Exposure to Radiofrequency Electromagnetic Field in the High-Frequency Band and Cognitive Function in Children and Adolescents: A Literature Review

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
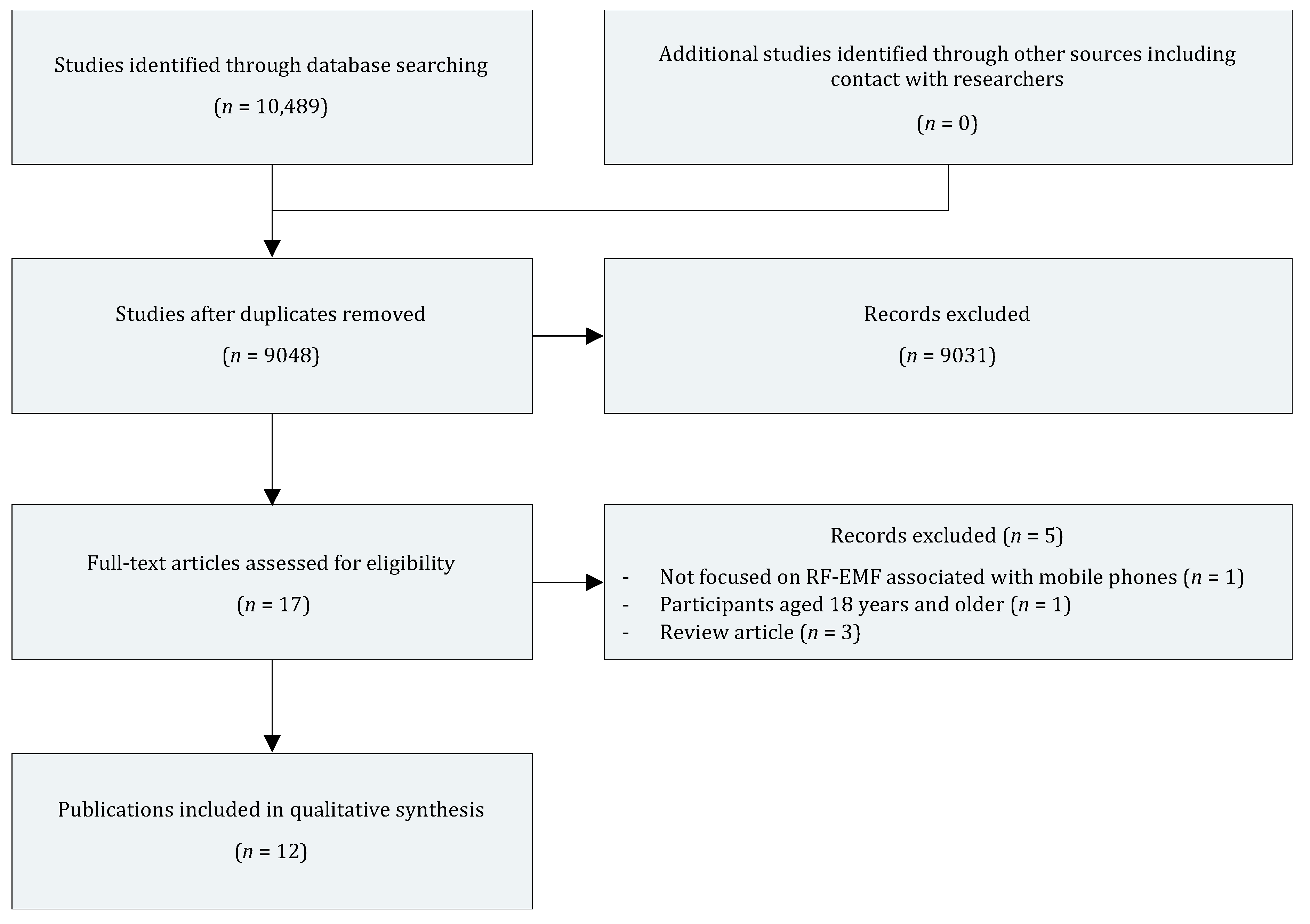
2.3. Screening and Data Extraction
2.4. Quality Assessment
3. Results
3.1. Literature Findings
3.1.1. MoRPhEUS
3.1.2. HERMES
3.1.3. ExPOSURE
3.1.4. ABCD
3.1.5. INMA
3.1.6. Combined Results from DNBC, INMA, and MOCEH
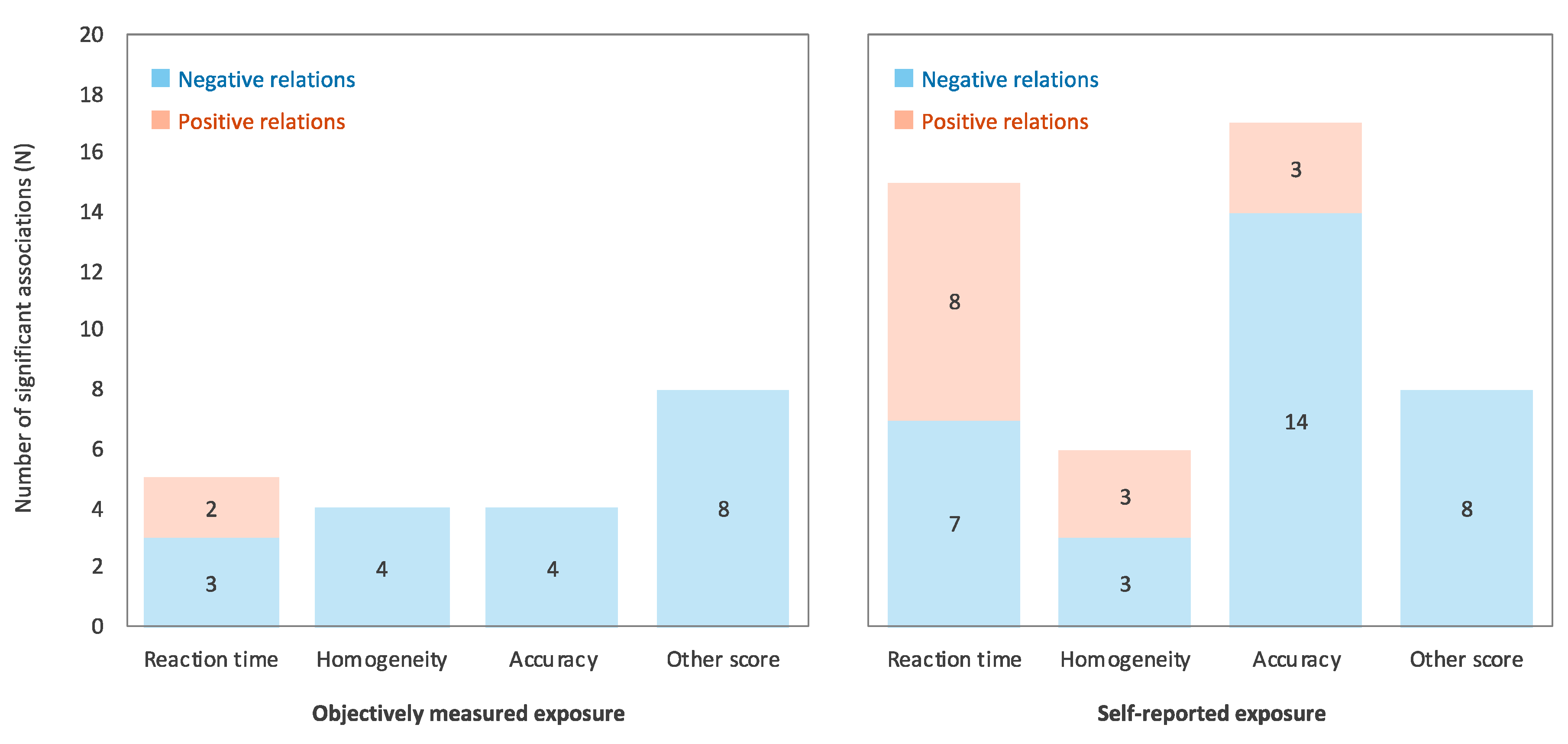
3.1.7. Cross-Sectional Study Using Objective Exposure Measurement
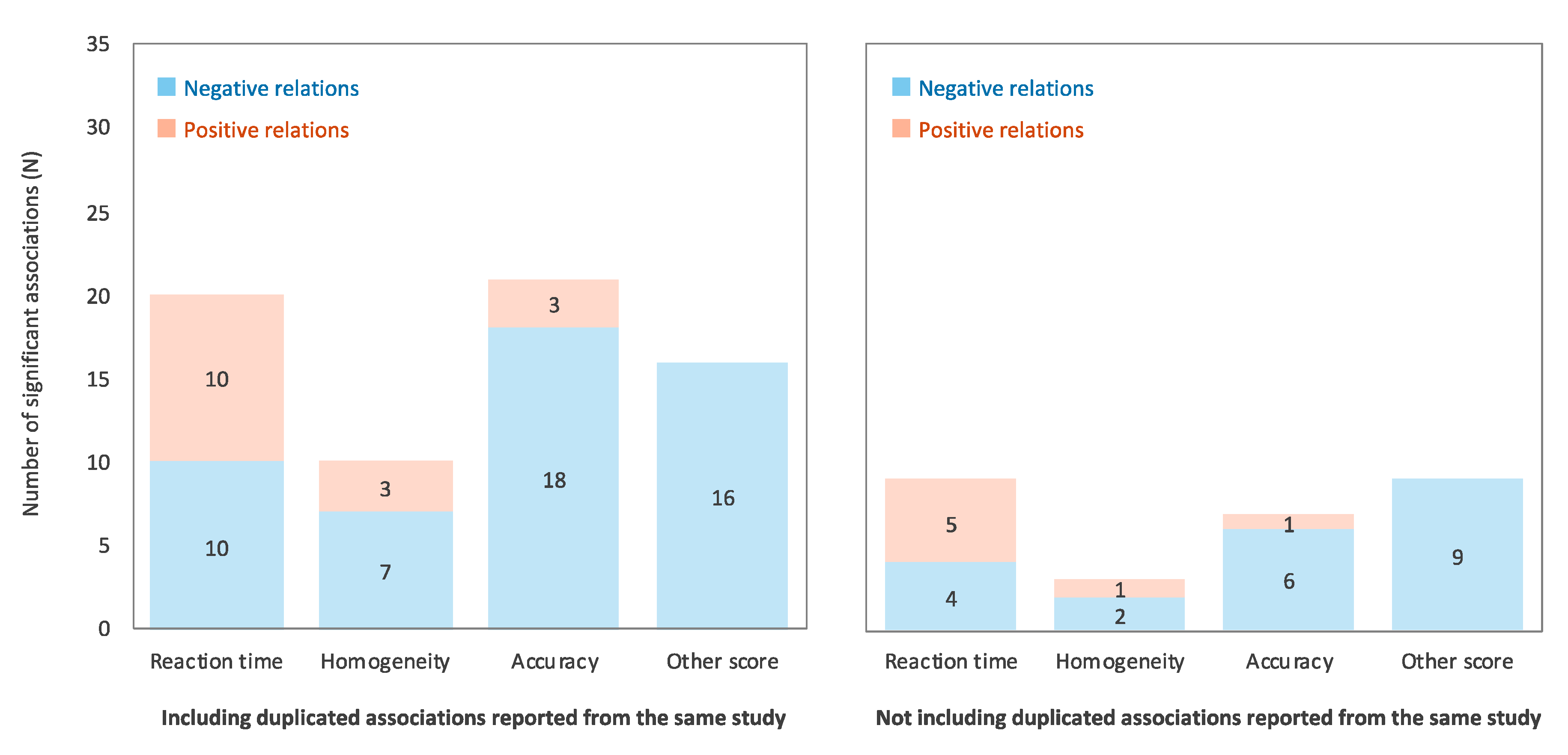
3.1.8. Summary
3.2. Possible Explanations for the Contradictory Results
3.2.1. Familiarity and Training Effects of Computer Usage
3.2.2. Self-Reported Radiofrequency Wave Exposure
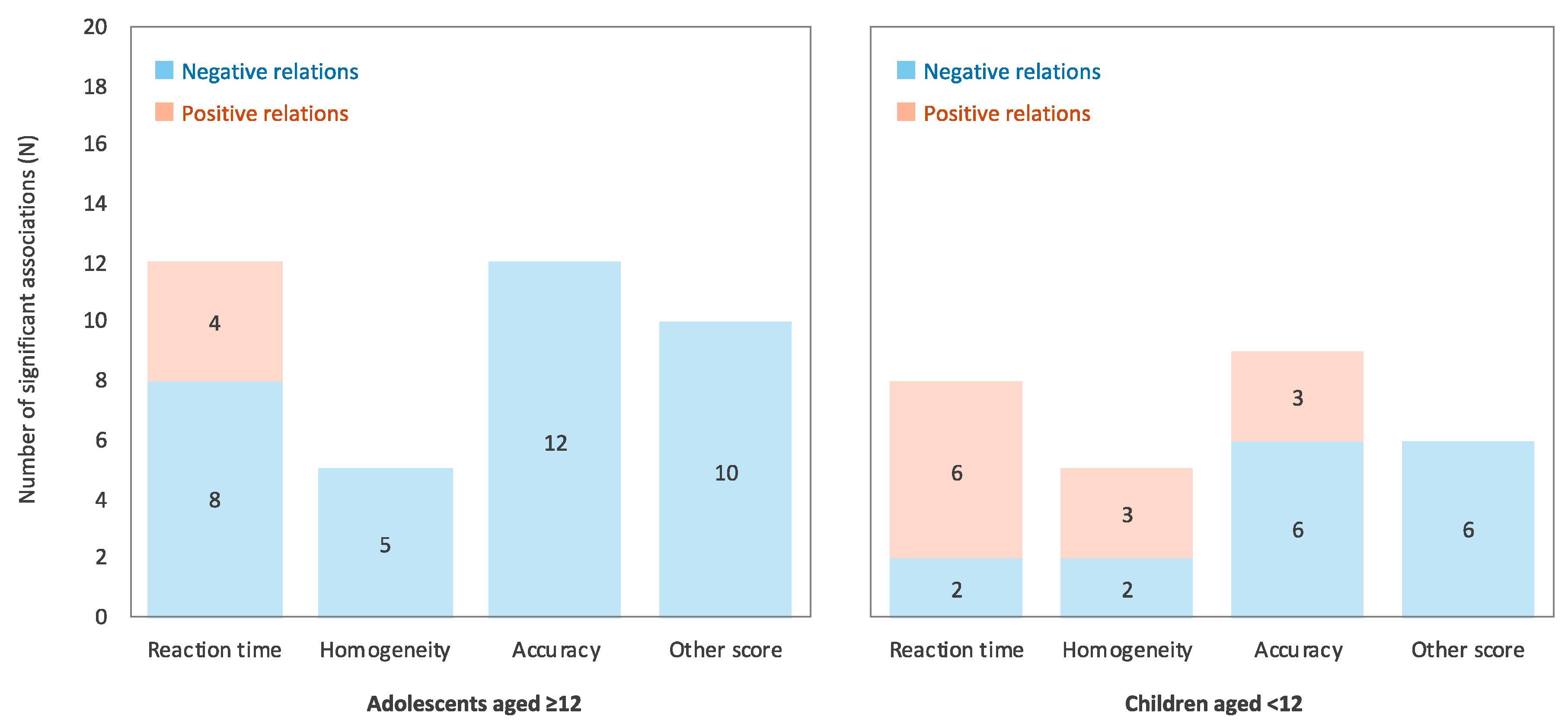
3.2.3. Participants’ Age
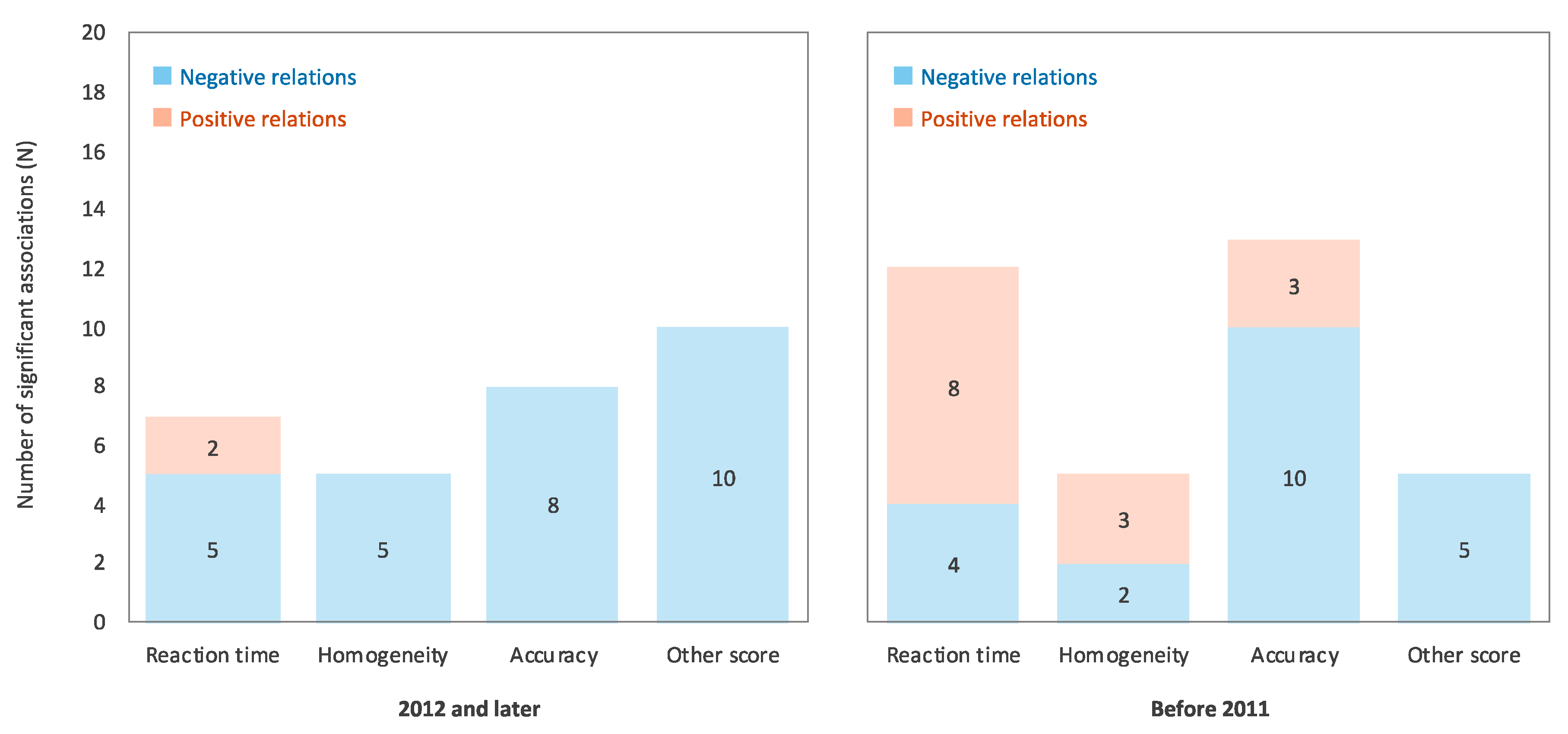
3.2.4. Era of Study Conduction
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Hofferth, S.L.; Moon, U.J. Cell phone use and child and adolescent reading proficiency. Psychol. Pop. Media Cult. 2012, 1, 108–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, F.; Gao, P.; He, M.; Li, M.; Wang, C.; Zeng, Q.; Zhou, Z.; Yu, Z.; Zhang, L. Association between mobile phone use and inattention in 7102 Chinese adolescents: A population-based cross-sectional study. BMC Public Health 2014, 14, 1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Office of Press and Public Relations. In WHO Research Agenda for Radiofrequency Fields; World Health Organization: Geneva, Switzerland, 2010; ISBN 978-92-4-159994-8. [Google Scholar]
- Redmayne, M. New Zealand adolescents’ cellphone and cordless phone user-habits: Are they at increased risk of brain tumours already? A cross-sectional study. Environ. Health 2013, 12, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The INTERPHONE Study Group Brain tumour risk in relation to mobile telephone use: Results of the INTERPHONE international case—Control study. Int. J. Epidemiol. 2010, 39, 675–694. [CrossRef] [PubMed] [Green Version]
- Hyland, G.J. Physics and biology of mobile telephony. Lancet 2000, 356, 1833–1836. [Google Scholar] [CrossRef]
- International Commission on Non-Ionizing Radiation Protection (ICNIRP)1 Guidelines for limiting exposure to electromagnetic fields (100 kHz to 300 GHz). Health Phys. 2020, 118, 483–524. [CrossRef] [PubMed]
- Baum, G.L.; Ciric, R.; Roalf, D.R.; Betzel, R.F.; Moore, T.M.; Shinohara, R.T.; Kahn, A.E.; Vandekar, S.N.; Rupert, P.E.; Quarmley, M.; et al. Modular segregation of structural brain networks supports the development of executive function in youth. Curr. Biol. 2017, 27, 1561–1572.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luna, B. Developmental changes in cognitive control through adolescence. Adv. Child. Dev. Behav. 2009, 37, 233–278. [Google Scholar] [CrossRef] [PubMed]
