A Moderated-Mediation Model of the Relationship between Dietary Satisfaction and Fatigue in Older Adults with Diabetes: The Role of Meal Planning and Depressive Symptoms


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Variables
2.3. Statistical Analyses
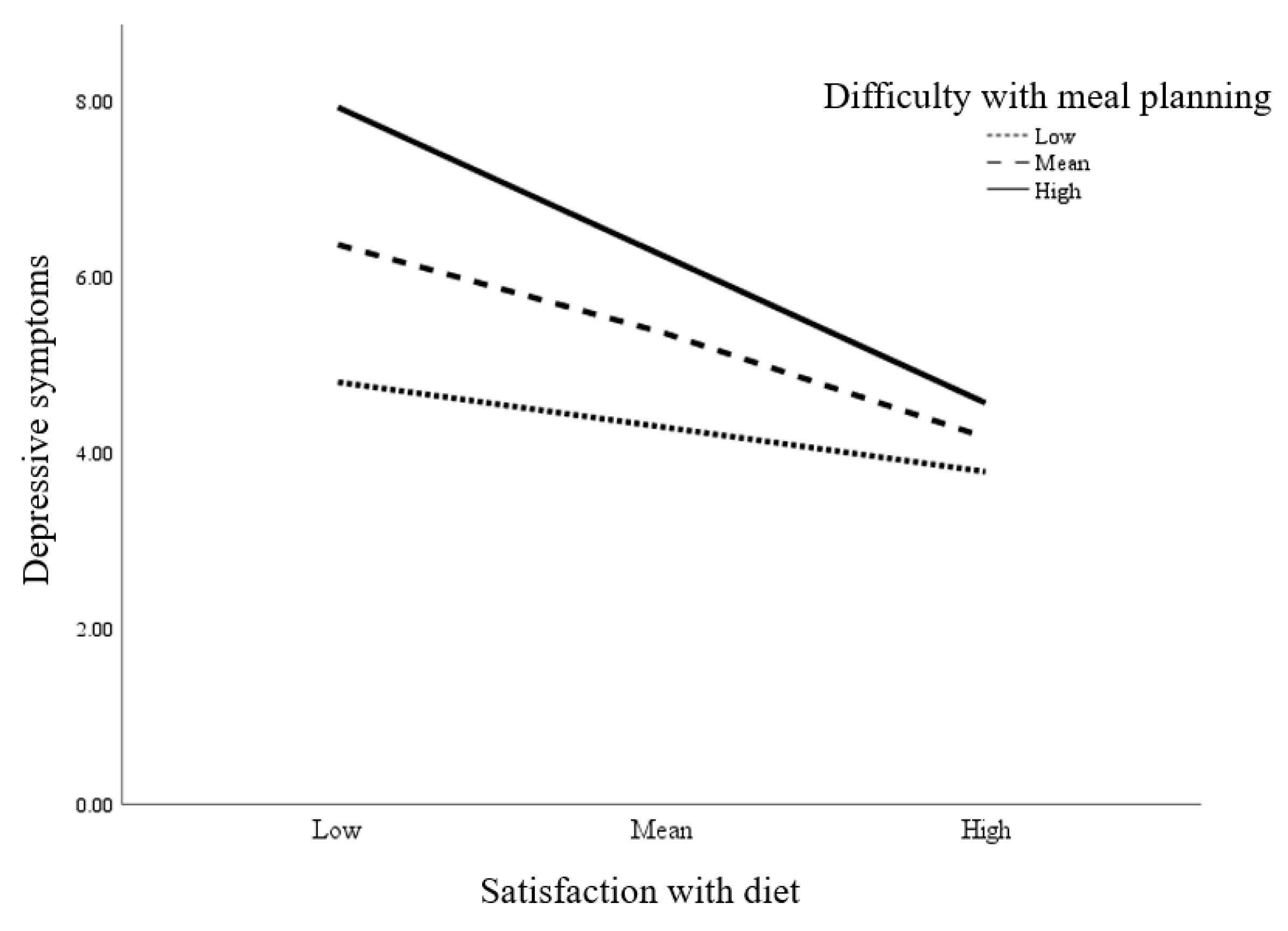
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- International Diabetes Federation (IDF). IDF Diabetes Atlas 2017, 8th ed.; IDF: Brussels, Belgium, 2017; p. 150. [Google Scholar]
- LeRoith, D.; Biessels, G.J.; Braithwaite, S.S.; Casanueva, F.F.; Draznin, B.; Halter, J.B.; Hirsch, I.B.; McDonnell, M.E.; Molitch, M.E.; Nurad, M.H.; et al. Treatment of diabetes in older adults: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metabol. 2019, 104, 1520–1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eldadah, B.A. Fatigue and fatigability in older adults. PMR 2010, 2, 406–413. [Google Scholar] [CrossRef]
- Mills, R.J.; Young, C.A. A medical definition of fatigue in multiple sclerosis. QJM 2008, 101, 49–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, C.A.; Mackey, D.C.; Glynn, N.W.; Ferrucci, L.G. Walking energetics, fatigability, and fatigue in older adults: The study of energy and aging pilot. J. Gerontol A Biol. Sci. Med. Sci. 2014, 70, 487–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritschi, C.; Quinn, L. Fatigue in patients with diabetes: A review. J. Psychosom Res. 2010, 69, 33–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritschi, C.; Quinn, L.; Hacker, E.D.; Penckofer, S.M.; Wang, E.; Foreman, M.; Ferrans, C.E. Fatigue in women with type 2 diabetes. Diabetes Educ. 2012, 38, 662–672. [Google Scholar] [CrossRef] [PubMed]
- Kalra, S.; Sahay, R. Diabetes fatigue syndrome. Diabetes Ther. 2018, 9, 1421–1429. [Google Scholar] [CrossRef] [Green Version]
- Griggs, S.; Morris, N.S. Fatigue among adults with type 1 diabetes mellitus and implications for self-management: An integrative review. Diabetes Educ. 2018, 44, 325–339. [Google Scholar] [CrossRef]
- Burke, S.E.; Samuel, I.B.H.; Zhao, Q.; Cagle, J.; Cohen, R.A.; Kluger, B.; Ding, M. Task-based cognitive fatigability for older adults and validation of mental fatigability subscore of Pittsburgh fatigability scale. Front. Aging Neurosci. 2018, 10, 327327. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Son, H. Fatigue-related factors for community-dwelling older adults with diabetes: A theory-guided multi-dimensional approach using the dynamic biopsychosocial model. Int. J. Environ. Res. Public Health 2019, 16, 4502. [Google Scholar] [CrossRef] [Green Version]
- Soyuer, F.; Şenol, V. Fatigue and physical activity levels of 65 and over older people living in rest home. Int. J. Gerontol. 2011, 5, 13–16. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 1. Improving care and promoting health in populations: Standards of medical care in diabetes—2019. Diabetes Care 2019, 42, S7–S12. [Google Scholar] [CrossRef] [Green Version]
