Occupational Risk for Post-Traumatic Stress Disorder and Trauma-Related Depression: A Systematic Review with Meta-Analysis

 and
and 
Abstract
:1. Introduction
- Is there an increased risk of PTSD or depression among workers in specific occupations with frequent exposure to trauma (train drivers, soldiers, firefighters, police officers, paramedics, emergency doctors, war journalists or war photographers, prison staff, or psychiatric staff)? If so, how high is this risk?
- Is there an increased risk of PTSD or depression among employees who have been exposed to occupational trauma, violence, attacks, sexual harassment, or war? If so, how high is the risk?
2. Methods
3. Results
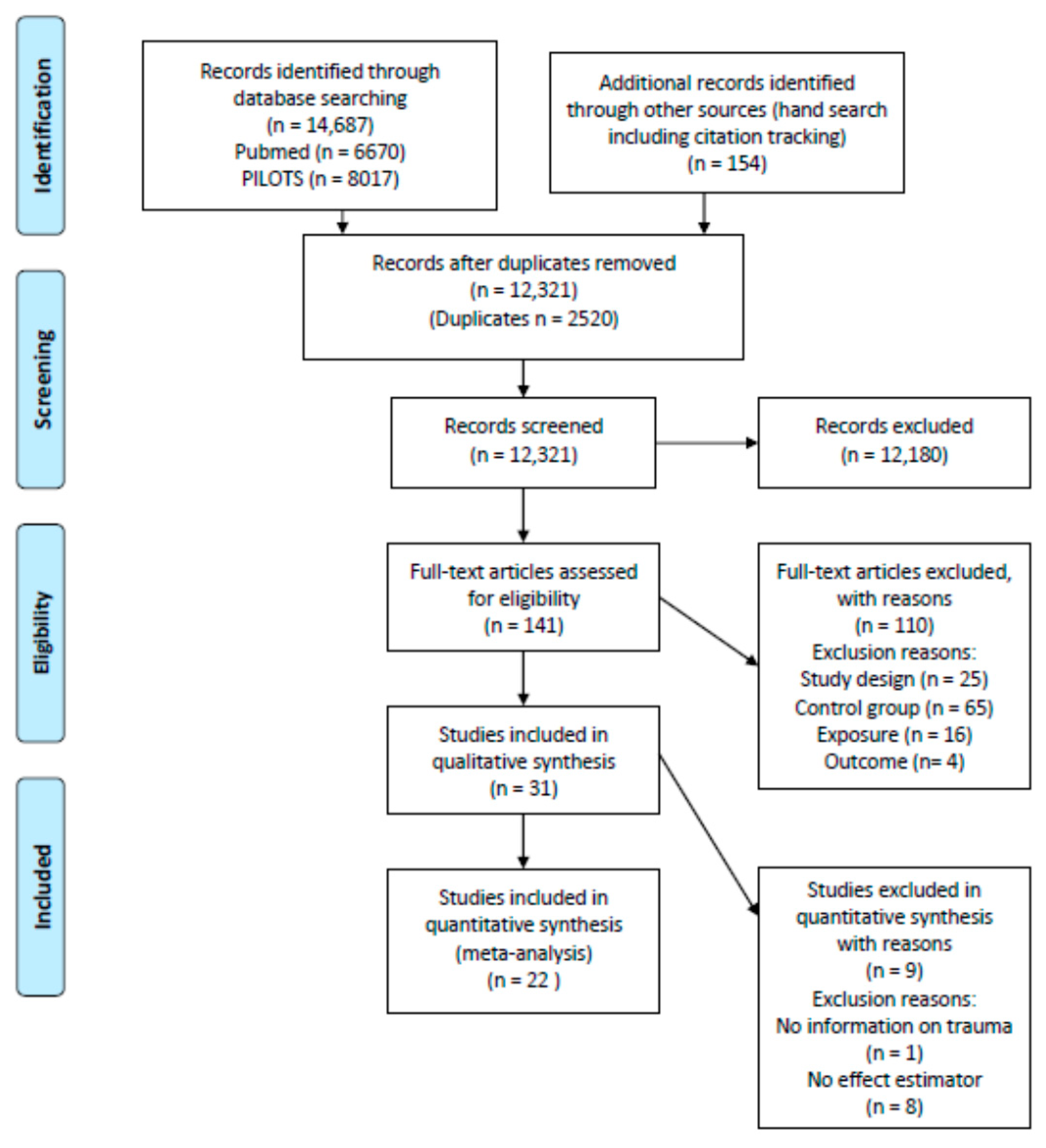
3.1. Search Results
3.2. Study Characteristics