- Tamnes, C.K.; Herting, M.M.; Goddings, A.-L.; Meuwese, R.; Blakemore, S.-J.; Dahl, R.E.; Güroğlu, B.; Raznahan, A.; Sowell, E.R.; Crone, E.A.; et al. Development of the cerebral cortex across adolescence: A multisample study of inter-related longitudinal changes in cortical volume, surface area, and thickness. J. Neurosci. 2017, 37, 3402–3412. [Google Scholar] [CrossRef]
- Wierenga, L.; Langen, M.; Ambrosino, S.; van Dijk, S.; Oranje, B.; Durston, S. Typical development of basal ganglia, hippocampus, amygdala and cerebellum from age 7 to 24. NeuroImage 2014, 96, 67–72. [Google Scholar] [CrossRef]
- Barth, A.; Winker, R.; Ponocny-Seliger, E.; Mayrhofer, W.; Ponocny, I.; Sauter, C.; Vana, N. A meta-analysis for neurobehavioural effects due to electromagnetic field exposure emitted by GSM mobile phones. Occup. Environ. Med. 2008, 65, 342–346. [Google Scholar] [CrossRef] [PubMed]
- Abramson, M.J.; Benke, G.P.; Dimitriadis, C.; Inyang, I.O.; Sim, M.R.; Wolfe, R.S.; Croft, R.J. Mobile telephone use is associated with changes in cognitive function in young adolescents. Bioelectromagnetics 2009, 30, 678–686. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Benke, G.; Dimitriadis, C.; Inyang, I.; Sim, M.R.; Wolfe, R.; Croft, R.J.; Abramson, M.J. Use of mobile phones and changes in cognitive function in adolescents. Occup. Environ. Med. 2010, 67, 861–866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetc, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; ISBN 978-0-648-84880-6. [Google Scholar]
- Foerster, M.; Thielens, A.; Joseph, W.; Eeftens, M.; Röösli, M. A prospective cohort study of adolescents’ memory performance and individual brain dose of microwave radiation from wireless communication. Environ. Health Perspect. 2018, 126, 077007. [Google Scholar] [CrossRef] [Green Version]
- Roser, K.; Schoeni, A.; Röösli, M. Mobile phone use, behavioural problems and concentration capacity in adolescents: A prospective study. Int. J. Hyg. Environ. Health 2016, 219, 759–769. [Google Scholar] [CrossRef] [Green Version]
- Schoeni, A.; Roser, K.; Röösli, M. Memory performance, wireless communication and exposure to radiofrequency electromagnetic fields: A prospective cohort study in adolescents. Environ. Int. 2015, 85, 343–351. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, C.R.; Benke, G.; Smith, C.L.; Redmayne, M.; Dimitriadis, C.; Dalecki, A.; Macleod, S.; Sim, M.R.; Croft, R.J.; Wolfe, R.; et al. Use of mobile and cordless phones and change in cognitive function: A prospective cohort analysis of Australian primary school children. Environ. Health 2017, 16, 62. [Google Scholar] [CrossRef] [Green Version]
