|---|---|---|---|---|---|
| Colorectal Cancer | p-Value | Colorectal Cancer | p-Value | |||
| No (N = 2360) | Yes (N = 57) | No (N = 4514) | Yes (N = 54) | |||
| Follow-up (years, Median (IQR)) | 10.43 (8.5–12.48) | 4.76 (2.91–7.79) | <0.001 | 10.44 (9.48–12.88) | 5.55 (3.06–7.53) | <0.001 |
| Age (years, Mean ± SD) | 59.66 ± 10.93 | 64.18 ± 8.67 | 0.002 | 59.95 ± 11.2 | 64.72 ± 9.19 | 0.001 |
| Physical activity (days/week, Mean ± SD) | 3.97 ± 2.86 | 4.26 ± 2.7 | 0.754 | 2.99 ± 2.96 | 3.2 ± 3.02 | 0.60 |
| Intake of fruits or vegetables (days/week, Mean ± SD) | 5.43 ± 1.44 | 5.19 ± 1.57 | 0.28 | 5.51 ± 1.46 | 5.04 ± 1.8 | 0.073 |
| Intake of beef or pork (days/week, Mean ± SD) | 2.55 ± 1.4 | 2.44 ± 1.49 | 0.732 | 1.75 ± 1.33 | 1.31 ± 1.33 | 0.012 |
| Alcohol consumption [N(%)] | ||||||
| Non-drinkers | 640 (27.12) | 7 (12.28) | 0.03 | 3598 (79.71) | 45 (83.33) | 0.796 |
| Moderate drinkers (<24 g/day) | 797 (33.77) | 26 (45.61) | 797 (17.66) | 8 (14.81) | ||
| Heavy drinkers (≥24 g/day) | 923 (39.11) | 24 (42.11) | 119 (2.64) | 1 (1.85) | ||
| Smoking status [N(%)] | ||||||
| Non-smokers | 483 (20.47) | 12 (21.05) | 0.952 | 4186 (92.73) | 52 (96.3) | 0.894 |
| Moderate smokers (<20 pack-year) | 669 (28.35) | 17 (29.82) | 263 (5.83) | 2 (3.7) | ||
| Heavy smokers (≥20 pack-year) | 1208 (51.19) | 28 (49.12) | 65 (1.44) | 0 (0) | ||
| Education level [N(%)] | ||||||
| Illiterate | 222 (9.41) | 6 (10.53) | 0.448 | 1445 (32.01) | 24 (44.44) | 0.24 |
| Middle school or less | 1443 (61.14) | 39 (68.42) | 2505 (55.49) | 26 (48.15) | ||
| High school | 484 (20.51) | 10 (17.54) | 438 (9.7) | 3 (5.56) | ||
| College or more | 211 (8.94) | 2 (3.51) | 126 (2.79) | 1 (1.85) | ||
| Residential area [N(%)] | ||||||
| Sancheong-gun | 1270 (53.81) | 23 (40.35) | 0.209 | 2380 (52.72) | 21 (38.89) | 0.072 |
| Changwon-si | 485 (20.55) | 16 (28.07) | 867 (19.21) | 13 (24.07) | ||
| Chooncheon-si | 167 (7.08) | 7 (12.28) | 438 (9.7) | 3 (5.56) | ||
| Choongjoo-si | 281 (11.91) | 8 (14.04) | 558 (12.36) | 11 (20.37) | ||
| Haman-gun | 157 (6.65) | 3 (5.26) | 271 (6) | 6 (11.11) | ||
| Metabolic syndrome [N(%)] | ||||||
| No (No. of components of MetS < 3) | 1848 (78.31) | 45 (78.95) | 0.907 | 3243 (71.84) | 28 (51.85) | 0.001 |
| Yes (No. of components of MetS ≥ 3) | 512 (21.69) | 12 (21.05) | 1271 (28.16) | 26 (48.15) | ||
| Blood pressure [N(%)] | ||||||
| Normal BP | 996 (42.2) | 21 (36.84) | 0.418 | 2017 (44.68) | 19 (35.19) | 0.163 |
| High BP | 1364 (57.8) | 36 (63.16) | 2497 (55.32) | 35 (64.81) | ||
| BMI [N(%)] | ||||||
| <25 kg/m2 | 1667 (70.64) | 40 (70.18) | 0.94 | 2840 (62.92) | 33 (61.11) | 0.785 |
| ≥25 kg/m2 | 693 (29.36) | 17 (29.82) | 1674 (37.08) | 21 (38.89) | ||
| HDL cholesterol [N(%)] | ||||||
| Normal HDL | 1913 (81.06) | 54 (94.74) | 0.009 | 2309 (51.15) | 26 (48.15) | 0.661 |
| Low HDL | 447 (18.94) | 3 (5.26) | 2205 (48.85) | 28 (51.85) | ||
| Triglyceride level [N(%)] | ||||||
