Self-Isolation Due to COVID-19 Is Linked to Small One-Year Changes in Depression, Sleepiness, and Insomnia: Results from a Clinic for Sleep Disorders in Shiga Prefecture, Japan

 , , ,
, , , 
Abstract
:1. Introduction
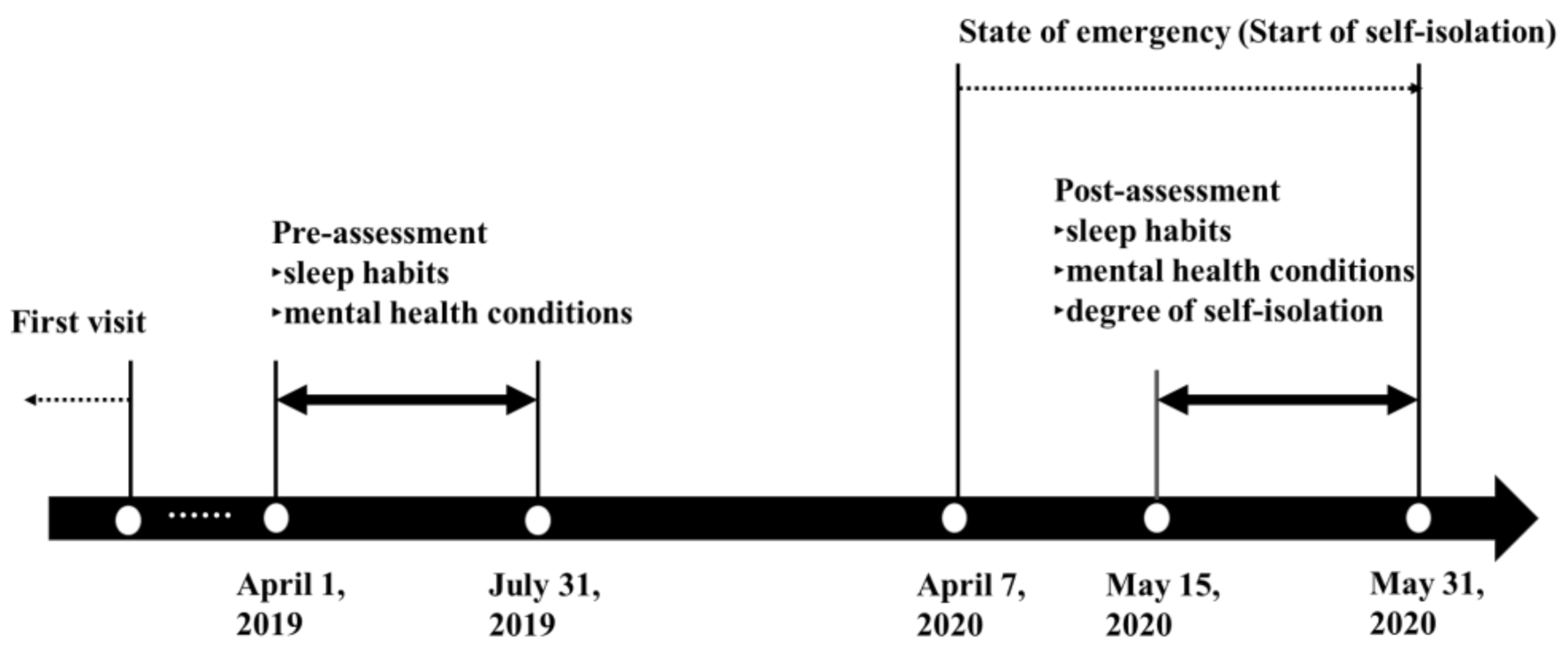
2. Materials and Methods
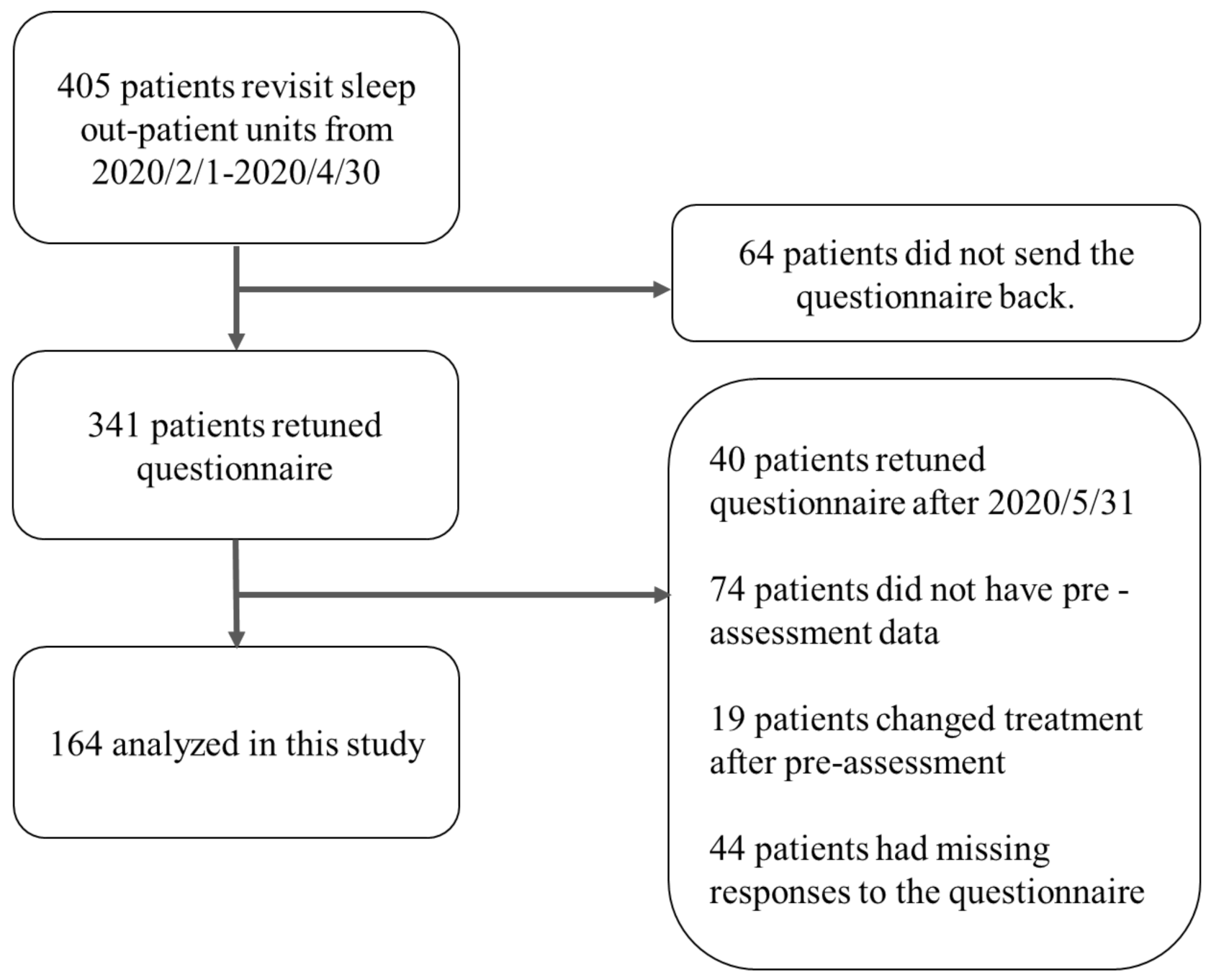
2.1. Participants
2.2. Measures
2.2.1. Degree of Self-Isolation
2.2.2. Changes in Lifestyle
2.2.3. Mental Health Conditions
2.3. Statistical Analysis
2.4. Ethical Considerations
3. Results
3.1. Participants
3.2. Changes in Sleep Habits, Depression, Sleepiness, and Insomnia
3.3. Effects of Changes in Sleep Habits and Social Interactions on Depression, Insomnia, and Sleepiness
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Altena, E.; Baglioni, C.; Espie, C.A.; Ellis, J.; Gavriloff, D.; Holzinger, B.; Schlarb, A.; Frase, L.; Jernelöv, S.; Riemann, D. Dealing with sleep problems during home confinement due to the COVID-19 outbreak: Practical recommendations from a task force of the European CBT-I Academy. J. Sleep Res. 2020, 4, e13052. [Google Scholar] [CrossRef]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]
- Serafini, G.; Parmigiani, B.; Amerio, A.; Aguglia, A.; Sher, L.; Amore, M. The psychological impact of COVID-19 on the mental health in the general population. QJM 2020, 113, 531–537. [Google Scholar] [CrossRef]
- Wang, J.; Wang, J.X.; Yang, G.S. The psychological impact of COVID-19 on Chinese individuals. Yonsei Med. J. 2020, 61, 438–440. [Google Scholar] [CrossRef]
- Zhou, J.; Liu, L.; Xue, P.; Yang, X.; Tang, X. Mental health response to the COVID-19 outbreak in China. Am. J. Psychiatry 2020, 177, 7. [Google Scholar] [CrossRef]
- Cabinet Secretariat. COVID-19 Information and Resources. 2020. Available online: https://corona.go.jp/en/ (accessed on 8 June 2020).