- Brzozek, C.; Benke, K.K.; Zeleke, B.M.; Croft, R.J.; Dalecki, A.; Dimitriadis, C.; Kaufman, J.; Sim, M.R.; Abramson, M.J.; Benke, G. Uncertainty analysis of mobile phone use and its effect on cognitive function: The application of monte carlo simulation in a cohort of Australian primary school children. Int. J. Environ. Res. Public Health 2019, 16, 2428. [Google Scholar] [CrossRef] [Green Version]
- Redmayne, M.; Smith, C.L.; Benke, G.; Croft, R.J.; Dalecki, A.; Dimitriadis, C.; Kaufman, J.; Macleod, S.; Sim, M.R.; Wolfe, R.; et al. Use of mobile and cordless phones and cognition in Australian primary school children: A prospective cohort study. Environ. Health 2016, 15, 26. [Google Scholar] [CrossRef] [Green Version]
- Guxens, M.; Vermeulen, R.; van Eijsden, M.; Beekhuizen, J.; Vrijkotte, T.G.M.; van Strien, R.T.; Kromhout, H.; Huss, A. Outdoor and indoor sources of residential radiofrequency electromagnetic fields, personal cell phone and cordless phone use, and cognitive function in 5–6 years old children. Environ. Res. 2016, 150, 364–374. [Google Scholar] [CrossRef] [PubMed]
- Calvente, I.; Pérez-Lobato, R.; Núñez, M.-I.; Ramos, R.; Guxens, M.; Villalba, J.; Olea, N.; Fernández, M.F. Does exposure to environmental radiofrequency electromagnetic fields cause cognitive and behavioral effects in 10-year-old boys? Bioelectromagnetics 2016, 37, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Sudan, M.; Birks, L.E.; Aurrekoetxea, J.J.; Ferrero, A.; Gallastegi, M.; Guxens, M.; Ha, M.; Lim, H.; Olsen, J.; González-Safont, L.; et al. Maternal cell phone use during pregnancy and child cognition at age 5 years in 3 birth cohorts. Environ. Int. 2018, 120, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Meo, S.A.; Almahmoud, M.; Alsultan, Q.; Alotaibi, N.; Alnajashi, I.; Hajjar, W.M. Mobile phone base station tower settings adjacent to school buildings: Impact on students’ cognitive health. Am. J. Men’s Health 2019, 13, 1557988318816914. [Google Scholar] [CrossRef] [PubMed]
- Cardis, E.; Richardson, L.; Deltour, I.; Armstrong, B.; Feychting, M.; Johansen, C.; Kilkenny, M.; McKinney, P.; Modan, B.; Sadetzki, S.; et al. The INTERPHONE study: Design, epidemiological methods, and description of the study population. Eur. J. Epidemiol. 2007, 22, 647–664. [Google Scholar] [CrossRef] [Green Version]
- Roser, K.; Schoeni, A.; Bürgi, A.; Röösli, M. Development of an RF-EMF exposure surrogate for epidemiologic research. Int. J. Environ. Res. Public Health 2015, 12, 5634–5656. [Google Scholar] [CrossRef]
