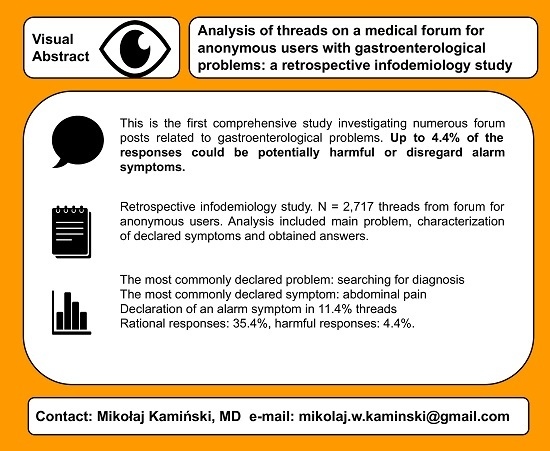
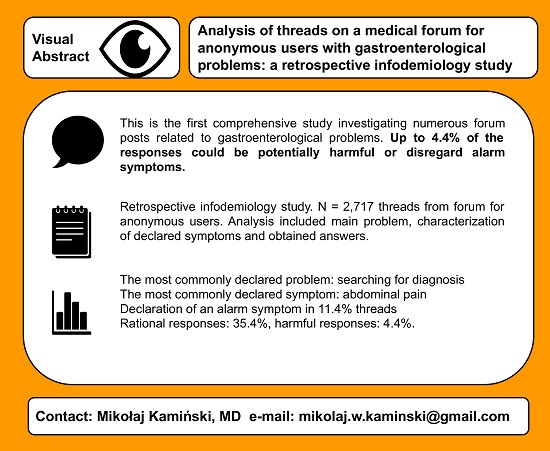
Analysis of Answers to Queries among Anonymous Users with Gastroenterological Problems on an Internet Forum

 , , , , , and
, , , , , and 
Abstract
:
1. Introduction
2. Material and Methods
2.1. Data Collection
2.2. Data Analysis
3. Results
3.1. General Characteristics
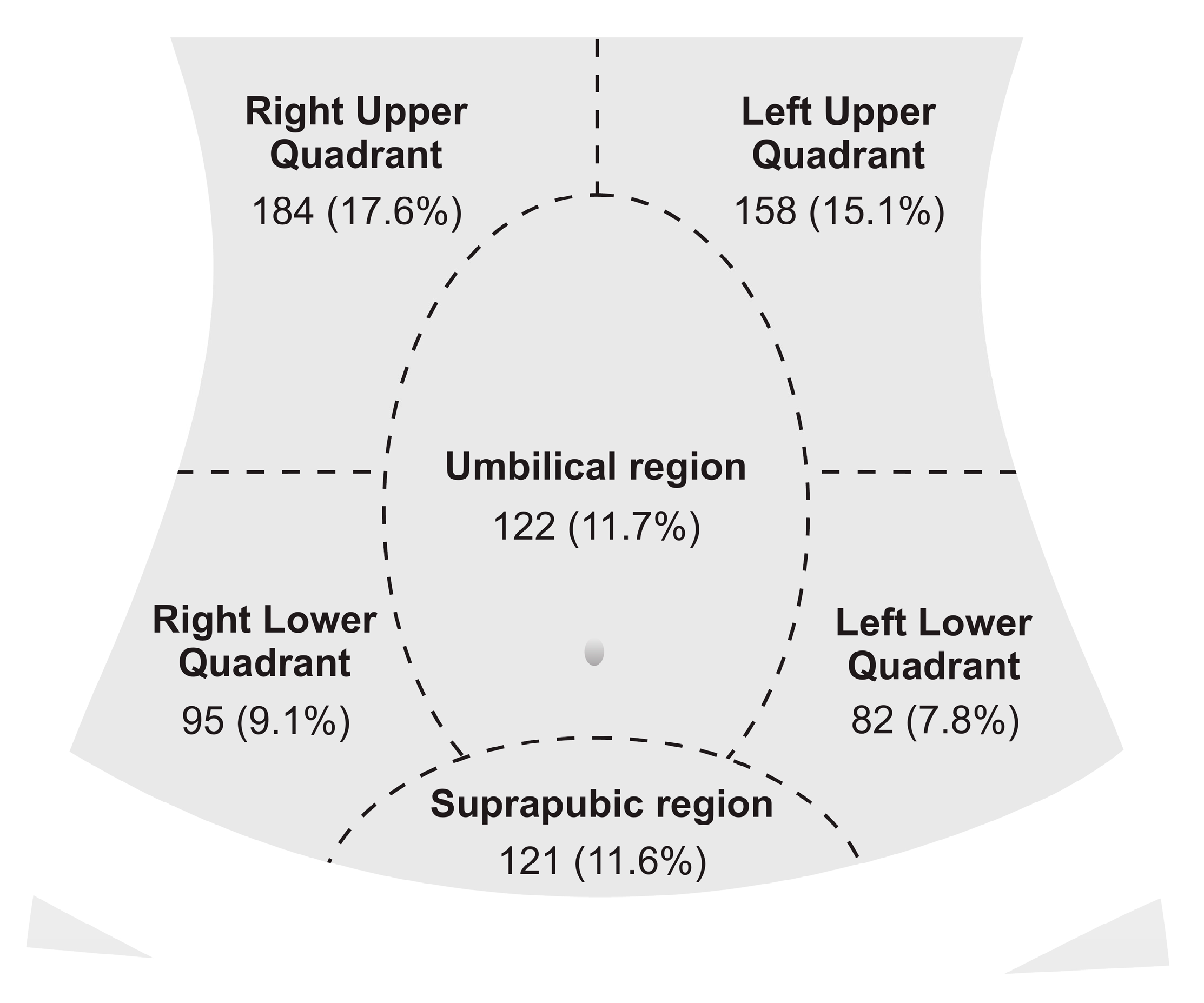
3.2. Declared Symptoms
3.3. Declared Conditions
3.4. Posts with Answers
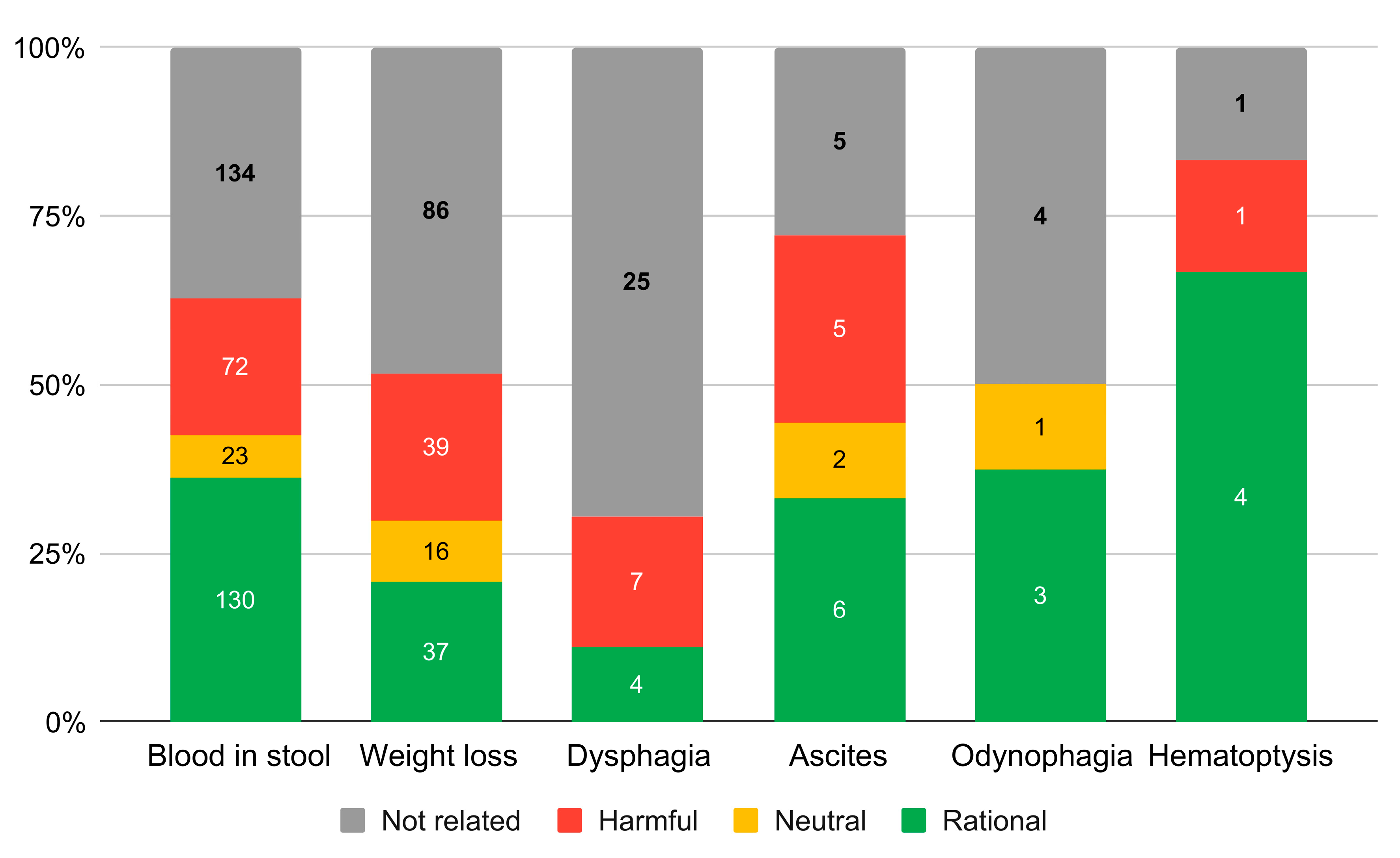
3.5. Analysis of the Answers
3.6. Duplicated Posts
4. Discussion
4.1. Main Findings
4.2. Strengths and Practical Implications
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Spiegel, B.M.R.; Khanna, D.; Bolus, R.; Agarwal, N.; Khanna, P.; Chang, L. Understanding gastrointestinal distress: A framework for clinical practice. Am. J. Gastroenterol. 2011, 106, 380–385. [Google Scholar] [CrossRef] [Green Version]
- Oliveria, S.A.; Christos, P.J.; Talley, N.J.; Dannenberg, A.J. Heartburn Risk Factors, Knowledge, and Prevention Strategies: A Population-Based Survey of Individuals with Heartburn. Arch. Intern. Med. 1999, 159, 1592. [Google Scholar] [CrossRef] [Green Version]
- Edwards, N.I.; Jones, D. The prevalence of faecal incontinence in older people living at home. Age Ageing 2001, 30, 503–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitehead, W.E.; Borrud, L.; Goode, P.S.; Meikle, S.; Mueller, E.R.; Tuteja, A.; Weidner, A.; Weinstein, M.; Ye, W. Pelvic Floor Disorders Network Fecal incontinence in US adults: Epidemiology and risk factors. Gastroenterology 2009, 137, 512–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, A.G.; Scherer, A.M.; Zikmund-Fisher, B.J.; Larkin, K.; Barnes, G.D.; Fagerlin, A. Prevalence of and Factors Associated with Patient Nondisclosure of Medically Relevant Information to Clinicians. JAMA Netw. Open 2018, 1, e185293. [Google Scholar] [CrossRef] [PubMed]
- Baeten, R.; Spasova, S.; Vanhercke, B.; Coster, S. Inequalities in Access to Healthcare: A Study of National Policies 2018; European Commission: Brussel, Belgium, 2018. [Google Scholar]
