Living with Systemic Lupus Erythematosus: A Profile of Young Female Patients


 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Procedure
2.2. Measures
2.3. Statistical Analyses
3. Results
3.1. Socio-Demographic Profile of SLE Patients
3.2. Course of Disease
3.3. Health Status and Health Care Utilization
3.4. SLE Impact
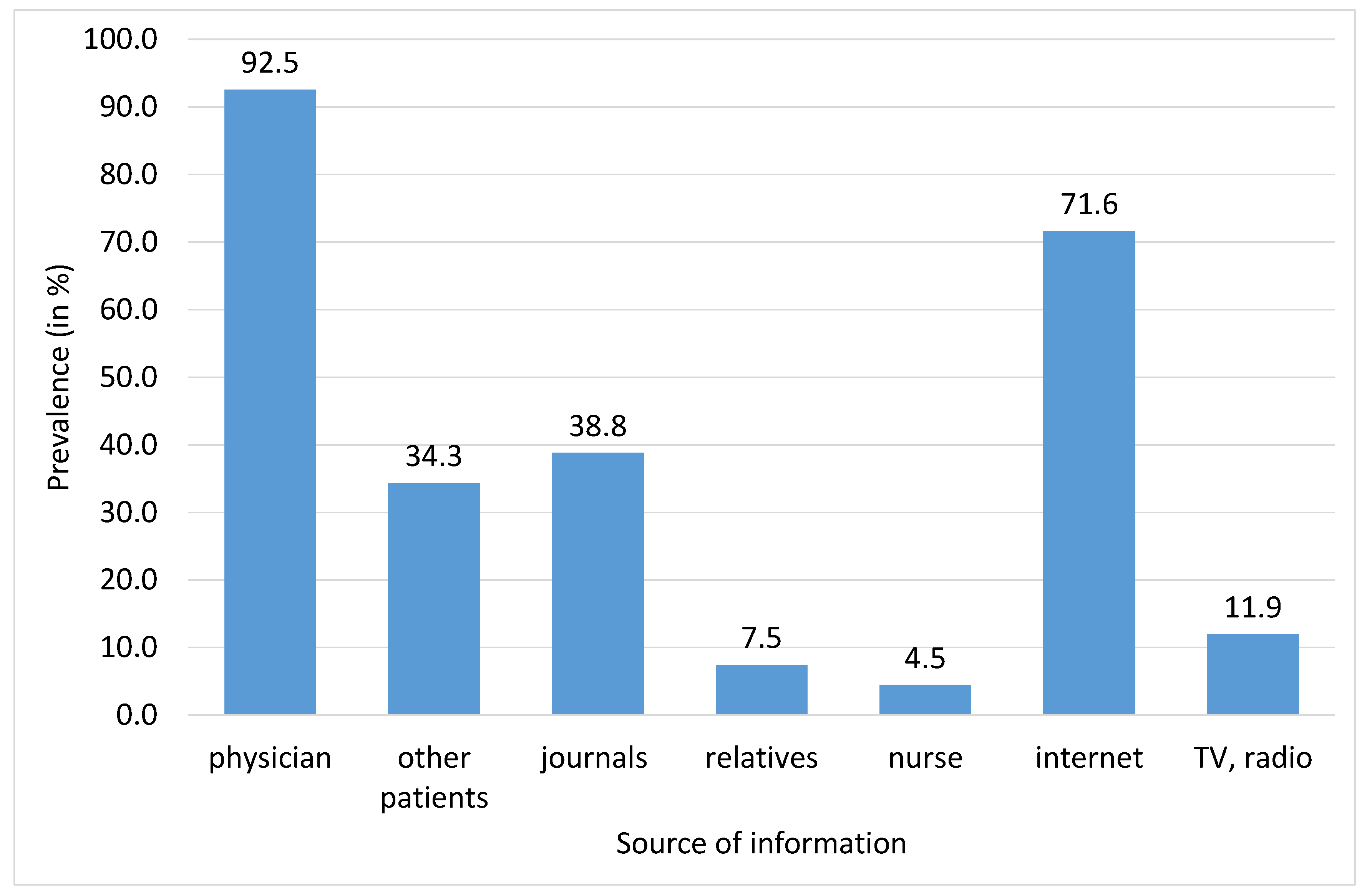
3.5. SLE Awareness
3.6. The Association of Patient’s Perspective with Clinical Activity
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ivorra, J.A.R.; Fernández-Llanio-Comella, N.; San-Martín-Álvarez, A.; Vela-Casasempere, P.; Saurí-Ferrer, I.; González-de-Julián, S.; Vivas-Consuelo, D. Health-related quality of life in patients with systemic lupus erythematosus: A Spanish study based on patient reports. Clin. Rheumatol. 2019, 38, 1857–1864. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.; Dekis, A.; Clarke, A.E. Hospitalizations in patients with systemic lupus erythematosus: Updated analyses from 2006 to 2011. Arthritis Res. Ther. 2012, 14, A59. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz-Oner, S.; Ilhan, B.; Can, M.; Alibaz-Oner, F.; Polat-Korkmaz, O.; Ozen, G.; Mumcu, G.; Kremers, H.M.; Tuglular, S.; Direskeneli, H. Fatigue in systemic lupus erythematosus: Association with disease activity, quality of life and psychosocial factors. Rheumatology 2017, 76, 913–919. [Google Scholar] [CrossRef] [PubMed]
- Lisnevskaia, L.; Murphy, G.; Isenberg, D. Systemic lupus erythematosus. Lancet 2014, 384, 1878–1888. [Google Scholar] [CrossRef]
- Fernández-Ávila, D.G.; Bernal-Macías, S.; Rincón-Riaño, D.N.; Gutiérrez Dávila, J.M.; Rosselli, D. Prevalence of systemic lupus erythematosus in Colombia: Data from the national health registry 2012–2016. Lupus 2019, 28, 1273–1278. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman-Górska, I. Postępy w Reumatologii Klinicznej; Lek. PZWL: Warsawa, Poland, 2014; pp. 129–159. [Google Scholar]
- McElhone, K.; Abbott, J.; The, L.S. A review of health related quality of life in systemic lupus erythematosus. Lupus 2006, 15, 633–643. [Google Scholar] [CrossRef] [PubMed]
- Marzena Olesińska, M.; Saletra, A. Quality of life in systemic lupus erythematosus and its measurement. Reumatologia 2018, 56, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Haikel, K.A.B.; Al Tulaihi, B. Awareness of systemic lupus erythematosus among primary health care patients in Riyadh, Saudi Arabia. Saudi Med. J. 2019, 40, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Vitali, C.; Bencivelli, W.; Isenberg, D.A.; Smolen, J.S.; Snaith, M.L.; Sciuto, M.; Neri, R.; Bombardieri, S. Disease activity in systemic lupus erythematosus: Report of the Consensus Study Group of the European Workshop for Rheumatology Research. II. Identification of the variables indicative of disease activity and their use in the development of an activity score. The European Consensus Study Group for Disease Activity in SLE. Exp. Rheumatol. 1992, 10, 541–547. [Google Scholar]
