Understanding the Experiences and Needs of Migrant Women Affected by Female Genital Mutilation Using Maternity Services in Australia


Abstract
:1. Introduction
2. Materials and Methods
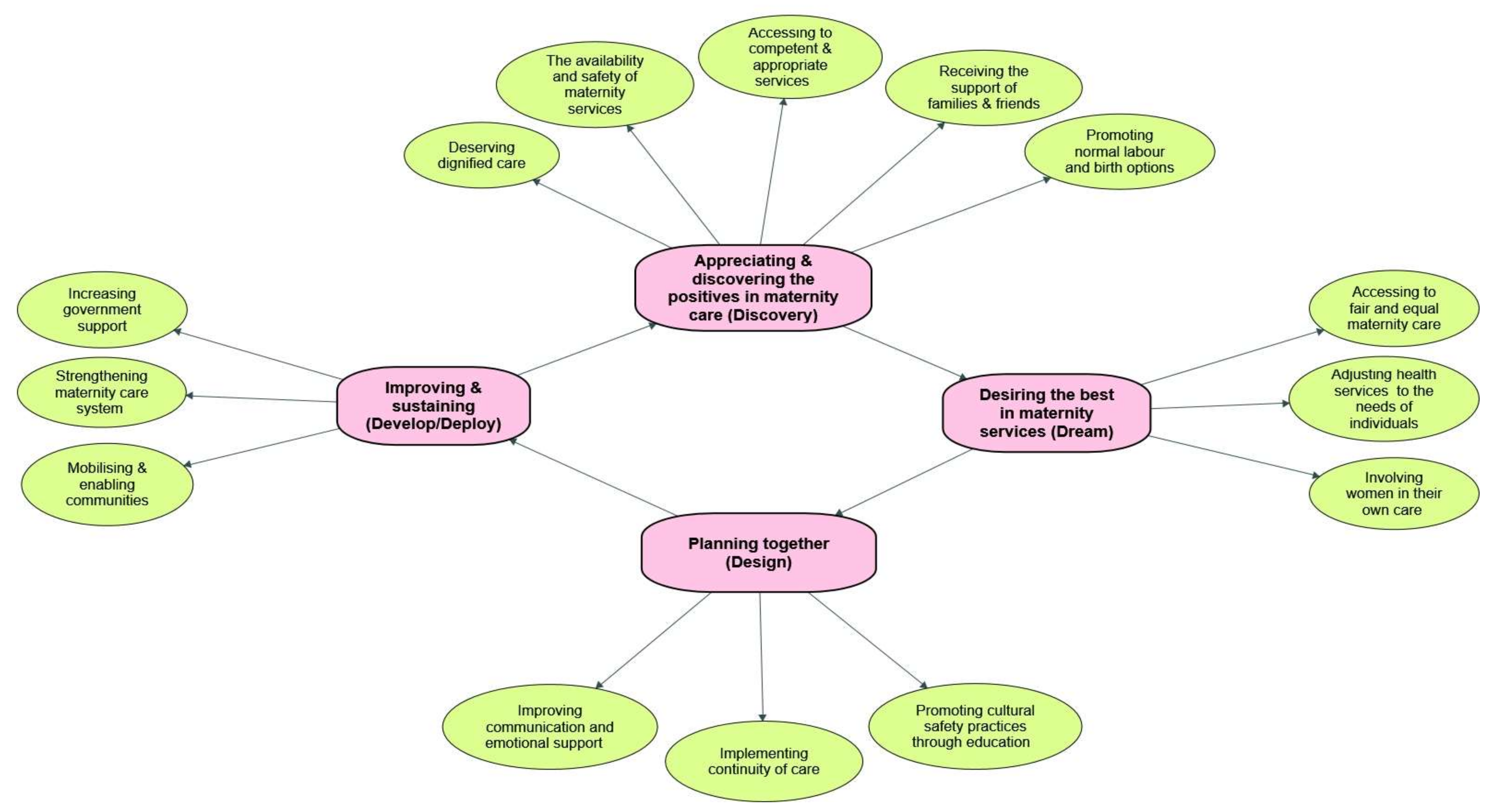
3. Results
3.1. Appreciating and Discovering the Positives in Maternity Care (Discovering)
The good thing was always feeling safe, knowing there are all the facilities, medicines and machines and skills you might need available within the hospital. I really felt relaxed in both my deliveries. Overall pregnancy was a happy experience for me and I knew they would help me straightaway compared to my country where nothing is available.(W18)
… it is not like that the doctors and midwives in Australia come across a circumcised woman every day, you know. And I don’t blame them if they are surprised or ask you millions of questions.(W13)
The medical staff need to understand this issue [FGM] and be knowledgeable about it and if they don’t have hands-on experience and skills please do not touch us and make our situation worse. You need to feel safe knowing that they get training before coming to women with FGM.(W23)
If these midwives and doctors know where to cut (de-infibulation), how to cut and when to cut it will be so helpful for us and for them because we will not have a problem and they will be relaxed and confident in what they do. Now, as soon as they see us they are shaking … Oh my God. They can get advice from doctors and midwives who worked in our country and have real experience of treatment of women with FGM.(FGD3)
3.2. Desiring the Best in Maternity Services (Dreaming)
They need to listen to women as they know their body better. Not everything is going to be according to the recipe in the book. They have to look at each individual pregnancy separately.