3.2.1. Study Design and Country of Study
3.2.2. Outcomes Studied
- Study Population
- Exposure
- Comparison Group
3.3. Risk of Bias Evaluation
3.4. Study Results
3.5. Meta-Analysis
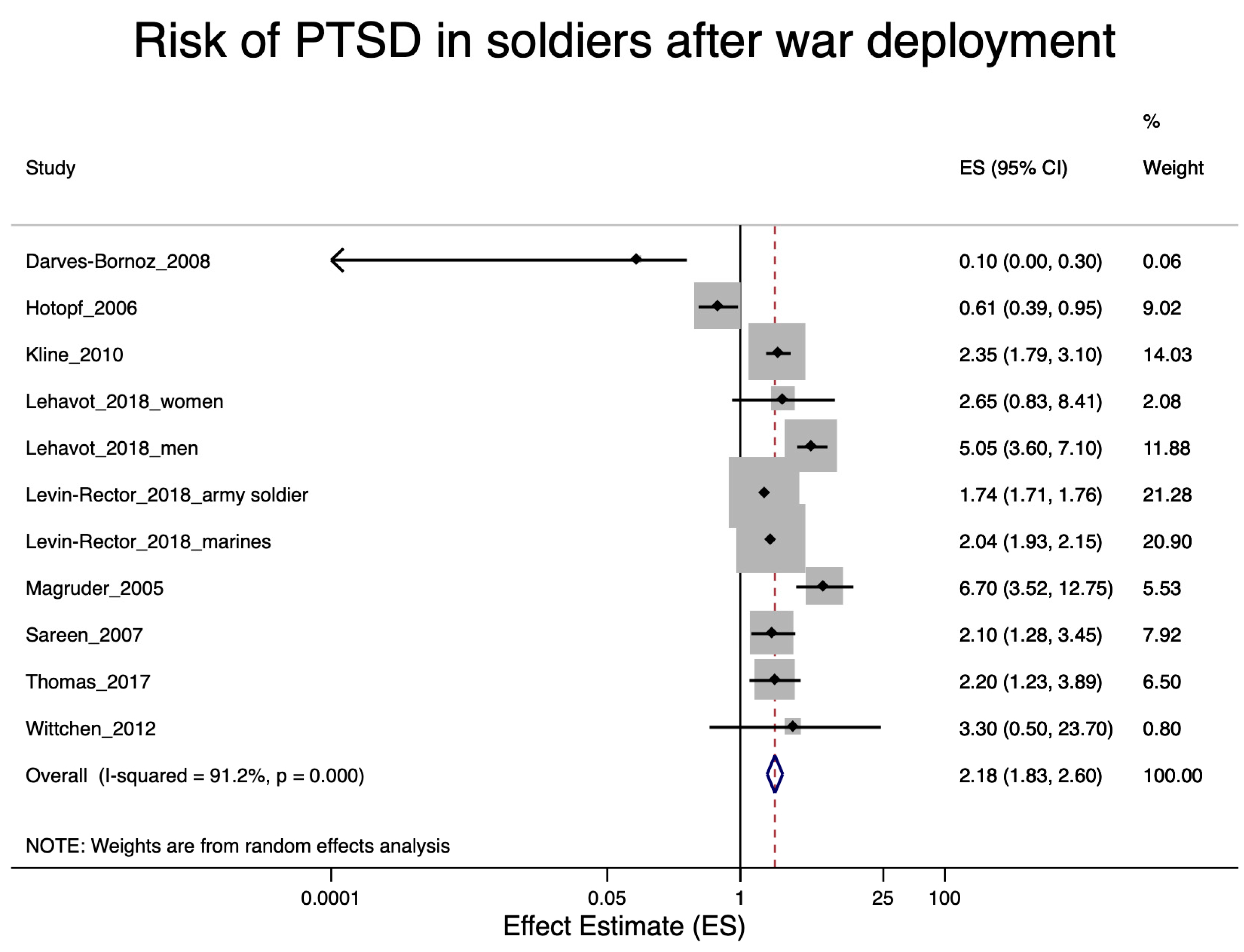
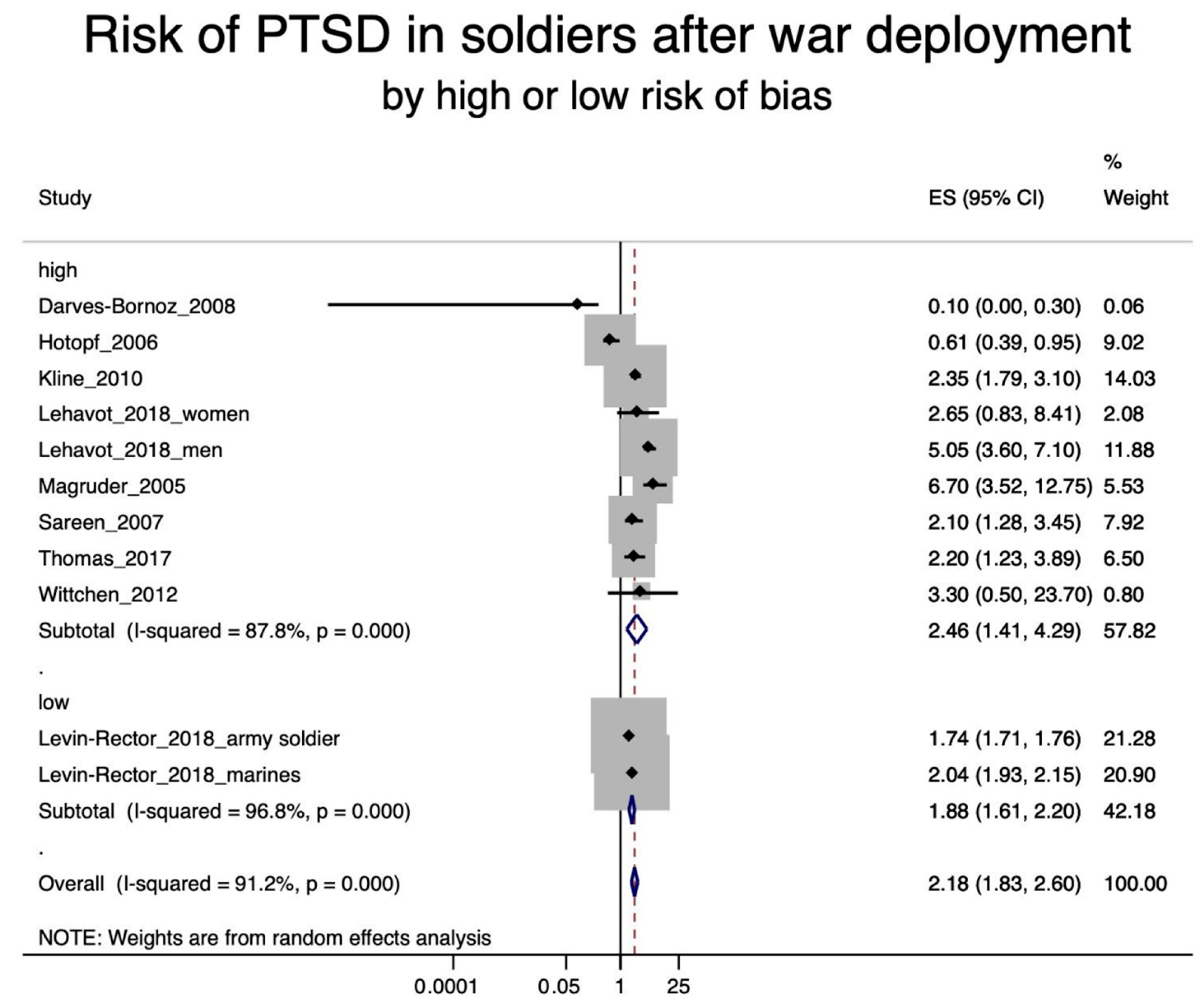
3.5.1. PTSD in Soldiers after War Deployment
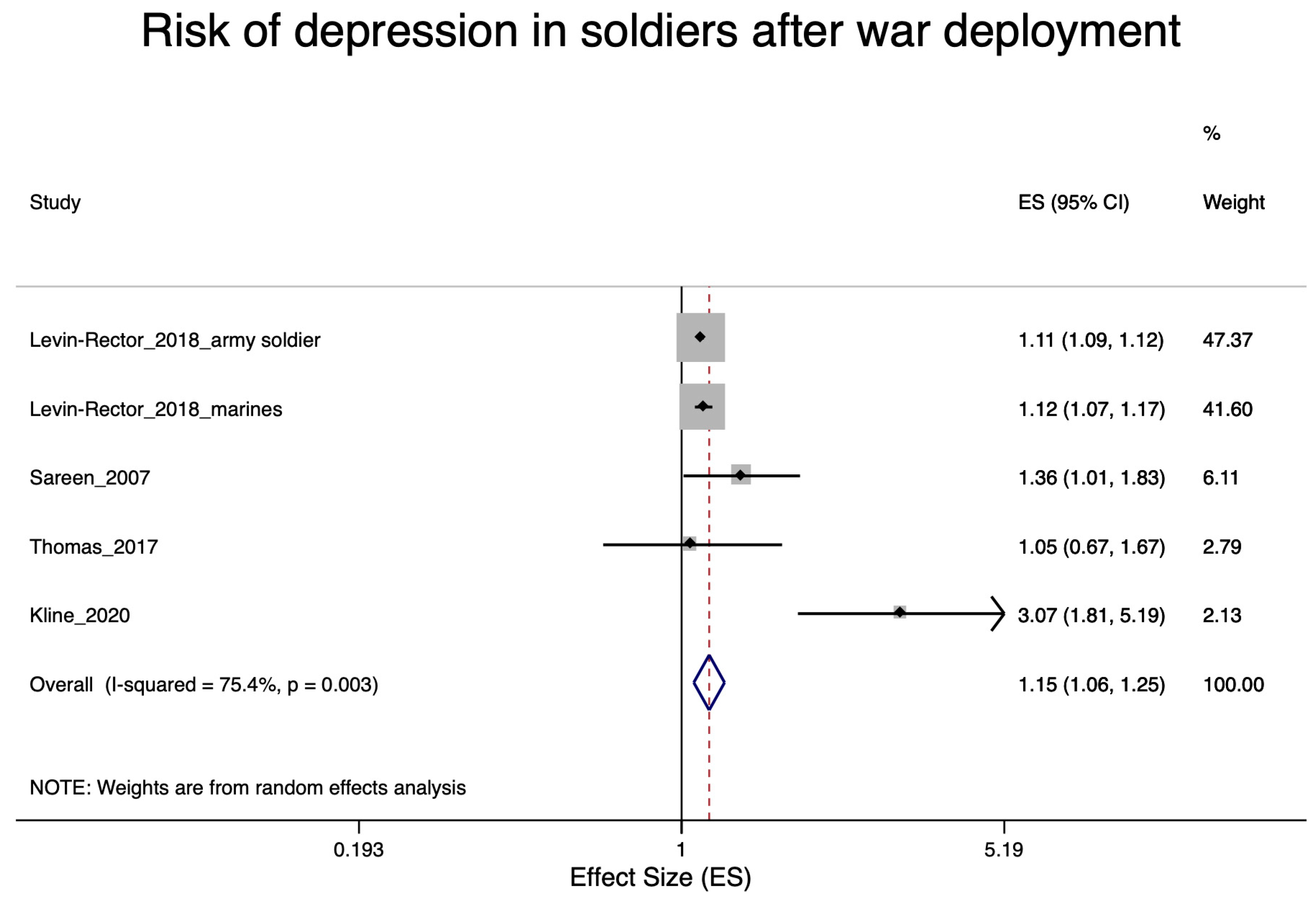
3.5.2. Depression in Soldiers after War Deployment
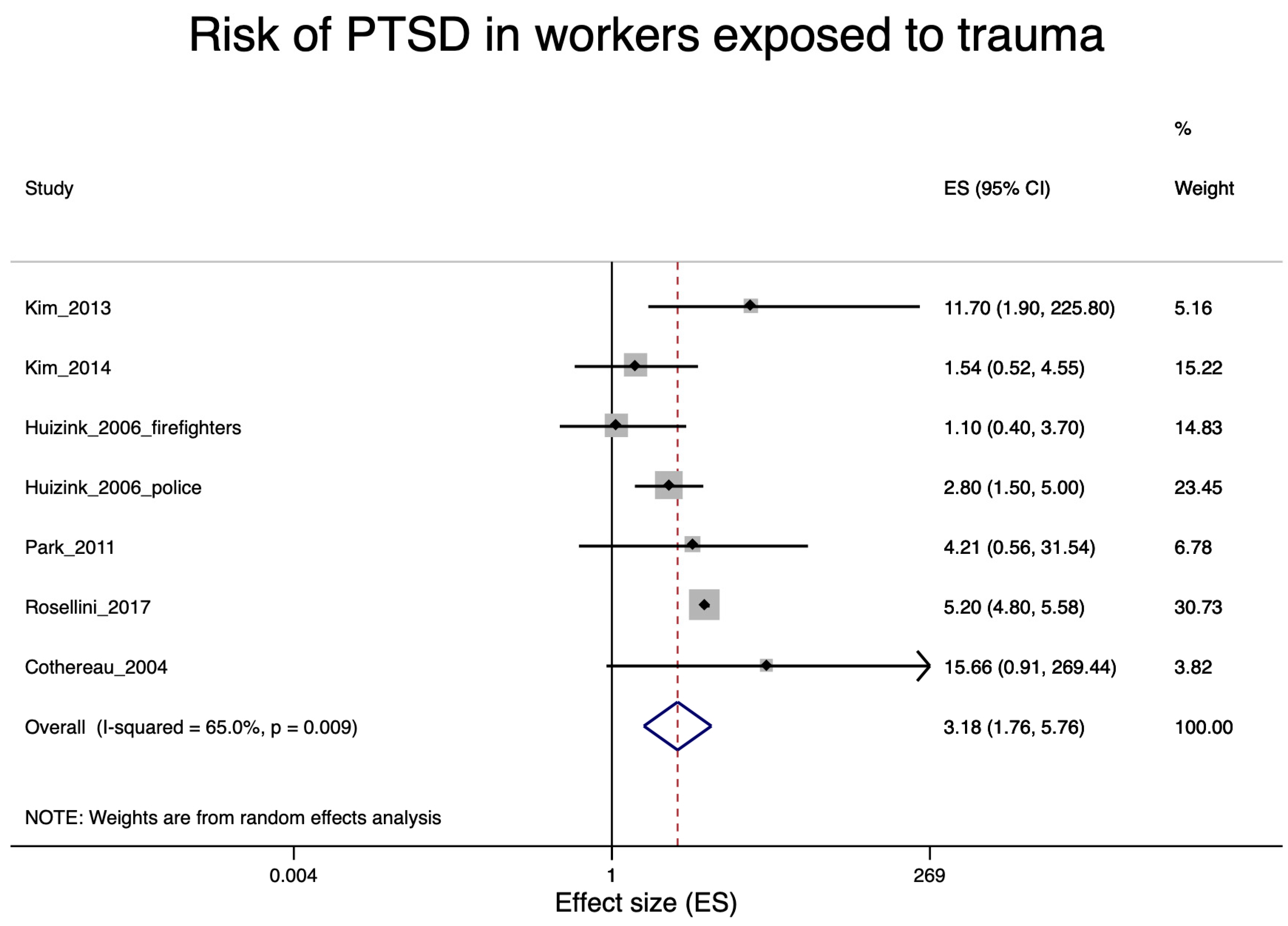
3.5.3. PTSD in Workers Exposed to Occupational Trauma
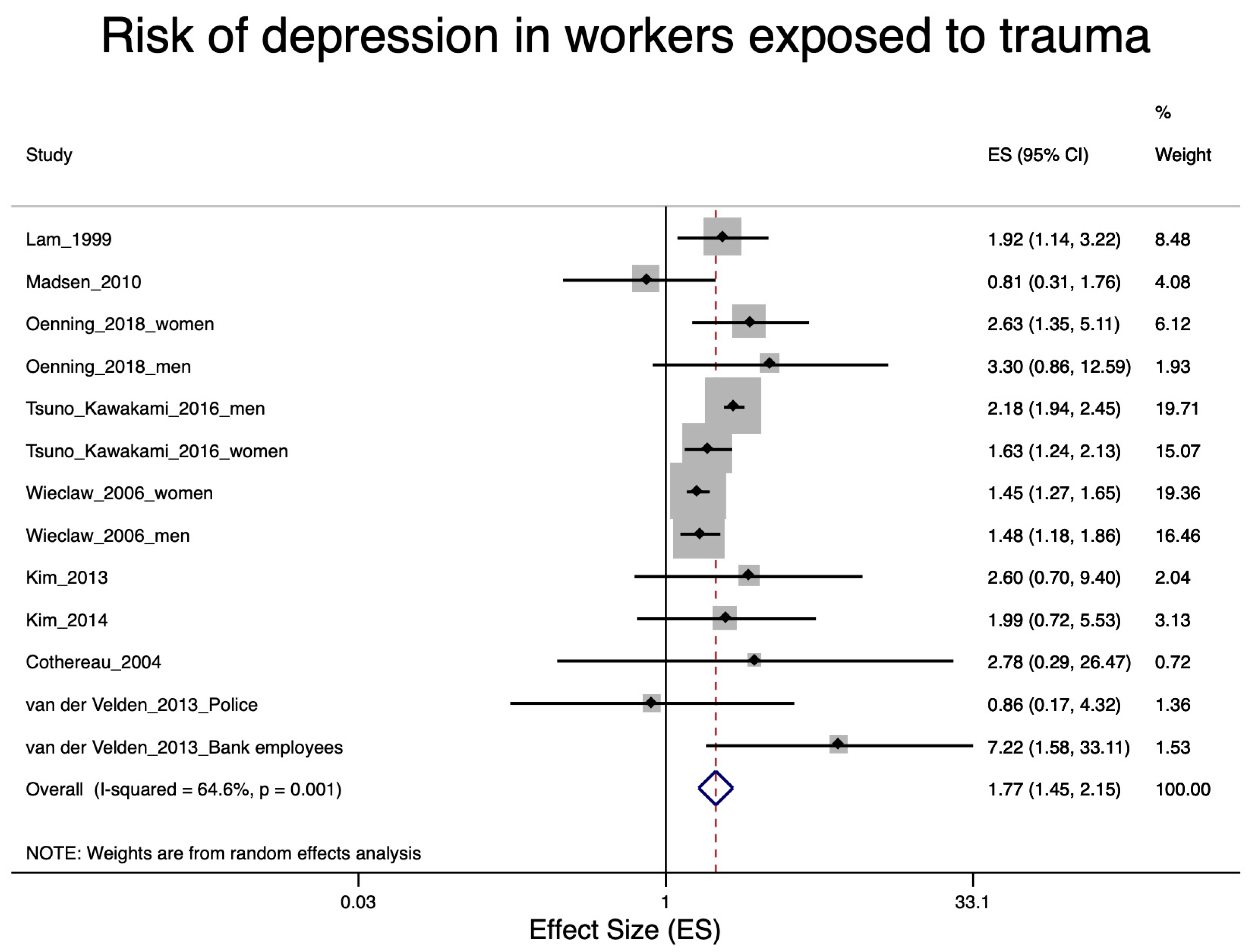
3.5.4. Depression in Workers Exposed to Occupational Trauma
3.6. Quality of Evidence Assessment (GRADE)
3.6.1. PTSD in Soldiers after War Deployment
3.6.2. Depression in Soldiers after War Deployment
3.6.3. Depression in Workers Exposed to Trauma
