Impact of Dining Hall Structural Changes on Food Choices: A Pre-Post Observational Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. The Structural Changes
2.2. Study Methods
2.3. Data Analysis
3. Results
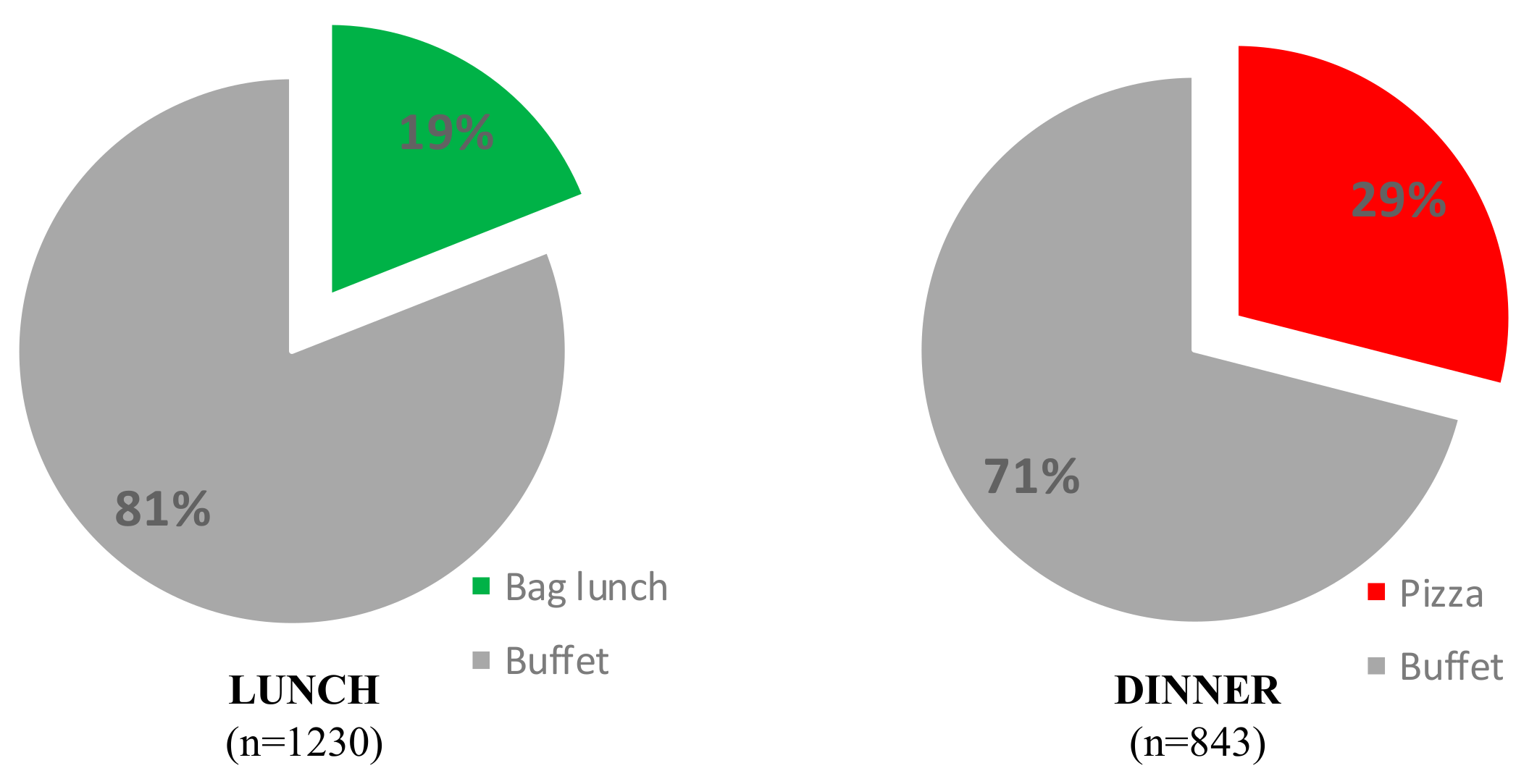
3.1. Observation
3.2. Plate Photography
4. Discussion
Limitations and Future Research Directions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Healthfulness Classification of Foods Made Available for Selection

{kind=link}
| Food Counter | Type of Dish | Rating | Number (before) | Number (after) |
|---|---|---|---|---|
| Main | Meat (lean/trimmed) | Green | 1 | 0 |
| Main | Meat (non-trimmed) or mixed dishes (casserole/stir fry) below fat/salt limit | Orange | 11 | 8 |
| Main | Deep-fried food or Mixed dishes (casseroles/stir fry) above fat/salt limit | Red | 5 | 7 |
| Vegetable | Plain potato | Green | 1 | 1 |
| Vegetable | Mashed potato | Orange | 0 | 2 |
| Vegetable | Roast potato (added salt/oil/fat) | Orange | 0 | 0 |
| Vegetable | Potato fries or potato bake (added cream or cheese) | Red | 1 | 2 |
| Vegetable | Plain vegetables | Green | 8 | 8 |
| Vegetable | Roast vegetables (added salt/oil/fat) | Orange | 0 | 1 |
| Vegetable | Plain rice | Green | 2 | 1 |
| Vegetable | Fried rice/noodles | Orange | 0 | 2 |
| Salad | Plain salad/vinegar dressed salad or separate salad vegetables | Green | 18 | 19 |
| Salad | Plain fruit pieces | Green | 6 | 10 |
| Salad | Creamy dressed salad (vegetable) | Orange | 5 | 5 |
| Salad | Creamy dressed salad (added processed meat or cheese) | Red | 1 | 0 |
| Sandwich | Bread | Green | 6 | 4 |
| Sandwich | Sliced lean meat | Green | 2 | 3 |
| Sandwich | Hard-boiled egg | Green | 2 | 1 |
| Sandwich | Wrap/sandwich portions 1 (vegetable only) | Green | 1 | 1 |
| Sandwich | Egg/tuna mayonnaise mix | Orange | 2 | 2 |
| Sandwich | Cheese | Orange | 2 | 2 |
| Sandwich | Wrap/sandwich portions 1 (cheese/egg mayonnaise mixes) | Orange | 1 | 0 |
| Sandwich | Processed meat | Red | 5 | 3 |
| Sandwich | Wrap/sandwich portions 1 (processed meat) | Red | 1 | 1 |
| Food Counter | Type of Dish | Rating | Number (before) | Number (after) |
|---|---|---|---|---|
| Main | Meat (lean/trimmed) | Green | 1 | 0 |
| Main | Meat (non-trimmed) or mixed dishes (casserole/stir fry) below fat/salt limit | Orange | 7 | 2 |
| Main | Deep-fried food or Mixed dishes (casseroles/stir fry) above fat/salt limit | Red | 4 | 7 |
| Vegetable | Plain potato | Green | 2 | 0 |
