SARS-CoV-2 Infections and COVID-19 Fatality: Estimation of Infection Fatality Ratio and Current Prevalence




Abstract
:1. Introduction
- (i.)
- Which is the actual IFR, estimated as the number of deaths due to COVID-19 with respect to the number of SARS-CoV-2 infected people? IFR is studied instead of CFR, because most of the available data report all confirmed SARS-CoV-2 infected people as positive cases, without distinguishing between asymptomatic cases and COVID-19 patients, including subclinical and more serious cases.
- (ii.)
- Which is the actual prevalence hereto, estimated as the number of (currently) infected people with respect to the entire population, both in a specific population and all over the world?
2. Materials and Methods
2.1. Data
2.2. Existing Methods for Estimating IFR
2.3. Proposed Approach for Estimating IFR and Prevalence
- (i.)
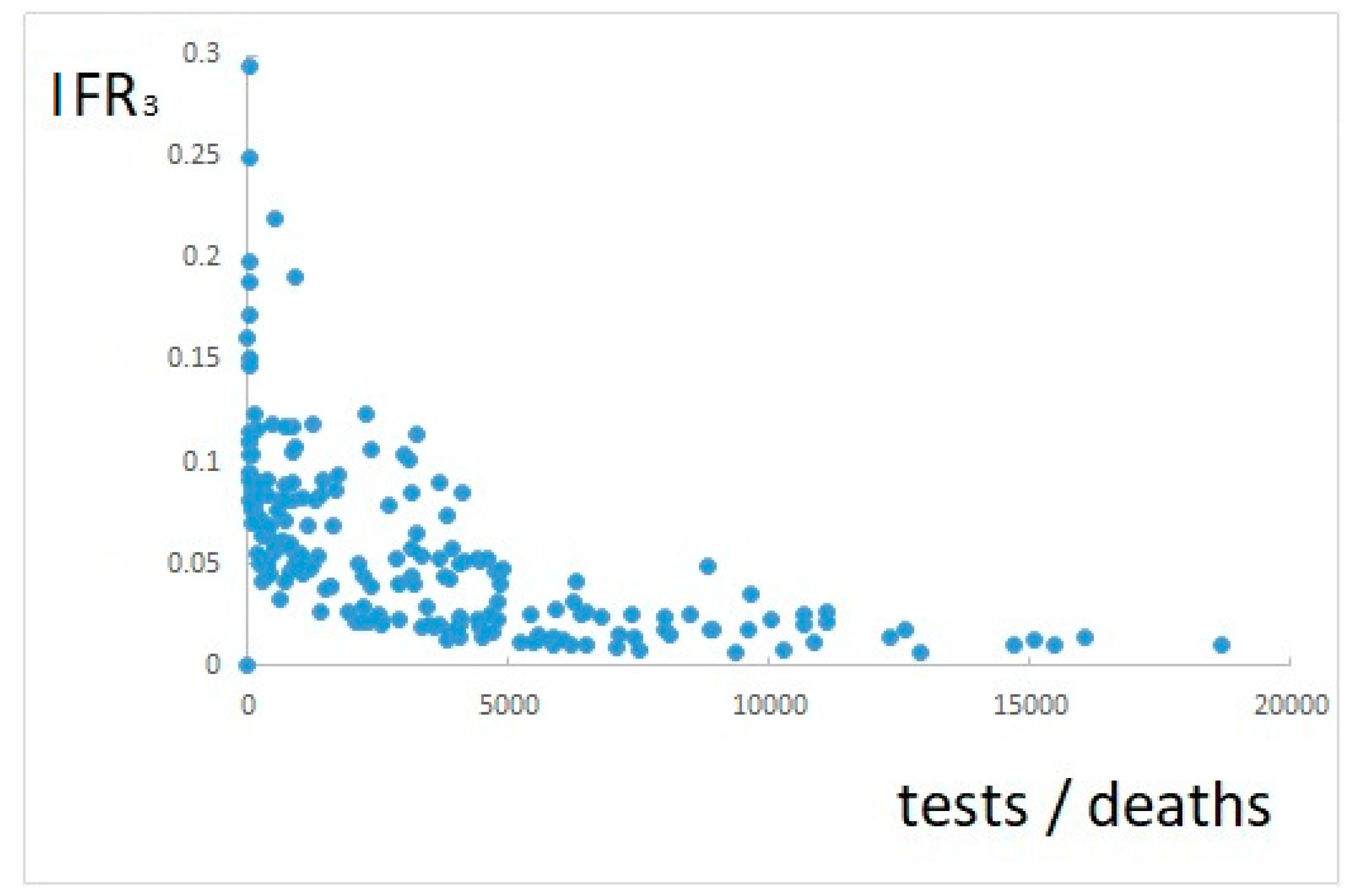
- obviously, the estimate of new positives on day i is better the more tests are performed on day i;
- (ii.)
