Inverse Association between Statin Use and Stomach Cancer Incidence in Individuals with Hypercholesterolemia, from the 2002–2015 NHIS-HEALS Data

 , ,
, , 
Abstract
:1. Introduction
2. Methods
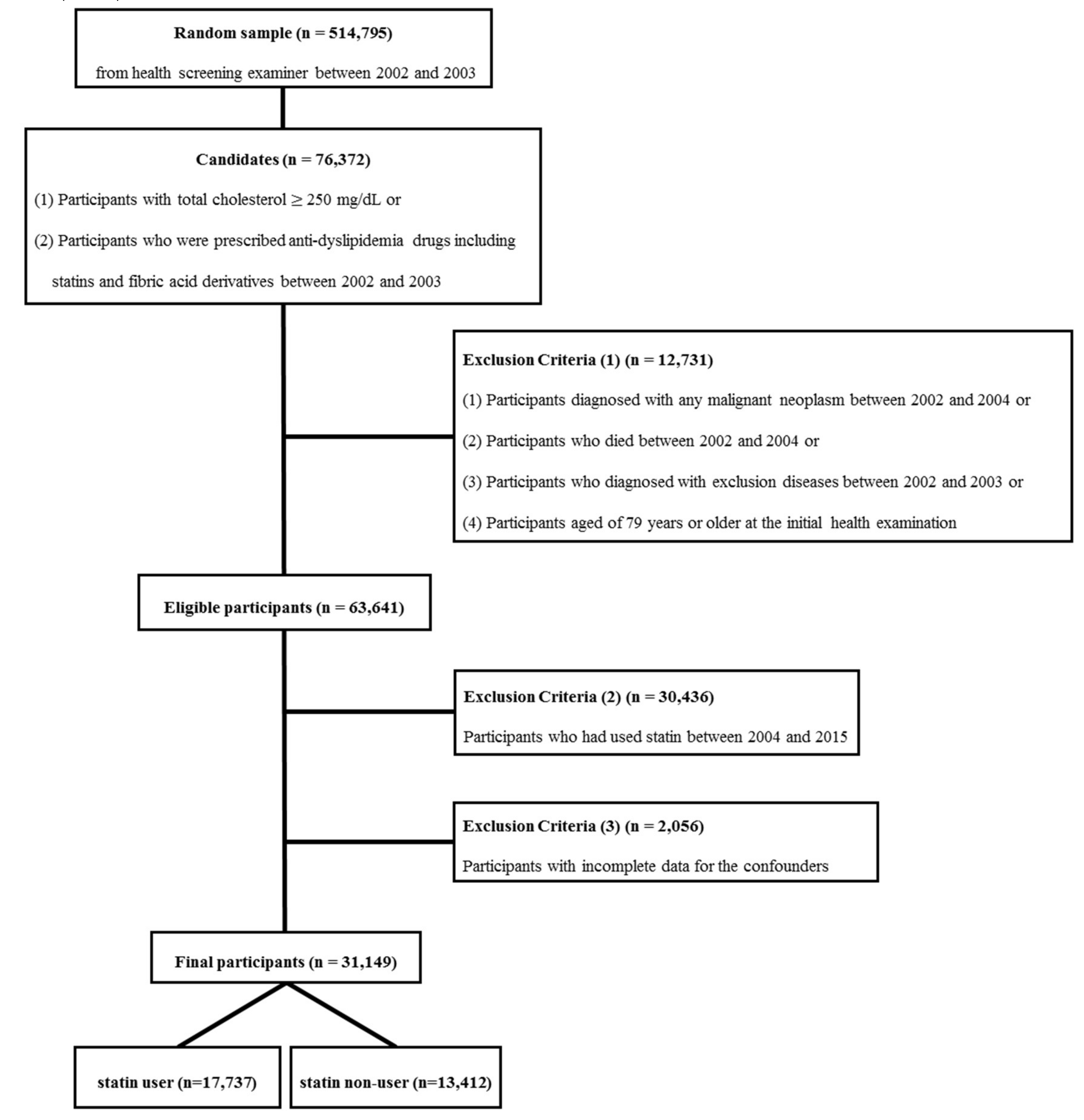
2.1. Study Participants
- (1)
- Participants diagnosed with malignant neoplasm with an International Classification of Diseases (ICD-10) code of C00–C97 or D00–D09 between January 2002 and December 2004;
- (2)
- Participants who died from any cause between January 2002 and December 2004;
- (3)
- Participants diagnosed with ischemic heart diseases (ICD-10 code I20–I25) or cerebrovascular diseases (ICD-10 code I60–I69) between January 2002 and December 2003;
- (4)
- Participants aged 79 years or older at the time of the initial screening between January 2002 and December 2003.
