Oral Health Profiles and Related Quality of Life in Thalassemia Children in Relation to Iron Overload: A Cross-Sectional Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Interview and Questionnaire
2.3. Saliva Sampling
2.4. Oral Clinical Examination
2.5. Ethical Considerations
2.6. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Schwartz, E.; Cohen, A.; Surrey, S. Overview of the β Thalassemias: Genetic and Clinical Aspects. Hemoglobin 1988, 12, 551–564. [Google Scholar] [CrossRef]
- Porter, J.B. A risk-benefit assessment of iron-chelation therapy. Drug Saf. 1997, 17, 407–421. [Google Scholar] [CrossRef]
- Taher, A.T.; Saliba, A.N. Iron overload in thalassemia: Different organs at different rates. Hematol. Am. Soc. Hematol. Educ. Progr. 2017, 2017, 265–271. [Google Scholar] [CrossRef] [Green Version]
- Coates, T.D.; Carson, S.; Wood, J.C.; Berdoukas, V. Management of iron overload in hemoglobinopathies: What is the appropriate target iron level? Ann. N. Y. Acad. Sci. 2016, 1368, 95–106. [Google Scholar] [CrossRef]
- Clarke, S.-A.; Skinner, R.; Guest, J.; Darbyshire, P.; Cooper, J.; Shah, F.; Roberts, I.; Eiser, C. Health-related quality of life and financial impact of caring for a child with Thalassaemia Major in the UK. Child Care Health Dev. 2010, 36, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Thavorncharoensap, M.; Torcharus, K.; Nuchprayoon, I.; Riewpaiboon, A.; Indaratna, K.; Ubol, B.-O. Factors affecting health-related quality of life in Thai children with thalassemia. BMC Hematol. 2010, 10, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adam, S. Quality of life outcomes in thalassaemia patients in Saudi Arabia: A cross-sectional study. East. Mediterr. Health J. 2019, 25, 887–895. [Google Scholar] [CrossRef] [PubMed]