| Vegetable | Mashed potato | Orange | 0 | 0 |
| Vegetable | Roast potato (added salt/oil/fat) | Orange | 1 | 0 |
| Vegetable | Potato fries or potato bake (added cream or cheese) | Red | 0 | 4 |
| Vegetable | Plain vegetables | Green | 8 | 6 |
| Vegetable | Roast vegetables (added salt/oil/fat) | Orange | 1 | 0 |
| Vegetable | Plain rice | Green | 2 | 1 |
| Vegetable | Fried rice/noodles | Orange | 0 | 0 |
| Salad | Plain salad/vinegar dressed salad or separate salad vegetables | Green | 15 | 10 |
| Salad | Plain fruit pieces | Green | 9 | 7 |
| Salad | Creamy dressed salad (vegetable) | Orange | 4 | 3 |
| Salad | Creamy dressed salad (added processed meat or cheese) | Red | 1 | 0 |
| Sandwich | Bread | Green | 3 | 31 |
| Sandwich | Sliced lean meat | Green | 2 | 0 |
| Sandwich | Hard-boiled egg | Green | 0 | 0 |
| Sandwich | Wrap/sandwich portions (vegetable only) | Green | 0 | 0 |
| Sandwich | Egg/tuna mayonnaise mix | Orange | 2 | 0 |
| Sandwich | Cheese | Orange | 2 | 11 |
| Sandwich | Wrap/sandwich portions (cheese/egg mayonnaise mixes) | Orange | 0 | 0 |
| Sandwich | Processed meat | Red | 3 | 0 |
| Sandwich | Wrap/sandwich portions (processed meat) | Red | 2 | 0 |
References
- Truong, V.D. Social marketing: A systematic review of research 1998–2012. Soc. Mar. Q. 2014, 20, 15–34. [Google Scholar] [CrossRef]
- Dibb, S. Up, up and away: Social marketing breaks free. J. Mark. Manag. 2014, 30, 1159–1185. [Google Scholar] [CrossRef]
- Kennedy, A.M.; Parsons, A. Macro-social marketing and social engineering: A systems approach. J. Soc. Market. 2012, 2, 37–51. [Google Scholar] [CrossRef]
- Hoek, J.; Jones, S.C. Regulation, public health and social marketing: A behaviour change trinity. J. Soc. Market. 2011, 1, 32–44. [Google Scholar] [CrossRef]
- Gordon, R. Unlocking the potential of upstream social marketing. Eur. J. Mark. 2013, 47, 1525–1547. [Google Scholar] [CrossRef]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronto, R.; Wu, J.H.; Singh, G.M. The global nutrition transition: Trends, disease burdens and policy interventions. Public Health Nutr. 2018. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; Amann, M.; Anderson, H.R.; Andrews, K.G.; Aryee, M.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [Green Version]
- Singh, G.M.; Micha, R.; Khatibzadeh, S.; Lim, S.; Ezzati, M.; Mozaffarian, D. Response to letter regarding article, "Estimated Global, Regional, and National Disease Burdens Related to Sugar-Sweetened Beverage Consumption in 2010". Circulation 2016, 133, E596. [Google Scholar] [CrossRef] [Green Version]