3.6.4. PTSD in Workers Exposed to Trauma
4. Discussion
4.1. PTSD Risks due to Occupational Trauma
4.2. Depression Risks due to Occupational Trauma
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bonde, J.P.; Utzon-Frank, N.; Bertelsen, M.; Borritz, M.; Eller, N.; Nordentoft, M.; Olesen, K.; Rod, N.H.; Rugulies, R. Risk of depressive disorder following disasters and military deployment: Systematic review with meta-analysis. Br. J. Psychiatry 2016, 208, 330–336. [Google Scholar] [CrossRef]
- Utzon-Frank, N.; Breinegaard, N.; Bertelsen, M.; Borritz, M.; Eller, N.H.; Nordentott, M.; Olesen, K.; Rod, N.H.; Rugulies, R.; Bonde, J.P. Occurrence of delayed-onset post-traumatic stress disorder: A systematic review and meta-analysis of prospective studies. Scand. J. Work Environ. Health 2014, 40, 215–229. [Google Scholar] [CrossRef] [Green Version]
- Magruder, K.M.; Yeager, D.E. The prevalence of PTSD across war eras and the effect of deployment on PTSD: A systematic review and meta-analysis. Psychiatr. Annals 2009, 39. [Google Scholar] [CrossRef]
- Xue, C.; Ge, Y.; Tang, B.; Liu, Y.; Kang, P.; Wang, M.; Zhang, L. A meta-analysis of risk factors for combat-related PTSD among military personnel and veterans. PLoS ONE 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kieffer, C. What Recognition of Work-Related Mental Disorders? A Study on 10 European Countries. Available online: http://www.europeanforum.org/documents/24/eurogip_81en_recognition_wr_mental_disorders_europe.pdf (accessed on 10 December 2020).