- Agarwal, N.; Kumar, V. Burden of lupus on work: Issues in the employment of individuals with lupus. Work 2016, 55, 429–439. [Google Scholar] [CrossRef] [PubMed]
- Ekblom-Kullberg, S.; Kautiainen, H.; Alha, P.; Leirisalo-Repo, M.; Julkunen, H. Education, employment, absenteeism, and work disability in women with systemic lupus erythematosus. Scand. J. Rheumatol. 2015, 44, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Macejová, Ž.; Záriková, M.; Oetterová, M. Systemic lupus erythematosus-disease impact on patients. Cen. Eur. J. Public Health 2013, 3, 171–173. [Google Scholar] [CrossRef] [Green Version]
- Drenkard, C.; Bao, G.; Dennis, G.; Kan, H.J.; Jhingran, P.M.; Molta, C.T.; Lim, S.S. Burden of systemic lupus erythematosus on employment and work productivity: Data from a large cohort in the southeastern United States. Arthritis Care Res. 2014, 66, 878–887. [Google Scholar] [CrossRef] [PubMed]
- Utset, T.O.; Baskaran, A.; Segal, B.M.; Trupin, L.; Ogale, S.; Herberich, E.; Kalunian, K. Work disability, lost productivity and associated risk factors in patients diagnosed with systemic lupus erythematosus. Lupus Sci. Med. 2015, 2, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, M.P.; Möller, S.; Bygum, A.; Voss, A.; Bliddal, M. Epidemiology of cutaneous lupus erythematosus and the associated risk of systemic lupus erythematosus: A nationwide cohort study in Denmark. Lupus 2018, 27, 1424–1430. [Google Scholar] [CrossRef] [PubMed]
- Kawalec, P.P.; Malinowski, K.P. The indirect costs of systemic autoimmune diseases, systemic lupus erythematosus, systemic sclerosis and sarcoidosis: A summary of 2012 real-life data from the Social Insurance Institution in Poland. Expert Rev. Pharm. Outcomes Res. 2015, 15, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Hajduk, A.; Nowicka-Sauer, K.; Smoleńska, Ż.; Czuszyńska, Z.; Zdrojewski, Z. Prevalence and correlates of suicidal thoughts in patients with neuropsychiatric lupus. Lupus 2016, 25, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Buyon, J.P.; Kim, M.Y.; Guerra, M.M.; Laskin, C.A.; Petri, M.; Lockshin, M.D.; Sammaritano, L.; Branch, D.W.; Porter, T.F.; Sawitzke, A.; et al. Predictors of pregnancy outcomes in patients with lupus: A cohort study. Ann. Intern. Med. 2015, 163, 153–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beusterien, K.; Bell, J.A.; Grinspan, J.; Utset, T.O.; Kan, H.; Narayanan, S. Physician-patient interactions and outcomes in systemic lupus erythematosus (SLE): A conceptual model. Lupus 2013, 22, 1038–1045. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Sayyed, Z.; Ameer, M.A.; Arif, A.W.; Kiran, F.N.U.; Iftikhar, A.; Iftikhar, W.; Ahmad, M.Q.; Malik, M.B.; Kumar, V.; et al. Systemic lupus erythematosus: An overview of the disease pathology and its management. Cureus 2018, 10, e3288. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| N (in %) | |
|---|---|
| Education | |
| University | 26 (38.8) |
| Secondary (school-leaving examination) | 26 (38.8) |
| Elementary or apprentice | 15 (22.4) |