2.2. Variables
2.3. Statin Use Assessment
2.4. Diagnosis of Stomach Cancer
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ministry of Health and Welfare, Korea Central Cancer Registry, National Cancer Center. Available online: http://ncc.re.kr/manage/manage03_033_list.jsp (accessed on 13 July 2018).
- International Agency for Research on Cancer. Globocan 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012. Available online: http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx (accessed on 13 July 2018).
- Statistics Korea. Available online: http://kostat.go.kr/portal/eng/index.action (accessed on 13 July 2019).
- Newman, T.B.; Hulley, S.B. Carcinogenicity of lipid-lowering drugs. JAMA 1996, 275, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Dimitroulakos, J.; Marhin, W.H.; Tokunaga, J.; Irish, J.; Gullane, P.; Penn, L.Z.; Kamel-Reid, S. Microarray and biochemical analysis of lovastatin-induced apoptosis of squamous cell carcinomas. Neoplasia 2002, 4, 337–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keyomarsi, K.; Sandoval, L.; Band, V.; Pardee, A.B. Synchronization of tumor and normal cells from G1 to multiple cell cycles by lovastatin. Cancer Res. 1991, 51, 3602–3609. [Google Scholar] [PubMed]
- Boudreau, D.M.; Yu, O.; Jhonson, J. Statin Use and Cancer Risk: Acomprehensive Review. HHS 2010, 9, 603–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cocco, P.; Fadda, D.; Schwartz, A.G. Subject expressing the glucose-6-phosphate dehydrogenase deficient phenotype experience a lower cardivacular mortality. QJM 2008, 101, 161–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisano, M.; Cocco, P.; Cherchi, R.; Onnis, R.; Cherchi, P. Glucose-6-Phosphate dehydrogenase deficiency and lung cancer: A hospital based case-control study. Tumori J. 1991, 77, 12–15. [Google Scholar] [CrossRef]
- Lee, J.; Lee, S.H.; Hur, K.Y.; Woo, S.Y.; Kim, S.W.; Kang, W.K. Statins and the risk of gastric cancer in diabetes patients. BMC Cancer 2012, 12, 596. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.D.; Zeng, K.; Xue, F.Q.; Chen, J.H.; Chen, Y.Q. Statins are associated with reduced risk of gastric cancer: A meta-analysis. Eur. J. Clin. Pharmacol. 2013, 69, 1855–1860. [Google Scholar] [CrossRef]
- Chiu, H.F.; Ho, S.C.; Chang, C.C.; Wu, T.N.; Yang, C.Y. Statins are associated with a reduced risk of gastric cancer: A population-based case-control study. Am. J. Gastroenterol. 2011, 106, 2098–2103. [Google Scholar] [CrossRef]
- Seong, S.C.; Kim, Y.Y.; Park, S.K.; Khang, Y.H.; Kim, H.C.; Park, J.H.; Kang, H.J.; Do, C.H.; Song, J.S.; Lee, E.J.; et al. Cohort profile: The National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) in Korea. BMJ Open 2017, 7, e016640. [Google Scholar] [CrossRef] [Green Version]
- Holstein, S.A.; Hohl, R.J. Isoprenoids: Remarkable diversity of form and function. Lipids 2004, 39, 293–309. [Google Scholar] [CrossRef] [PubMed]