- Nienhaus, A.; Drechsel-Schlund, C.; Schambortski, H.; Schablon, A. Gewalt und Diskriminierung am Arbeitsplatz. Bundesgesundheitsblatt Gesundh. Gesundh. 2016, 59, 88–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Netherlands Center for Occupational Diseases. Registration Guidelines: E003 Job-Related Depression; Netherlands Center for Occupational Diseases: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Berger, W.; Coutinho, E.S.F.; Figueira, I.; Marques-Portella, C.; Luz, M.P.; Neylan, T.C.; Marmar, C.R.; Mendlowicz, M.V. Rescuers at risk: A systematic review and meta-regression analysis of the worldwide current prevalence and correlates of PTSD in rescue workers. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 1001–1011. [Google Scholar] [CrossRef] [PubMed]
- Sterud, T.; Ekeberg, Ø.; Hem, E. Health status in the ambulance services: A systematic review. BMC Health Serv. Res. 2006, 6, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hegg-Deloye, S.; Brassard, P.; Jauvin, N.; Prairie, J.; Larouche, D.; Poirier, P.; Tremblay, A.; Corbeil, P. Current state of knowledge of post-traumatic stress, sleeping problems, obesity and cardiovascular disease in paramedics. Emerg. Med. J. 2014, 31, 242–247. [Google Scholar] [CrossRef]
- Bolm-Audorff, U.; Petereit-Haack, G.; Seidler, A. Relationship between Occupational Trauma, Posttraumatic Stress Disorder and Depression—An Assessment of Systematic Reviews. Psychiatr. Prax. 2019, 46, 184–190. [Google Scholar] [CrossRef]
- AMSTAR. AMSTAR Checklist. Available online: https://amstar.ca/Amstar_Checklist.php (accessed on 3 June 2020).
- Shea, B.J.; Grimshaw, J.M.; Wells, G.A.; Boers, M.; Andersson, N.; Hamel, C.; Porter, A.C.; Tugwell, P.; Moher, D.; Bouter, L.M. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Med. Res. Methodol. 2007, 7, 10. [Google Scholar] [CrossRef] [Green Version]
- Shea, B.J.; Hamel, C.; Wells, G.A.; Bouter, L.M.; Kristjansson, E.; Grimshaw, J.; Henry, D.A.; Boers, M. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. J. Clin. Epidemiol. 2009, 62, 1013–1020. [Google Scholar] [CrossRef] [Green Version]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic Criteria From DSM-IV; American Psychiatric Press, Inc.: Washington, DC, USA, 1994. [Google Scholar]
- Aoki, Y.; Malcolm, E.; Yamaguchi, S.; Thornicroft, G.; Henderson, C. Mental illness among journalists: A systematic review. Int. J. Soc. Psychiatry 2013, 59, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Bills, C.B.; Levy, N.A.; Sharma, V.; Charney, D.S.; Herbert, R.; Moline, J.; Katz, C.L. Mental health of workers and volunteers responding to events of 9/11: Review of the literature. Mt. Sinai J. Med. 2008, 75, 115–127. [Google Scholar] [CrossRef] [PubMed]
- Clarner, A.; Graessel, E.; Scholz, J.; Niedermeier, A.; Uter, W.; Drexler, H. Work-related posttraumatic stress disorder (PTSD) and other emotional diseases as consequence of traumatic events in public transportation: A systematic review. Int Arch. Occup. Environ. Health 2015, 88, 549–564. [Google Scholar] [CrossRef] [PubMed]
- Ijaz, S.; Verbeek, J.; Seidler, A.; Lindbohm, M.-L.; Ojajärvi, A.; Orsini, N.; Costa, G.; Neuvonen, K. Night-shift work and breast cancer—A systematic review and meta-analysis. Scand. J. Work Environ. Health 2013, 431–447. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Kai, F.Y. What’s the relative risk?: A method of correcting the odds ratio in cohort studies of common outcomes. JAMA 1998, 280, 1690–1691. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; Debeer, H. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Hulshof, C.T.; Colosio, C.; Daams, J.G.; Ivanov, I.D.; Prakash, K.; Kuijer, P.P.; Leppink, N.; Mandic-Rajcevic, S.; Masci, F.; Van der Molen, H.F. WHO/ILO work-related burden of disease and injury: Protocol for systematic reviews of exposure to occupational ergonomic risk factors and of the effect of exposure to occupational ergonomic risk factors on osteoarthritis of hip or knee and selected other musculoskeletal diseases. Environ. Int. 2019, 125, 554–566. [Google Scholar]
- Romero Starke, K.; Kofahl, M.; Freiberg, A.; Schubert, M.; Groß, M.L.; Schmauder, S.; Hegewald, J.; Kämpf, D.; Stranzinger, J.; Nienhaus, A. Are daycare workers at a higher risk of Parvovirus B19 Infection? A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 1392. [Google Scholar] [CrossRef] [Green Version]
- Romero Starke, K.; Kofahl, M.; Freiberg, A.; Schubert, M.; Groß, M.L.; Schmauder, S.; Hegewald, J.; Kämpf, D.; Stranzinger, J.; Nienhaus, A. The risk of cytomegalovirus infection in daycare workers: A systematic review and meta-analysis. Int. Arch. Occup. Environ. Health 2019, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Petereit-Haack, G.; Bolm-Audorff, U.; Seidler, A. Occupational Risk of Posttraumatic Stress Disorder (PTSD) and Trauma-Related Depression: A Systematic Review. International Prospective Register of Systematic Reviews (PROSPERO). Available online: http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42019122774 (accessed on 1 December 2020).