| Living | |
| with partner | 36 (54.5) |
| with family relatives | 22 (33.3) |
| alone | 8 (12.1) |
| Having job or studying | |
| Student or employed | 36 (53.7) |
| Other | 31 (46.3) |
| Disablement due to SLE | |
| Without | 26 (38.8) |
| Partial disability retirement | 22 (32.8) |
| Full disability retirement | 19 (28.4) |
| Mean (SD); (Min-Max); Median | |
|---|---|
| Age | 44.03 (12.48); (23–79); 43.50 |
| Age when first symptoms occurred | 28.37 (11.88); (9–74); 25.00 |
| Age when diagnosed SLE | 29.92 (11.42); (10–74); 27.00 |
| Age when disability retirement was given | 33.05 (10.19); (18–54); 31.00 |
| Time between first symptoms and setting diagnose | 1.49 (2.19); (0–12); 1.00 |
| Average duration of SLE | 13.1 (8.1); (1–42); 13.00 |
| N (in %) | |
|---|---|
| SLE status | |
| Without symptoms | 10 (14.9) |
| Stabilized | 43 (64.2) |
| Relapse with symptoms | 12 (17.9) |
| Pharmacological treatment of SLE | |
| No | 2 (3.1) |
| Yes | 63 (96.9) |
| Visited physician in the past month due to SLE | |
| None | 15 (22.7) |
| Once in the past month | 28 (42.4) |
| At least twice in the past month | 23 (34.2) |
| Hospitalized in the past year due to SLE | |
| No | 40 (59.7) |
| Hospitalized at least once in the past year | 27 (40.3) |
| Health complaints during remission (at least once a week, significant symptom intensity) | |
| Fatigue | 24 (35.8) |
| Pain | 20 (29.9) |
| Decreased physical activity | 17 (25.4) |
| Cosmetic defects | 16 (23.9) |
| Dry mucosa | 8 (11.9) |
| Sleep difficulties | 9 (13.4) |
| Reduced motor skills | 10 (14.9) |
| Memory problems | 4 (6.0) |
| Depression | 2 (3.0) |
| No health complaint | 24 (35.8) |
| One health complaint | 22 (32.8) |
| Two and more health complaints | 21 (31.4) |
| Mean (SD); (Min–Max); Median | |
| ANA | 2.06 (0.81); (0–3); 2.00 |
| ECLAM | 1.94 (2.35); (0–7); 0.00 |
| Inflammation—ESR | 36.43 (16.67); (8.00–70.00); 38.00 |
| N (in %) | |
|---|---|
| SLE impact on life generally | |
| Very restrictive | 15 (23.1) |
| Restrictive | 37 (56.9) |
| Moderately or not restrictive | 13 (20.0) |
| SLE related restrictions in daily activities in the past week (considerable restrictions or impossibility to participate in activity) | |
| At work or at school | 19 (32.8) |
| Household chores | 27 (40.9) |
| Vigorous activities or doing sport | 51 (77.3) |
| Meetings with friends or relatives | 7 (10.6) |
| Participation on social events | 11 (16.7) |
| Being in sunshine | 53 (81.5) |
| Family life | 16 (24.6) |
| Relationship with partner | 13 (20.3) |
| Sexual life | 15 (23.8) |
| Missing varies from 1 to 9 | |
| Undesirable side effects of pharmacological treatment | |
| No | 13 (19.4) |
| Yes | 48 (71.6) |
| I do not know | 6 (9.0) |
| N (in %) | |
|---|---|
| Having sufficient information about SLE | 45 (67.2) |
| Having sufficient information about SLE treatment | 44 (65.7) |
| Be familiar with SLE patient organization | 33 (49.3) |
| Being a member of SLE patient organization | 11 (17.5) |
