Alternative Tobacco Product Use in Critically Ill Patients

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Sample
2.2. Enrollment of Patients
2.3. Collection of Data
2.4. Statistical Analysis
3. Results
3.1. Cohort Description
3.2. Baseline Characteristics of Study Participants
3.3. Clinical Characteristics of Survey Responders vs. Non-Responders
3.4. Clinical Characteristics of Self- vs. Surrogate Responders
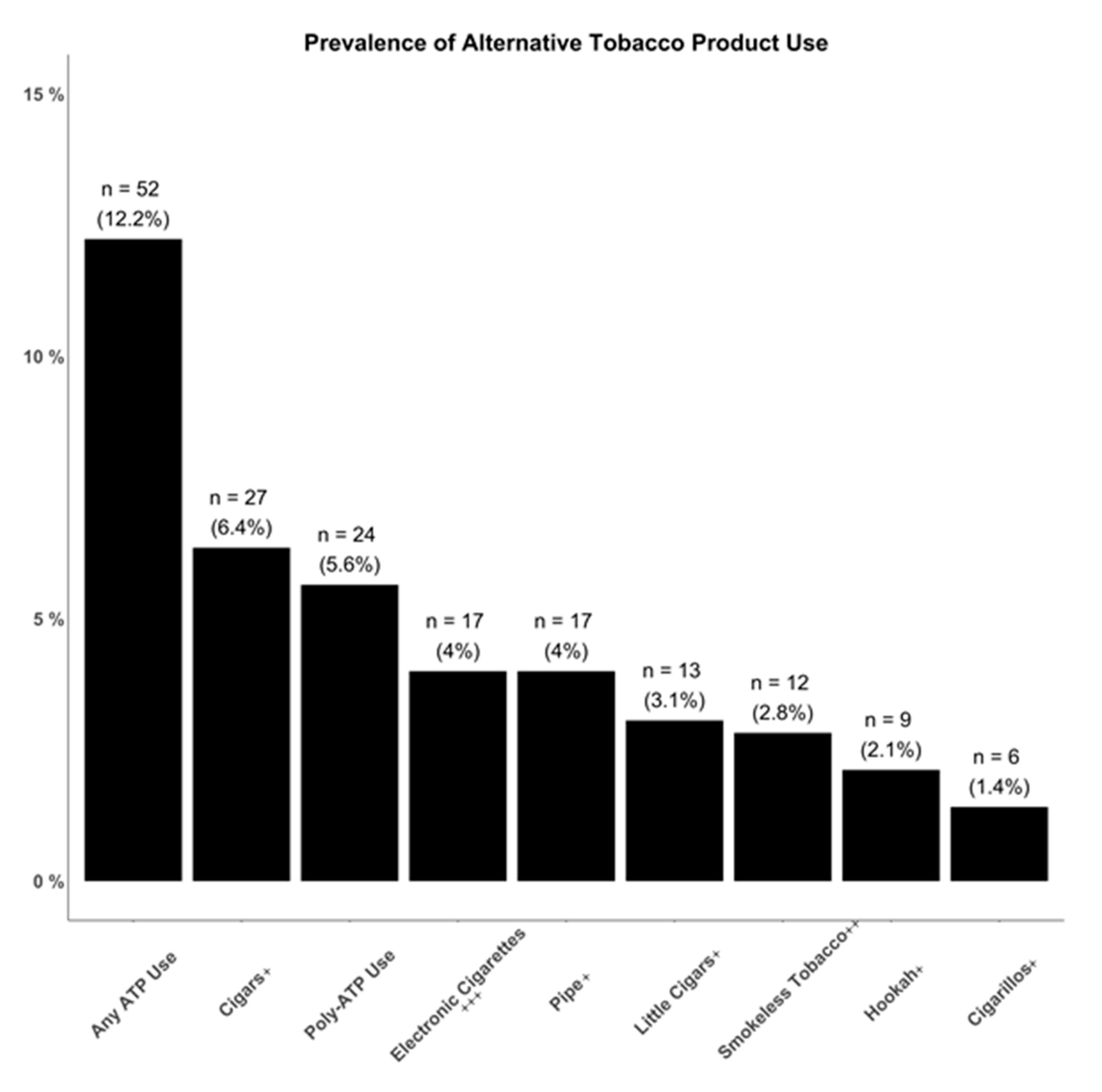
3.5. Prevalence of Alternative Tobacco Product Usage
3.6. Barriers to Collection of ATP Data in Critically Ill Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Popova, L.; Ling, P.M. Alternative tobacco product use and smoking cessation: A national study. Am. J. Public Health 2013, 103, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Amrock, S.M.; Weitzman, M. Alternative tobacco products as a second front in the war on tobacco. JAMA 2015, 314, 1507–1508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrell, P.T.; Naqvi, S.M.H.; Plunk, A.D.; Ji, M.; Martins, S.S. Patterns of youth tobacco and polytobacco usage: The shift to alternative tobacco products. Am. J. Drug Alcohol Abus. 2016, 1–9. [Google Scholar] [CrossRef]
- Backinger, C.L.; Fagan, P.; O’Connell, M.E.; Grana, R.; Lawrence, D.; Bishop, J.A.; Gibson, J.T. Use of other tobacco products among u.S. Adult cigarette smokers: Prevalence, trends and correlates. Addict. Behav. 2008, 33, 472–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schier, J.G.; Meiman, J.G.; Layden, J.; Mikosz, C.A.; VanFrank, B.; King, B.A.; Salvatore, P.P.; Weissman, D.N.; Thomas, J.; Melstrom, P.C.; et al. states investigating severe pulmonary disease among people who use e-cigarettes [press release]. Centers for Disease Control and Prevention. Morb. Mortal. Wkly. Rep. 2019, 68, 787. [Google Scholar] [CrossRef]
- Lee, Y.O.; Hebert, C.J.; Nonnemaker, J.M.; Kim, A.E. Multiple tobacco product use among adults in the united states: Cigarettes, cigars, electronic cigarettes, hookah, smokeless tobacco and snus. Prev. Med. 2014, 62, 14–19. [Google Scholar] [CrossRef]
- Dinakar, C.; O’Connor, G.T. The health effects of electronic cigarettes. N. Engl. J. Med. 2016, 375, 1372–1381. [Google Scholar] [CrossRef]
- Garland, A.; Olafson, K.; Ramsey, C.D.; Yogendran, M.; Fransoo, R. Epidemiology of critically ill patients in intensive care units: A population-based observational study. Crit. Care 2013, 17, R212. [Google Scholar] [CrossRef] [Green Version]