| Normal TG | 1552 (65.76) | 40 (70.18) | 0.488 | 3148 (69.74) | 27 (50) | 0.002 |
| High TG | 808 (34.24) | 17 (29.82) | 1366 (30.26) | 27 (50) | ||
| FBS [N(%)] | ||||||
| Normal FBS | 2047 (86.74) | 46 (80.7) | 0.186 | 4042 (89.54) | 49 (90.74) | 0.775 |
| High FBS | 313 (13.26) | 11 (19.3) | 472 (10.46) | 5 (9.26) | ||
| Total | Men | Women | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Methods | Cases (N) | Controls (N) | HR (OR) (95% CI) | p-Value | Cases (N) | Controls (N) | HR (OR) (95% CI) | p-Value | Cases (N) | Controls (N) | HR (OR) (95% CI) | p-Value |
| (a) Metabolic syndrome | ||||||||||||
| Cox hazard regression | ||||||||||||
| Unadjusted | 111 | 6874 | 1.46 (0.99, 2.16) | 0.060 | 57 | 2360 | 0.94 (0.50, 1.78) | 0.856 | 54 | 4514 | 2.33 (1.37, 3.97) | 0.002 |
| Multivariable (a) | 111 | 6874 | 1.55 (1.04, 2.33) | 0.033 | 57 | 2360 | 1.04 (0.54, 1.99) | 0.908 | 54 | 4514 | 2.12 (1.22, 3.68) | 0.008 |
| PS-based logistic regression | ||||||||||||
| Matched for PS | 67 | 3573 | 1.32 (0.81, 2.13) | 0.266 | 25 | 1013 | 0.93 (0.42, 2.03) | 0.847 | 38 | 2542 | 2.19 (1.10, 4.33) | 0.025 |
| Stratification into 5 strata by PS | 111 | 6862 | 1.48 (1.00, 2.19) | 0.050 | 57 | 2345 | 1.06 (0.56, 2.02) | 0.859 | 53 | 4505 | 2.23 (1.32, 3.77) | 0.003 |
| Regression adjusted with PS | ||||||||||||
| as a continuous term | 111 | 6874 | 1.45 (0.97, 2.16) | 0.071 | 57 | 2360 | 1.05 (0.55, 2.01) | 0.878 | 54 | 4514 | 2.03 (1.17, 3.53) | 0.012 |
| as a quintile term | 111 | 6874 | 1.48 (0.99, 2.22) | 0.054 | 57 | 2360 | 1.02 (0.54, 1.95) | 0.947 | 54 | 4514 | 2.07 (1.20, 3.58) | 0.009 |
| Weighted models | ||||||||||||
| IPTW model | 111 | 6874 | 1.43 (1.11, 1.85) | 0.007 | 57 | 2360 | 1.06 (0.73, 1.52) | 0.772 | 54 | 4514 | 2.03 (1.40, 2.95) | <0.001 |
| SMRW model | 111 | 6874 | 1.44 (1.04, 2.01) | 0.031 | 57 | 2360 | 0.92 (0.52, 1.64) | 0.780 | 54 | 4514 | 2.48 (1.63, 3.75) | <0.001 |
| (b) Triglyceride level | ||||||||||||
| Cox hazard regression | ||||||||||||
| Unadjusted | 111 | 6874 | 1.39 (0.95, 2.03) | 0.090 | 57 | 2360 | 0.79 (0.45, 1.39) | 0.416 | 54 | 4514 | 2.27 (1.33, 3.87) | 0.003 |
| Multivariable (a) | 111 | 6874 | 1.33 (0.91, 1.95) | 0.145 | 57 | 2360 | 0.84 (0.47, 1.5) | 0.557 | 54 | 4514 | 2.06 (1.2, 3.55) | 0.009 |
| PS-based logistic regression | ||||||||||||
| Matched for PS | 76 | 4360 | 1.36 (0.86, 2.14) | 0.191 | 32 | 1606 | 1.11 (0.55, 2.21) | 0.777 | 40 | 2746 | 2.08 (1.07, 4.02) | 0.031 |
| Stratification into 5 strata by PS | 111 | 6866 | 1.3 (0.89, 1.9) | 0.168 | 57 | 2354 | 0.82 (0.47, 1.45) | 0.498 | 53 | 4501 | 2.26 (1.32, 3.84) | 0.003 |
| Regression adjusted with PS | ||||||||||||
| as a continuous term | 111 | 6874 | 1.28 (0.87, 1.88) | 0.210 | 57 | 2360 | 0.85 (0.48, 1.51) | 0.570 | 54 | 4514 | 2.02 (1.18, 3.48) | 0.011 |
| as a quintile term | 111 | 6874 | 1.28 (0.87, 1.88) | 0.202 | 57 | 2360 | 0.82 (0.46, 1.46) | 0.504 | 54 | 4514 | 2.03 (1.18, 3.50 | 0.010 |
| Weighted models | ||||||||||||
