A Systematic Review and Meta-Analysis of Short-Term Ambient Ozone Exposure and COPD Hospitalizations


Abstract
:1. Introduction
2. Material and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Extraction
2.5. Risk-of-Bias Assessment
2.6. Data Synthesis
2.7. Statistical Methods
3. Results
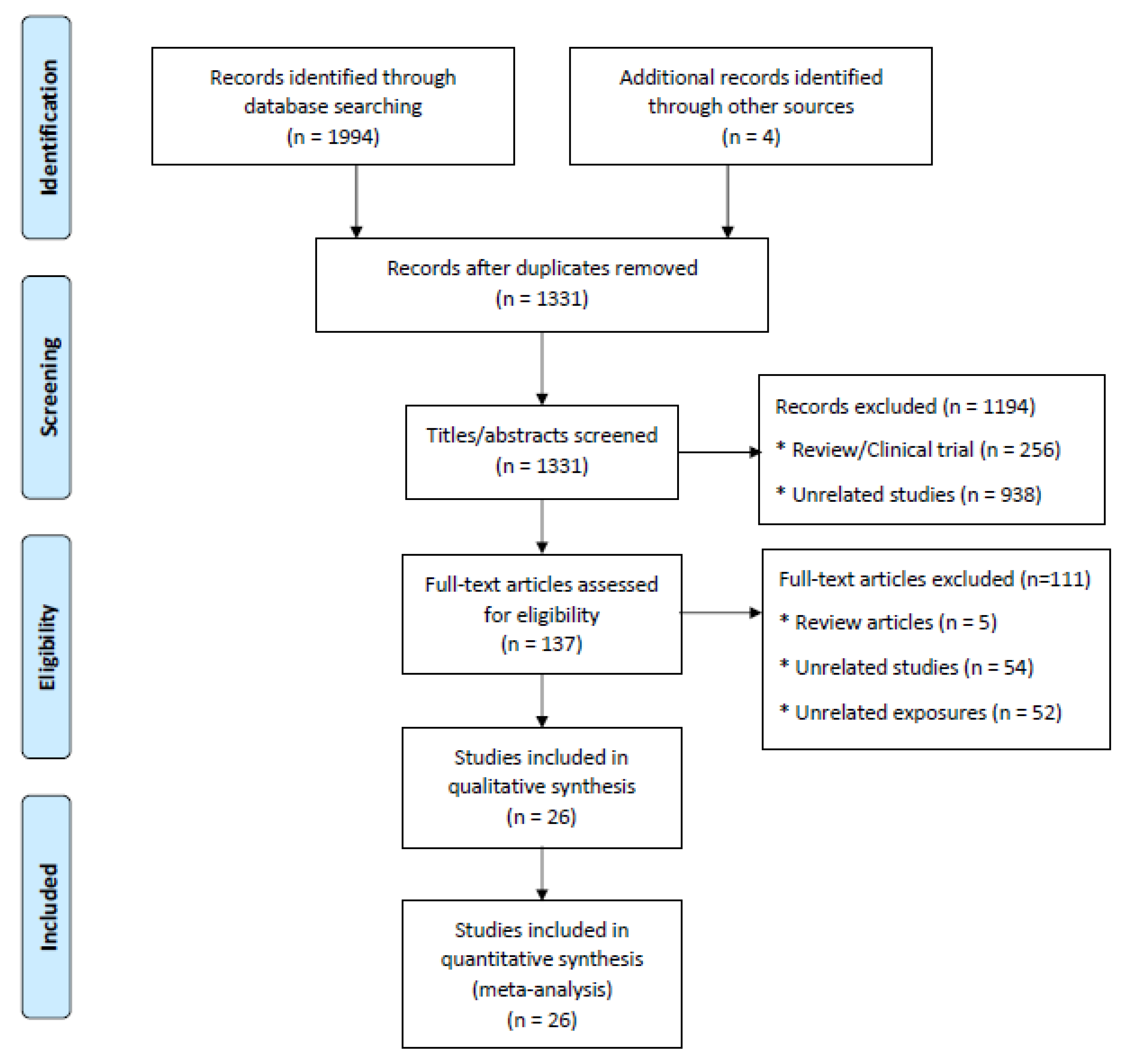
3.1. Search Findings and Study Characteristics
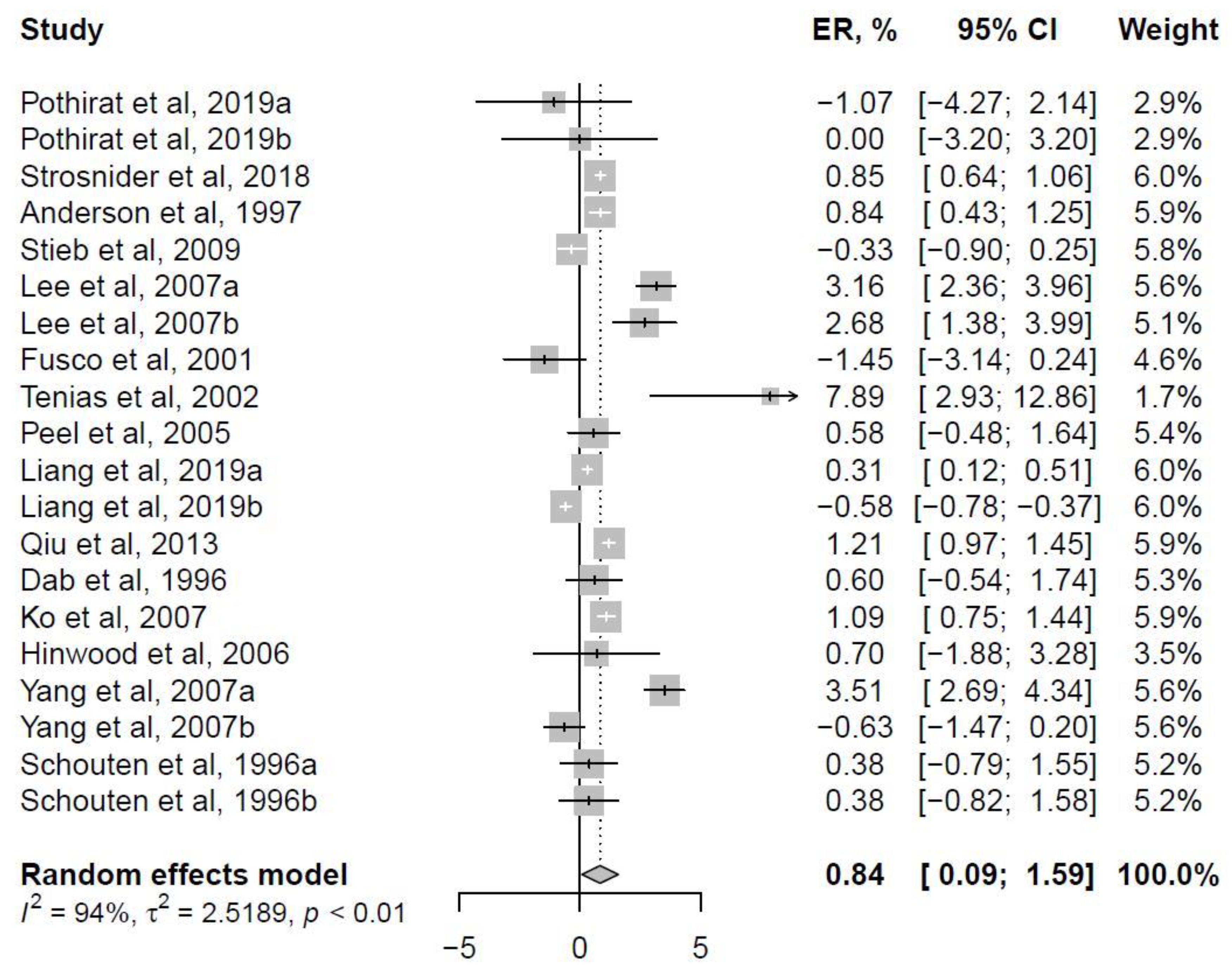
3.2. Ambient Level Ozone Exposure and COPD Hospitalizations
3.3. Publication Bias
3.4. Heterogeneity by Meta-Analysis
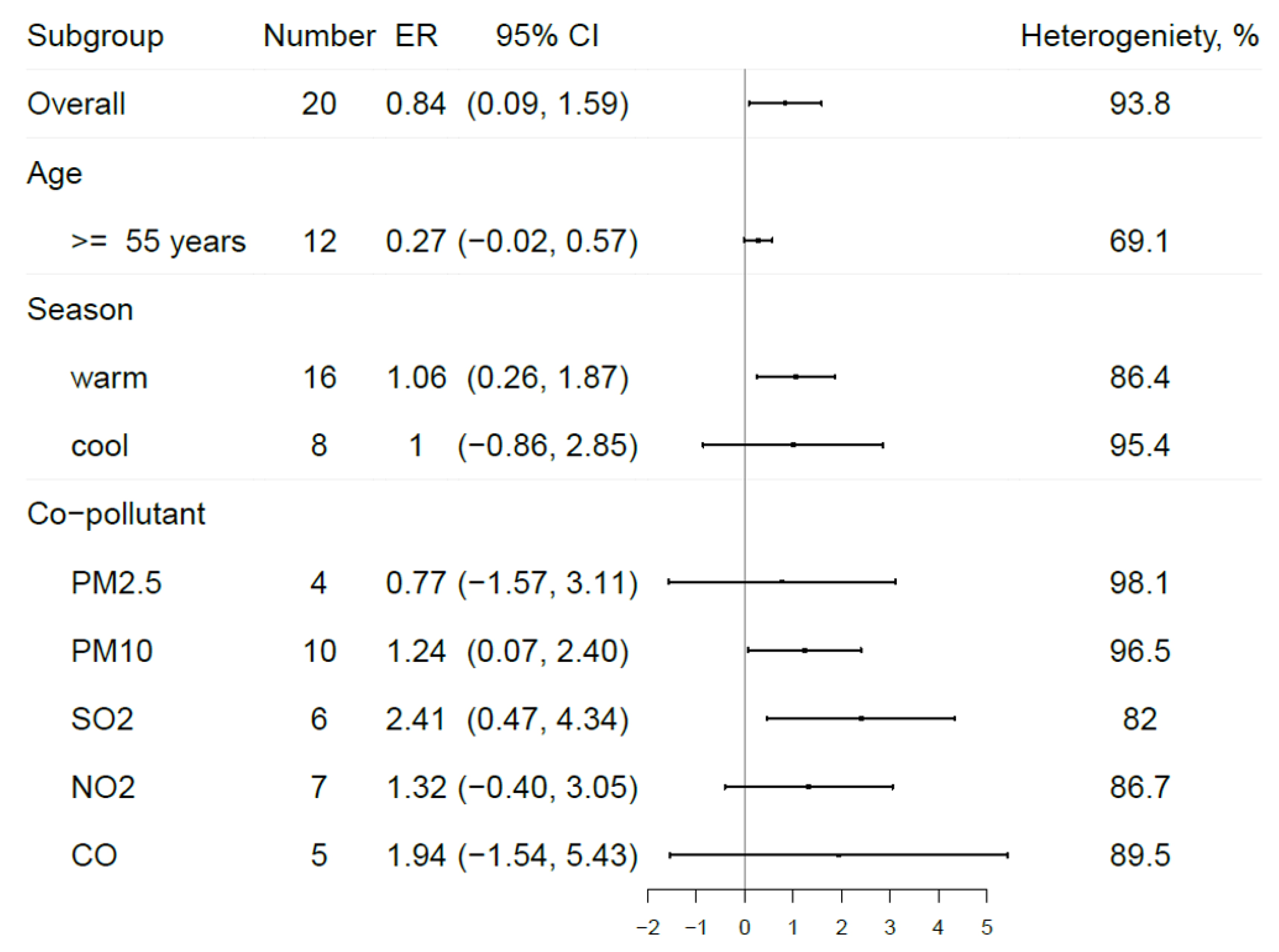
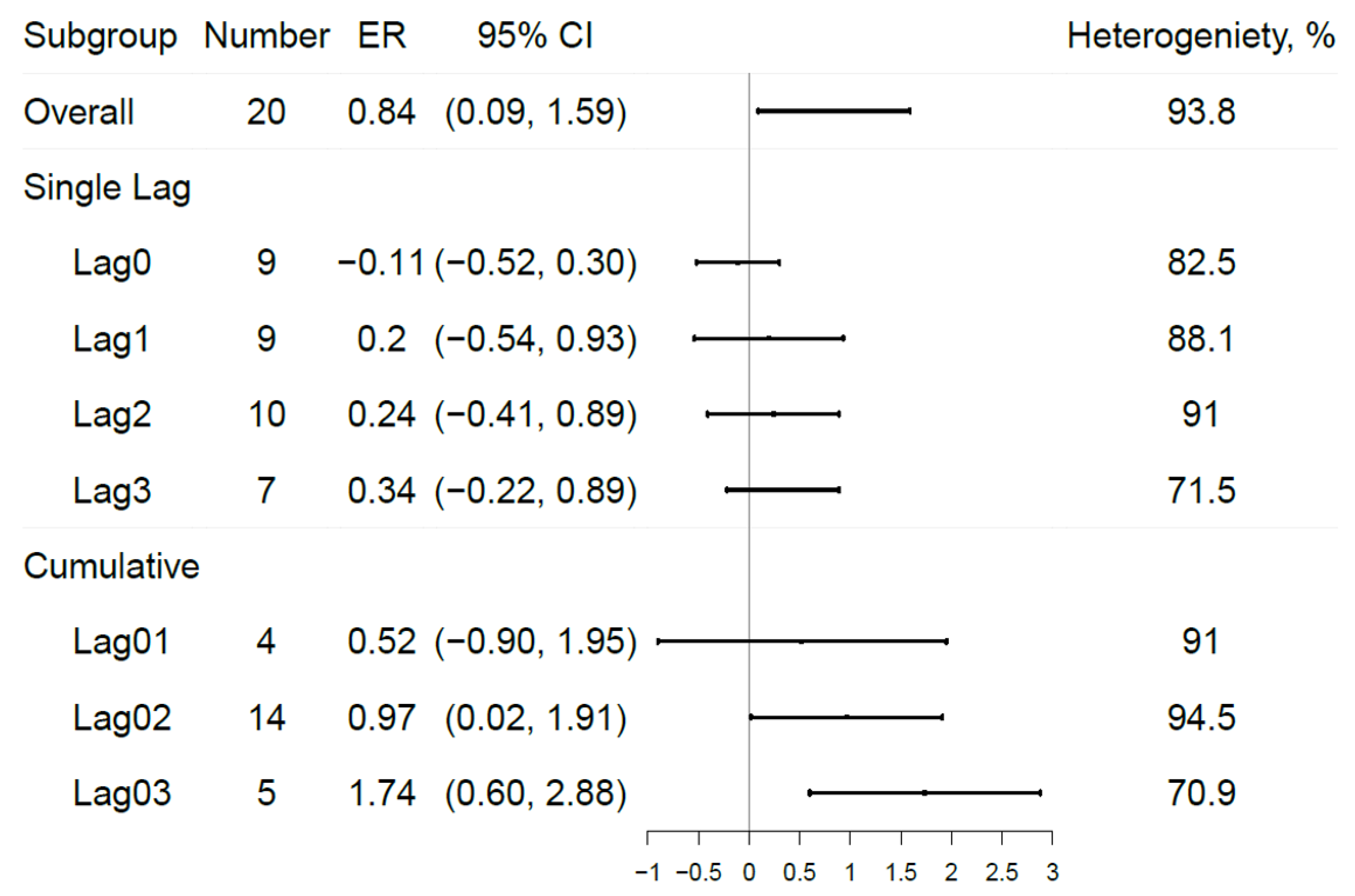
3.5. Subgroup Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Burney, P.G.; Patel, J.; Newson, R.; Minelli, C.; Naghavi, M. Global and regional trends in COPD mortality, 1990–2010. Eur. Respir. J. 2015, 45, 1239–1247. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Abajobir, A.A.; Abate, K.H.; Abera, S.F.; Agrawal, A.; Ahmed, M.B.; Aichour, A.N.; Aichour, I.; Aichour, M.T.E.; Alam, K.; et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Resp. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, R.W.; Kang, S.; Anderson, H.R.; Mills, I.C.; Walton, H.A. Epidemiological time series studies of PM2.5 and daily mortality and hospital admissions: A systematic review and meta-analysis. Thorax 2014, 69, 660–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.H.; Fan, L.C.; Mao, B.; Yang, J.W.; Choi, A.M.K.; Cao, W.J.; Xu, J.F. Short-term Exposure to Ambient Fine Particulate Matter Increases Hospitalizations and Mortality in COPD: A Systematic Review and Meta-analysis. Chest 2016, 149, 447–458. [Google Scholar] [CrossRef]
- Huls, A.; Schikowski, T. Ambient particulate matter and COPD in China: A challenge for respiratory health research. Thorax 2017, 72, 771–772. [Google Scholar] [CrossRef] [PubMed]
- Amoatey, P.; Takdastan, A.; Sicard, P.; Hooke, P.K.; Baawain, M.; Omidvarborna, H.; Allahyari, S.; Esmaeilzadeh, A.; De Marco, A.; Khanaibadi, Y.O. Short and long-term impacts of ambient ozone on health in Ahvaz, Iran. Hum. Ecol. Risk Assess. 2019, 25, 1336–1351. [Google Scholar] [CrossRef]
- English, P.; Balmes, J. Associations between Ozone and Fine Particulate Matter and Respiratory Illness Found to Vary between Children and Adults Implications for US Air Quality Policy. Am. J. Respir. Crit. Care Med. 2019, 199, 817–819. [Google Scholar] [CrossRef]