- Burns, D.M. Cigarette smoking among the elderly: Disease consequences and the benefits of cessation. Am. J. Health Promot. 2000, 14, 357–361. [Google Scholar] [CrossRef]
- Muthukrishnan, A.; Warnakulasuriya, S. Oral health consequences of smokeless tobacco use. Indian J. Med Res. 2018, 148, 35–40. [Google Scholar]
- Kadhum, M.; Sweidan, A.; Jaffery, A.E.; Al-Saadi, A.; Madden, B. A review of the health effects of smoking shisha. Clin. Med. 2015, 15, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Washam, C. Can cigarette alternatives deliver a safer fix? Environ. Health Perspect 2011, 119, A286–A287. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, R.J. Non-cigarette tobacco products: What have we learnt and where are we headed? Tob. Control. 2012, 21, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Chun, L.F.; Moazed, F.; Calfee, C.S.; Matthay, M.A.; Gotts, J.E. Pulmonary toxicity of e-cigarettes. Am. J. Physiol. Lung Cell. Mol. Physiol. 2017, 313, L193–L206. [Google Scholar] [CrossRef]
- Carroll, A.J.; Labarthe, D.R.; Huffman, M.D.; Hitsman, B. Global tobacco prevention and control in relation to a cardiovascular health promotion and disease prevention framework: A narrative review. Prev. Med. 2016, 93, 189–197. [Google Scholar] [CrossRef] [Green Version]
- Dutra, L.M.; Glantz, S.A. E-cigarettes and conventional cigarette use among us adolescents: A cross-sectional study. JAMA Pediatrics 2014, 168, 610–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhattacharyya, N. Trends in the use of smokeless tobacco in united states, 2000–2010. Laryngoscope 2012, 122, 2175–2178. [Google Scholar] [CrossRef]
- Bao, W.; Liu, B.; Du, Y.; Snetselaar, L.G.; Wallace, R.B. Electronic cigarette use among young, middle-aged, and older adults in the united states in 2017 and 2018. JAMA Intern. Med. 2019, 180, 313–314. [Google Scholar] [CrossRef]
- Syamlal, G.; Jamal, A.; King, B.A.; Mazurek, J.M. Electronic cigarette use among working adults—United States, 2014. Mmwr. Morb. Mortal. Wkly. Rep. 2016, 65, 557–561. [Google Scholar] [CrossRef]
- Wilson, F.A.; Wang, Y. Recent findings on the prevalence of e-cigarette use among adults in the U.S. Am. J. Prev. Med. 2017, 52, 385–390. [Google Scholar] [CrossRef]