- Casey, P.J. Protein lipidation in cell signaling. Science 1995, 268, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Fritz, G. HMG-CoA reductase inhibitors (statins) as anticancer drugs (review). Int. J. Oncol. 2005, 27, 1401–1409. [Google Scholar] [CrossRef] [PubMed]
- Jakobisiak, M.; Golab, J. Potential antitumor effects of statins (Review). Int. J. Oncol. 2003, 23, 1055–1069. [Google Scholar] [CrossRef]
- Wong, W.W.; Dimitroulakos, J.; Minden, M.D.; Penn, L.Z. HMG-CoA reductase inhibitors and the malignant cell: The statin family of drugs as triggers of tumor-specific apoptosis. Leukemia 2002, 16, 508–519. [Google Scholar] [CrossRef] [Green Version]
- Park, H.J.; Kong, D.; Iruela-Arispe, L.; Begley, U.; Tang, D.; Galper, J.B. 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors interfere with angiogenesis by inhibiting the geranylgeranylation of RhoA. Circ. Res. 2002, 91, 143–150. [Google Scholar] [CrossRef]
- Alonso, D.F.; Farina, H.G.; Skilton, G.; Gabri, M.R.; De Lorenzo, M.S.; Gomez, D.E. Reduction of mouse mammary tumor formation and metastasis by lovastatin, an inhibitor of the mevalonate pathway of cholesterol synthesis. Breast Cancer Res. Treat. 1998, 50, 83–93. [Google Scholar] [CrossRef]
- Endres, M. Statins: Potential new indications in inflammatory conditions. Atheroscler. Suppl. 2006, 7, 31–35. [Google Scholar] [CrossRef]
- Graaf, M.R.; Beiderbeck, A.B.; Egberts, A.C.; Richel, D.J.; Guchelaar, H.J. The risk of cancer in users of statins. J. Clin. Oncol. 2004, 22, 2388–2394. [Google Scholar] [CrossRef]
- Haukka, J.; Sankila, R.; Klaukka, T.; Lonnqvist, J.; Niskanen, L.; Tanskanen, A.; Wahlbeck, K.; Tiihonen, J. Incidence of cancer and statin usage--record linkage study. Int. J. Cancer 2010, 126, 279–284. [Google Scholar] [CrossRef]
- Kuoppala, J.; Lamminpaa, A.; Pukkala, E. Statins and cancer: A systematic review and meta-analysis. Eur. J. Cancer 2008, 44, 2122–2132. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Kang, H.T. Association between Socioeconomic Status and Cancer Screening in Koreans over 40 Years in Age Based on the 2010–2012 Korean National Health and Nutrition Examination Survey. Korean J. Fam. Med. 2016, 37, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Larsen, S.B.; Dehlendorff, C.; Skriver, C.; Dalton, S.O.; Jespersen, C.G.; Borre, M.; Brasso, K.; Nørgaard, M.; Johansen, C.; Sørensen, H.T.; et al. Postdiagnosis Statin Use and Mortality in Danish Patients With Prostate Cancer. J. Clin. Oncol. 2017, 35, 3290–3297. [Google Scholar] [CrossRef]
- Wang, A.; Aragaki, A.K.; Tang, J.Y.; Kurian, A.W.; Manson, J.E.; Chlebowski, R.T.; Simon, M.; Desai, P.; Wassertheil-Smoller, S.; Liu, S.; et al. Statin use and all-cancer survival: Prospective results from the Women’s Health Initiative. Br. J. Cancer 2016, 115, 129–135. [Google Scholar] [CrossRef]
- Ahern, T.P.; Pedersen, L.; Tarp, M.; Cronin-Fenton, D.P.; Garne, J.P.; Silliman, R.A.; Sørensen, H.T.; Lash, T.L. Statin prescriptions and breast cancer recurrence risk: A Danish nationwide prospective cohort study. J. Natl. Cancer Inst. 2011, 103, 1461–1468. [Google Scholar] [CrossRef] [Green Version]