- the quantity of tests should not be evaluated as an absolute value, but with respect to the number of actual positive cases;
- (iii.)
- the number of actual positive cases on day i is unknown, but according to Equation (3) it is proportional to new deaths on day i + T.
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 31 October 2020).
- Weston, S.; Friedman, M.B. COVID-19: Knowns, Unknowns, and Questions. mSphere 2020, 5, e00203–e00220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Cheng, Z. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Yu, T. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Tang, J.W.; Tambyah, P.A.; Hui, D.S.C. Emergence of a novel coronavirus causing respiratory illness from Wuhan, China. J. Infect. 2020, 80, 350–371. [Google Scholar] [CrossRef] [PubMed]
- Habibzadeh, P.; Stoneman, E.K. The novel coronavirus: A bird’s eye view. Int J. Occup Envrion. Med. 2020, 11, 65–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Surveillance for Human Infection with Novel Coronavirus (2019-nCoV); World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection When Novel Coronavirus (2019-nCoV) Infection Is Suspected; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Russell, C.; Millar, J.; Baillie, J. Clinical evidence does not support corticosteroid treatment for 2019-nCoV lung injury. Lancet 2020, 395, 473–475. [Google Scholar] [CrossRef] [Green Version]
- Paules, C.I.; Marston, H.D.; Fauci, A.S. Coronavirus infections—More than just the common cold. JAMA 2020, 323, 707–708. [Google Scholar] [CrossRef] [Green Version]
- Holshue, M.L.; DeBolt, C.; Lindquist, S.; Lofy, K.H.; Wiesman, J.; Bruce, H.; Spitters, C.; Ericson, K.; Wilkerson, S.; Tural, A.; et al. First case of 2019 novel coronavirus in the United States. N. Engl. J. Med. 2020, 382, 929–936. [Google Scholar] [CrossRef]
- Wang, Z.; Chen, X.; Lu, Y.; Chen, F.; Zhang, W. Clinical characteristics and therapeutic procedure for four cases with 2019 novel coronavirus pneumonia receiving combined Chinese and Western medicine treatment. Biosci. Trends 2020, 14, 64–68. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020, 30, 269–271. [Google Scholar] [CrossRef]
- De Wit, E.; Feldmann, F.; Cronin, J.; Jordan, R.; Okumura, A.; Thomas, T.; Feldmann, H. Prophylactic and therapeutic remdesivir (GS-5734) treatment in the rhesus macaque model of MERS-CoV infection. Proc. Natl. Acad. Sci. USA 2020, 3, 20192208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Wang, X.-J. Potential inhibitors for 2019-nCoV coronavirus M protease from clinically approved medicines. J. Genet. Genom. 2020, 47, 119. [Google Scholar] [CrossRef] [PubMed]
- Lu, H. Drug treatment options for the 2019-new coronavirus (2019-nCoV). Biosci. Trends 2020, 14, 69–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulut, C.; Kato, Y. Epidemiology of COVID-19. Turk. J. Med. Sci. 2020, 50, 563–570. [Google Scholar] [CrossRef]
- NYC Health—Confirmed and Probable COVID-19 Deaths Daily Report. Available online: https://www1.nyc.gov/assets/doh/downloads/pdf/imm/covid-19-deaths-confirmed-probable-daily-05022020.pdf (accessed on 31 October 2020).