- Egerton, T.; Chastin, S.F.; Stensvold, D.; Helbostad, J.L. Fatigue may contribute to reduced physical activity among older people: An observational study. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 670–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guadagnoli, L.; Mutlu, E.A.; Doerfler, B.; Ibrahim, A.; Brenner, D.; Taft, T.H. Food-related quality of life in patients with inflammatory bowel disease and irritable bowel syndrome. Qual. Life Res. 2019, 28, 2195–2205. [Google Scholar] [CrossRef]
- Sato, E.; Ochiai, R.; Shibayama, T.; Nishigaki, M.; Abe, Y.; Sawa, T.; Suzukama, Y.; Kazuma, K. Reliability and validity of revised and short form versions of diabetes diet-related quality of life scale. Diabetol. Int. 2017, 8, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Delahanty, L.M.; Hayden, D.; Ammerman, A.; Nathan, D.M. Medical nutrition therapy for hypercholesterolemia positively affects patient satisfaction and quality of life outcomes. Ann. Behav. Med. 2002, 24, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Franz, M.J.; MacLeod, J.; Evert, A.; Brown, C.; Gradwell, E.; Handu, D.; Reppert, A.; Robinson, M. Academy of nutrition and dietetics nutrition practice guideline for type 1 and type 2 diabetes in adults: Systematic review of evidence for medical nutrition therapy effectiveness and recommendations for integration into the nutrition care process. J. Acad. Nutr. Diet. 2017, 117, 1659–1679. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.K.; Kristeller, J.L.; Headings, A.; Nagaraja, H. Comparison of a mindful eating intervention to a diabetes self-management intervention among adults with type 2 diabetes: A randomized controlled trial. Health Educ. Behav. 2014, 41, 145–154. [Google Scholar] [CrossRef] [Green Version]
- Weijman, I.; Kant, I.; Swaen, G.M.; Ros, W.J.G.; Rutten, G.E.H.M.; Schaufeli, W.B.; Schabracq, M.J.; Winnubst, J.A.M. Diabetes, employment and fatigue-related complaints: A comparison between diabetic employees, “healthy” employees, and employees with other chronic diseases. J. Occup. Environ. Med. 2004, 46, 828–836. [Google Scholar] [CrossRef] [PubMed]
- Zhu, B.; Martyn-Nemeth, P.; Ruggiero, L.; Park, C.G.; Zhang, Y.; Fritschi, C. Associations between fatigue, sleep disturbance and eating style in adults with type 2 diabetes: A correlational study. J. Clin. Nurs. 2019, 28, 3200–3209. [Google Scholar] [CrossRef] [PubMed]
- Patrick, S.; Connick, P. Psychometric properties of the PHQ-9 depression scale in people with multiple sclerosis: A systematic review. PLoS ONE 2019, 14, e0197943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amtmann, D.; Kim, J.; Chung, H.; Bamer, A.M.; Askew, R.L.; Wu, S.; Cook, K.F.; Johnson, K.L. Comparing CESD-10, PHQ-9, and PROMIS depression instruments in individuals with multiple sclerosis. Rehabil. Psychol. 2014, 59, 220–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huibers, M.J.; Leone, S.S.; van Amelsvoort, L.G.; Kant, I.; Knottnerus, J.A. Associations of fatigue and depression among fatigued employees over time: A 4-year follow-up study. J. Psychosom. Res. 2007, 63, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Teel, C.; Sabus, C.; McGinnis, P.; Kluding, P. Fatigue in type 2 Diabetes: Impact on quality of life and predictors. PLoS ONE 2016, 11, e0165652. [Google Scholar] [CrossRef] [PubMed]