- Adam, S.S.; Afifi, H.H.; Thomas, M.; Magdy, P.; El-Kamah, G. Quality of Life Outcomes in a Pediatric Thalassemia Population in Egypt. Hemoglobin 2017, 13, 1–5. [Google Scholar] [CrossRef]
- Abetz-Webb, L.; Baladi, J.-F.; Jones, P.; Rofail, D. The impact of iron overload and its treatment on quality of life: Results from a literature review. Health Qual. Life Outcomes 2006, 4, 1–73. [Google Scholar] [CrossRef] [Green Version]
- Porter, J.; Bowden, D.K.; Economou, M.; Troncy, J.; Ganser, A.; Habr, D.; Martin, N.; Gater, A.; Rofail, D.; Abetz-Webb, L.; et al. Health-Related Quality of Life, Treatment Satisfaction, Adherence and Persistence in β-Thalassemia and Myelodysplastic Syndrome Patients with Iron Overload Receiving Deferasirox: Results from the EPIC Clinical Trial. Anemia 2012, 2012, 297641. [Google Scholar] [CrossRef] [Green Version]
- Adeyemo, T.A.; Adediran, A.; Akanmu, A.S.; Adeyemo, W.L.; Akinbami, A.J.A. Orofacial manifestations of hematological disorders: Anemia and hemostatic disorders. Indian J. Dent. Res. 2011, 22, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Andreu-Arasa, V.C.; Chapman, M.N.; Kuno, H.; Fujita, A.; Sakai, O. Craniofacial Manifestations of Systemic Disorders: CT and MR Imaging Findings and Imaging Approach. Radiographics 2018, 38, 890–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cutando, A.; Gil Montoya, J.A.; Garrido, J.D.D.L.-G. Thalassemias and their dental implications. Med. Oral 2002, 7, 36–45. [Google Scholar]
- Phrai-In, N.; Noikeaw, J.; Sukprasert, N.; Taya, T.; Samnieng, P. Oral Health Status and Impact on Oral Health-Related Quality of Life in Children with Thalassemia Major. UI Proc. Health Med. 2017, 1, 144–146. [Google Scholar] [CrossRef] [Green Version]