- Martini, M.; Bragazzi, N. Googling for neurological disorders: From seeking health-related information to patient empowerment, advocacy and open self-disclosure in the Neurology 2.0 era. J. Med. Internet Res. 2019. [Google Scholar] [CrossRef] [PubMed]
- Andreassen, H.K.; Bujnowska-Fedak, M.M.; Chronaki, C.E.; Dumitru, R.C.; Pudule, I.; Santana, S.; Voss, H.; Wynn, R. European citizens’ use of E-health services: A study of seven countries. BMC Public Health 2007, 7, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDaid, D.; Park, A.-L. Online Health: Untangling the Web; Bupa: London, UK, 2010. [Google Scholar]
- Beck, F.; Richard, J.-B.; Nguyen-Thanh, V.; Montagni, I.; Parizot, I.; Renahy, E. Use of the internet as a health information resource among French young adults: Results from a nationally representative survey. J. Med. Internet Res. 2014, 16, e128. [Google Scholar] [CrossRef]
- Kamiński, M.; Loniewski, I.; Misera, A.; Marlicz, W. Heartburn-Related Internet Searches and Trends of Interest across Six Western Countries: A Four-Year Retrospective Analysis Using Google Ads Keyword Planner. IJERPH 2019, 16, 4591. [Google Scholar] [CrossRef] [Green Version]
- Vydiswaran, V.G.V.; Reddy, M. Identifying peer experts in online health forums. BMC Med. Inf. Decis. Mak. 2019, 19, 68. [Google Scholar] [CrossRef] [Green Version]
- Gavrila, V.; Garrity, A.; Hirschfeld, E.; Edwards, B.; Lee, J.M. Peer Support Through a Diabetes Social Media Community. J. Diabetes Sci. Technol. 2019, 13, 493–497. [Google Scholar] [CrossRef] [PubMed]
- Kauw, D.; Repping-Wuts, H.; Noordzij, A.; Stikkelbroeck, N.; Hermus, A.; Faber, M. The contribution of online peer-to-peer communication among patients with adrenal disease to patient-centered care. J. Med. Internet Res. 2015, 17, e54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wray, J.; Brown, K.; Tregay, J.; Crowe, S.; Knowles, R.; Bull, K.; Gibson, F. Parents’ Experiences of Caring for Their Child at the Time of Discharge After Cardiac Surgery and During the Postdischarge Period: Qualitative Study Using an Online Forum. J. Med. Internet Res. 2018, 20, e155. [Google Scholar] [CrossRef]
- Saran, I.; Fink, G.; McConnell, M. How does anonymous online peer communication affect prevention behavior? Evidence from a laboratory experiment. PLoS ONE 2018, 13, e0207679. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. Infodemiology and Infoveillance. Am. J. Prev. Med. 2011, 40, S154–S158. [Google Scholar] [CrossRef]