If a woman has undergone FGM they need to look after her even after birth and even if there is not any visible harm there is always a change and she needs that emotional support.(W20)
After they open you during delivery I wish there is someone who stitches it very very nicely so it doesn’t look very open.(FGD1)
…I went overseas and closed it by a midwife in my country. You know last time I [got] closed myself in Sudan it was because it was so big and ugly they left me totally open at least they could have stitched me back to make me look like normal.(W22)
My husband and mother in law made the decision for me. If it was up to me I would have chosen a caesar straightaway. I did not want all that pain and trauma, but midwife went with my husband and mother in law’s decision without listening to me.(FGD1)
Sometimes you are in a position where you have to follow whatever they say. Maybe because our knowledge is limited and the language also is a big, big problem.(W18)
3.3. Planning Together for Improved Maternity Services (Designing)
If I am a midwife I make you feel good and I need to understand what you believe in so I can understand if you see FGM as a good thing or bad thing. Then I can talk to you and guide you accordingly… first you need to get a sense of what women believe in, otherwise they may not disclose anything.(W12)
I was shy and hide my FGM until birth and I am sure many other would do that. In our culture women won’t talk about it believe me or not. There is shame and stigma with those topics’.(W23)
It is very important for women because we want to trust someone and by changing midwives and doctors we will be lost. I will also develop my confidence in her competence and make sure she can manage my birth and I am in safe hands. That’s a huge support for me knowing that I am safe and someone knows my issues and concerns.(W17)
You know little by little each time after I started to visit the doctors and midwives and they didn’t make me feel embarrassed [because of FGM] and they asked me so many questions when I went to them. And the way they talked to me was so good. You know, you feel so good when someone listens to you. They were not in a rush to get to the next patient and kick me out of their office. They spend time with you and do what they need to do while they kept privacy.(W13)
Sometimes you just want someone to talk to and ask for nothing else, just someone to ask you what your feelings after birth are or how you are because it is a hard time. … I want a midwife or nurse to provide care for me beyond giving medicines, I want them to talk to me and support me emotionally and mentally.(W17)
Sometimes they don’t even talk about FGM with us and just write everything down and say all is good without giving us the details. I think it is mostly because they don’t know anything about FGM and they just look at you and they have no idea.(W17)
3.4. Improving and Sustaining Maternity Services (Developing/Deploying)
Still many people in the community believe it is a good thing to do on their daughters [FGM]. … I will not let my daughter to undergo FGM but we need to remove pressure of the community on families. If no one wants a girl without FGM then everybody forced to do it. We need to end that by educating community and change this culture.(W22)