| ECLAM | ESR | ANA | ||||
|---|---|---|---|---|---|---|
| Mean (SD) | Significance | Mean (SD) | Significance | Mean (SD) | Significance | |
| Disablement | ns | ns | ns | |||
| (1) without | 1.50 (2.06) | 39.39 (15.84) | 2.15 (0.88) | |||
| (2) partial disability retirement | 2.27 (2.64) | 33.27 (17.47) | 1.86 (0.77) | |||
| (3) full disability retirement | 2.16 (2.39) | 35.74 (16.99) | 2.16 (0.77) | |||
| SLE status | p ˂ 0.001 | p ˂ 0.001 | p ˂ 0.001 | |||
| (1) remission without symptoms | 0.30 (0.68) | 1vs.3, 2vs.3 | 17.90 (3.07) | 1vs.2,1vs.3, 2vs.3 | 1.30 (0.48) | 1vs.2,1vs.3, 2vs.3 |
| (2) stabilized | 1.81 (2.05) | 37.35 (15.48) | 2.07 (0.74) | |||
| (3) with symptoms | 4.00 (3.02) | 51.17 (11.42) | 2.83 (0.39) | |||
| Visited physician in the past month | ns | p ˂ 0.05 | ns | |||
| (1) none | 1.53 (1.85) | 29.60 (13.33) | 1vs3 | 2.07 (0.80) | ||
| (2) once in the past month | 1.57 (2.15) | 34.61 (15.61) | 1.93 (0.72) | |||
| (3) at least twice in past month | 2.70 (2.79) | 43.65 (17.75) | 2.30 (0.82) | |||
| Being hospitalized in the past year | ns | ns | ns | |||
| (1) no | 1.78 (2.06) | 34.38 (16.16) | 1.93 (0.80) | |||
| (2) at least once in past year | 2.19 (2.75) | 39.26 (17.29) | 2.26 (0.81) | |||
| Health complaints at least once a week of significant intensity | ns | ns | ns | |||
| (1) none | 1.88 (2.36) | 34.96 (16.85) | 1.88 (0.85) | |||
| (2) one health complaint | 2.23 (2.35) | 33.18 (14.80) | 2.00 (0.82) | |||
| (3) two and more health complaints | 1.71 (2.41) | 41.24 (17.94) | 2.33 (0.73) | |||
| SLE impact on life | ns | ns | ns | |||
| (1) very restrictive | 2.73 (2.82) | 39.20 (20.55) | 2.33 (0.82) | |||
| (2) restrictive | 1.87 (2.28) | 37.97 (15.87) | 2.00 (0.78) | |||
| (3) moderately or not restrictive | 1.46 (2.02) | 31.23 (13.31) | 2.08 (0.76) | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macejova, Z.; Madarasova Geckova, A.; Husarova, D.; Zarikova, M.; Kotradyova, Z. Living with Systemic Lupus Erythematosus: A Profile of Young Female Patients. Int. J. Environ. Res. Public Health 2020, 17, 1315. https://doi.org/10.3390/ijerph17041315
Macejova Z, Madarasova Geckova A, Husarova D, Zarikova M, Kotradyova Z. Living with Systemic Lupus Erythematosus: A Profile of Young Female Patients. International Journal of Environmental Research and Public Health. 2020; 17(4):1315. https://doi.org/10.3390/ijerph17041315
Chicago/Turabian StyleMacejova, Zelmira, Andrea Madarasova Geckova, Daniela Husarova, Michaela Zarikova, and Zuzana Kotradyova. 2020. "Living with Systemic Lupus Erythematosus: A Profile of Young Female Patients" International Journal of Environmental Research and Public Health 17, no. 4: 1315. https://doi.org/10.3390/ijerph17041315
APA StyleMacejova, Z., Madarasova Geckova, A., Husarova, D., Zarikova, M., & Kotradyova, Z. (2020). Living with Systemic Lupus Erythematosus: A Profile of Young Female Patients. International Journal of Environmental Research and Public Health, 17(4), 1315. https://doi.org/10.3390/ijerph17041315