- Berg, A.M.; Hem, E.; Lau, B.; Ekeberg, Ø. An exploration of job stress and health in the Norwegian police service: A cross sectional study. J. Occup. Med. Toxicol. 2006, 1, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darves-Bornoz, J.M.; Alonso, J.; de Girolamo, G.; Graaf, R.d.; Haro, J.M.; Kovess-Masfety, V.; Lepine, J.P.; Nachbaur, G.; Negre-Pages, L.; Vilagut, G. Main traumatic events in Europe: PTSD in the European study of the epidemiology of mental disorders survey. J. Trauma. Stress 2008, 21, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Feinstein, A. Mexican journalists: An investigation of their emotional health. J. Trauma. Stress 2012, 25, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Feinstein, A.; Owen, J.; Blair, N. A hazardous profession: War, journalists, and psychopathology. Am. J. Psychiatry 2002, 159, 1570–1575. [Google Scholar] [CrossRef] [PubMed]
- Hotopf, M.; Hull, L.; Fear, N.T.; Browne, T.; Horn, O.; Iversen, A.; Jones, M.; Murphy, D.; Bland, D.; Earnshaw, M. The health of UK military personnel who deployed to the 2003 Iraq war: A cohort study. Lancet 2006, 367, 1731–1741. [Google Scholar] [CrossRef]
- Huizink, A.C.; Slottje, P.; Witteveen, A.B.; Bijlsma, J.A.; Twisk, J.W.; Smidt, N.; Bramsen, I.; Van Mechelen, W.; Van der Ploeg, H.M.; Bouter, L.M. Long term health complaints following the Amsterdam Air Disaster in police officers and fire-fighters. Occup. Environ. Med. 2006, 63, 657–662. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.-R.; Yim, H.W.; Jo, S.-J.; Choi, B.; Jeong, S.H.; Lee, K.S.; Park, J.-I.; Chang, S.M. Major depressive disorder, panic disorder, and post-traumatic stress disorder in Korean subway drivers. Int. Arch. Occup. Environ. Health 2013, 86, 471–477. [Google Scholar] [CrossRef]
- Kim, S.-e.; Kim, H.-R.; Park, J.-I.; Lee, H.W.; Lee, J.; Byun, J.; Yim, H.W. The association between psychiatric disorders and work-related problems among subway drivers in Korea. Ann. Occup. Environ. Med. 2014, 26, 39. [Google Scholar] [CrossRef] [Green Version]
- Kline, A.; Falca-Dodson, M.; Sussner, B.; Ciccone, D.S.; Chandler, H.; Callahan, L.; Losonczy, M. Effects of repeated deployment to Iraq and Afghanistan on the health of New Jersey Army National Guard troops: Implications for military readiness. Am. J. Public Health 2010, 100, 276–283. [Google Scholar] [CrossRef]
- Lam, L.; Ross, F.; Cass, D.; Quine, S.; Lazarus, R. The impact of work related trauma on the psychological health of nursing staff: A cross sectional study. Aust. J. Adv. Nurs. 1999, 16, 14–20. [Google Scholar] [PubMed]
- Lehavot, K.; Katon, J.G.; Chen, J.A.; Fortney, J.C.; Simpson, T.L. Post-traumatic stress disorder by gender and veteran status. Am. J. Prev. Med. 2018, 54, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Levin-Rector, A.; Hourani, L.L.; Van Dorn, R.A.; Bray, R.M.; Stander, V.A.; Cartwright, J.K.; Morgan, J.K.; Trudeau, J.; Lattimore, P.K. Predictors of Posttraumatic Stress Disorder, Anxiety Disorders, Depressive Disorders, and Any Mental Health Condition Among US Soldiers and Marines, 2001–2011. J. Trauma. Stress 2018, 31, 568–578. [Google Scholar] [CrossRef] [PubMed]
- Luce, A.; Firth-Cozens, J.; Midgley, S.; Burges, C. After the Omagh bomb: Posttraumatic stress disorder in health service staff. J. Trauma. Stress 2002, 15, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Madsen, I.E.; Diderichsen, F.; Burr, H.; Rugulies, R. Person-related work and incident use of antidepressants: Relations and mediating factors from the Danish work environment cohort study. Scand. J. Work Environ. Health 2010, 36, 435–444. [Google Scholar] [CrossRef] [Green Version]
- Magruder, K.M.; Frueh, B.C.; Knapp, R.G.; Davis, L.; Hamner, M.B.; Martin, R.H.; Gold, P.B.; Arana, G.W. Prevalence of posttraumatic stress disorder in Veterans Affairs primary care clinics. Gen. Hosp. Psychiatry 2005, 27, 169–179. [Google Scholar] [CrossRef]
- Niedhammer, I.; Lesuffleur, T.; Algava, E.; Chastang, J. Classic and emergent psychosocial work factors and mental health. Occup Med. 2015, 65, 126–134. [Google Scholar] [CrossRef] [Green Version]
- Oenning, N.S.X.; Ziegelmann, P.K.; De Goulart, B.N.G.; Niedhammer, I. Occupational factors associated with major depressive disorder: A Brazilian population-based study. J. Affect. Disord. 2018, 240, 48–56. [Google Scholar] [CrossRef]
- Opie, T.; Lenthall, S.; Dollard, M.; Wakerman, J.; MacLeod, M.; Knight, S.; Dunn, S.; Rickard, G. Trends in workplace violence in the remote area nursing workforce. Aust J. Adv. Nurs. 2010, 27, 18. [Google Scholar]
- Park, W. Nurses’ Posttraumatic Stress, Level of Exposure, and Coping Five Years After Hurricane Katrina. Ph.D. Thesis, Georgia State University, Atlanta, GA, USA, 2011. [Google Scholar]
- Proctor, S.; Heeren, T.; White, R.; Wolfe, J.; Borgos, M.; Davis, J.; Pepper, L.; Clapp, R.; Sutker, P.; Vasterling, J. Health status of Persian Gulf War veterans: Self-reported symptoms, environmental exposures and the effect of stress. Int. J. Epidemiol. 1998, 27, 1000–1010. [Google Scholar] [CrossRef]
- Rosellini, A.J.; Street, A.E.; Ursano, R.J.; Chiu, W.T.; Heeringa, S.G.; Monahan, J.; Naifeh, J.A.; Petukhova, M.V.; Reis, B.Y.; Sampson, N.A. Sexual assault victimization and mental health treatment, suicide attempts, and career outcomes among women in the US Army. Am. J. Public Health 2017, 107, 732–739. [Google Scholar] [CrossRef] [PubMed]