- Preliminary Estimate of Excess Mortality During the COVID-19 Outbreak—New York City, March 11–May 2, 2020. Mmwr. Morb. Mortal. Wkly. Rep. 2020, 69, 603–605. [CrossRef]
- Amid Ongoing COVID-19 Pandemic, Governor Cuomo Announces Results of Completed Antibody Testing Study of 15,000 People Showing 12.3 Percent of Population Has COVID-19 Antibodies. Available online: https://www.governor.ny.gov/news/amid-ongoing-covid-19-pandemic-governor-cuomo-announces-results-completed-antibody-testing (accessed on 31 October 2020).
- United States Census Bureau—Quick Facts New York City, New York. Available online: https://www.census.gov/quickfacts/fact/table/newyorkcitynewyork/AGE775219#AGE775218 (accessed on 31 October 2020).
- NYC Health—Coronavirus Disease 2019 (COVID-19) Daily Data Summary. Available online: https://www1.nyc.gov/assets/doh/downloads/pdf/imm/covid-19-daily-data-summary-05022020-1.pdf (accessed on 31 October 2020).
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Novel Coronavirus Press Conference at United Nations of Geneva. Available online: https://www.who.int/docs/default-source/coronaviruse/transcripts/who-audio-script-ncov-rresser-unog-29jan2020.pdf?sfvrsn=a7158807_4 (accessed on 31 October 2020).
- Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). Available online: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf (accessed on 31 October 2020).
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—3 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---3-march-2020 (accessed on 31 October 2020).
- Kazemi-Karyani, A.; Safari-Faramani, R.; Amini, S.; Ramezani-Doroh, V.; Berengjian, F.; Dizaj, M.Y.; Hashempour, R.; Dizaj, J.Y. World one-hundred days after COVID-19 outbreak: Incidence, case fatality rate, and trend. J. Educ. Health Prom. 2020, 9, 199. [Google Scholar]
- Ghani, A.C.; Donnelly, C.A.; Cox, D.R.; Griffin, J.T.; Fraser, C.; Lam, T.H.; Ho, L.M.; Chan, W.S.; Anderson, R.M.; Hedley, A.J. Methods for Estimating the Case Fatality Ratio for a Novel, Emerging Infectious Disease. Am. J. Epidemiol. 2005, 162, 479–486. [Google Scholar] [CrossRef]
- Coronavirus (COVID-19) Mortality Rate. Available online: https://www.worldometers.info/coronavirus/coronavirus-death-rate/#nhc (accessed on 31 October 2020).
- COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 31 October 2020).