- Hu, S.; Homa, D.; Wang, T.; Gomez, Y.; Walton, K.; Lu, H.; Neff, L. State-specific patterns of cigarette smoking, smokeless tobacco use, and e-cigarette use among adults—United states, 2016. Prev. Chronic Dis. 2019, 16. [Google Scholar] [CrossRef] [Green Version]
- Salloum, R.G.; Thrasher, J.F.; Kates, F.R.; Maziak, W. Water pipe tobacco smoking in the united states: Findings from the national adult tobacco survey. Prev. Med. 2015, 71, 88–93. [Google Scholar] [CrossRef] [Green Version]
- Bowler, R.P.; Hansel, N.N.; Jacobson, S.; Graham Barr, R.; Make, B.J.; Han, M.K.; O’Neal, W.K.; Oelsner, E.C.; Casaburi, R.; Barjaktarevic, I.; et al. Electronic cigarette use in us adults at risk for or with copd: Analysis from two observational cohorts. J. Gen. Intern. Med. 2017, 32, 1315–1322. [Google Scholar] [CrossRef] [Green Version]
- Xie, Z.; Ossip, D.J.; Rahman, I.; Li, D. Use of electronic cigarettes and self-reported chronic obstructive pulmonary disease diagnosis in adults. Nicotine Tob Res. 2020, 22, 1155–1161. [Google Scholar] [CrossRef]
- Asch, D.A.; Jedrziewski, M.K.; Christakis, N.A. Response rates to mail surveys published in medical journals. J. Clin. Epidemiol. 1997, 50, 1129–1136. [Google Scholar] [CrossRef]
- Glassberg, A.E.; Luce, J.M.; Matthay, M.A. Reasons for nonenrollment in a clinical trial of acute lung injury. Chest. 2008, 134, 719–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Rompaey, B.; Elseviers, M.M.; Schuurmans, M.J.; Shortridge-Baggett, L.M.; Truijen, S.; Bossaert, L. Risk factors for delerium in intensive care patients: A prospective cohort study. Crit. Care. 2009, 13, R77. [Google Scholar] [CrossRef] [Green Version]
- Chlan, L.; Guttormson, J.; Tracy, M.F.; Bremer, K.L. Strategies for overcoming site and recruitment challenges in research studies based in intensive care units. Am. J. Crit. Care. 2009, 18, 410–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berkman, C.S.; Leipzig, R.M.; Greenberg, S.A.; Inouye, S.K. Methodologic issues in conducting research on hospitalized older people. J. Am. Geriatr. Soc. 2001, 49, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Services DoHaH. Protection of human subjects. Code of Federal Regulations. 15 January 2009. Available online: https://www.hhs.gov/ohrp/sites/default/files/ohrp/humansubjects/regbook2013.pdf.pdf (accessed on 11 November 2020).