Change is dependent on families. In my family, I have already talked to my kids about the stuff like FGM and the even bigger impact of it on society. I think that’s how we will spread the word and stop it, otherwise it is never going to be stopped. Now people believe in this society that talking about this issue is wrong or Haram [prohibited by religion]. I don’t care; I will talk to my children because I don’t want them to grow up blindly.(W18)
At the moment most of the trainings are for women. We need men to talk to men so we can engage them otherwise you cannot force them to sit in a class. You need to train more men to open up and talk about this issue with other men in the community and engage them at the same level as women. Men are still looking at it as a good thing.(W15)
…We need to create an environment where people talk about it. You know it is very hard to disclose such issues at community level, as it is a very private matter. I guess if we bring up stories and how women are suffering this would be effective to change this culture in the future. Imagine you’re living for someone else’s pleasure and you’re getting none.(W13)
They [policy makers] need to identify women with FGM as a priority at policy level and provide them with things they want. We want services which all women deserve …. We are in a developed country and we should have access to standard care from an experienced health provider.(W21)
Make sure they [women affected with FGM] are OK, mentally and physically. Do the follow up afterwards. Education and individualised support not only for women who have undergone FGM but also to train staff and the community. It goes both ways.(W16)
Facilitating and funding community training such as workshops for men and women we can raise the awareness. It is also helpful to open the discussion around this issue. At the moment it is not culturally appropriate to even talk about it even in the family.(W20)
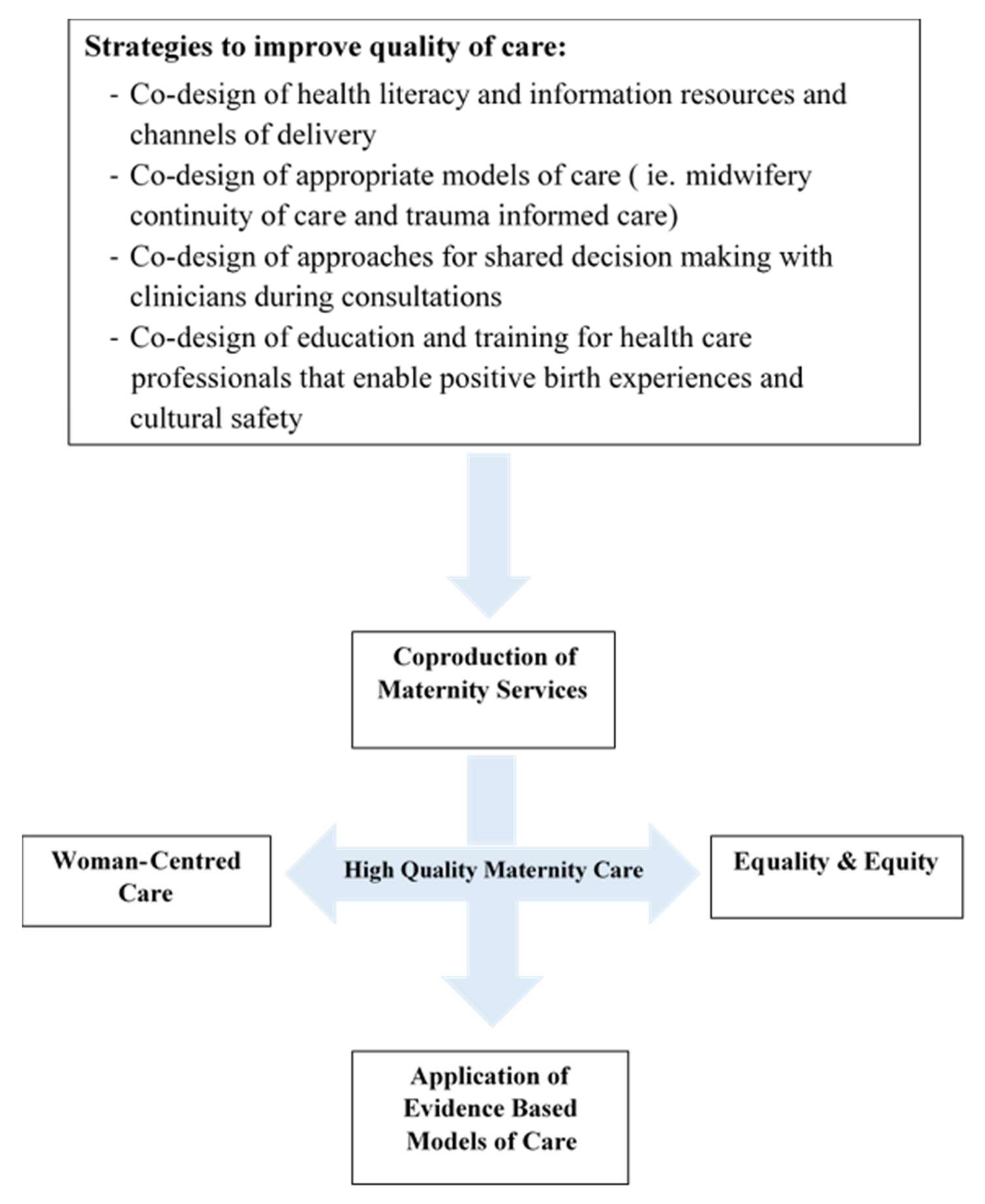
4. Discussion
4.1. Co-Design of Health Literacy Interventions
4.2. Co-Design of Evidence-Based Models of Care
4.3. Co-Design Approaches to Shared Decision Making
4.4. Co-Design of Health Professional Education and Training
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- UN. Eliminating Female Genital Mutilation: A Joint Interagency Statement; UNAIDS; UNDP; UNECA; UNESCO; UNFPA; UNHCHR; UNICEF; UNIFEM; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- UNICEF. The Dynamics of Social Change-Towards the Abandonment of Female Genital Mutilation/Cutting in Five African Countries; UNICEF: Florence, Italy, 2010. [Google Scholar]
- UNICEF. Female Genital Mutilation/Cutting: A Global Concern; UNICEF: New York, NY, USA, 2015. [Google Scholar]
- Korfker, D.G.; Reis, R.; Rijnders, M.E.; Meijer-van Asperen, S.; Read, L.; Sanjuan, M.; Herschderfer, K.; Buitendijk, S.E. The lower prevalence of female genital mutilation in the Netherlands: A nationwide study in Dutch midwifery practices. Int. J. Public Health 2012, 57, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Stockdale, J.; Fyle, J. Royal College of Midwives—Female Genital Mutilation: Report of a Survey on Midwives Views and Knowledge; The Royal College of Midwives: London, UK, 2012. [Google Scholar]
- WHO. WHO Guidelines on the Management of Health Complications from Female Genital Mutilation. 2016. Available online: Http://apps.who.int/iris/bitstream/10665/206437/1/9789241549646_eng.pdf?ua=1 (accessed on 17 October 2018).