- Mizumoto, K.; Kagaya, K.; Chowell, G. Early epidemiological assessment of the transmission potential and virulence of coronavirus disease 2019 (COVID-19) in Wuhan City, China, January–February, 2020. BMC Med. 2020, 18, 217. [Google Scholar] [CrossRef]
- Price-Haywood, E.G.; Burton, J.; Fort, D.; Seoane, L. Hospitalization and Mortality among Black Patients and White Patients with Covid-19. N. Engl. J. Med. 2020, 38, 2534–2543. [Google Scholar] [CrossRef]
- Khunti, K.; Platt, L.; Routen, A.; Abbasi, K. Covid-19 and ethnic minorities: An urgent agenda for overdue action. BMJ 2020, 369, m2503. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.Y.; Chen, L.; Wang, M. Presumed asymptomatic carrier transmission of COVID-19. JAMA 2020, 323, 1406–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.M.; Wei, L.; Xie, L.; Zhu, G.; Dela Cruz, C.S.D.; Sharma, L. Epidemiologic and clinical characteristics of novel coronavirus infections involving 13 patients outside Wuhan, China. JAMA 2020, 323, 1092–1093. [Google Scholar] [CrossRef]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Liu, W.; Zhang, Q.; Chen, J.; Xiang, R.; Song, H.; Shu, S.; Chen, L.; Liang, L.; Zhou, J.; You, L.; et al. Detection of Covid-19 in children in early January 2020 in Wuhan, China. N. Engl. J. Med. 2020, 382, 1370–1371. [Google Scholar] [CrossRef]
- Shen, K.L.; Yang, Y.H. Diagnosis and treatment of 2019 novel coronavirus infection in children: A pressing issue. World J. Pediatr. 2020, 16, 219–221. [Google Scholar] [CrossRef] [Green Version]
- Chan, J.F.-W.; Yuan, S.; Kok, K.-H.; To, K.K.-W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.-Y.; Poon, R.W.-S.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Harapan, H.; Itoh, N.; Yufika, A.; Winardi, W.; Keam, S.; Te, H.; Megawati, D.; Hayati, Z.; Wagner, A.L.; Mudatsir, M. Coronavirus disease 2019 (COVID-19): A literature review. J. Infect. Public Health 2020, 13, 667–673. [Google Scholar] [CrossRef]
- Pcm-Dpc/COVID-19. Available online: https://github.com/pcm-dpc/COVID-19 (accessed on 31 October 2020).
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Woodruff, A. COVID-19 Follow up Testing. J. Infect. 2020, 81, 647–679. [Google Scholar] [CrossRef] [PubMed]
- Lauer, S.A.; Grantz, K.H.; Bi, Q.; Jones, F.K.; Zheng, Q.; Meredith, H.R.; Azman, A.S.; Reich, N.G.; Lessler, J. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: Estimation and application. Ann. Intern. Med. 2020, 172, 577–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO—COVID-19 Weekly Epidemiological Update. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20201020-weekly-epi-update-10.pdf?sfvrsn=58786643_26&download=true (accessed on 31 October 2020).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Date | Total Positives | New Positives | Cumulative Recovered | Cumulative Deaths | New Deaths | Cumulative Cases | New Tests |
|---|---|---|---|---|---|---|---|
| 24 February 2020 | 221 | 221 | 1 | 7 | 7 | 229 | 4324 |
| 25 February 2020 | 311 | 93 | 1 | 10 | 3 | 322 | 4299 |
| 27 March 2020 | 66,414 | 5959 | 10,950 | 9134 | 969 | 86,498 | 33,019 |
| 02 June 2020 | 39,893 | 318 | 160,092 | 33,530 | 55 | 233,515 | 52,159 |
| 22 October 2020 | 169,302 | 16,079 | 259,456 | 36,968 | 136 | 465,726 | 170,392 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pota, M.; Pota, A.; Sirico, M.L.; Esposito, M. SARS-CoV-2 Infections and COVID-19 Fatality: Estimation of Infection Fatality Ratio and Current Prevalence. Int. J. Environ. Res. Public Health 2020, 17, 9290. https://doi.org/10.3390/ijerph17249290
Pota M, Pota A, Sirico ML, Esposito M. SARS-CoV-2 Infections and COVID-19 Fatality: Estimation of Infection Fatality Ratio and Current Prevalence. International Journal of Environmental Research and Public Health. 2020; 17(24):9290. https://doi.org/10.3390/ijerph17249290
Chicago/Turabian StylePota, Marco, Andrea Pota, Maria Luisa Sirico, and Massimo Esposito. 2020. "SARS-CoV-2 Infections and COVID-19 Fatality: Estimation of Infection Fatality Ratio and Current Prevalence" International Journal of Environmental Research and Public Health 17, no. 24: 9290. https://doi.org/10.3390/ijerph17249290
APA StylePota, M., Pota, A., Sirico, M. L., & Esposito, M. (2020). SARS-CoV-2 Infections and COVID-19 Fatality: Estimation of Infection Fatality Ratio and Current Prevalence. International Journal of Environmental Research and Public Health, 17(24), 9290. https://doi.org/10.3390/ijerph17249290