- Valenstein, M.; Copeland, L.A.; Blow, F.C.; McCarthy, J.F.; Zeber, J.E.; Gillon, L.; Bingham, C.R.; Stavenger, T. Pharmacy data identify poorly adherent patients with schizophrenia at increased risk for admission. Med. Care 2002, 40, 630–639. [Google Scholar] [CrossRef] [Green Version]
- Bertuccio, P.; Rosato, V.; Andreano, A.; Ferraroni, M.; Decarli, A.; Edefonti, V.; La Vecchia, C. Dietary patterns and gastric cancer risk: A systematic review and meta-analysis. Ann. Oncol. 2013, 24, 1450–1458. [Google Scholar] [CrossRef]
- Kim, H.J.; Chang, W.K.; Kim, M.K.; Lee, S.S.; Choi, B.Y. Dietary factors and gastric cancer in Korea: A case-control study. Int. J. Cancer 2002, 97, 531–535. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Men | Women | |
|---|---|---|
| Number | 16,588 | 14,561 |
| Age, years | 52.6 ± 0.1 | 58.7 ± 0.1 |
| Body Mass Index, kg/m2 | 24.9 ± 0.0 | 25.0 ± 0.0 |
| Systolic Blood Pressure, mmHg | 131.5 ± 0.1 | 131.0 ± 0.2 |
| Glucose, mg/dL | 108.1 ± 0.4 | 105.7 ± 0.4 |
| Total cholesterol, mg/dL | 247.1 ± 0.4 | 247.0 ± 0.4 |
| Diabetes Mellitus, % | 7.8 ± 0.2 | 9.6 ± 0.2 |
| Hypertension, % | 11.8 ± 0.3 | 20.3 ± 0.3 |
| Ever smokers, % | 58.6 ± 0.4 | 4.2 ± 0.2 |
| Drinking status, % | ||
| Rare | 34.3 ± 0.4 | 85.8 ± 0.3 |
| Sometimes | 45.9 ± 0.4 | 12.6 ± 0.3 |
| Often | 19.8 ± 0.3 | 1.7 ± 0.1 |
| Physical activity, % | ||
| Rare | 47.2 ± 0.4 | 65.1 ± 0.4 |
| Sometimes | 42.6 ± 0.4 | 23.6 ± 0.4 |
| Regular | 10.2 ± 0.2 | 11.3 ± 0.3 |
| Economic status, % | ||
| Low | 18.6 ± 0.3 | 27.5 ± 0.4 |
| Middle | 31.4 ± 0.4 | 32.4 ± 0.4 |
| High | 50.1 ± 0.4 | 40.1 ± 0.4 |
| Male | Non-Users | Low Users | High Users | P-value |
| Number | 8488 | 4050 | 4050 | NA |
| Age, years | 51.2 ± 0.1 | 53.4 ± 0.1 | 54.5 ± 0.1 | <0.001 |
| Body Mass Index, kg/m2 | 24.5 ± 0.0 | 25.0 ± 0.0 | 25.5 ± 0.0 | <0.001 |
| Systolic Blood Pressure, mmHg | 129.6 ± 0.2 | 132.0 ± 0.3 | 134.9 ± 0.3 | <0.001 |
| Glucose, mg/dL | 104.4 ± 0.6 | 107.8 ± 0.7 | 116.1 ± 0.8 | <0.001 |
| Total cholesterol, mg/dL | 263.2 ± 0.5 | 226.6 ± 0.7 | 234.0 ± 0.8 | <0.001 |
| Diabetes Mellitus, % | 2.9 ± 0.2 | 9.3 ± 0.5 | 16.3 ± 0.6 | <0.001 |
| Hypertension, % | 5.0 ± 0.2 | 14.5 ± 0.6 | 23.6 ± 0.7 | <0.001 |
| Ever smokers, % | 61.8 ± 0.5 | 55.7 ± 0.8 | 54.8 ± 0.8 | <0.001 |
| Drinking status, % | <0.001 | |||
| Rare | 32.9 ± 0.5 | 34.9 ± 0.7 | 36.6 ± 0.8 | |
| Sometimes | 46.7 ± 0.5 | 44.7 ± 0.8 | 45.3 ± 0.8 | |
| Often | 20.4 ± 0.4 | 20.3 ± 0.6 | 18.1 ± 0.6 | |
| Physical activity, % | <0.001 | |||
| Rare | 48.4 ± 0.5 | 48.2 ± 0.8 | 43.3 ± 0.8 | |
| Sometimes | 43.0 ± 0.5 | 41.2 ± 0.8 | 43.2 ± 0.8 | |
| Regular | 8.4 ± 0.3 | 10.6 ± 0.5 | 13.5 ± 0.5 | |
| Economic status, % | <0.001 | |||
| Low | 20.6 ± 0.4 | 17.1 ± 0.6 | 15.9 ± 0.6 | |
| Middle | 32.2 ± 0.5 | 31.8 ± 0.7 | 28.8 ± 0.7 | |
| High | 47.2 ± 0.5 | 51.1 ± 0.8 | 55.3 ± 0.8 | |
| Female | Non-User | Low User | High User | P-value |
| Number | 4924 | 4818 | 4819 | NA |
| Age, years | 58.2 ± 0.1 | 58.7 ± 0.1 | 59.3 ± 0.1 | <0.001 |