- Moreh, E.; Jacobs, J.M.; Stessman, J. Fatigue, function, and mortality in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65A, 887–895. [Google Scholar] [CrossRef] [PubMed]
- Mänty, M.; Rantanen, T.; Era, P.; Avlund, K. Fatigue and depressive symptoms in older people. J. Appl. Gerontol. 2014, 33, 505–514. [Google Scholar] [CrossRef]
- Jeong, J.; Seo, S. Importance of satisfaction with food for older adults’ quality of life. Br. Food J. 2014, 116, 1276–1290. [Google Scholar] [CrossRef]
- Cattan, M.; White, M.; Bond, J.; Learmouth, A. Preventing social isolation and loneliness among older people: A systematic review of health promotion interventions. Ageing Soc. 2005, 25, 41–67. [Google Scholar] [CrossRef] [Green Version]
- Jain, A.; Sharma, R.; Choudhary, P.K.; Yadav, N.; Jain, G.; Maanju, M. Study of fatigue, depression, and associated factors in type 2 diabetes mellitus in industrial workers. Ind. Psychiatry J. 2015, 24, 179–184. [Google Scholar] [CrossRef]
- Khamseh, M.E.; Baradaran, H.R.; Rajabali, H. Depression and diabetes in Iranian patients: A comparative study. Int. J. Psychiatry Med. 2007, 37, 81–86. [Google Scholar] [CrossRef]
- Song, Y.; Song, H.-J.; Han, H.-R.; Park, S.-Y.; Nam, S.; Kim, M.T. Unmet needs for social support and effects on diabetes self-care activities in Korean Americans with type 2 diabetes. Diabetes Educ. 2012, 38, 77–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale: Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef]
- Singh, R.; Kluding, P.M. Fatigue and related factors in people with type 2 diabetes. Diabetes Educ. 2013, 39, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, J.I.; Yesavage, J.A. Geriatric depression scale (GDS): Recent evidence and development of a shorter version. In Clinical Gerontology: A Guide to Assessment and Intervention; Brink, T.L., Ed.; Haworth Press: Philadelphia, PA, USA, 1986; pp. 165–174. [Google Scholar]
- Jang, Y.; Small, B.J.; Haley, W.E. Cross-cultural comparability of the geriatric depression scale: Comparison between older Koreans and older Americans. Aging Ment. Health 2001, 5, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process. Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017; ISBN 978-1-60918-230-4. [Google Scholar]
- Young-Hyman, D.; de Groot, M.; Hill-Briggs, F.; Gonzalez, J.S.; Hood, K.; Peyrot, M. Psychosocial care for people with diabetes: A position statement of the American Diabetes Association. Diabetes Care 2016, 39, 2126–2140. [Google Scholar] [CrossRef] [Green Version]
- Vesnaver, E.; Keller, H.H.; Payette, H.; Shatenstein, B. Dietary resilience as described by older community-dwelling adults from the NuAge study “If there is a will–there is a way!”. Appetite 2012, 58, 730–738. [Google Scholar] [CrossRef]
- Doherty, T.A.; Barker, L.A.; Denniss, R.; Jalil, A.; Beer, M.D. The cooking task: Making a meal of executive functions. Front. Behav. Neurosci. 2015, 9, 22. [Google Scholar] [CrossRef] [Green Version]