- Babu, N.S.V.; Shah, S. Comparative Assessment of Salivary Flow Rate, Buffering Capacity, Resting PH and Dental Caries in Children with Beta Thalassemia. J. Middle East N. Afr. Sci. 2018, 4, 18–22. [Google Scholar] [CrossRef]
- Akcalı, A.; Yıldız, M.S.; Akcalı, Z.; Huck, O.; Friedmann, A.; Akcalı, A.; Mehmet, S.Y.; Zeynep, A.; Olivier, H.; Anton, F. Periodontal condition of patients with Thalassemia Major: A systematic review and meta-analysis. Arch. Oral Biol. 2019, 102, 113–121. [Google Scholar] [CrossRef]
- Lugliè, P.F.; Campus, G.; Deiola, C.; Mela, M.G.; Gallisai, D. Oral condition, chemistry of saliva, and salivary levels of Streptococcus mutans in thalassemic patients. Clin. Oral Investig. 2002, 6, 223–226. [Google Scholar] [CrossRef]
- Lattanzi, A.P.; Silveira, F.M.; Guimarães, L.; Antunes, L.A.; dos Santos Antunes, L.; Assaf, A.V. Effects of oral health promotion programs on adolescents’ oral health related quality of life: A systematic review. Int. J. Dent. Hyg. 2020. [Google Scholar] [CrossRef]
- Slade, G. (Ed.) Measuring Oral Health and Quality of Life. In Dental Ecology; University of North Carolina: Chapel Hill, NC, USA, 1996. [Google Scholar]
- Amirabadi, F.; Saravani, S.; Miri-Aliabad, G.; Khorashadi-Zadeh, M. The Association between Dental Health Status and Oral Health-Related Quality of Life of Children Diagnosed with beta-Thalassemia Major in Zahedan City, Iran. Int. J. Pediatr. 2019, 7, 8985–8991. [Google Scholar]
- Ebeid, F.S.; Khan, N.I. The Adverse Impact of Thalassemia Major on Adolescents’ Oral Health-related Quality of Life. J. Pediatr. Hematol. 2020, 42, e345–e351. [Google Scholar] [CrossRef]