| Body Mass Index, kg/m2 | 24.3 ± 0.0 | 25.2 ± 0.0 | 25.4 ± 0.0 | <0.001 |
| Systolic Blood Pressure, mmHg | 128.6 ± 0.3 | 131.1 ± 0.3 | 133.3 ± 0.3 | <0.001 |
| Glucose, mg/dL | 103.7 ± 0.9 | 104.6 ± 0.6 | 108.8 ± 0.7 | <0.001 |
| Total cholesterol, mg/dL | 266.9 ± 0.6 | 234.4 ± 0.7 | 239.3 ± 0.7 | <0.001 |
| Diabetes Mellitus, % | 3.2 ± 0.3 | 10.0 ± 0.4 | 15.7 ± 0.5 | <0.001 |
| Hypertension, % | 9.9 ± 0.4 | 20.6 ± 0.6 | 30.5 ± 0.7 | <0.001 |
| Ever smokers, % | 4.7 ± 0.3 | 4.0 ± 0.3 | 3.9 ± 0.3 | 0.092 |
| Drinking status, % | <0.001 | |||
| Rare | 83.5 ± 0.5 | 85.5 ± 0.5 | 88.4 ± 0.5 | |
| Sometimes | 14.4 ± 0.5 | 12.8 ± 0.5 | 10.4 ± 0.4 | |
| Often | 2.0 ± 0.2 | 1.7 ± 0.2 | 1.2 ± 0.2 | |
| Physical activity, % | <0.001 | |||
| Rare | 70.3 ± 0.7 | 65.7 ± 0.7 | 59.3 ± 0.7 | |
| Sometimes | 20.4 ± 0.6 | 23.0 ± 0.6 | 27.6 ± 0.6 | |
| Regular | 9.3 ± 0.4 | 11.4 ± 0.5 | 13.1 ± 0.5 | |
| Economic status, % | <0.001 | |||
| Low | 31.6 ± 0.7 | 27.8 ± 0.6 | 23.1 ± 0.6 | |
| Middle | 31.8 ± 0.7 | 33.6 ± 0.7 | 31.9 ± 0.7 | |
| High | 36.6 ± 0.7 | 38.6 ± 0.7 | 44.9 ± 0.7 |
| Hazard Ratios (95% Confidence Intervals) | Male | Female |
|---|---|---|
| Model 1 | ||
| Low users vs Non-users | 0.922 (0.741–1.149) | 0.656 (0.486–0.885) |
| High users vs Non-users | 0.521 (0.402–0.676) | 0.395 (0.280–0.559) |
| Model 2 | ||
| Low users vs Non-users | 0.930 (0.746–1.158) | 0.657 (0.486–0.887) |
| High users vs Non-users | 0.532 (0.410–0.690) | 0.397 (0.280–0.562) |
| Model 3 | ||
| Low users vs Non-users | 0.953 (0.755–1.203) | 0.629 (0.457–0.865) |
| High users vs Non-users | 0.526 (0.399–0.693) | 0.370 (0.256–0.535) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
You, H.-S.; You, N.; Lee, J.-W.; Lim, H.-J.; Kim, J.; Kang, H.-T. Inverse Association between Statin Use and Stomach Cancer Incidence in Individuals with Hypercholesterolemia, from the 2002–2015 NHIS-HEALS Data. Int. J. Environ. Res. Public Health 2020, 17, 1054. https://doi.org/10.3390/ijerph17031054
You H-S, You N, Lee J-W, Lim H-J, Kim J, Kang H-T. Inverse Association between Statin Use and Stomach Cancer Incidence in Individuals with Hypercholesterolemia, from the 2002–2015 NHIS-HEALS Data. International Journal of Environmental Research and Public Health. 2020; 17(3):1054. https://doi.org/10.3390/ijerph17031054
Chicago/Turabian StyleYou, Hyo-Sun, Nayoung You, Jae-Woo Lee, Hyoung-Ji Lim, Joungyoun Kim, and Hee-Taik Kang. 2020. "Inverse Association between Statin Use and Stomach Cancer Incidence in Individuals with Hypercholesterolemia, from the 2002–2015 NHIS-HEALS Data" International Journal of Environmental Research and Public Health 17, no. 3: 1054. https://doi.org/10.3390/ijerph17031054
APA StyleYou, H. -S., You, N., Lee, J. -W., Lim, H. -J., Kim, J., & Kang, H. -T. (2020). Inverse Association between Statin Use and Stomach Cancer Incidence in Individuals with Hypercholesterolemia, from the 2002–2015 NHIS-HEALS Data. International Journal of Environmental Research and Public Health, 17(3), 1054. https://doi.org/10.3390/ijerph17031054