- Crosland, P.; Ananthapavan, J.; Davison, J.; Lambert, M.; Carter, R. The economic cost of preventable disease in Australia: A systematic review of estimates and methods. Aust. N. Z. J. Public Health 2019. [Google Scholar] [CrossRef]
- Rodriguez, N.R.; DiMarco, N.M.; Langley, S. Nutrition and athletic performance. Med. Sci. Sports Exerc. 2009, 41, 709–731. [Google Scholar] [CrossRef]
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- Johnson-Askew, W.L.; Fisher, R.A.; Yaroch, A.L. Decision making in eating behavior: State of the science and recommendations for future research. nn. Behav. Med. 2009, 38, S88–S92. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.G. Foodservice perspective in institutions. In Meals in Science and Practice: Interdisciplinary Research and Business Applications; Meiselman, H.L., Ed.; Woodhead Publishing Ltd.: Cambridge, UK, 2009; pp. 50–65. [Google Scholar]
- Conklin, M.T.; Lambert, C.U.; Cranage, D.A. Nutrition information at point of selection could benefit college students. Top. Clin. Nutr. 2005, 20, 90–96. [Google Scholar] [CrossRef]
- Levitsky, D.A.; Halbmaier, C.A.; Mrdjenovic, G. The freshman weight gain: A model for the study of the epidemic of obesity. Int. J. Obes. 2004, 28, 1435–1442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pliner, P.; Saunders, T. Vulnerability to freshman weight gain as a function of dietary restraint and residence. Physiol. Behav. 2008, 93, 76–82. [Google Scholar] [CrossRef]
- Gortmaker, S.L.; Swinburn, B.A.; Levy, D.; Carter, R.; Mabry, P.L.; Finegood, D.T.; Huang, T.; Marsh, T.; Moodie, M.L. Changing the future of obesity: Science, policy, and action. Lancet 2011, 378, 838–847. [Google Scholar] [CrossRef] [Green Version]
- Kumanyika, S.K. Minisymposium on obesity: Overview and some strategic considerations. Annu. Rev. Public Health 2001, 22, 293–308. [Google Scholar] [CrossRef] [Green Version]
- Carins, J.E.; Pang, B.; Knox, K.; Wilmott, T.; Storr, R.; Robertson, D.; Rundle-Thiele, S.; Pettigrew, S. International food service initiatives: An Evidence Check rapid review; Commissioned by the Australian Government Department of Health and brokered by the Sax Institute for The Australian Prevention Partnership Centre; Australian Government Department of Health: Sydney, Australia, 2017.