- Shiga Prefecture. A Message from the Governor of Shiga Prefecture. Available online: https://www.pref.shiga.lg.jp/ippan/kenkouiryouhukushi/yakuzi/ (accessed on 5 October 2020).
- Baglioni, C.; Battagliese, G.; Feige, B.; Spiegelhalder, K.; Nissen, C.; Voderholzer, U.; Lombardo, C.; Riemann, D. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect. Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef]
- Takami, M.; Kadotani, H.; Nishikawa, K.; Sumi, Y.; Nakabayashi, T.; Fujii, Y.; Matsuo, M.; Yamada, N.; The NinjaSleep Study Group. Quality of life, depression, and productivity of city government employees in Japan: A comparison study using the Athens insomnia scale and insomnia severity index. Sleep Sci. Pr. 2018, 2, 4. [Google Scholar]
- Leone, M.J.; Sigman, M.; Golombek, D.A. Effects of lockdown on human sleep and chronotype during the COVID-19 pandemic. Curr. Biol. 2020, 30, R930–R931. [Google Scholar] [CrossRef]
- Djernes, J.K. Prevalence and predictors of depression in populations of elderly: A review. Acta Psychiatr. Scand. 2006, 113, 372–387. [Google Scholar] [CrossRef]
- Hom, M.A.; Chu, C.; Rogers, M.L.; Joiner, T.E. A meta-analysis of the relationship between sleep problems and loneliness. Clin. Psychol. Sci. 2020, 8, 799–824. [Google Scholar] [CrossRef]
- Kadotani, H.; Nagai, Y.; Sozu, T. Railway suicide attempts are associated with amount of sunlight in recent days. J. Affect. Disord. 2014, 152, 162–168. [Google Scholar] [CrossRef]
- Okawa, M.; Shirakawa, S.; Uchiyama, M.; Oguri, M.; Kohsaka, M.; Mishima, K.; Sakamoto, K.; Inoue, H.; Kamei, K.; Takahashi, K. Seasonal variation of mood and behaviour in a healthy middle-aged population in Japan. Acta Psychiatr. Scand. 1996, 94, 211–216. [Google Scholar] [CrossRef]
- Muramatsu, K.; Miyaoka, H.; Kamijima, K.; Muramatsu, Y.; Yoshida, M.; Otsubo, T.; Gejyo, F. The Patient Health Questionnaire, Japanese version: Validity according to the Mini-International Neuropsychiatric Interview-Plus. Psychol. Rep. 2007, 101, 952–960. [Google Scholar]
- Takegami, M.; Suzukamo, Y.; Wakita, T.; Noguchi, H.; Chin, K.; Kadotani, H.; Inoue, Y.; Oka, Y.; Nakamura, T.; Green, J.; et al. Development of a Japanese version of the Epworth Sleepiness Scale (JESS) based on item response theory. Sleep Med. 2009, 10, 556–565. [Google Scholar] [CrossRef]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. The diagnostic validity of the Athens Insomnia Scale. J. Psychosom. Res. 2003, 55, 263–267. [Google Scholar] [CrossRef]
- Okajima, I.; Nakajima, S.; Kobayashi, M.; Inoue, Y. Development and validation of the Japanese version of the Athens Insomnia Scale. Psychiatry Clin. Neurosci. 2013, 67, 420–425. [Google Scholar] [CrossRef]
- National Police Agency, Japan. Number of Monthly Suicides in 2020. Available online: https://www.npa.go.jp/safetylife/seianki/jisatsu/R02/202009sokuhouti.pdf (accessed on 20 October 2020). (In Japanese).
- Mann, J.J.; Metts, A.V. The economy and suicide: Aninteraction of societal and intrapersonal risk factors. Crisis 2017, 38, 141–146. [Google Scholar] [CrossRef]
- Jiménez, Ó.; Sánchez-Sánchez, L.C.; García-Montes, J.M. Psychological impact of COVID-19 confinement and its relationship with meditation. Int. J. Environ. Res. Public Health 2020, 17, 6642. [Google Scholar] [CrossRef]
- Cellini, N.; Canale, N.; Mioni, G.; Costa, S. Changes in sleep pattern, sense of time and digital media use during COVID-19 lockdown in Italy. J. Sleep Res. 2020, 29, e13074. [Google Scholar] [CrossRef]
- Lee, P.H.; Marek, J.; Nálevka, P. Crowdsourced smartphone data reveal altered sleep/wake pattern in quarantined Chinese during the COVID-19 outbreak. Chronobiol. Int. 2020, 37, 1181–1190. [Google Scholar] [CrossRef]
- OECD. Gender Data Portal. 2020. Available online: https://www.oecd.org/gender/data/OECD_1564_TUSupdatePortal.xlsx (accessed on 6 October 2020).