- Blignault, I.; Haghshenas, A. Identification of Australians from culturally and linguistically diverse backgrounds in national health data collections. Aust. Health Rev. 2005, 29, 455–468. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, A.L.; Lisboa, M. Estimating the Prevalence of Female Genital Mutilation in Portugal. Public Health 2016, 139, 53–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziyada, M.M.; Norberg-Schulz, M.; Johansen, R.E.B. Estimating the magnitude of female genital mutilation/cutting in Norway: An extrapolation model. BMC Public Health 2016, 16, 110. [Google Scholar] [CrossRef] [Green Version]
- Australian Institute of Health and Welfare. Towards Estimating the Prevalence of Female Genital Mutilation/Cutting in Australia; AIHW: Canberra, Australia, 2019. [Google Scholar]
- Hulton, L.A.; Matthews, Z.; Stones, R.W. Aframework for the Evaluation of Quality of Care in Maternity Services; University of Southampton: Southampton, UK, 2000. [Google Scholar]
- Van den Broek, N.; Graham, W. Quality of care for maternal and newborn health: The neglected agenda. BJOG Int. J. Obstet. Gynaecol. 2009, 116 (Suppl. 1), 18–21. [Google Scholar] [CrossRef]
- Burnett, A.; Ndovi, T. The health of forced migrants. BMJ 2018, 363, k4200. [Google Scholar] [CrossRef]
- Varol, N.; Hall, J.J.; Black, K.; Turkmani, S.; Dawson, A. Evidence-based policy responses to strengthen health, community and legislative systems that care for women in Australia with female genital mutilation/cutting. Reproduct. Health 2017, 14, 63. [Google Scholar] [CrossRef] [Green Version]
- Gibson-Helm, M.; Teede, H.; Block, A.; Knight, M.; East, C.; Wallace, E.M.; Boyle, J. Maternal health and pregnancy outcomes among women of refugee background from African countries: A retrospective, observational study in Australia. BMC Pregnancy Childbirth 2014, 14, 392–403. [Google Scholar] [CrossRef]
- Belihu, F.B.; Davey, M.-A.; Small, R. Perinatal health outcomes of East African immigrant populations in Victoria, Australia: A population based study. BMC Pregnancy Childbirth 2016, 16, 86. [Google Scholar] [CrossRef] [Green Version]
- Dawson, A.J.; Turkmani, S.; Varol, N.; Nanayakkara, S.; Sullivan, E.; Homer, C.S.E. Midwives’ experiences of caring for women with female genital mutilation: Insights and ways forward for practice in Australia. Women Birth 2015, 28, 207–214. [Google Scholar] [CrossRef]
- Dawson, A.; Homer, C.S.; Turkmani, S.; Black, K.; Varol, N. A systematic review of doctors’ experiences and needs to support the care of women with female genital mutilation. Int. J. Gynecol. Obstet. 2015, 131, 35–40. [Google Scholar] [CrossRef]
- Dixon, S.; Agha, K.; Ali, F.; El-Hindi, L.; Kelly, B.; Locock, L.; Otoo-Oyortey, N.; Penny, S.; Plugge, E.; Hinton, L. Female genital mutilation in the UK—Where are we, where do we go next? Involving communities in setting the research agenda. Res. Involv. Engagem. 2018, 4, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connelly, E.; Murray, N.; Baillot, H.; Howard, N. Missing from the debate? A qualitative study exploring the role of communities within interventions to address female genital mutilation in Europe. BMJ Open 2018, 8, e021430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogunsiji, O. Female Genital Mutilation (FGM): Australian Midwives’ Knowledge and Attitudes. Health Care Women Int. 2014, 36, 179–193. [Google Scholar] [CrossRef] [PubMed]
- WHO. Standards for Improving Quality of Maternal and Newborn Care in Health Facilities. Available online: http://apps.who.int/iris/bitstream/10665/249155/1/9789241511216-eng.pdf?ua=1 (accessed on 16 December 2018).