- Eysenbach, G. Infodemiology and infoveillance: Framework for an emerging set of public health informatics methods to analyze search, communication and publication behavior on the Internet. J. Med. Internet Res. 2009, 11, e11. [Google Scholar] [CrossRef]
- Ayers, J.W.; Westmaas, J.L.; Leas, E.C.; Benton, A.; Chen, Y.; Dredze, M.; Althouse, B.M. Leveraging Big Data to Improve Health Awareness Campaigns: A Novel Evaluation of the Great American Smokeout. JMIR Public Health Surveill. 2016, 2, e16. [Google Scholar] [CrossRef]
- Cole, J.; Watkins, C.; Kleine, D. Health Advice from Internet Discussion Forums: How Bad Is Dangerous? J. Med. Internet Res. 2016, 18, e4. [Google Scholar] [CrossRef] [Green Version]
- Hoffman-Goetz, L.; Donelle, L.; Thomson, M.D. Clinical guidelines about diabetes and the accuracy of peer information in an unmoderated online health forum for retired persons. Inf. Health Soc. Care 2009, 34, 91–99. [Google Scholar] [CrossRef]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis, 2nd ed.; Springer: Cham, Switzeland, 2016; ISBN 978-3-319-24277-4. [Google Scholar]
- Kingod, N.; Cleal, B.; Wahlberg, A.; Husted, G.R. Online Peer-to-Peer Communities in the Daily Lives of People with Chronic Illness: A Qualitative Systematic Review. Qual. Health Res. 2017, 27, 89–99. [Google Scholar] [CrossRef] [Green Version]
- Van Riel, N.; Auwerx, K.; Debbaut, P.; Van Hees, S.; Schoenmakers, B. The effect of Dr Google on doctor–patient encounters in primary care: A quantitative, observational, cross-sectional study. BJGP Open 2017, 1, 833. [Google Scholar] [CrossRef] [PubMed]
- Ziółkowski, B.A.; Pacholec, A.; Kudlicka, M.; Ehrmann, A.; Muszyński, J. Prevalence of abdominal symptoms in the Polish population. Gastroenterol. Rev. 2012, 1, 20–25. [Google Scholar] [CrossRef] [Green Version]
- Almario, C.V.; Ballal, M.L.; Chey, W.D.; Nordstrom, C.; Khanna, D.; Spiegel, B.M.R. Burden of Gastrointestinal Symptoms in the United States: Results of a Nationally Representative Survey of Over 71,000 Americans. Am. J. Gastroenterol. 2018, 113, 1701–1710. [Google Scholar] [CrossRef] [PubMed]