- Matsuo, M.; Masuda, F.; Sumi, Y.; Takahashi, M.; Yamada, N.; Ohira, M.H.; Fujiwara, K.; Kanemura, T.; Kadotani, H. Comparisons of portable sleep monitors of different modalities: Potential as naturalistic sleep recorders. Front. Neurol. 2016, 7, 110. [Google Scholar] [CrossRef]
- Voitsidis, P.; Gliatas, I.; Bairachtari, V.; Papadopoulou, K.; Papageorgiou, G.; Parlapani, E.; Syngelakis, M.; Holeva, V.; Diakogiannis, I. Insomnia during the COVID-19 pandemic in a Greek population. Psychiatry Res. 2020, 289, 113076. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Pre | Post | Z | p-Value | ||
|---|---|---|---|---|---|---|
| Median | Median | |||||
| No/little self-isolation (N = 92) | ||||||
| Wake up time (hh:mm) | 6:00 | (5:00–6:30) | 6:00 | (5:05–7:00) | 29.00 | 0.938 |
| Bedtime (hh:mm) | 23:00 | (22:00–24:00) | 23:00 | (22:00–24:00) | 20.00 | 0.009 |
| Total sleep time (hh:mm) | 6:00 | (5:07–7:30) | 6:30 | (5:37–7:30) | 37.00 | 0.749 |
| Sleep onset latency (min) | 10 | (5–20) | 10 | (5–20) | 33.00 | 0.460 |
| PHQ–9 | 2.00 | (1.00–5.00) | 3.00 | (0.25–6.00) | 36.00 | 0.540 |
| ESS | 6.00 | (4.00–8.75) | 6.00 | (3.00–8.00) | 28.00 | 0.013 |
| AIS | 3.00 | (1.00–6.00) | 3.00 | (2.00–6.00) | 42.00 | 0.249 |
| Strong self-isolation (N = 72) | ||||||
| Wake up time (hh:mm) | 6:10 | (5:22–7:15) | 6:20 | (5:30–7:15) | 25.00 | 0.713 |
| Bedtime (hh:mm) | 23:30 | (22:00–24:30) | 23:00 | (22:00–24:00) | 11.00 | 0.006 |
| Total sleep time (hh:mm) | 6:00 | (5:30–7:00) | 6:30 | (5:30–7:30) | 37.00 | 0.014 |
| Sleep onset latency (min) | 10 | (5.5–7.5) | 10 | (8.2–30) | 26.00 | 0.306 |
| PHQ-9 | 2.00 | (1.00–6.75) | 2.00 | (0.25–5.00) | 21.00 | 0.057 |
| ESS | 6.00 | (4.00–11.00) | 6.00 | (4.00–8.75) | 26.00 | 0.202 |
| AIS | 4.50 | (2.00–6.00) | 4.00 | (2.00–6.00) | 29.00 | 0.441 |
| Variables | Changes in PHQ-9 | Changes in ESS | Changes in AIS | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Step 1 | p-Value | Step 2 | p-Value | Step 1 | p-Value | Step 2 | p-Value | Step 1 | p-Value | Step 2 | p-Value | |
| Age | 0.262 | 0.025 | 0.171 | 0.068 | 0.009 | 0.938 | 0.023 | 0.846 | 0.171 | 0.144 | −0.025 | 0.770 |
| Sex | −0.197 | 0.091 | −0.002 | 0.987 | −0.169 | 0.168 | −0.077 | 0.526 | −0.241 | 0.041 | −0.125 | 0.151 |
| Degree of social participation | −0.100 | 0.287 | −0.145 | 0.216 | 0.079 | 0.352 | ||||||
| Changes in wake-up time | −0.037 | 0.736 | 0.045 | 0.740 | 0.092 | 0.347 | ||||||
| Changes in bedtime | 0.145 | 0.171 | 0.059 | 0.660 | −0.149 | 0.119 | ||||||
| Changes in total sleep time | 0.287 | 0.034 | 0.280 | 0.101 | −0.337 | 0.005 | ||||||
| Changes in sleep onset latency | 0.069 | 0.588 | −0.200 | 0.210 | 0.106 | 0.356 | ||||||
| Changes in PHQ-9 | - | - | −0.224 | 0.158 | 0.586 | 0.000 | ||||||
| Changes in ESS | −0.143 | 0.158 | - | - | 0.252 | 0.004 | ||||||
| Changes in AIS | 0.725 | 0.000 | 0.489 | 0.004 | - | - | ||||||
| R2 | 0.127 | 0.009 | 0.521 | 0.000 | 0.029 | 0.361 | 0.248 | 0.029 | 0.103 | 0.023 | 0.612 | 0.000 |