- Zhang, M.; Hsu, R.; Hsu, C.-Y.; Kordesch, K.; Nicasio, E.; Cortez, A.; McAlpine, I.; Brady, S.; Zhuo, H.; Kangelaris, K.N.; et al. FGF-23 and PTH levels in patients with acute kidney injury: A cross-sectional case series study. Ann. Intensive Care 2011, 1, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agrawal, A.; Matthay, M.A.; Kangelaris, K.N.; Stein, J.; Chu, J.C.; Imp, B.M.; Cortez, A.; Abbott, J.; Liu, K.D.; Calfee, C.S. Plasma angiopoietin-2 predicts the onset of acute lung injury in critically ill patients. Am. J. Respir. Crit. Care Med. 2013, 187, 736–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kangelaris, K.N.; Prakash, A.; Liu, K.D.; Aouizerat, B.; Woodruff, P.G.; Erle, D.J.; Rogers, A.; Seeley, E.J.; Chu, J.; Liu, T.; et al. Increased expression of neutrophil-related genes in patients with early sepsis-induced ards. Am. J. Physiol. Lung Cell. Mol. Physiol. 2015, 308, L1102–L1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinert, D.F.; Allen, J.P. The alcohol use disorders identification test: An update of research findings. Alcohol. Clin. Exp. Res. 2007, 31, 185–199. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, S.J.; Zhuo, H.; Benowitz, N.L.; Thompson, B.T.; Liu, K.D.; Matthay, M.A.; Calfee, C.S.; NLHBI ARDS Network. Prevalence and impact of active and passive cigarette smoking in acute respiratory distress syndrome. Crit. Care Med. 2014, 42, 2058–2068. [Google Scholar] [CrossRef] [PubMed]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Soulakova, J.N.; Crockett, L.J. Consistency and recanting of ever-smoking status reported by self and proxy respondents one year apart. J. Addict. Behav. Ther. Rehabil. 2014, 3, 1000113. [Google Scholar]
- Knaus, W.A.; Wagner, D.P.; Draper, E.A.; Zimmerman, J.E.; Bergner, M.; Bastos, P.G.; Sirio, C.A.; Murphy, D.J.; Lotring, T.; Damiano, A.; et al. The APACHE III prognostic system. Chest 1991, 100, 1619–1636. [Google Scholar] [CrossRef] [Green Version]
- Cook, D.J. Enrollment of intensive care unit patients into clinical studies: A trinational survey of researchers’ experiences, beliefs, and practices. Crit. Care Med. 2008, 36, 2100–2105. [Google Scholar] [CrossRef]
- Kasza, K.A.; Ambrose, B.K.; Conway, K.P.; Borek, N.; Taylor, K.; Goniewicz, M.L.; Cummings, K.M.; Sharma, E.; Pearson, J.L.; Green, V.R.; et al. Tobacco-product use by adults and youths in the united states in 2013 and 2014. N. Engl. J. Med. 2017, 376, 342–353. [Google Scholar] [CrossRef] [Green Version]
- Majeed, B.A.; Sterling, K.L.; Weaver, S.R.; Pechacek, T.F.; Eriksen, M.P. Prevalence and harm perceptions of hookah smoking among u.S. Adults, 2014–2015. Addict. Behav. 2017, 69, 78–86. [Google Scholar] [CrossRef]
- Hiratsuka, V.Y.; Avey, J.P.; Trinidad, S.B.; Beans, J.A.; Robinson, R.F. Views on electronic cigarette use in tobacco screening and cessation in an alaska native healthcare setting. Int. J. Circumpolar Health 2015, 74. [Google Scholar] [CrossRef] [PubMed]
- Grana, R.; Benowitz, N.; Glantz, S.A. E-cigarettes: A scientific review. Circulation 2014, 129, 1972–1986. [Google Scholar] [CrossRef] [PubMed]