- van Eijsden, M.; Vrijkotte, T.G.M.; Gemke, R.J.B.J.; van der Wal, M.F. Cohort profile: The Amsterdam Born Children and their Development (ABCD) study. Int. J. Epidemiol. 2011, 40, 1176–1186. [Google Scholar] [CrossRef] [Green Version]
- Guxens, M.; Ballester, F.; Espada, M.; Fernández, M.F.; Grimalt, J.O.; Ibarluzea, J.; Olea, N.; Rebagliato, M.; Tardón, A.; Torrent, M.; et al. Cohort profile: The INMA—INfancia y Medio Ambiente—(Environment and Childhood) Project. Int. J. Epidemiol. 2012, 41, 930–940. [Google Scholar] [CrossRef] [Green Version]
- Azizi, E.; Stainer, M.J.; Abel, L.A. Is experience in multi-genre video game playing accompanied by impulsivity? Acta Psychol. 2018, 190, 78–84. [Google Scholar] [CrossRef]
- Dye, M.W.G.; Green, C.S.; Bavelier, D. Increasing speed of processing with action video games. Curr. Dir. Psychol. Sci. 2009, 18, 321–326. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.; Spence, I. Playing shooter and driving videogames improves top-down guidance in visual search. Atten. Percept. Psychophys. 2013, 75, 673–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, J.; Tang, T.; Hu, G.; Zheng, J.; Wang, Y.; Wang, Q.; Su, J.; Zou, Y.; Peng, X. Association between exposure to electromagnetic fields from high voltage transmission lines and neurobehavioral function in children. PLoS ONE 2013, 8, e67284. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, S.W.S.; Nyberg, L.; Bäckman, L. Intra-individual variability in behavior: Links to brain structure, neurotransmission and neuronal activity. Trends Neurosci. 2006, 29, 474–480. [Google Scholar] [CrossRef]
- Verrender, A.; Loughran, S.P.; Dalecki, A.; McKenzie, R.; Croft, R.J. Pulse modulated radiofrequency exposure influences cognitive performance. Int. J. Radiat. Biol. 2016, 92, 603–610. [Google Scholar] [CrossRef]
- Samkange-Zeeb, F.; Berg, G.; Blettner, M. Validation of self-reported cellular phone use. J. Expo. Anal. Environ. Epidemiol. 2004, 14, 245–248. [Google Scholar] [CrossRef] [Green Version]
- Vrijheid, M.; Cardis, E.; Armstrong, B.K.; Auvinen, A.; Berg, G.; Blaasaas, K.G.; Brown, J.; Carroll, M.; Chetrit, A.; Christensen, H.C.; et al. Validation of short term recall of mobile phone use for the Interphone study. Occup. Environ. Med. 2006, 63, 237–243. [Google Scholar] [CrossRef] [Green Version]
- Lenroot, R.K.; Giedd, J.N. Brain development in children and adolescents: Insights from anatomical magnetic resonance imaging. Neurosci. Biobehav. Rev. 2006, 30, 718–729. [Google Scholar] [CrossRef]
- Casey, B.J.; Tottenham, N.; Liston, C.; Durston, S. Imaging the developing brain: What have we learned about cognitive development? Trends Cogn. Sci. 2005, 9, 104–110. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | PY | Study Design | Conducted Year | Participants | Exposure | Cognitive Task | Outcome | Main Findings |