- Sareen, J.; Cox, B.J.; Afifi, T.O.; Stein, M.B.; Belik, S.-L.; Meadows, G.; Asmundson, G.J. Combat and peacekeeping operations in relation to prevalence of mental disorders and perceived need for mental health care: Findings from a large representative sample of military personnel. Arch. Gen. Psychiatry 2007, 64, 843–852. [Google Scholar] [CrossRef] [PubMed]
- Sterud, T.; Hem, E.; Ekeberg, Ø.; Lau, B. Health problems and help-seeking in a nationwide sample of operational Norwegian ambulance personnel. BMC Public Health 2008, 8, 3. [Google Scholar] [CrossRef] [Green Version]
- Thomas, M.; Harpaz-Rotem, I.; Tsai, J.; Southwick, S.; Pietrzak, R. Mental and Physical Health Conditions in US Combat Veterans: Results From the National Health and Resilience in Veterans Study. Prim. Care Companion CNS Disord. 2017, 19. [Google Scholar] [CrossRef] [PubMed]
- Tsuno, K.; Kawakami, N. The impact of work-related physical assaults on mental health among Japanese employees with different socioeconomic status: The Japan Work Stress and Health Cohort Study (JSTRESS). SSM Popul. Health 2016, 2, 572–579. [Google Scholar] [CrossRef] [Green Version]
- Van der Velden, P.G.; Rademaker, A.R.; Vermetten, E.; Portengen, M.-A.; Yzermans, J.C.; Grievink, L. Police officers: A high-risk group for the development of mental health disturbances? A cohort study. BMJ Open 2013, 3, e001720. [Google Scholar] [CrossRef] [Green Version]
- Wieclaw, J.; Agerbo, E.; Mortensen, P.B.; Burr, H.; Tüchsen, F.; Bonde, J.P. Work related violence and threats and the risk of depression and stress disorders. J. Epidemiol. Community Health 2006, 60, 771–775. [Google Scholar] [CrossRef] [Green Version]
- Wittchen, H.-U.; Schönfeld, S.; Kirschbaum, C.; Thurau, C.; Trautmann, S.; Steudte, S.; Klotsche, J.; Höfler, M.; Hauffa, R.; Zimmermann, P. Traumatic experiences and posttraumatic stress disorder in soldiers following deployment abroad: How big is the hidden problem? Dtsch. Arztebl. Int. 2012, 109, 559. [Google Scholar]
- Zhao, S.; Xie, F.; Wang, J.; Shi, Y.; Zhang, S.; Han, X.; Sun, Z.; Shi, L.; Li, Z.; Mu, H. Prevalence of workplace violence against Chinese nurses and its association with mental health: A cross-sectional survey. Arch. Psychiatr. Nurs. 2018, 32, 242–247. [Google Scholar] [CrossRef]
- Cothereau, C.; De Beaurepaire, C.; Payan, C.; Cambou, J.; Rouillon, F.; Conso, F. Professional and medical outcomes for French train drivers after “person under train” accidents: Three year follow up study. Occup. Environ. Med. 2004, 61, 488–494. [Google Scholar] [CrossRef] [Green Version]
- Ben-Ezra, M.; Palgi, Y.; Wolf, J.J.; Shrira, A. Psychiatric symptoms and psychosocial functioning among hospital personnel during the Gaza war: A repeated cross–sectional study. Psychiatry Res. 2011, 189, 392–395. [Google Scholar] [CrossRef] [PubMed]
- Rücker, G.; Schwarzer, G.; Carpenter, J.R.; Schumacher, M. Undue reliance on I2 in assessing heterogeneity may mislead. BMC Med. Res. Methodol. 2008, 8, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Priebe, K.; Kleindienst, N.; Schropp, A.; Dyer, A.; Krüger-Gottschalk, A.; Schmahl, C.; Steil, R.; Bohus, M. Defining the index trauma in post-traumatic stress disorder patients with multiple trauma exposure: Impact on severity scores and treatment effects of using worst single incident versus multiple traumatic events. Eur. J. Psychotraumatol. 2018, 9, 1486124. [Google Scholar] [CrossRef] [PubMed]
- Dsm-Iv-tr, A. Diagnostic and Statistical Manual of Mental Disorders, Text Revision; American Psychiatric Association: Washington, DC, USA, 2000; Volume 75, pp. 78–85. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical manual of mental disorders (DSM-5 ®); Psychiatric Association Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Stein, J.Y.; Wilmot, D.V.; Solomon, Z. Does one size fit all? Nosological, clinical, and scientific implications of variations in PTSD Criterion A. J. Anxiety Disord. 2016, 43, 106–117. [Google Scholar] [CrossRef]
- Karam, E.G.; Friedman, M.J.; Hill, E.D.; Kessler, R.C.; McLaughlin, K.A.; Petukhova, M.; Sampson, L.; Shahly, V.; Angermeyer, M.C.; Bromet, E.J. Cumulative traumas and risk thresholds: 12-month PTSD in the World Mental Health (WMH) surveys. Depress. Anxiety 2014, 31, 130–142. [Google Scholar] [CrossRef]
- Gradus, J.L. Prevalence and prognosis of stress disorders: A review of the epidemiologic literature. Clin. Epidemiol. 2017, 9, 251–260. [Google Scholar] [CrossRef]
- Maercker, A.; Lorenz, L. Adjustment disorder diagnosis: Improving clinical utility. World J. Biol. Psychiatry 2018, 19, S3–S13. [Google Scholar] [CrossRef] [Green Version]
- Maercker, A.; Hecker, T. Trauma-und Gewaltfolgen–psychische Auswirkungen. Bundesgesundheitsblatt Gesundh. Gesundh. 2016, 59, 28–34. [Google Scholar] [CrossRef]
- Walter, K.H.; Levine, J.A.; Highfill-McRoy, R.M.; Navarro, M.; Thomsen, C.J. Prevalence of Posttraumatic Stress Disorder and Psychological Comorbidities Among U.S. Active Duty Service Members, 2006–2013. J. Trauma. Stress 2018, 31, 837–844. [Google Scholar] [CrossRef]