- Schwartz, J. The Year of Ozone. Am. J. Respir. Crit. Care Med. 2016, 193, 1077–1079. [Google Scholar] [CrossRef] [Green Version]
- U.S. Environmental Protection Agency. EPA Air Quality Criteria for Ozone and Related Photochemical Oxidants (Final Report, 2006); U.S. Environmental Protection Agency: Washington, DC, USA, 2006.
- Khaniabadi, Y.O.; Daryanoosh, M.; Sicard, P.; Takdastan, A.; Hopke, P.K.; Esmaeili, S.; De Marco, A.; Rashidi, R. Chronic obstructive pulmonary diseases related to outdoor PM10, O3, SO2, and NO2 in a heavily polluted megacity of Iran. Environ. Sci. Pollut. Res. Int. 2018, 25, 17726–17734. [Google Scholar] [CrossRef]
- De Marco, A.; Proietti, C.; Anav, A.; Ciancarella, L.; D’Elia, I.; Fares, S.; Fornasier, M.F.; Fusaro, L.; Gualtieri, M.; Manes, F.; et al. Impacts of air pollution on human and ecosystem health, and implications for the National Emission Ceilings Directive: Insights from Italy. Environ. Int. 2019, 125, 320–333. [Google Scholar] [CrossRef]
- Sicard, P.; Khaniabadi, Y.O.; Perez, S.; Gualtieri, M.; De Marco, A. Effect of O3, PM10 and PM2.5 on cardiovascular and respiratory diseases in cities of France, Iran and Italy. Environ. Sci. Pollut. Res. Int. 2019, 26, 32645–32665. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.Q.; Li, G.X.; Tian, L.; Guo, Q.; Pan, X.C. Short-term exposure to air pollution and morbidity of COPD and asthma in East Asian area: A systematic review and meta-analysis. Environ. Res. 2016, 148, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Ji, M.; Cohan, D.S.; Bell, M.L. Meta-analysis of the association between short-term exposure to ambient ozone and respiratory hospital admissions. Environ. Res. Lett. 2011, 6, 024006. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.; Chatzidiakou, L.; Kuku, M.O.; Jones, R.L.; Smeeth, L.; Beevers, S.; Kelly, F.J.; Barratt, B.; Quint, J.K. Global Associations between Air Pollutants and Chronic Obstructive Pulmonary Disease Hospitalizations A Systematic Review. Ann. Am. Thorac. Soc. 2016, 13, 1814–1827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.H.; Sun, S.Z.; Tang, R.; Qiu, H.; Huang, Q.Y.; Mason, T.G.; Tian, L.W. Major air pollutants and risk of COPD exacerbations: A systematic review and meta-analysis. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 3079–3091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reid, C.E.; Considine, E.M.; Watson, G.L.; Telesca, D.; Pfister, G.G.; Jerrett, M. Associations between respiratory health and ozone and fine particulate matter during a wildfire event. Environ. Int. 2019, 129, 291–298. [Google Scholar] [CrossRef]