|---|---|---|---|---|---|---|---|---|
| Abramson et al. [13] | 2009 | Cross-sectional | Data were collected during 2005 and 2006. | 317 students 11–14 years old From MoRPhEUS | Mobile phone usage was assessed using questionnaire completed by children and their parents. | Signal detection task Moving card monitoring task One card learning task Associative learning task Stroop task N-back task | Simple reaction Choice reaction Attention Visual memory Associative memory Interference control Working memory | Mobile phone use was associated with poor accuracy on the N-back task, shorter reaction time on the simple reaction time task, poor accuracy and shorter reaction time on the associative learning task, and longer completion time on the Stroop task. |
| Thomas et al. [14] | 2010 | Prospective cohort | Baseline data were collected during 2005 and 2006. Follow-up investigations were conducted approximately 1 year after baseline. | 236 students 12–13 years old From MoRPhEUS | Mobile phone usage was assessed using self-reported questionnaire. | Signal detection task Moving card monitoring task One card learning task Associative learning task Stroop task N-back task | Simple reaction Choice reaction Attention Visual memory Associative memory Interference control Working memory | Mobile phone use at baseline was associated with smaller reductions in response times on the 2-back task and One card learning task. Increased mobile phone use was associated with smaller reductions in reaction time on the simple reaction task and larger reductions in reaction time on the 2-back task. |
| Foerster et al. [17] | 2018 | Prospective cohort | Baseline data were collected in June 2012 (1st wave) and April 2014 (2nd wave). Follow-up investigations were conducted approximately 1 year after each baseline until April 2016. | 669–676 children 10–17 years old From HERMES study | Daily quantitative mobile phone use was obtained from the mobile phone network operators. Mobile phone and other wireless communication devices use was assessed using self-reported questionnaire. | Intelligenz-Struktur-Test | Figural memory Verbal memory | Increase in estimated cumulative RF-EMF brain dose scores was associated with decreased figural memory score. |
| Roser et al. [18] | 2016 | Prospective cohort | Baseline data were collected between June 2012 and February 2013. Follow-up investigations were conducted approximately 1 year after baseline. | 439 adolescents 12–17 years old From HERMES study | Daily quantitative mobile phone use was obtained from the mobile phone network operators. Mobile phone and other wireless communication devices use was assessed using self-reported questionnaire. | FAKT-II | Concentration | In the cross-sectional analysis, mobile phone usage and cumulative RF-EMF dose were associated with poor FAKT- II performance, while no such association was found in the longitudinal analysis. |