| ΔR2 | 0.394 | 0.000 | 0.219 | 0.021 | 0.509 | 0.000 | ||||||
| Variables | Changes in PHQ-9 | Changes in ESS | Changes in AIS | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Step 1 | p-Value | Step 2 | p-Value | Step 1 | p-Value | Step 2 | p-Value | Step 1 | p-Value | Step 2 | p-Value | |
| Age | 0.060 | 0.571 | 0.002 | 0.989 | 0.139 | 0.192 | 0.131 | 0.242 | 0.217 | 0.038 | 0.093 | 0.334 |
| Sex | 0.018 | 0.866 | −0.059 | 0.599 | 0.047 | 0.657 | 0.055 | 0.631 | 0.163 | 0.116 | 0.213 | 0.029 |
| Degree of social participation | −0.058 | 0.626 | 0.095 | 0.426 | 0.303 | 0.003 | ||||||
| Changes in wake-up time | 0.097 | 0.377 | −0.054 | 0.630 | −0.151 | 0.114 | ||||||
| Changes in bedtime | −0.096 | 0.386 | 0.060 | 0.593 | −0.025 | 0.798 | ||||||
| Changes in total sleep time | 0.131 | 0.291 | 0.093 | 0.459 | −0.417 | 0.000 | ||||||
| Changes in sleep onset latency | 0.122 | 0.270 | −0.155 | 0.166 | 0.024 | 0.803 | ||||||
| Changes in PHQ-9 | - | - | 0.173 | 0.121 | 0.190 | 0.048 | ||||||
| Changes in ESS | 0.168 | 0.121 | - | - | 0.008 | 0.937 | ||||||
| Changes in AIS | 0.247 | 0.048 | 0.010 | 0.937 | - | - | ||||||
| R2 | 0.004 | 0.846 | 0.113 | 0.334 | 0.020 | 0.405 | 0.088 | 0.544 | 0.067 | 0.047 | 0.319 | 0.000 |
| ΔR2 | 0.109 | 0.202 | 0.068 | 0.529 | 0.252 | 0.000 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ubara, A.; Sumi, Y.; Ito, K.; Matsuda, A.; Matsuo, M.; Miyamoto, T.; Kadotani, H. Self-Isolation Due to COVID-19 Is Linked to Small One-Year Changes in Depression, Sleepiness, and Insomnia: Results from a Clinic for Sleep Disorders in Shiga Prefecture, Japan. Int. J. Environ. Res. Public Health 2020, 17, 8971. https://doi.org/10.3390/ijerph17238971
Ubara A, Sumi Y, Ito K, Matsuda A, Matsuo M, Miyamoto T, Kadotani H. Self-Isolation Due to COVID-19 Is Linked to Small One-Year Changes in Depression, Sleepiness, and Insomnia: Results from a Clinic for Sleep Disorders in Shiga Prefecture, Japan. International Journal of Environmental Research and Public Health. 2020; 17(23):8971. https://doi.org/10.3390/ijerph17238971
Chicago/Turabian StyleUbara, Ayaka, Yukiyoshi Sumi, Kazuki Ito, Arichika Matsuda, Masahiro Matsuo, Towa Miyamoto, and Hiroshi Kadotani. 2020. "Self-Isolation Due to COVID-19 Is Linked to Small One-Year Changes in Depression, Sleepiness, and Insomnia: Results from a Clinic for Sleep Disorders in Shiga Prefecture, Japan" International Journal of Environmental Research and Public Health 17, no. 23: 8971. https://doi.org/10.3390/ijerph17238971
APA StyleUbara, A., Sumi, Y., Ito, K., Matsuda, A., Matsuo, M., Miyamoto, T., & Kadotani, H. (2020). Self-Isolation Due to COVID-19 Is Linked to Small One-Year Changes in Depression, Sleepiness, and Insomnia: Results from a Clinic for Sleep Disorders in Shiga Prefecture, Japan. International Journal of Environmental Research and Public Health, 17(23), 8971. https://doi.org/10.3390/ijerph17238971