- Mayne, S.L.; Auchincloss, A.H.; Michael, Y.L. Impact of policy and built environment changes on obesity-related outcomes: A systematic review of naturally occurring experiments. Obes Rev. 2015, 16, 362–375. [Google Scholar] [CrossRef]
- Bowen, D.J.; Barrington, W.E.; Beresford, S.A.A. Identifying the Effects of Environmental and Policy Change Interventions on Healthy Eating. Annu Rev. Publ Health 2015, 36, 289–306. [Google Scholar] [CrossRef] [Green Version]
- Lieberman, L.D.; Golden, S.D.; Earp, J.A.L. structural approaches to health promotion: What do we need to know about policy and environmental change? Health Educ. Behav. 2013, 40, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, L.D.; Earp, J.A.L. reflections on structural change: Where do we go from here? Health Educ. Behav. 2015, 42, 141s–142s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lusch, R.F. Marketing’s evolving identity: Defining our future. J. Public Policy Mark. 2007, 26, 261–268. [Google Scholar] [CrossRef]
- Brennan, L.; Previte, J.; Fry, M.L. Social marketing’s consumer myopia: Applying a behavioural ecological model to address wicked problems. J. Soc. Market. 2016, 6, 219–239. [Google Scholar] [CrossRef]
- David, P.; Rundle-Thiele, S.; Pang, B.; Knox, K.; Parkinson, J.; Hussenoeder, F. Engaging the dog owner community in the design of an effective koala aversion program. Soc. Mar. Q. 2019, 25, 55–68. [Google Scholar] [CrossRef]
- Carins, J.E.; Rundle-Thiele, S.R.; Parkinson, J.E. A picture says a thousand words: A food selection observational method. Health Promot. J. Austr. 2016, 27, 94–101. [Google Scholar] [CrossRef] [Green Version]
- National Health and Medical Research Council. Australian Dietary Guidelines; NHMRC: Canberra, Australia, 2013. [Google Scholar]
- Phan, U.T.X.; Chambers, E. Motivations for meal and snack times: Three approaches reveal similar constructs. Food Qual. Pref. 2018, 68, 267–275. [Google Scholar] [CrossRef]
- Rappoport, L.; Downey, R.G.; Huff-Corzine, L. Conceptual differences between meals. Food Qual. Pref. 2001, 12, 9–17. [Google Scholar] [CrossRef]
- Denscombe, M. The Good Research Guide: For. Small-Scale Social Research Projects; McGraw-Hill International: Berkshire, UK, 2010. [Google Scholar]
- Gittelsohn, J.; Shankar, A.V.; West, K.P.; Ram, R.M.; Gnywali, T. Estimating reactivity in direct observation studies of health behaviors. Hum. Organ. 1997, 56, 182–189. [Google Scholar] [CrossRef]
- Sisnowski, J.; Street, J.M.; Merlin, T. Improving food environments and tackling obesity: A realist systematic review of the policy success of regulatory interventions targeting population nutrition. PLoS ONE 2017, 12. [Google Scholar] [CrossRef] [Green Version]
- Brambila-Macias, J.; Shankar, B.; Capacci, S.; Mazzocchi, M.; Perez-Cueto, F.J.A.; Verbeke, W.; Trail, W.B. Policy interventions to promote healthy eating: A review of what works, what does not, and what is promising. Food Nutr. Bull. 2011, 32, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Wymer, W. Developing more effective social marketing strategies. J. Soc. Market. 2011, 1, 17–31. [Google Scholar] [CrossRef]
- Almestahiri, R.; Rundle-Thiele, S.; Parkinson, J.; Arli, D. The use of the major components of social marketing: A systematic review of tobacco cessation programs. Soc. Mar. Q. 2017, 23, 232–248. [Google Scholar] [CrossRef]
- Hill, J.O.; Peters, J.C.; Catenacci, V.A.; Wyatt, H.R. International strategies to address obesity. Obes Rev. 2008, 9, 41–47. [Google Scholar] [CrossRef]