| Schoeni et al. [19] | 2015 | Prospective cohort | Baseline data were collected between June 2012 and February 2013. Follow-up investigations were conducted approximately 1 year after baseline. | 234 adolescents 7th, 8th, and 9th grades From HERMES study | Daily quantitative mobile phone use was obtained from the mobile phone network operators. Mobile phone and other wireless communication devices use was assessed using self-reported questionnaire. | Intelligenz-Struktur-Test | Figural memory Verbal memory | An increase in mobile phone call duration was associated with a decrease in figural memory. Cumulative RF-EMF brain and whole-body dose were associated with decreases in figural memory scores. |
| Bhatt et al. [20] | 2017 | Prospective cohort | Data were collected in November 2010–February 2012 (baseline) and March 2012–March 2013 (follow-up). | 412 children 4th grade (9 or 10 years old) From ExPOSURE study | Mobile phone and cordless phone voice calls and number of text message or SMS were assessed using self-reported questionnaire. | Signal detection task Identification task One card learning task Groton maze learning task Go/No-go task Stroop task One-back task | Simple reaction Choice reaction Memory Executive function Response inhibition Interference control Working memory | Increase in mobile phone usage was associated with larger reduction in reaction time in the Go/No-go task, smaller reduction in the errors on the Groton maze learning task, and larger increase in reaction time on the Stroop task. Increase in cordless phone usage was associated with smaller reduction in accuracy on the Signal detection task. |
| Brzozek et al. [21] | 2019 | Prospective cohort | Data were collected twice, approximately one year apart between 2011 and 2013. | 412 children 4th grade (9 or 10 years old) From ExPOSURE study | Mobile phone use was assessed using self-reported questionnaire. | Signal detection task Identification task One card learning task Groton maze learning task Go/No-go task Stroop task One-back task | Simple reaction Choice reaction Memory Executive function Response inhibition Interference control Working memory | Mobile phone calls were associated with shorter reaction time in the Go/No-go task, lower accuracy on the Groton maze learning task, and poor Stroop task performance. |