- Locher, J.L.; Ritchie, C.S.; Roth, D.L.; Baker, P.S.; Bodner, E.V.; Allman, R.M. Social isolation, support, and capital and nutritional risk in an older sample: Ethnic and gender differences. Soc. Sci. Med. 2005, 60, 747–761. [Google Scholar] [CrossRef] [Green Version]
- Algren, M.H.; Ekholm, O.; Nielsen, L.; Ersbøll, A.K.; Bak, C.K.; Andersen, P.T. Social isolation, loneliness, socioeconomic status, and health-risk behaviour in deprived neighbourhoods in Denmark: A cross-sectional study. SSM Popul. Health 2020, 10, 100546. [Google Scholar] [CrossRef]
- Conklin, A.I.; Forouhi, N.G.; Surtees, P.; Khaw, K.T.; Wareham, N.J.; Monsivais, P. Social relationships and healthful dietary behaviour: Evidence from over-50s in the EPIC cohort, UK. Soc. Sci. Med. 2014, 100, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Ciechanowski, P.S.; Katon, W.J.; Russo, J.E. Depression and diabetes: Impact of depressive symptoms on adherence, function, and costs. Arch. Intern. Med. 2000, 160, 3278–3285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edfors, E.; Westergren, A. Home-living elderly people’s views on food and meals. J. Aging Res. 2012, 2012, 761291. [Google Scholar] [CrossRef] [Green Version]
- Weijman, I.; Ros, W.J.G.; Rutten, G.E.H.M.; Schaufeli, W.B.; Schabracq, M.J.; Winnubst, J.A.M. Frequency and perceived burden of diabetes self-management activities in employees with insulin-treated diabetes: Relationships with health outcomes. Diabetes Res. Clin. Pract. 2005, 68, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Nanayakkara, N.; Pease, A.; Ranasinha, S.; Wischer, N.; Andrikopoulos, S.; Speight, J.; Andrikopoulos, S.; Zoungas, S. Depression and diabetes distress in adults with type 2 diabetes: Results from the Australian National Diabetes Audit (ANDA) 2016. Sci. Rep. 2018, 8, 7846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, S.E.; Kim, S.; Bishop, A.; Hermann, J. Poor nutritional status among low-income older adults: Examining the interconnection between self-care capacity, food insecurity, and depression. J. Acad. Nutr. Diet 2019, 119, 1687–1694. [Google Scholar] [CrossRef]
- De Morais, C.; Oliveira, B.; Afonso, C.; Lumbers, M.; Raats, M.; de Almeida, M.D.V. Nutritional risk of European elderly. Eur. J. Clin. Nutr. 2013, 67, 1215–1219. [Google Scholar] [CrossRef]
- Holmes, B.A.; Roberts, C.L. Diet quality and the influence of social and physical factors on food consumption and nutrient intake in materially deprived older people. Eur. J. Clin. Nutr. 2011, 65, 538–545. [Google Scholar] [CrossRef] [Green Version]
- Ahlgren, S.S.; Shultz, J.A.; Massey, L.K.; Hicks, B.C.; Wysham, C. Development of a preliminary diabetes dietary satisfaction and outcomes measure for patients with type 2 diabetes. Qual. Life Res. 2004, 13, 819–832. [Google Scholar] [CrossRef]
- Rad, G.S.; Bakht, L.A.; Feizi, A.; Moheb, S. Importance of social support in diabetes care. J. Educ. Health Promot. 2013, 2, 62. [Google Scholar] [CrossRef] [Green Version]
- Drewnowski, A.; Evans, W.J. Nutrition, physical activity, and quality of life in older adults: Summary. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, 89–94. [Google Scholar] [CrossRef] [Green Version]