- Bascombe, T.M.S.; Scott, K.N.; Ballard, D.; Smith, S.A.; Thompson, W.; Berg, C.J. Primary healthcare provider knowledge, beliefts and clinic-based practives regarding alternative tobacco products and marijuana: A qualitative study. Health Educ. Res. 2016, 31, 375–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benowitz, N.L.; Hukkanen, J.; Jacob, P. Nicotine chemistry, metabolism, kinetics and biomarkers. Handb. Exp. Pharm. 2009, 192, 29–60. [Google Scholar]
- Calfee, C.S.; Gallagher, D.; Abbott, J.; Thompson, B.T.; Matthay, M.A.; NHLBI ARDS Network. Plasma angiopoietin-2 in clinical acute lung injury: Prognostic and pathogenetic significance. Crit. Care Med. 2012, 40, 1731–1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breslin, E.; Hanafin, J.; Clancy, L. It’s not all about price: Factors associated with roll-your-own tobacco use among young people-a qualitative study. BMC Public Health 2018, 18, 991. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Hospital A (n = 465) | Hospital B (n = 68) | p-Value | Overall (n = 533) |
|---|---|---|---|---|
| Survey Completion | 368 (79) | 57 (84) | 0.37 | 425 (80) |
| Age, mean ± SD | 66 ± 16 | 63 ± 13 | 0.32 | 65 ± 16 |
| Male | 257 (55) | 41 (60) | 0.65 | 298 (56) |
| Race | 0.002 * | |||
| African American | 60 (13) | 16 (24) | 76 (14) | |
| Asian | 132 (28) | 11 (16) | 143 (27) | |
| Caucasian | 217 (47) | 25 (37) | 242 (45) | |
| Other | 56 (12) | 16 (24) | 72 (14) | |
| Hispanic | 49 (11) | 15 (22) | 0.01 * | 64 (12) |
| Insurance | 0.03 * | |||
| Medicaid | 92 (20) | 22 (32) | 114 (21) | |
| Medicare | 237 (51) | 35 (51) | 272 (51) | |
| Private Insurance | 128 (27) | 10 (15) | 134 (25) | |
| None | 10 (2) | 0 (0) | 10 (2) | |
| Other | 2 (0) | 1 (1) | 3 (1) | |
| Cigarette Smoking History (Chart) | 0.004 * | |||
| Current Cigarette Smoker | 56 (12) | 19 (28) | 75 (14) | |
| Former Cigarette Smoker | 163 (35) | 21 (31) | 184 (35) | |
| Never Cigarette Smoker | 217 (47) | 23 (34) | 240 (45) | |
| Unknown | 29 (6) | 5 (7) | 34 (6) | |
| Cigarette Smoking History (Survey) ** | 0.002 * | |||
| Current Cigarette Smoker | 43 (12) | 15 (26) | 58 (14) | |
| Former Cigarette Smoker | 135 (37) | 24 (42) | 159 (38) | |
| Never Cigarette Smoker | 189 (52) | 18 (32) | 207 (49) | |
| Poly-ATP Use (Survey) ** | 35 (10) | 8 (14) | 0.30 | 43 (10) |
| Variable | ATP User (n = 44) | Non-User (n = 215) | p-Value |
|---|---|---|---|
| Hospital A vs. Hospital B | 0.04 * | ||
| Hospital A | 35 (80) | 197 (90) | |
| Hospital B | 9 (20) | 18 (10) | |
| Enrolled to Hospital Floor or ICU | 0.33 | ||
| Hospital Floor | 10 (23) | 65 (30) | |
| ICU | 34 (77) | 150 (70) | |
| Age, mean ± SD | 57 ± 17 | 62 ± 14 | 0.08 |
| Male | 36 (82) | 128 (59) | 0.01 * |
| Race | 0.11 | ||
| African American | 7 (16) | 33 (15) | |
| Asian | 2 (5) | 46 (21) | |
| Caucasian | 28 (64) | 107 (50) | |
| Other | 7 (15) | 29 (14) | |
| Insurance | 0.19 | ||
| Medicaid | 12 (27) | 51 (24) | |
| Medicare | 24 (55) | 101 (46) | |
| Private Insurance | 6 (14) | 61 (28) | |
| None | 1 (2) | 3 (1) | |
| Other | 1 (2) | 2 (1) | |
| Chronic Heart Disease | 9 (20) | 45 (21) | 0.94 |