- Farsi, N.J.; El-Housseiny, A.A.; Farsi, D.J.; Farsi, N.M. Validation of the Arabic Version of the Early Childhood Oral Health Impact Scale (ECOHIS). BMC Oral Health 2017, 17, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pahel, B.T.; Rozier, R.G.; Slade, G.D. Parental perceptions of children’s oral health: The Early Childhood Oral Health Impact Scale (ECOHIS). Health Qual. Life Outcomes 2007, 5, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ismail, N.S.; Ghani, N.M.; Supaat, S.; Kharuddin, A.F.; Ardini, Y.D. The early childhood oral health impact scale (ECOHIS): Assessment tool in oral health related quality of life. J. Int. Dent. Med. Res. 2018, 11, 162–168. [Google Scholar]
- Heintze, U.; Birkhed, D.; Björn, H. Secretion rate and buffer effect of resting and stimulated whole saliva as a function of age and sex. Swed. Dent. J. 1983, 7, 227–238. [Google Scholar] [PubMed]
- Oleary, T.J.; Drake, R.B.; Naylor, J.E. The Plaque Control Record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef] [PubMed]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar]
- World Medical Association. World Medical Association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Meuric, V.; Lainé, F.; Boyer, E.; Le Gall-David, S.; Oger, E.; Bourgeois, D.; Bouchard, P.; Bardou-Jacquet, E.; Turmel, V.; Bonnaure-Mallet, M.; et al. Periodontal status and serum biomarker levels in HFE haemochromatosis patients. A case-series study. J. Clin. Periodontol. 2017, 44, 892–897. [Google Scholar] [CrossRef] [Green Version]
- Catunda, R.Q.; Levin, L.; Kornerup, I.; Gibson, M.P. Prevalence of Periodontitis in Young Populations: A Systematic Review. Oral Health Prev. Dent. 2019, 17, 195–202. [Google Scholar]
- Ali, S.S.; Tarawah, A.M.; Al-Hawsawi, Z.M.; Zolaly, M.A.; Turkustani, W. Comprehensive patient care improves quality of life in transfusion dependent patients with β-thalassemia. Saudi Med. J. 2015, 36, 575–579. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | All BTM Participants (n = 39) | Participants with SFL <2000 ng/mL (n = 20) | Participants with SFL ≥2000 ng/mL (n = 19) | p-Value |