- Best, R.L.; Appleton, K.M. The consumption of protein-rich foods in older adults: An exploratory focus group study. J. Nutr. Educ. Behav. 2013, 45, 751–755. [Google Scholar] [CrossRef] [Green Version]
- Quandt, S.A.; Chen, H.; Bell, R.A.; Savoca, M.R.; Anderson, A.M.; Leng, X.; Kohrman, T.; Gilbert, G.H.; Arcury, T.A. Food avoidance and food modification practices of older rural adults: Association with oral health status and implications for service provision. Gerontologist 2010, 50, 100–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.H.; Mo, J. The factors influencing meal satisfaction in older adults: A systematic review and meta-analysis. Asian Nurs. Res. 2019, 13, 169–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanley, K. Nutrition considerations for the growing population of older adults with diabetes. Diabetes Spectr. 2014, 27, 29–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorner, B. Position of the American Dietetic Association: Individualized nutrition approaches for older adults in health care communities. J. Am. Diet Assoc. 2010, 110, 1549–1553. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Potential Predictors | Prevalence of Moderate or Severe Fatigue n (%) | Severity of Fatigue M ± SD | p | |
|---|---|---|---|---|
| Sociodemographic Characteristics | ||||
| Age | <75 years | 20 (32.3) | 3.73 ± 1.79 | 0.428 |
| ≥75 years | 42 (67.7) | 4.00 ± 1.81 | ||
| Gender | Men | 27 (43.5) | 3.88 ± 1.57 | 0.937 |
| Women | 35 (56.5) | 3.91 ± 1.94 | ||
| Marital Status | Widowed/divorced/separated | 30 (48.4) | 3.97 ± 1.84 | 0.685 |
| Married/partnered | 32 (51.6) | 3.84 ± 1.78 | ||
| Education | <High School Education | 32 (51.6) | 4.01 ± 2.15 | 0.476 |
| ≥High School Education | 30 (48.4) | 3.78 ± 1.52 | ||
| Household Income | ≤1,000,000 KRW/month | 40 (64.5) | 4.14 ± 1.88 | 0.295 |
| >1,000,000 KRW/month | 22 (35.5) | 3.78 ± 1.76 | ||
| Clinical Characteristics | ||||
| Years Having Diabetes | <10 years | 27 (43.5) | 3.82 ± 1.77 | 0.662 |
| ≥10 years | 35 (56.5) | 3.97 ± 1.84 | ||
| Comorbidities | <2 | 43 (69.4) | 3.98 ± 1.83 | 0.518 |
| ≥2 | 19 (30.6) | 3.76 ± 1.75 | ||
| Psychological Characteristics | ||||
| Difficulty with Meal Planning | Not at All Difficult | 19 (30.6) | 3.45 ± 1.83 | 0.012 |
| Not so Difficult or Somewhat Difficult | 17 (27.4) | 3.78 ± 1.59 | ||
| Very Difficult or Extremely Difficult | 26 (41.9) | 4.56 ± 1.80 | ||
| Satisfaction with Diet | <Median | 38 (61.3) | 4.32 ± 1.74 | 0.004 |
| ≥Median | 24 (38.7) | 3.41 ± 1.75 | ||
| Burden of Diet Therapy | <Median | 34 (54.8) | 4.00 ± 1.74 | 0.525 |
| ≥Median | 28 (45.2) | 3.80 ± 1.87 | ||
| Perceived Merits of Diet Therapy | <Median | 34 (54.8) | 4.03 ± 1.81 | 0.387 |
| ≥Median | 28 (45.2) | 3.75 ± 1.79 | ||
| Depressive symptoms | Not-depressed | 24 (38.7) | 3.40 ± 1.73 | <0.001 |
| Mild Depression | 23 (37.1) | 3.62 ± 1.53 | ||
| Severe Depression | 15 (24.2) | 5.41 ± 1.33 | ||
| Eating Context | ||||
| Exclusively Eating Alone † | No | 41 (66.1) | 3.70 ± 1.73 | 0.037 |
| Yes | 21 (33.9) | 4.44 ± 1.89 | ||
| Eating out | Less than 2 times a week | 48 (77.4) | 4.11 ± 1.81 | 0.028 |