| Cerebrovascular Disease | 3 (7) | 10 (5) | 0.47 |
| Chronic Lung Disease | 12 (27) | 62 (29) | 0.83 |
| Solid Tumor Malignancy | 9 (20) | 55 (25) | 0.51 |
| Cigarette Smoking History (Survey) | <0.001 * | ||
| Current Cigarette Smoker | 18 (41) | 25 (12) | |
| Former Cigarette Smoker | 19 (43) | 73 (34) | |
| Never Cigarette Smoker | 7 (16) | 116 (54) | |
| Alcohol Use | 22 (51) | 55 (27) | 0.001 * |
| Alcohol Abuse | 7 (16) | 10 (5) | 0.008 * |
| Clinical Outcomes, ICU Patients | |||
| In-hospital Mortality | 1 (3) | 14 (9) | 0.31 |
| APACHE III, mean ± SD | 77 ± 29 | 76 ± 29 | 0.8 |
| Clinical Outcomes, Floor Patients | |||
| In-hospital Mortality | 1 (10) | 3 (5) | 0.44 |
| APACHE III, mean ± SD | 39 ± 19 | 47 ± 24 | 0.25 |
| Variable | Self-Responder (n = 259) | Surrogate Responder (n = 166) | p-Value |
|---|---|---|---|
| Current ATP Use, n (%) | 44 (17) | 8 (5) | <0.001 * |
| Poly-ATP Use | 21 (8) | 2 (1) | 0.01 * |
| Smokeless Tobacco ++ | 10 (4) | 2 (1) | 0.18 |
| Electronic Cigarettes +++ | 13 (5) | 4 (2) | 0.26 |
| Cigars + | 23 (9) | 4 (2) | 0.01 * |
| Little Cigars + | 11 (4) | 2 (1) | 0.08 |
| Pipe + | 15 (6) | 2 (1) | 0.04 * |
| Hookah + | 8 (3) | 1 (1) | 0.16 |
| Variable | EARLI (n = 425) | PATH (n = 32,320) | p-Value | NHIS (n = 36,697) | p-Value | TPRPS (n = 11,708) | p-Value |
|---|---|---|---|---|---|---|---|
| Electronic Cigarettes +++ | 17 (4) | 1616 (5) | 0.38 | 1395 (3.8) | 0.83 | - | - |
| Cigars + | 27 (6.4) | 1907 (5.9) | 0.69 | - | - | - | - |
| Cigarillos + | 6 (1.4) | 1099 (3.4) | 0.02 * | - | - | - | - |
| Hookah + | 9 (2.1) | 679 (2.1) | 0.98 | - | - | 277 (1.5) | 0.31 |
| Pipe + | 17 (4) | 323 (1) | <0.001 * | - | - | - | - |
| Smokeless Tobacco ++ | 12 (2.8) | 1002 (3.1) | 0.74 | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, T.; Deiss, T.J.; Lippi, M.W.; Jauregui, A.; Vessel, K.; Ke, S.; Belzer, A.; Zhuo, H.; Kangelaris, K.N.; Gomez, A.D.; et al. Alternative Tobacco Product Use in Critically Ill Patients. Int. J. Environ. Res. Public Health 2020, 17, 8707. https://doi.org/10.3390/ijerph17238707
Liu T, Deiss TJ, Lippi MW, Jauregui A, Vessel K, Ke S, Belzer A, Zhuo H, Kangelaris KN, Gomez AD, et al. Alternative Tobacco Product Use in Critically Ill Patients. International Journal of Environmental Research and Public Health. 2020; 17(23):8707. https://doi.org/10.3390/ijerph17238707
Chicago/Turabian StyleLiu, Tom, Thomas J. Deiss, Matthew W. Lippi, Alejandra Jauregui, Kathryn Vessel, Serena Ke, Annika Belzer, Hanjing Zhuo, Kirsten N. Kangelaris, Antonio D. Gomez, and et al. 2020. "Alternative Tobacco Product Use in Critically Ill Patients" International Journal of Environmental Research and Public Health 17, no. 23: 8707. https://doi.org/10.3390/ijerph17238707
APA StyleLiu, T., Deiss, T. J., Lippi, M. W., Jauregui, A., Vessel, K., Ke, S., Belzer, A., Zhuo, H., Kangelaris, K. N., Gomez, A. D., Matthay, M. A., Liu, K. D., & Calfee, C. S. (2020). Alternative Tobacco Product Use in Critically Ill Patients. International Journal of Environmental Research and Public Health, 17(23), 8707. https://doi.org/10.3390/ijerph17238707