|---|---|---|---|---|
| Age-years (±SD) | 9 (3) | 9 (3) | 10 (3) | 0.683 |
| Gender-F/M (%) | 24 (62)/15 (38) | 11 (55)/9 (45) | 13 (68)/6 (32) | 0.389 |
| Body Mass Index–kg/m2 (±SD) | 15.3 (2) | 15.6 (2) | 15.1 (3) | 0.593 |
| Saliva Secretion rate-mL/min (±SD) | 2.8 (1) | 3.1 (1) | 2.6 (1) | 0.538 |
| Plaque Index-% (±SD) | 70 (29) | 73 (31) | 67 (28) | 0.877 |
| Gingival Bleeding Index-% (±SD) | 38 (25) | 40 (25) | 37 (26) | 0.944 |
| Decayed, missing and filled tooth surfaces (±SD) | 3.2 (4) | 3.0 (4) | 3.4 (3) | 0.349 |
| Number of decayed tooth surfaces (±SD) | 2.3 (3) | 1.9 (2) | 2.8 (3) | 0.399 |
| Number of missing tooth surfaces (±SD) | 1 (1) | 0.4 (1) | 0.6 (1) | 0.280 |
| Number of filled tooth surfaces (±SD) | 0 (0) | 0.1 (0) | 0.0 (0) | 0.330 |
| Early Childhood Oral Health Impact Scale (ECOHIS) (±SD) | 4.5 (4) | 3.8 (4) | 5.3 (5) | 0.334 |
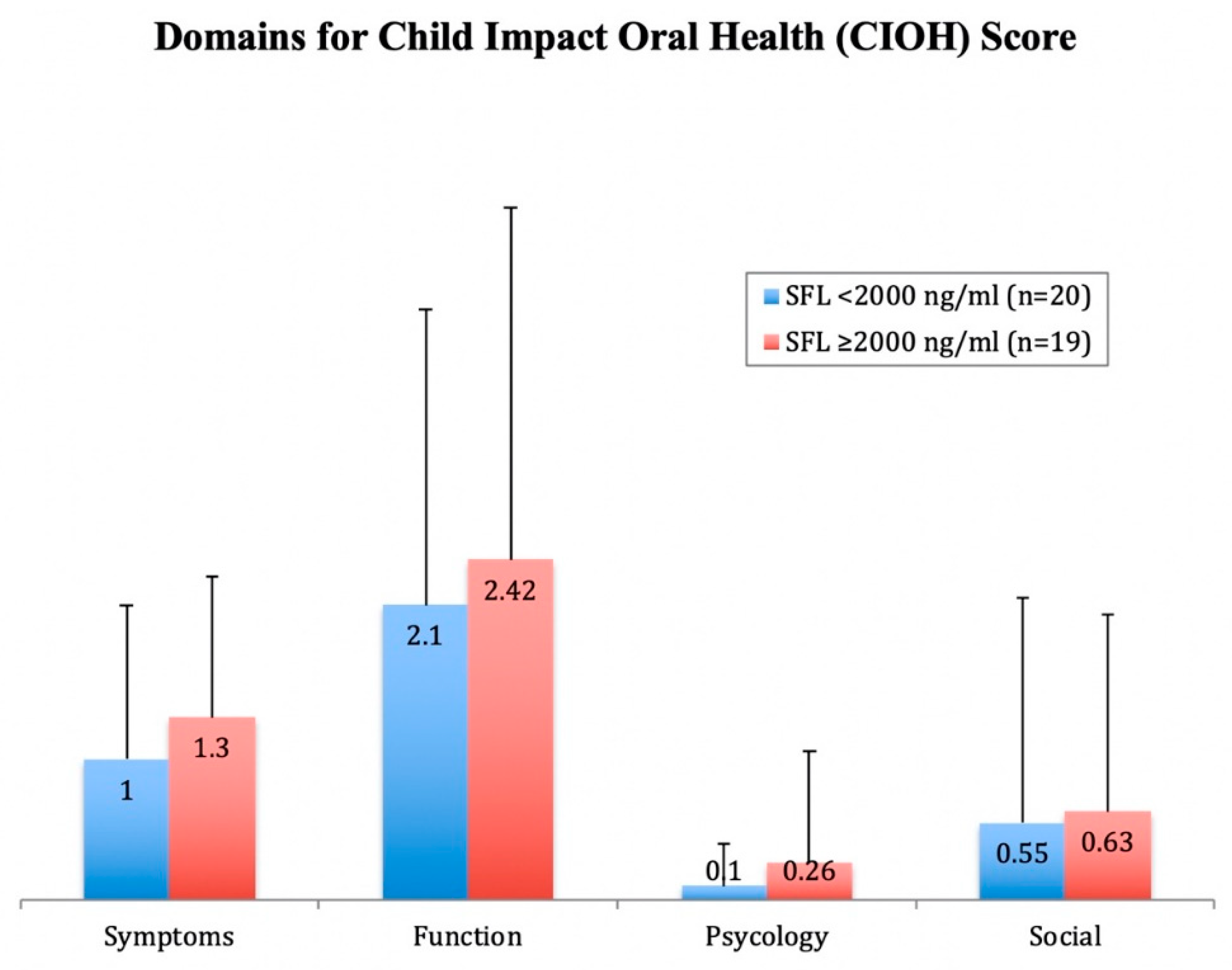
| Child Impact Oral Health (CIOH) Section (±SD) | 4.2 (4) | 3.8 (4) | 4.6 (4) | 0.598 |
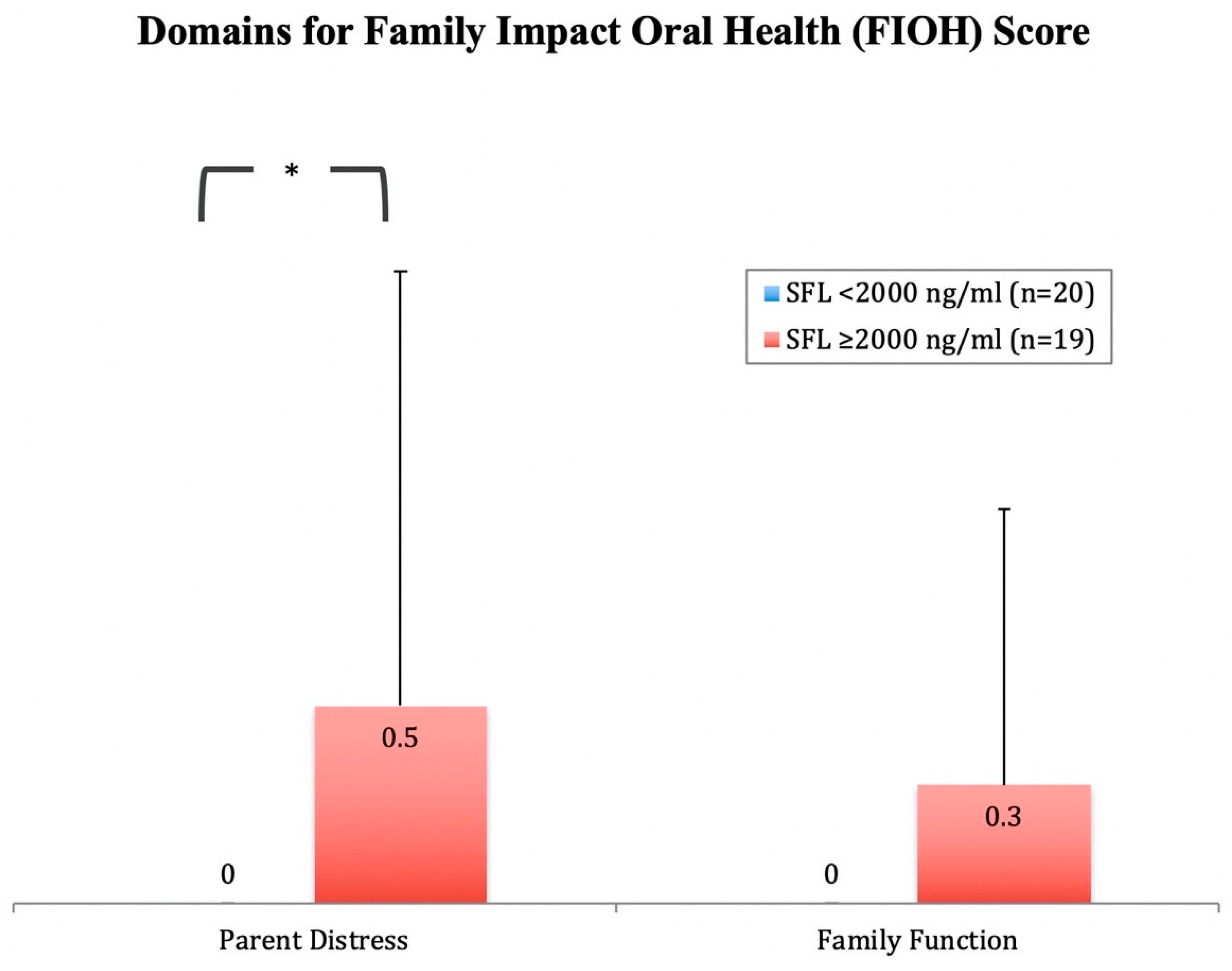
| Family Impact Oral Health (FIOH) Section (±SD) | 0.4 (1) | 0.0 (0) | 0.7 (2) | 0.033 * |
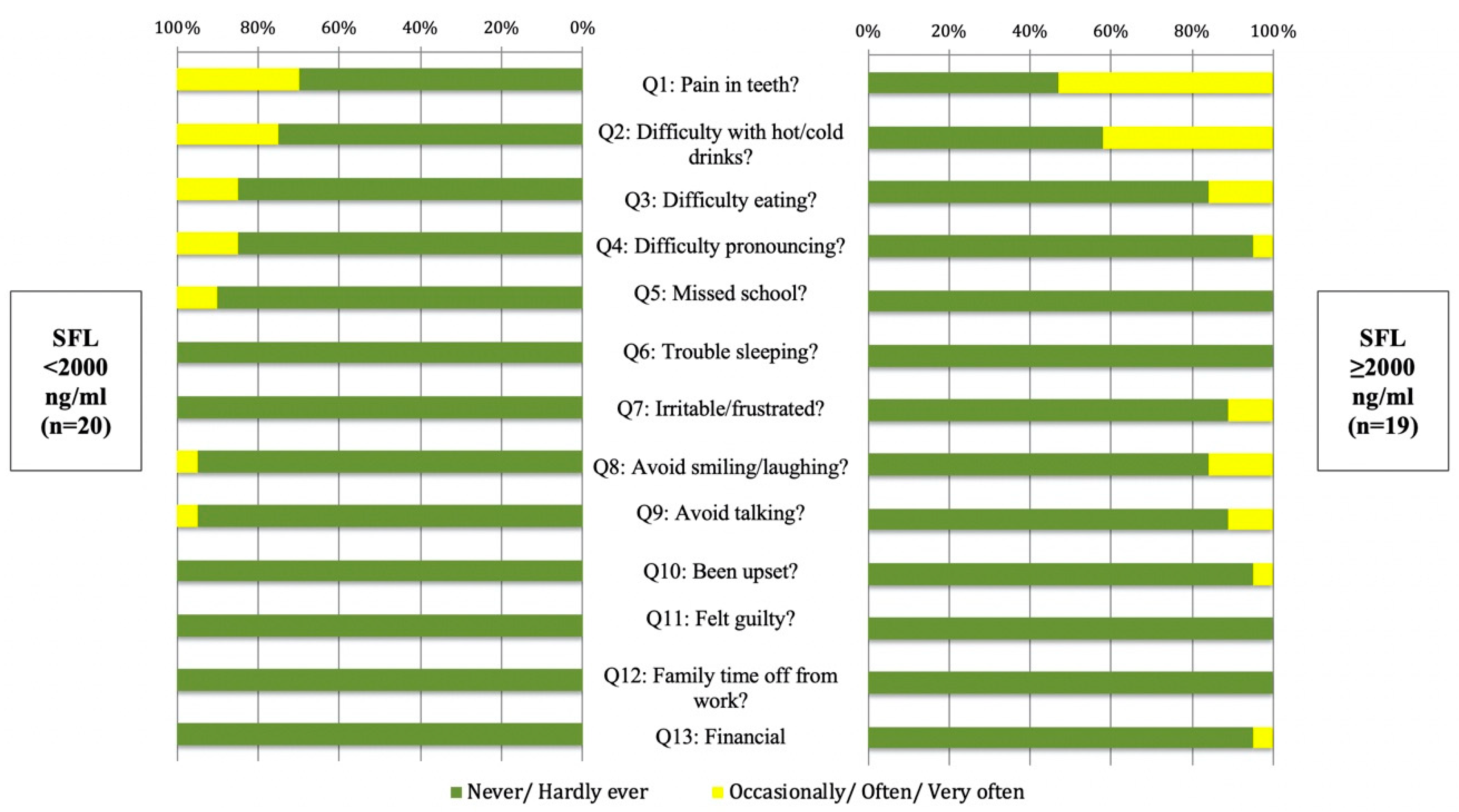
| Domain | Never/Hardly Ever | Occasionally/Often/Very Often |
|---|---|---|
| Question | (%) | (%) |
| Child Symptoms Domain | ||
| 23 (59) | 16 (41) |
| Child Function Domain | ||
| How often has your child … because of dental problems or dental treatments? | ||
| 26 (67) | 13 (33) |
| 33 (85) | 6 (15) |
| 35 (90) | 4 (10) |
| 37 (95) | 2 (5) |
| Child Psychological Domain | ||
| How often has your child … because of dental problems or dental treatments? | ||
| 39 (100) | 0 (0) |
| 37 (95) | 2 (5) |