- Lake, A.; Townshend, T. Obesogenic environments: Exploring the built and food environments. J. R. Soc. Promot. Health 2006, 126, 262–267. [Google Scholar] [CrossRef]
- Larson, N.; Story, M. A review of environmental influences on food choices. nn. Behav. Med. 2009, 38, 56–73. [Google Scholar] [CrossRef]
- Snyder, L.B.; Hamilton, M.A.; Mitchell, E.W.; Kiwanuka-Tondo, J.; Fleming-Milici, F.; Proctor, D. A meta-analysis of the effect of mediated health communication campaigns on behavior change in the United States. J. Health Commun. 2004, 9, 71–96. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.; Rothstein, H.R. Converting among effect sizes. In Introduction to meta-analysis; Wiley: West Sussex, UK, 2009; pp. 45–49. [Google Scholar]
- Michie, S.; Abraham, C.; Whittington, C.; McAteer, J.; Gupta, S. Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychol. 2009, 28, 690–701. [Google Scholar] [CrossRef] [Green Version]
- Dawson, J. Retailer activity in shaping food choice. Food Qual. Pref. 2013, 28, 339–347. [Google Scholar] [CrossRef]
- Gase, L.; Dunning, L.; Kuo, T.; Simon, P.; Fielding, J.E. Restaurant owners‘ perspectives on a voluntary program to recognize restaurants for offering reduced -size portions, Los Angeles County, 2012. Prev. Chronic Dis. 2014, 11. [Google Scholar] [CrossRef] [Green Version]
- Glanz, K.; Basil, M.; Maibach, E.; Goldberg, J.; Snyder, D. Why Americans eat what they do: Taste, nutrition, cost, convenience, and weight control concerns as influences on food consumption. J. Am. Diet. Assoc. 1998, 98, 1118–1126. [Google Scholar] [CrossRef]
- Laroche, H.H.; Ford, C.; Hansen, K.; Cai, X.Y.; Just, D.R.; Hanks, A.S.; Wansink, B. Concession stand makeovers: A pilot study of offering healthy foods at high school concession stands. J. Public Health 2015, 37, 116–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carins, J.E.; Rundle-Thiele, S.R.; Parkinson, J.E. Delivering healthy food choice: A dual-process model enquiry. Soc. Mar. Q. 2017, 23, 266–283. [Google Scholar] [CrossRef] [Green Version]
- Hanks, A.S.; Just, D.R.; Smith, L.E.; Wansink, B. Healthy convenience: Nudging students toward healthier choices in the lunchroom. J. Public Health 2012, 34, 370–376. [Google Scholar] [CrossRef] [Green Version]
- Olstad, D.L.; Goonewardene, L.A.; McCargar, L.J.; Raine, K.D. If we offer it, will children buy it? Sales of healthy foods mirrored their availability in a community sport, commercial setting in Alberta, Canada. Child. Obes 2015, 11, 156–164. [Google Scholar] [CrossRef]
- Fildes, A.; Charlton, J.; Rudisill, C.; Littlejohns, P.; Prevost, A.T.; Gulliford, M.C. Probability of an obese person attaining normal body weight: Cohort study using electronic health records. Am. J. Public Health 2015, 105, e54–e59. [Google Scholar] [CrossRef] [Green Version]
- Baur, L.A. Tackling the epidemic of childhood obesity. Can. Med. Assoc. J. 2009, 180, 701–702. [Google Scholar] [CrossRef] [Green Version]
- Western Australian Government. Healthy Options WA: Food and Nutrition Policy for WA Health Services and Facilities; Health, D.o., Ed.; WA Government: Perth, Australia, 2009.
- Queensland Government. A Better Choice Healthy Food and Drink Supply Strategy for Queensland Health Facilities; Queensland Government: Brisbane, Australia, 2007.
- NSW Health. Live Life Well @ Health: Healthier Food & Drink Choices—Staff & Visitors in NSW Health Facilities; NSW Government: Sydney, Australia, 2009.