- Stachowska, E.; Maciejewska, D.; Ryterska, K.; Baszuk, P.; Skonieczna-Żydecka, K.; Czerwińska-Rogowska, M.; Palma, J.; Gudan, A.; Mruk, H.; Wolska, A.; et al. Abdominal Pain and Disturbed Bowel Movements are Frequent among Young People. A Population Based Study in Young Participants of the Woodstock Rock Festival in Poland. J. Gastrointestin. Liver Dis. 2018, 27, 379–383. [Google Scholar]
- Skonieczna-Żydecka, K.; Stachowska, E.; Maciejewska, D.; Ryterska, K.; Palma, J.; Czerwińska-Rogowska, M.; Kaczmarczyk, M.; Gudan, A.; Mruk, H.; Świniarska, B.; et al. The Digestive Health among Participants of the Woodstock Rock Festival in Poland-A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2018, 15, 2256. [Google Scholar] [CrossRef] [Green Version]
- Fendrick, A. Self-selection and use patterns of over-the-counter omeprazole for frequent heartburn. Clin. Gastroenterol. Hepatol. 2004, 2, 17–21. [Google Scholar] [CrossRef]
- Ellis, B.G.; Thompson, M.R. Factors identifying higher risk rectal bleeding in general practice. Br. J. Gen. Pract. 2005, 55, 949–955. [Google Scholar]
- Eslick, G.D.; Kalantar, J.S.; Talley, N.J. Rectal bleeding: Epidemiology, associated risk factors, and health care seeking behaviour: A population-based study. Colorectal Dis. 2009, 11, 921–926. [Google Scholar] [CrossRef]
- Talley, N.J.; Jones, M. Self-reported rectal bleeding in a United States community: Prevalence, risk factors, and health care seeking. Am. J. Gastroenterol. 1998, 93, 2179–2183. [Google Scholar] [CrossRef]
- Marchant, A.; Hawton, K.; Stewart, A.; Montgomery, P.; Singaravelu, V.; Lloyd, K.; Purdy, N.; Daine, K.; John, A. A systematic review of the relationship between internet use, self-harm and suicidal behaviour in young people: The good, the bad and the unknown. PLoS ONE 2017, 12, e0181722. [Google Scholar] [CrossRef]
- Zalsman, G.; Hawton, K.; Wasserman, D.; van Heeringen, K.; Arensman, E.; Sarchiapone, M.; Carli, V.; Höschl, C.; Barzilay, R.; Balazs, J.; et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry 2016, 3, 646–659. [Google Scholar] [CrossRef]