| 3 times or more a week | 14 (22.6) | 3.32 ± 1.66 |
| Depressive Symptoms | Fatigue | ||
|---|---|---|---|
| Model 1 | Model 2 | ||
| Difficulty with Meal Planning | 0.487 * [0.118, 0.855] | 0.328 ** [0.136, 0.519] | 0.232 * [0.049, 0.415] |
| Satisfaction with Diet | −0.292 ** [−0.453, −0.130] | −0.155 *** [−0.239, −0.071] | −0.098 * [−0.180, −0.016] |
| Burden of Dietary Restrictions | 0.021 [−0.137, 0.180] | 0.010 [−0.072, 0.093] | 0.006 [−0.070, 0.083] |
| Perceived Value of Diet Therapy | −0.241 ** [−0.409, −0.072] | 0.013 [−0.074, 0.101] | 0.061 [−0.023, 0.145] |
| Eating Alone | 1.209 [−0.085, 2.504] | 0.541 [−0.131, 1.213] | 0.303 [−0.331, 0.936] |
| Frequency of Eating Out | 0.061 [−0.430, −0.551] | 0.131 [−0.124, 0.386] | 0.119 [−0.118, 0.356] |
| Depressive symptoms | 0.197 *** [0.110, 0.284] | ||
| Adjusted R2 | 0.197 | 0.164 | 0.279 |
| R2 change | 0.094 | ||
| F | 6.449 *** | 5.096 *** | 6.986 *** |
| F change | 15.476 *** | ||
| VIF | 1.003–1.090 | 1.004–1.145 | 1.084–1.438 |
| Durbin–Watson | 1.718 | 1.180 | |
| p-value | <0.001 | <0.001 | <0.001 |
| Depressive Symptoms | |||||||
|---|---|---|---|---|---|---|---|
| b | SE(b) | t | p | 95% CI (Lower, Upper) | △R2 | p | |
| Satisfaction with Diet | −0.316 | 0.084 | −3.780 | <0.001 | −0.481, −0.150 | ||
| Difficulty with Meal Planning | 0.621 | 0.184 | 3.376 | 0.001 | 0.25, 0.984 | ||
| Satisfaction with Diet * Difficulty with Meal Planning | −0.107 | 0.052 | −2.058 | 0.042 | −0.211, −0.004 | 0.028 | <0.001 |
| Moderated by Difficulty with Meal Planning * | |||||||
| Low Difficulty with Meal Planning | −0.147 | 0.112 | −1.306 | 0.194 | −0.369, 0.076 | ||
| Mean Difficulty with Meal Planning | −0.316 | 0.083 | −3.780 | <0.001 | −0.481, −0.150 | ||
| High Difficulty with Meal Planning | −0.484 | 0.122 | −3.982 | <0.001 | −0.725, −0.244 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Son, H. A Moderated-Mediation Model of the Relationship between Dietary Satisfaction and Fatigue in Older Adults with Diabetes: The Role of Meal Planning and Depressive Symptoms. Int. J. Environ. Res. Public Health 2020, 17, 8823. https://doi.org/10.3390/ijerph17238823
Kim H, Son H. A Moderated-Mediation Model of the Relationship between Dietary Satisfaction and Fatigue in Older Adults with Diabetes: The Role of Meal Planning and Depressive Symptoms. International Journal of Environmental Research and Public Health. 2020; 17(23):8823. https://doi.org/10.3390/ijerph17238823
Chicago/Turabian StyleKim, Hyerang, and Heesook Son. 2020. "A Moderated-Mediation Model of the Relationship between Dietary Satisfaction and Fatigue in Older Adults with Diabetes: The Role of Meal Planning and Depressive Symptoms" International Journal of Environmental Research and Public Health 17, no. 23: 8823. https://doi.org/10.3390/ijerph17238823
APA StyleKim, H., & Son, H. (2020). A Moderated-Mediation Model of the Relationship between Dietary Satisfaction and Fatigue in Older Adults with Diabetes: The Role of Meal Planning and Depressive Symptoms. International Journal of Environmental Research and Public Health, 17(23), 8823. https://doi.org/10.3390/ijerph17238823