| Child Self-Image/Social Interaction Domain | ||
| How often has your child … because of dental problems or dental treatments? | ||
| 35 (90) | 4 (10) |
| 36 (92) | 3 (8) |
| Parent Distress Domain | ||
| How often have you or another family member … because of your child’s dental problems or dental treatments? | ||
| 38 (97) | 1 (3) |
| 39 (100) | 0 (0) |
| Family Function Domain | ||
| How often … | ||
| 39 (100) | 0 (0) |
| 38 (97) | 1 (3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fadel, H.T.; Zolaly, M.A.; Alharbi, M.O.; Qarah, L.A.; Alrehili, M.S.; Alamri, A.D.; Tarawah, A.M. Oral Health Profiles and Related Quality of Life in Thalassemia Children in Relation to Iron Overload: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 9444. https://doi.org/10.3390/ijerph17249444
Fadel HT, Zolaly MA, Alharbi MO, Qarah LA, Alrehili MS, Alamri AD, Tarawah AM. Oral Health Profiles and Related Quality of Life in Thalassemia Children in Relation to Iron Overload: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2020; 17(24):9444. https://doi.org/10.3390/ijerph17249444
Chicago/Turabian StyleFadel, Hani T., Mohammed A. Zolaly, Manal O. Alharbi, Lujain A. Qarah, Maher S. Alrehili, Abdulaziz D. Alamri, and Ahmed M. Tarawah. 2020. "Oral Health Profiles and Related Quality of Life in Thalassemia Children in Relation to Iron Overload: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 17, no. 24: 9444. https://doi.org/10.3390/ijerph17249444
APA StyleFadel, H. T., Zolaly, M. A., Alharbi, M. O., Qarah, L. A., Alrehili, M. S., Alamri, A. D., & Tarawah, A. M. (2020). Oral Health Profiles and Related Quality of Life in Thalassemia Children in Relation to Iron Overload: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 17(24), 9444. https://doi.org/10.3390/ijerph17249444