| Redmayne et al. [22] | 2016 | Cross-sectional | Data were collected in mid-2011. | 575–589 children 8–11 years old From ExPOSURE study | Mobile phone and cordless phone use were assessed via the parents’ answers to the questionnaires. The ownership of mobile phone was assessed using self-reported questionnaire. | One-back task Signal detection task Identification task One card learning task Groton maze learning task Go/No-go task Stroop task | Simple reaction Choice reaction Memory Executive function Response inhibition Interference control Working memory | Mobile phone usage was associated with slower reaction time on the Go/No-go task. Cordless phone usage was associated with slower reaction time on the Stroop task, and lower accuracy on the One card learning task and Identification task. |
| Guxens et al. [23] | 2016 | Cross-sectional | Between January 2003 and March 2004, participants’ mothers were enrolled during their first prenatal visit to an obstetric care provider. | 2354 children 5–6 years old From ABCD study | RF-EMF (mobile phone base station) was estimated using the 3D geospatial radio wave propagation model NISMap. RF-EMF (indoor source, i.e., cordless phone base stations and Wi-Fi) was assessed using questionnaires answered by the mothers. Cell phone and cordless phone use was assessed using questionnaires answered by the mothers (Assessed when children were 7 years old). | Baseline speed task Response organization task Pursuit task Tracking task (Assessed at 5–6 years) | Simple reaction Inhibitory control Cognitive flexibility Visuomotor coordination | Residential RF-EMF exposure from mobile phone base station was associated with improved inhibitory control and cognitive flexibility and reduced visuomotor coordination. Residential presence of RF-EMF indoor source was associated with improved simple reaction time, inhibitory control, and visuomotor coordination. Personal cordless phone use was associated with reduced inhibitory control and cognitive flexibility and improved visuomotor coordination. |
| Calvente et al. [24] | 2016 | Cross-sectional | Participants were recruited at birth from 2000 through 2002, were evaluated at the age of 9–11 years. | 123 boys 9–11 years old From INMA-Granada cohort | Spot electric field measurements within the 100 kHz to 6 GHz frequency range were performed in the immediate surroundings of children’s dwellings. | K-BIT Letter-number sequencing Categorical verbal fluency Continuous Performance test TAVECI Trail Making Test A WISC-IV Go/No-go task Stroop task Trail Making Test B | IQ Language Executive function Working memory Verbal fluency Attention Memory Visuomotor coordination Simple reaction Response inhibition Interference control Cognitive flexibility | Children living in higher RF exposure areas had lower IQ and language scores. |