- Goetter, E.M.; Hoeppner, S.S.; Khan, A.J.; Charney, M.E.; Wieman, S.; Venners, M.R.; Avallone, K.M.; Rauch, S.A.; Simon, N.M. Combat-Related Posttraumatic Stress Disorder and Comorbid Major Depression in US Veterans: The Role of Deployment Cycle Adversity and Social Support. J. Trauma. Stress 2020. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Major Domains | Minor Domains | Overall | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | Study ID | Outcome | 1. Recruitment Procedure & Follow-up (in Cohort Studies) | 2. Exposure Definition and Measurement | 3. Outcome. Source and Validation | 4. Confounding and Effect Modification | 5. Analysis Method: Methods to Reduce Research Specific Bias | 6. Chronology | 7 Blinding | 8. Funding | 9. Conflict of Interest | |
| 1 | Berg et al. 2006 [27] | Depression | 0 | 0 | 2 | 2 | 0 | 0 | 1 | 2 | 2 | 0 |
| 2 | Darves-Bornoz et al. 2008 [28] | PTSD | 2 | 0 | 2 | 0 | 0 | 0 | 1 | 2 | 1 | 0 |
| 3 | Feinstein et al. 2002 [29] | PTSD, Depression | 2 | 2 | 2 | 2 | 0 | 0 | 1 | 2 | 1 | 0 |
| 4 | Feinstein 2012 [30] | PTSD, Depression | 2 | 2 | 2 | 0 | 0 | 0 | 1 | 1 | 1 | 0 |
| 5 | Hotopf et al. 2006 [31] | PTSD | 2 | 2 | 2 | 2 | 2 | 0 | 1 | 2 | 0 | 0 |
| 6 | Huizink et al 2006 [32] | PTSD | 2 | 2 | 2 | 2 | 2 | 0 | 1 | 1 | 1 | 0 |
| 7 | Kim et al. 2013 [33] | PTSD, Depression | 2 | 2 | 2 | 2 | 2 | 0 | 1 | 2 | 1 | 0 |
| 8 | Kim et al. 2014 [34] | PTSD, Depression | 2 | 2 | 2 | 2 | 2 | 0 | 1 | 2 | 1 | 0 |
| 9 | Kline et al. 2010 [35] | PTSD, Depression | 2 | 2 | 2 | 2 | 2 | 0 | 1 | 2 | 0 | 0 |
| 10 | Lam et al. 1999 [36] | Depression | 2 | 2 | 2 | 0 | 2 | 0 | 1 | 1 | 1 | 0 |
| 11 | Lehavot et al. 2018 [37] | PTSD | 2 | 2 | 2 | 0 | 2 | 0 | 1 | 2 | 2 | 0 |
| 12 | Levin-Rector et al. 2018 [38] | PTSD, Depression | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 2 |
| 13 | Luce et al. 2002 [39] | PTSD | 0 | 3 | 3 | 0 | 0 | 0 | 1 | 1 | 1 | 0 |
| 14 | Madsen et al. 2010 [40] | Depression | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 3 | 1 | 2 |
| 15 | Magruder et al. 2005 [41] | PTSD | 2 | 2 | 2 | 2 | 2 | 0 | 1 | 2 | 1 | 0 |
| 16 | Niedhammer et al. 2015 [42] | Depression | 2 | 2 | 2 | 2 | 2 | 0 | 1 | 2 | 2 | 0 |
| 17 | Oenning et al. 2018 [43] | Depression | 2 | 2 | 2 | 2 | 2 | 0 | 1 | 2 | 2 | 0 |
| 18 | Opie et al. 2010 [44] | PTSD | 0 | 2 | 2 | 0 | 0 | 0 | 1 | 1 | 1 | 0 |
| 19 | Park et al. 2011 [45] | PTSD | 0 | 2 | 2 | 0 | 0 | 0 | 1 | 1 | 1 | 0 |
| 20 | Proctor et al. 1998 [46] | PTSD | 2 | 2 | 0 | 0 | 0 | 0 | 1 | 2 | 1 | 0 |
| 21 | Rosellini et al. 2017 [47] | PTSD | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 2 |
| 22 | Sareen et al. 2007 [48] | PTSD Depression | 2 | 2 | 2 | 2 | 2 | 0 | 0 | 2 | 2 | 0 |
| 23 | Sterud et al. 2008 [49] | Depression | 0 | 2 | 2 | 2 | 0 | 0 | 1 | 2 | 2 | 0 |
| 24 | Thomas et al. 2017 [50] | PTSD Depression | 2 | 2 | 2 | 2 | 2 | 0 | 1 | 2 | 2 | 0 |
| 25 | Tsuno et al. 2016 [51] | Depression | 2 | 2 | 2 | 0 | 2 | 0 | 1 | 2 | 2 | 0 |
| 26 | van der Velden et al. 2013 [52] | Depression | 2 | 2 | 2 | 2 | 2 | 0 | 2 | 1 | 2 | 0 |
| 27 | Wieclaw et al. 2006 [53] | Depression | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| 28 | Wittchen et al. 2012 [54] | PTSD | 2 | 2 | 2 | 0 | 0 | 0 | 1 | 2 | 2 | 0 |
| 29 | Zhao et al. 2018 [55] | Depres-sion | 2 | 2 | 2 | 0 | 2 | 0 | 1 | 2 | 2 | 0 |
| 30 | Cothereau et al. 2003 [56] | PTSD, Depression | 2 | 2 | 2 | 2 | 0 | 0 | 1 | 1 | 1 | 0 |
| 31 | Ben-Esra et al. 2011 [57] | PTSD, Depression | 2 | 2 | 2 | 2 | 0 | 0 | 1 | 1 | 1 | 0 |
| Risk | Quality of Study Limitations, ↓ | Indirect-Ness of Evidence: ↓ | Inconsistency: ↓ | Imprecision, Range Confidence Interval Effect Size > 2.0: ↓ | Publication Bias, Yes: ↓ | Effect Estimate >2.0: ↑ >5.0: ↑↑ | Dose-Response Effect: ↑ | Residual Confounding: ↑ | Overall Certainty (High, Moderate, Low) |
|---|---|---|---|---|---|---|---|---|---|
| PTSD in soldiers after war deployment | no (-) 1 | no (-) | no (-) 2 | no (-) 1.83–2.60 | no - | no (-) 3 2.18 (1.83–2.60) | no - | no - | moderate |
| Depression in soldiers after war deployment | no (-) 4 | no (-) | no (-) 5 | no (-) 1.06–1.25 | no - | no (-) 1.15 (1.06–1.25) | no - | no - | moderate |
| Depression in workers after exposure to trauma | no (-) 6 | no (-) | no (-) 7 | no (-) 1.45–2.15 | no - | no (-) 1.77 (1.45–2.15) | no - | no - | moderate |
| PTSD in workers after exposure to trauma | no (-) 8 | no (-) | no (-) 9 | yes ↓ 1.76–5.76 | no - | yes ↑↑ 10 3.18 (1.76–5.76) | no - | no - | high |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petereit-Haack, G.; Bolm-Audorff, U.; Romero Starke, K.; Seidler, A. Occupational Risk for Post-Traumatic Stress Disorder and Trauma-Related Depression: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 9369. https://doi.org/10.3390/ijerph17249369
Petereit-Haack G, Bolm-Audorff U, Romero Starke K, Seidler A. Occupational Risk for Post-Traumatic Stress Disorder and Trauma-Related Depression: A Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(24):9369. https://doi.org/10.3390/ijerph17249369
Chicago/Turabian StylePetereit-Haack, Gabriela, Ulrich Bolm-Audorff, Karla Romero Starke, and Andreas Seidler. 2020. "Occupational Risk for Post-Traumatic Stress Disorder and Trauma-Related Depression: A Systematic Review with Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 24: 9369. https://doi.org/10.3390/ijerph17249369
APA StylePetereit-Haack, G., Bolm-Audorff, U., Romero Starke, K., & Seidler, A. (2020). Occupational Risk for Post-Traumatic Stress Disorder and Trauma-Related Depression: A Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health, 17(24), 9369. https://doi.org/10.3390/ijerph17249369