- Kruk, M.E.; Gage, A.D.; Arsenault, C.; Jordan, K.; Leslie, H.H.; Roder-DeWan, S.; Adeyi, O.; Barker, P.; Daelmans, B.; Doubova, S.V.; et al. High-quality health systems in the Sustainable Development Goals era: Time for a revolution. Lancet Glob. Health 2018, 6, e1196–e1252. [Google Scholar] [CrossRef] [Green Version]
- Bazely, P. Qualitative Data Analysis: Practical Strategies; Sage: London, UK, 2013. [Google Scholar]
- Trajkovski, S.; Schmied, V.; Vickers, M.; Jackson, D. Using appreciative inquiry to transform health care. Contemp. Nurse 2013, 45, 95–100. [Google Scholar] [CrossRef]
- Chenail, R.J. How to conduct clinical qualitative research on the patient’s experience. Qual. Rep. 2011, 16, 1173–1189. [Google Scholar]
- Carter, C.A.; Ruhe, M.C.; Weyer, S.; Litaker, D.; Fry, R.E.; Stange, K.C. An appreciative inquiry approach to practice improvement and transformative change in health care settings. Qual. Manag. Healthc. 2007, 16, 194–204. [Google Scholar] [CrossRef] [Green Version]
- McAdam, E.; Mirza, K.A.H. Drugs, hopes and dreams: Appreciative inquiry with marginalized young people using drugs and alcohol. J. Fam. Ther. 2009, 31, 175–193. [Google Scholar] [CrossRef]
- Michael, S. The promise of appreciative inquiry as an interview tool for field research. Dev. Pract. 2005, 15, 222–230. [Google Scholar] [CrossRef]
- Reed, J. Appreciative Inquiry; Sage Publications: Thousand Oaks, CA, USA, 2006. [Google Scholar]
- Edwin, T.C. Appreciative Inquiry: A Positive Approach to Change; Institute for Public Service and Policy Research, University of South Carolina: Columbia, SC, USA, 2013. [Google Scholar]
- Berggren, V.; Bergstrom, S.; Edberg, A.-K. Being different and vulnerable: Experiences of immigrant African women who have been circumcised and sought maternity care in Sweden. J. Transcult. Nurs. 2006, 17, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Centre for Epidemiology and Evidence. New South Wales Mothers and Babies; Ministry of Health: Sydney, NSW, Australia, 2017.
- Heckathorn, D.D. Respondent-driven sampling: A new approach to the study of hidden populations. Soc. Probl. 1997, 44, 174–199. [Google Scholar] [CrossRef]
- Penrod, J.; Preston, D.B.; Cain, R.E.; Starks, M.T. A discussion of chain referral as a method of sampling hard-to-reach populations. J. Transcult. Nurs. 2003, 14, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Gill, P.; Stewart, K.; Treasure, E.; Chadwick, B. Methods of data collection in qualitative research: Interviews and focus groups. Br. Dent. J. 2008, 204, 291–295. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Stuckey, H. The first step in Data Analysis: Transcribing and managing qualitative research data. J. Soc. Health Diabet. 2014, 2, 6–8. [Google Scholar] [CrossRef] [Green Version]
- Creswell, J.W. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 2nd ed.; Sage Publications: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Woods, L. Qualitative Data Analysis—Explorations with NVivo. Nurse Res. 2002, 9, 86–87. [Google Scholar] [CrossRef]
- WHO. Care of Girls and Women Living with Female Genital Mutilation: A Clinical Handbook; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Van Rossem, R.; Meekers, D.; Gage, A.J. Women’s position and attitudes towards female genital mutilation in Egypt: A secondary analysis of the Egypt demographic and health surveys, 1995–2014. BMC Public Health 2015, 15, 1. [Google Scholar] [CrossRef] [Green Version]
- Carolan, M.; Cassar, L. Antenatal care perceptions of pregnant African women attending maternity services in Melbourne, Australia. Midwifery 2010, 26, 189–201. [Google Scholar] [CrossRef]
- Lundberg, P.C.; Gerezgiher, A. Experiences from pregnancy and childbirth related to female genital mutilation among Eritrean immigrant women in Sweden. Midwifery 2008, 24, 214–225. [Google Scholar] [CrossRef]