| Sudan et al. [25] | 2018 | Prospective birth cohorts | Time periods of enrollment in each cohort were: 1996–2002 (DNBC), 2003–2008 (INMA), and 2006–2011 (MOCEH). Cognitive assessment was performed at the age of 60–64 months (DNBC), 49–82 months (INMA), and 47–77 months (MOCEH). | 3089 children 4–6 years old From DNBC, INMA, and MOCEH study | Cell phone use among mothers was assessed during pregnancy (Spain and Korea). Cell phone use during pregnancy was recalled by mothers when the children reached 7 years of age (Denmark). | WPPSI-R/MSCA | General cognition Verbal cognition Non-verbal cognition | No associations were found between prenatal cell phone use and WPPSI-R/MSCA scores. |
| Meo et al. [26] | 2018 | Cross-sectional | NA | 217 students 13–16 years old | RF-EMF exposure at school was monitored by the Narda Safety Test Solution SRM-3006. | Motor Screening task Spatial Working Memory task | Simple reaction Working memory | Children who were exposed to high RF-EMF produced by mobile base stations had poorer performance on the Motor Screening task and Spatial Working Memory task. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishihara, T.; Yamazaki, K.; Araki, A.; Teraoka, Y.; Tamura, N.; Hikage, T.; Omiya, M.; Mizuta, M.; Kishi, R. Exposure to Radiofrequency Electromagnetic Field in the High-Frequency Band and Cognitive Function in Children and Adolescents: A Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 9179. https://doi.org/10.3390/ijerph17249179
Ishihara T, Yamazaki K, Araki A, Teraoka Y, Tamura N, Hikage T, Omiya M, Mizuta M, Kishi R. Exposure to Radiofrequency Electromagnetic Field in the High-Frequency Band and Cognitive Function in Children and Adolescents: A Literature Review. International Journal of Environmental Research and Public Health. 2020; 17(24):9179. https://doi.org/10.3390/ijerph17249179
Chicago/Turabian StyleIshihara, Toru, Keiko Yamazaki, Atsuko Araki, Yuri Teraoka, Naomi Tamura, Takashi Hikage, Manabu Omiya, Masahiro Mizuta, and Reiko Kishi. 2020. "Exposure to Radiofrequency Electromagnetic Field in the High-Frequency Band and Cognitive Function in Children and Adolescents: A Literature Review" International Journal of Environmental Research and Public Health 17, no. 24: 9179. https://doi.org/10.3390/ijerph17249179
APA StyleIshihara, T., Yamazaki, K., Araki, A., Teraoka, Y., Tamura, N., Hikage, T., Omiya, M., Mizuta, M., & Kishi, R. (2020). Exposure to Radiofrequency Electromagnetic Field in the High-Frequency Band and Cognitive Function in Children and Adolescents: A Literature Review. International Journal of Environmental Research and Public Health, 17(24), 9179. https://doi.org/10.3390/ijerph17249179