- Predmore, Z.; Ramchand, R.; Ayer, L.; Kotzias, V.; Engel, C.; Ebener, P.; Kemp, J.E.; Karras, E.; Haas, G.L. Expanding Suicide Crisis Services to Text and Chat: Responders’ Perspectives of the Differences Between Communication Modalities. Crisis 2017, 38, 255–260. [Google Scholar] [CrossRef]
- Jones, R.B.; Soler-Lopez, M.; Zahra, D.; Shankleman, J.; Trenchard-Mabere, E. Using online adverts to increase the uptake of cervical screening amongst “real Eastenders”: An opportunistic controlled trial. BMC Res. Notes 2013, 6, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrell, A. Accuracy of online discussion forums on common childhood ailments. JMLA 2018, 106, 455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cima, R.R.; Anderson, K.J.; Larson, D.W.; Dozois, E.J.; Hassan, I.; Sandborn, W.J.; Loftus, E.V.; Pemberton, J.H. Internet use by patients in an inflammatory bowel disease specialty clinic. Inflamm. Bowel Dis. 2007, 13, 1266–1270. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Xu, L.; Li, L.; Zhi, M.; Gu, Y.; Wang, X.; Guo, H.; Li, Y.; Fan, Y.; Yang, B.; et al. Internet and WeChat used by patients with Crohn’s disease in China: A multi-center questionnaire survey. BMC Gastroenterol. 2019, 19, 97. [Google Scholar] [CrossRef] [Green Version]
- Lerrigo, R.; Coffey, J.T.R.; Kravitz, J.L.; Jadhav, P.; Nikfarjam, A.; Shah, N.H.; Jurafsky, D.; Sinha, S.R. The Emotional Toll of Inflammatory Bowel Disease: Using Machine Learning to Analyze Online Community Forum Discourse. Crohn’s Colitis 360 2019, 1, otz011. [Google Scholar] [CrossRef] [Green Version]
- Mukewar, S.; Mani, P.; Wu, X.; Lopez, R.; Shen, B. YouTube® and inflammatory bowel disease. J. Crohn’s Colitis 2013, 7, 392–402. [Google Scholar] [CrossRef] [Green Version]
- Van der Marel, S.; Duijvestein, M.; Hardwick, J.C.; van den Brink, G.R.; Veenendaal, R.; Hommes, D.W.; Fidder, H.H. Quality of web-based information on inflammatory bowel diseases. Inflamm. Bowel Dis. 2009, 15, 1891–1896. [Google Scholar] [CrossRef] [Green Version]
- Abitbol, V.; Lahmek, P.; Buisson, A.; Olympie, A.; Poupardin, C.; Chaussade, S.; Lesgourgues, B.; Nahon, S. Impact of complementary and alternative medicine on the quality of life in inflammatory bowel disease: Results from a French national survey. Eur. J. Gastroenterol. Hepatol. 2014, 26, 288–294. [Google Scholar] [CrossRef]