- Homer, C.S.; Foureur, M.J.; Allende, T.; Pekin, F.; Caplice, S.; Catling-Paull, C. ‘It’s more than just having a baby’ women’s experiences of a maternity service for Australian Aboriginal and Torres Strait Islander families. Midwifery 2012, 28, e509–e515. [Google Scholar] [CrossRef] [PubMed]
- Turkmani, S.; Homer, C.S.E.; Dawson, A. Maternity care experiences and health needs of migrant women from female genital mutilation–practicing countries in high-income contexts: A systematic review and meta-synthesis. Birth 2019, 46, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Gustavsson, S.; Gremyr, I.; Kenne, S.E. Designing quality of care—Contributions from parents; Parents’ experiences of care processes in paediatric care and their contribution to improvements of the care process in collaboration with healthcare professionals. J. Clin. Nurs. 2015, 25, 742–751. [Google Scholar] [CrossRef]
- Alo, O.A.; Gbadebo, B. Intergenerational attitude changes regarding female genital cutting in Nigeria. J. Women Health 2011, 20, 1655–1661. [Google Scholar] [CrossRef] [PubMed]
- Asekun-Olarinmoye, E.O.; Amusan, O.A. The impact of health education on attitudes towards female genital mutilation (FGM) in a rural Nigerian community. Eur. J. Contracept. Reproduct. Health Care 2008, 13, 289–297. [Google Scholar] [CrossRef]
- Origlia, P.; Jevitt, C.; Sayn-Wittgenstein, F.Z.; Cignacco, E. Experiences of Antenatal Care Among Women Who Are Socioeconomically Deprived in High-Income Industrialized Countries: An Integrative Review. J. Midwifery Women Health 2017, 62, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Ebert, L.; Bellchambers, H.; Ferguson, A.; Browne, J. Socially disadvantaged women’s views of barriers to feeling safe to engage in decision-making in maternity care. Women Birth 2014, 27, 132–137. [Google Scholar] [CrossRef]
- Svensson, P.; Carlzén, K.; Agardh, A. Exposure to culturally sensitive sexual health information and impact on health literacy: A qualitative study among newly arrived refugee women in Sweden. Cult. Health Sex. 2017, 19, 752–766. [Google Scholar] [CrossRef] [Green Version]
- Manderson, L.; Allotey, P. Storytelling, marginality, and community in Australia: How immigrants position their difference in health care settings. Med. Anthropol. 2003, 22, 1–21. [Google Scholar] [CrossRef]
- Mattern, E.; Lohmann, S.; Ayerle, G.M. Experiences and wishes of women regarding systemic aspects of midwifery care in Germany: A qualitative study with focus groups. BMC Pregnancy Childbirth 2017, 17, 389. [Google Scholar] [CrossRef]
- Renfrew, M.J.; McFadden, A.; Bastos, M.H.; Campbell, J.; Channon, A.A.; Cheung, N.F.; Silva, D.R.A.D.; Downe, S.; Kennedy, H.P.; Malata, A.; et al. Midwifery and quality care: Findings from a new evidence-informed framework for maternal and newborn care. Lancet 2014, 384, 1129–1145. [Google Scholar] [CrossRef]
- Andro, A.; Cambois, E.; Lesclingand, M. Long-term consequences of female genital mutilation in a European context: Self perceived health of FGM women compared to non-FGM women. Soc. Sc. Med. 2014, 106, 177–184. [Google Scholar] [CrossRef]
- Vloeberghs, E.; Van der Kwaak, A.; Knipscheer, J.; van den Muijsenbergh, M. Coping and chronic psychosocial consequences of female genital mutilation in the Netherlands. Ethn. Health 2012, 17, 677–695. [Google Scholar] [CrossRef] [PubMed]
- Liao, L.M.; Elliott, C.; Ahmed, F.; Creighton, S.M. Adult recall of childhood female genital cutting and perceptions of its effects: A pilot study for service improvement and research feasibility. J. Obstet. Gynaecol. 2013, 33, 292–295. [Google Scholar] [CrossRef]
- Caillet, M.; O’Neill, S.; Minsart, A.F.; Richard, F. Addressing FGM with Multidisciplinary Care. The Experience of the Belgian Reference Center CeMAViE. Curr. Sex. Health Rep. 2018, 10, 44–49. [Google Scholar] [CrossRef]