| IPTW model | 111 | 6874 | 1.28 (0.99, 1.66) | 0.063 | 57 | 2360 | 0.85 (0.58, 1.23) | 0.380 | 54 | 4514 | 1.98 (1.36, 2.89) | <0.001 |
| SMRW model | 111 | 6874 | 1.44 (1.05, 1.97) | 0.025 | 57 | 2360 | 0.79 (0.48, 1.30 | 0.350 | 54 | 4514 | 2.42 (1.6, 3.66) | <0.001 |
| N (Cases/Controls) | HR(OR) | 95% CI | p Value | |
|---|---|---|---|---|
| (a) Colon cancer (C18–C19) | ||||
| Cox hazard regression | ||||
| Unadjusted | 4549 (35/4514) | 1.88 | 0.96, 3.68 | 0.064 |
| Multivariable (a) | 4549 (35/4514) | 1.71 | 0.86, 3.43 | 0.128 |
| PS-based logistic regression | ||||
| Matched for PS | 2564 (25/2539) | 1.52 | 0.69, 3.39 | 0.302 |
| Stratification into 5 strata by PS | 4539 (34/4505) | 1.81 | 0.93, 3.5 | 0.079 |
| Regression adjusted with PS | ||||
| as a continuous term | 4549 (35/4514) | 1.6 | 0.8, 3.19 | 0.184 |
| as a quintile term | 4549 (35/4514) | 1.63 | 0.82, 3.24 | 0.164 |
| Weighted models | ||||
| IPTW model | 4549 (35/4514) | 3.29 | 1.29, 8.36 | 0.012 |
| SMRW model | 4549 (35/4514) | 1.92 | 1.12, 3.28 | 0.018 |
| (b) Rectum cancer (C20) | ||||
| Cox hazard regression | ||||
| Unadjusted | 4533 (19/4514) | 3.47 | 1.4, 8.64 | 0.007 |
| Multivariable (a) | 4533 (19/4514) | 3.25 | 1.28, 8.25 | 0.013 |
| PS-based logistic regression | ||||
| Matched for PS | 2554 (14/2540) | 3.67 | 1.03, 13.17 | 0.046 |
| Stratification into 5 strata by PS | 4522 (19/4503) | 3.16 | 1.3, 7.64 | 0.011 |
| Regression adjusted with PS | ||||
| as a continuous term | 4533 (19/4514) | 3.19 | 1.25, 8.16 | 0.015 |
| as a quintile term | 4533 (19/4514) | 3.29 | 1.29, 8.36 | 0.012 |
| Weighted models | ||||
| IPTW model | 4533 (19/4514) | 3.29 | 1.29, 8.36 | 0.012 |
| SMRW model | 4533 (19/4514) | 4.13 | 2.12, 8.06 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Park, E.Y.; Park, E.; Lim, M.K.; Oh, J.-K.; Kim, B. Metabolic Syndrome and Colorectal Cancer Risk: Results of Propensity Score-Based Analyses in a Community-Based Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 8687. https://doi.org/10.3390/ijerph17228687
Kim J, Park EY, Park E, Lim MK, Oh J-K, Kim B. Metabolic Syndrome and Colorectal Cancer Risk: Results of Propensity Score-Based Analyses in a Community-Based Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(22):8687. https://doi.org/10.3390/ijerph17228687
Chicago/Turabian StyleKim, Jinsun, Eun Young Park, Eunjung Park, Min Kyung Lim, Jin-Kyoung Oh, and Byungmi Kim. 2020. "Metabolic Syndrome and Colorectal Cancer Risk: Results of Propensity Score-Based Analyses in a Community-Based Cohort Study" International Journal of Environmental Research and Public Health 17, no. 22: 8687. https://doi.org/10.3390/ijerph17228687
APA StyleKim, J., Park, E. Y., Park, E., Lim, M. K., Oh, J. -K., & Kim, B. (2020). Metabolic Syndrome and Colorectal Cancer Risk: Results of Propensity Score-Based Analyses in a Community-Based Cohort Study. International Journal of Environmental Research and Public Health, 17(22), 8687. https://doi.org/10.3390/ijerph17228687