- Becker, H.M.; Grigat, D.; Ghosh, S.; Kaplan, G.G.; Dieleman, L.; Wine, E.; Fedorak, R.N.; Fernandes, A.; Panaccione, R.; Barkema, H.W. Living with Inflammatory Bowel Disease: A Crohn’s and Colitis Canada Survey. Can. J. Gastroenterol. Hepatol. 2015, 29, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Sudau, F.; Friede, T.; Grabowski, J.; Koschack, J.; Makedonski, P.; Himmel, W. Sources of Information and Behavioral Patterns in Online Health Forums: Qualitative Study. J. Med. Internet Res. 2014, 16, e10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borgmann, H.; Kliesch, S.; Roth, S.; Roth, M.; Degener, S. Feasibility and Efficacy of a Urologic Profession Campaign on Cryptorchidism Using Internet and Social Media. Urol. Int. 2017, 98, 478–482. [Google Scholar] [CrossRef]
- Graham, J.E.; Moore, J.L.; Bell, R.C.; Miller, T. Digital Marketing to Promote Healthy Weight Gain Among Pregnant Women in Alberta: An Implementation Study. J. Med. Internet Res. 2019, 21, e11534. [Google Scholar] [CrossRef]
- Bickart, B.; Schindler, R.M. Internet forums as influential sources of consumer information. J. Interact. Mark. 2001, 15, 31–40. [Google Scholar] [CrossRef]
- Pitta, D.A.; Fowler, D. Internet community forums: An untapped resource for consumer marketers. J. Consum. Mark. 2005, 22, 265–274. [Google Scholar] [CrossRef]
- Sweet, M. Pharmaceutical marketing and the internet. Aust. Prescr. 2009, 32, 2–4. [Google Scholar] [CrossRef] [Green Version]
- Abdellaoui, R.; Foulquié, P.; Texier, N.; Faviez, C.; Burgun, A.; Schück, S. Detection of Cases of Noncompliance to Drug Treatment in Patient Forum Posts: Topic Model Approach. J. Med. Internet Res. 2018, 20, e85. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Top | Ailment | Conditions |
|---|---|---|
| 1. | Abdominal pain | Gastroenteritis |
| 1046 (38.5%) [20.1%] | 96 (3.53%) [13.4%] | |
| 2. | Diarrhoea | Irritable bowel syndrome |
| 454 (16.71%) [8.7%] | 67 (2.47%) [9.4%] | |
| 3. | Bloating | Haemorrhoids |
| 354 (13.03%) [6.8%] | 45 (1.66%) [6.3%] | |
| 4. | Nausea | Helicobacter pylori infection |
| 307 (11.30%) [5.9%] | 44 (1.62%) [6.1%] | |
| 5. | Constipation | Hiatal hernia |
| 288 (10.60%) [5.5%] | 39 (1.44%) [5.4%] | |
| 6. | Flatulence | Inflammatory bowel disease |