- Shaw, D.; Guise, J.M.; Shah, N.; Gemzell-Danielsson, K.; Joseph, K.S.; Levy, B.; Wong, F.; Woodd, S.; Main, E.K. Drivers of maternity care in high-income countries: Can health systems support woman-centred care? Lancet 2016, 388, 2282–2295. [Google Scholar] [CrossRef]
- Asma, H.; Trister, G.K.; Nicole, W. A Meta-Synthesis of the Birth Experiences of African Immigrant Women Affected by Female Genital Cutting. J. Midwifery Women Health 2018, 63, 185–195. [Google Scholar]
- Wilson, J.M.; Fauci, J.E.; Goodman, L.A. Bringing trauma-informed practice to domestic violence programs: A qualitative analysis of current approaches. Am. J. Orthopsychiatry 2015, 85, 586–599. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, S. Intersectional Trauma-Informed Intimate Partner Violence (IPV) Services: Narrowing the Gap between IPV Service Delivery and Survivor Needs. J. Fam. Violence 2019, 34, 55–64. [Google Scholar] [CrossRef]
- Mihelicova, M.; Brown, M.; Shuman, V. Trauma-Informed Care for Individuals with Serious Mental Illness: An Avenue for Community Psychology’s Involvement in Community Mental Health. Am. J. Orthopsychiatry 2018, 61, 141–152. [Google Scholar] [CrossRef]
- Castro, E.M.; Malfait, S.; Van Regenmortel, T.; Van Hecke, A.; Sermeus, W.; Vanhaecht, 5. Co-design for implementing patient participation in hospital services: A discussion paper. Patient Educ. Couns. 2018, 101, 1302–1305. [Google Scholar] [CrossRef] [PubMed]
- Correa-Velez, I.; Ryan, J. Developing a best practice model of refugee maternity care. Women Birth 2012, 25, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Dahlberg, U.; Aune, I. The woman’s birth experience—The effect of interpersonal relationships and continuity of care. Midwifery 2013, 29, 407–415. [Google Scholar] [CrossRef] [PubMed]
- WHO. Recommendations: Intrapartum Care for a Positive Childbirth Experience; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Hackett, C.L.; Mulvale, G.; Miatello, A. Co-designing for quality: Creating a user-driven tool to improve quality in youth mental health services. Health Expect. 2018, 21, 1013–1023. [Google Scholar] [CrossRef] [PubMed]
- Higginbottom, G.M.A.; Hadziabdic, E.; Yohani, S.; Paton, P. Immigrant women’s experience of maternity services in Canada: A meta-ethnography. Midwifery 2014, 30, 544–559. [Google Scholar] [CrossRef]
- Longtin, Y.; Sax, H.; Leape, L.L.; Sheridan, S.E.; Donaldson, L.; Pittet, D. Patient participation: Current knowledge and applicability to patient safety. Mayo Clin. Proc. 2010, 85, 53–62. [Google Scholar] [CrossRef] [Green Version]
- Repper, J.; Breeze, J. User and carer involvement in the training and education of health professionals: A review of the literature. Int. J. Nurs. Stud. 2007, 44, 511–519. [Google Scholar] [CrossRef]
- Kieft, R.A.; de Brouwer, B.B.; Francke, A.L.; Delnoij, D.M. How nurses and their work environment affect patient experiences of the quality of care: A qualitative study. BMC Health Serv. Res. 2014, 14, 249–258. [Google Scholar] [CrossRef] [Green Version]
- Coupland, K.; Davis, E.; Gregory, K. Learning from life. Mental Health Care 2001, 4, 166–169. [Google Scholar]
- Beckett, K.; Earthy, S.; Sleney, J.; Barnes, J.; Kellezi, B.; Barker, M.; Clarkson, J.; Coffey, F.; Elder, G.; Kendrick, D.; et al. Providing effective trauma care: The potential for service provider views to enhance the quality of care (qualitative study nested within a multicentre longitudinal quantitative study). BMJ Open 2014, 4, e005668. [Google Scholar] [CrossRef] [Green Version]
- Stickley, T.; Rush, B.; Shaw, R.; Smith, A.; Collier, R.; Cook, J.; Shaw, T.; Gow, D.; Felton, A.; Roberts, S. Participation in nurse education: The PINE project. J. Mental Health Train. Educ. Pract. 2009, 4, 11–18. [Google Scholar] [CrossRef]