- Kelly, B.; Flood, V.M.; Yeatman, H. Measuring local food environments: An overview of available methods and measures. Health Place 2011, 17, 1284–1293. [Google Scholar] [CrossRef]
- Saelens, B.E.; Glanz, K.; Sallis, J.F.; Frank, L.D. Nutrition Environment Measures Study in restaurants (NEMS-R): Development and evaluation. Am. J. Prev. Med. 2007, 32, 273–281. [Google Scholar] [CrossRef]
- Baker, A.H.; Wardle, J. Sex differences in fruit and vegetable intake in older adults. Appetite 2003, 40, 269–275. [Google Scholar] [CrossRef]
- Leblanc, V.; Bégin, C.; Corneau, L.; Dodin, S.; Lemieux, S. Gender differences in dietary intakes: What is the contribution of motivational variables? J. Human Nutr. Diet. 2015, 28, 37–46. [Google Scholar] [CrossRef]
- Kafetsios, K.; Sideridis, G.D. Attachment, social support and well-being in young and older adults. J. Health Psychol. 2006, 11, 863–875. [Google Scholar] [CrossRef]
- Siewert, K.; Antoniw, K.; Kubiak, T.; Weber, H. The more the better? The relationship between mismatches in social support and subjective well-being in daily life. J. Health Psychol. 2011, 16, 621–631. [Google Scholar] [CrossRef] [PubMed]

| Lunch | Food Counter | Before (n = 1294) | After (n = 1230) |
| Usage (%) | Usage (%) | ||
| Paper Bag Lunch | - | 230 (19%) | |
| Main dish | 1201 (93%) ** | 1049 (85%) ** | |
| Hot Vegetable | 972 (75%) * | 974 (79%) * | |
| Salad bar | 857 (66%) ns | 811 (66%) ns | |
| Sandwich bar | 988 (76%)** | 458 (37%)** | |
| Dinner | Food Counter | Before (n = 787) | After (n = 843) |
| Usage (%) | Usage (%) | ||
| MYO Pizza | - | 244 (29%) | |
| Main dish | 774 (98%) ** | 648 (77%) ** | |
| Hot Vegetable | 709 (90%) ** | 556 (66%) ** | |
| Salad bar | 463 (59%) ** | 403 (48%) ** | |
| Sandwich bar 1 | 469 (60%) | - |
| Lunch | Selections1 | Before (n = 159) | After (n = 224) | ||||
| Mean | (95% CI) | Mode | Mean | (95% CI) | Mode | ||
| Red | 0.65 ** | (0.53, 0.77) | 0 | 0.86 ** | (0.76, 0.96) | 1 | |
| Orange | 1.04 ** | (0.92, 1.16) | 1 | 1.45 ** | (1.32, 1.58) | 1 | |
| Green | 3.87 ** | (3.61, 4.14) | 4 | 2.97 ** | (2.75, 3.19) | 2 | |
| Total | 5.56 ns | (5.27, 5.85) | 5 | 5.27 ns | (5.04, 5.50) | 4 | |
| Dinner | Selections | Before (n = 139) | After (n = 51 2) | ||||
| Mean | (95% CI) | Mode | Mean | (95% CI) | Mode | ||
| Red | 0.40 ** | (0.31, 0.50) | 0 | 1.31 ** | (1.08, 1.55) | 1 | |
| Orange | 1.15 ** | (1.03, 1.28) | 1 | 0.67 ** | (0.49, 0.84) | 2 | |
| Green | 3.94 ** | (3.65, 4.23) | 4 | 3.18 ** | (2.80, 3.56) | 3 | |
| Total | 5.50 ns | (5.21, 5.78) | 5 | 5.16 ns | (4.75, 5.56) | 5 | |
| Lunch | Number of Options Provided | Before n (%) | After n (%) |
| Red | 13 (16%) | 14 (17%) | |
| Orange | 21 (26%) | 21 (25%) | |
| Green | 47 (58%) | 48 (58%) | |
| Total | 81 (100%) | 83 (100%) | |
| Dinner | Number of Options Provided | Before n (%) | After n (%) |
| Red | 10 (14%) | 11 (25%) | |
| Orange | 17 (25%) | 6 (14%) | |
| Green | 42 (61%) | 27 (61%) | |
| Total | 69 (100%) | 44 (100%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carins, J.; Rundle-Thiele, S.; Ronto, R. Impact of Dining Hall Structural Changes on Food Choices: A Pre-Post Observational Study. Int. J. Environ. Res. Public Health 2020, 17, 913. https://doi.org/10.3390/ijerph17030913
Carins J, Rundle-Thiele S, Ronto R. Impact of Dining Hall Structural Changes on Food Choices: A Pre-Post Observational Study. International Journal of Environmental Research and Public Health. 2020; 17(3):913. https://doi.org/10.3390/ijerph17030913
Chicago/Turabian StyleCarins, Julia, Sharyn Rundle-Thiele, and Rimante Ronto. 2020. "Impact of Dining Hall Structural Changes on Food Choices: A Pre-Post Observational Study" International Journal of Environmental Research and Public Health 17, no. 3: 913. https://doi.org/10.3390/ijerph17030913
APA StyleCarins, J., Rundle-Thiele, S., & Ronto, R. (2020). Impact of Dining Hall Structural Changes on Food Choices: A Pre-Post Observational Study. International Journal of Environmental Research and Public Health, 17(3), 913. https://doi.org/10.3390/ijerph17030913