| 256 (9.42%) [4.9%] | 30 (1.10%) [4.2%] | |
| 7. | Intestinal rumbling | Peptic ulcer disease |
| 218 (8.02%) [4.2%] | 26 (0.96%) [3.6%] | |
| 8. | Fatigue | Pregnancy |
| 189 (6.96%) [3.6%] | 22 (0.81%) [3.1%] | |
| 9. | Blood in stool | Hypothyroidism |
| 183 (6.74%) [3.5%] | 20 (0.74%) [2.8%] | |
| 10. | Vomit | Duodenitis |
| 153 (5.63%) [2.9%] | 19 (0.70%) [2.7%] | |
| 11. | Heartburn | Food allergy or intolerance |
| 144 (5.30%) [2.8%] | 16 (0.59%) [2.2%] | |
| 12. | Belching | Anxiety disorders |
| 136 (5.01%) [2.6%] | 15 (0.55%) [2.1%] | |
| 13. | Rectal or anal pain | Overweight |
| 97 (3.57%) [1.9%] | 14 (0.52%) [2.0%] | |
| 14. | Weight loss | Biliary system diseases |
| 94 (3.46%) [1.8%] | 12 (0.44%) [1.7%] | |
| 15. | Loss of appetite | Parasites infection |
| Coeliac disease | ||
| 89 (3.28%) [1.7%] | 11 (0.40%) [1.5%] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamiński, M.; Borger, M.; Prymas, P.; Muth, A.; Stachowski, A.; Łoniewski, I.; Marlicz, W. Analysis of Answers to Queries among Anonymous Users with Gastroenterological Problems on an Internet Forum. Int. J. Environ. Res. Public Health 2020, 17, 1042. https://doi.org/10.3390/ijerph17031042
Kamiński M, Borger M, Prymas P, Muth A, Stachowski A, Łoniewski I, Marlicz W. Analysis of Answers to Queries among Anonymous Users with Gastroenterological Problems on an Internet Forum. International Journal of Environmental Research and Public Health. 2020; 17(3):1042. https://doi.org/10.3390/ijerph17031042
Chicago/Turabian StyleKamiński, Mikołaj, Michał Borger, Piotr Prymas, Agnieszka Muth, Adam Stachowski, Igor Łoniewski, and Wojciech Marlicz. 2020. "Analysis of Answers to Queries among Anonymous Users with Gastroenterological Problems on an Internet Forum" International Journal of Environmental Research and Public Health 17, no. 3: 1042. https://doi.org/10.3390/ijerph17031042
APA StyleKamiński, M., Borger, M., Prymas, P., Muth, A., Stachowski, A., Łoniewski, I., & Marlicz, W. (2020). Analysis of Answers to Queries among Anonymous Users with Gastroenterological Problems on an Internet Forum. International Journal of Environmental Research and Public Health, 17(3), 1042. https://doi.org/10.3390/ijerph17031042