- Simpson, A.; Reynolds, L.; Light, I.; Attenborough, J. Talking with the experts: Evaluation of an online discussion forum involving mental health service users in the education of mental health nursing students. Nurse Educ. Today 2008, 28, 633–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Study Code | Age | Age Underwent FGM | Country of Origin | Date of Last Birth in Australia | Education Level | First Language | Employment Status | # Children Born in Australia | # Live Birth | Years Lived in Australia |
|---|---|---|---|---|---|---|---|---|---|---|
| Astur | 30–35 | 5–10 | Somali | 2012 | Secondary | Somali | Employed | 1 | 1 | 20–25 |
| Bilan | 30–35 | 5–10 | Somali | 2005 | Primary | Somali | Housewife | 5 | 5 | 20–25 |
| Calaso | 30–35 | 1–5 | Somali | 2013 | Secondary | Somali | Employed | 1 | 1 | 10–15 |
| Bilqis | 30–35 | 1–5 | Somali | 2010 | Secondary | Somali | Employed | 3 | 3 | 20–25 |
| Indah | 40–45 | <1 | Indonesia | 2004 | Tertiary | Indonesian | Employed | 3 | 3 | 15–20 |
| Aminata | 40–45 | 10–15 | Sierra Leone | 2013 | Tertiary | Creole Temne | Employed | 2 | 3 | 10–15 |
| Binta | 25–30 | 5–10 | Sierra Leone | 2016 | Tertiary | Temne | Employed | 2 | 2 | 15–20 |
| Arifa | 30–35 | 1–5 | Sudan | 2013 | Secondary | Arabic | Employed | 3 | 4 | 10–15 |
| Fiza | 35–40 | 5–10 | Sudan | 2009 | Tertiary | Arabic | Employed | 2 | 2 | 15–20 |
| Mariatu | 25–30 | 15–20 | Sierra Leone | 2017 | Secondary | Creole Temne | Housewife | 2 | 2 | 5–10 |
| Hiba | 40–45 | 1–5 | Sudan | 2011 | Secondary | Arabic | Housewife | 3 | 5 | 10–15 |
| Nadia | 40–45 | <1 | Sudan | 2006 | Tertiary | Arabic | Employed | 1 | 1 | 10–15 |
| Rita | 35–40 | 1–5 | Sudan | 2015 | Tertiary | Arabic | Housewife | 3 | 5 | 5–10 |
| Yusra | 35–40 | 5–10 | Sudan | 2017 | Tertiary | Arabic | Housewife | 4 | 5 | 5–10 |
| Faduma | 40–45 | 1–5 | Somali | 2009 | Secondary | Somali | Housewife | 5 | 5 | 15–20 |
| Kia | 35–40 | 1–5 | Ethiopia | 2011 | Secondary | Arabic | Employed | 3 | 3 | 15–20 |
| Zara | 25–30 | 5–10 | Sudan | 2016 | Tertiary | Arabic | Housewife | 2 | 2 | 10–15 |
| Fatma | 40–45 | 1–5 | Sudan | 2012 | Secondary | Arabic | Housewife | 2 | 5 | 10–15 |
| Nour | 30–35 | 5–10 | Egypt | 2016 | Tertiary | Arabic | Employed | 3 | 3 | 5–10 |
| Gamal | 35–40 | 1–5 | Egypt | 2015 | Tertiary | Arabic | Employed | 3 | 3 | 5–10 |
| Asima | 30–35 | 1–5 | Sudan | 2014 | Tertiary | Arabic | Housewife | 1 | 1 | 5–10 |
| Harum | 35–40 | <1 | Indonesia | 2012 | Tertiary | Bahasa | Housewife | 2 | 3 | 5–10 |
| Zaineb | 40–45 | 1–5 | Somali | 2007 | Primary | Somali | Housewife | 1 | 1 | 10–15 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turkmani, S.; Homer, C.S.E.; Dawson, A.J. Understanding the Experiences and Needs of Migrant Women Affected by Female Genital Mutilation Using Maternity Services in Australia. Int. J. Environ. Res. Public Health 2020, 17, 1491. https://doi.org/10.3390/ijerph17051491
Turkmani S, Homer CSE, Dawson AJ. Understanding the Experiences and Needs of Migrant Women Affected by Female Genital Mutilation Using Maternity Services in Australia. International Journal of Environmental Research and Public Health. 2020; 17(5):1491. https://doi.org/10.3390/ijerph17051491
Chicago/Turabian StyleTurkmani, Sabera, Caroline S. E. Homer, and Angela J. Dawson. 2020. "Understanding the Experiences and Needs of Migrant Women Affected by Female Genital Mutilation Using Maternity Services in Australia" International Journal of Environmental Research and Public Health 17, no. 5: 1491. https://doi.org/10.3390/ijerph17051491
APA StyleTurkmani, S., Homer, C. S. E., & Dawson, A. J. (2020). Understanding the Experiences and Needs of Migrant Women Affected by Female Genital Mutilation Using Maternity Services in Australia. International Journal of Environmental Research and Public Health, 17(5), 1491. https://doi.org/10.3390/ijerph17051491