- Pothirat, C.; Chaiwong, W.; Liwsrisakun, C.; Bumroongkit, C.; Deesomchok, A.; Theerakittikul, T.; Limsukon, A.; Tajarernmuaug, P.; Phetsuk, N. Acute effects of air pollutants on daily mortality and hospitalizations due to cardiovascular and respiratory diseases. J. Thorac. Dis. 2019, 11, 3070–3083. [Google Scholar] [CrossRef]
- Liang, L.; Cai, Y.; Barratt, B.; Lyu, B.; Chan, Q.; Hansell, A.L.; Xie, W.; Zhang, D.; Kelly, F.J.; Tong, Z. Associations between daily air quality and hospitalisations for acute exacerbation of chronic obstructive pulmonary disease in Beijing, 2013–2017: An ecological analysis. Lancet Planet. Health 2019, 3, e270–e279. [Google Scholar] [CrossRef] [Green Version]
- Szyszkowicz, M.; Kousha, T.; Castner, J.; Dales, R. Air pollution and emergency department visits for respiratory diseases: A multi-city case crossover study. Environ. Res. 2018, 163, 263–269. [Google Scholar] [CrossRef]
- Vinikoor-Imler, L.C.; Owens, E.O.; Nichols, J.L.; Ross, M.; Brown, J.S.; Sacks, J.D. Evaluating Potential Response-Modifying Factors for Associations between Ozone and Health Outcomes: A Weight-of-Evidence Approach. Environ. Health Perspect. 2014, 122, 1166–1176. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.Y.; Chen, C.J. Air pollution and hospital admissions for chronic obstructive pulmonary disease in a subtropical city: Taipei, Taiwan. J. Toxicol. Environ. Health A 2007, 70, 1214–1219. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.M.; Tsai, S.S.; Chang, C.C.; Ho, C.K.; Yang, C.Y. Air pollution and hospital admissions for chronic obstructive pulmonary disease in a tropical city: Kaohsiung, Taiwan. Inhal. Toxicol. 2007, 19, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Fusco, D.; Forastiere, F.; Michelozzi, P.; Spadea, T.; Ostro, B.; Arca, M.; Perucci, C.A. Air pollution and hospital admissions for respiratory conditions in Rome, Italy. Eur. Respir. J. 2001, 17, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J. Air-Pollution and Hospital Admissions for the Elderly in Detroit, Michigan. Am. J. Respir. Crit. Care Med. 1994, 150, 648–655. [Google Scholar] [CrossRef]
- Morgan, G.; Corbett, S.; Wlodarczyk, J. Air pollution and hospital admissions in Sydney, Australia, 1990 to 1994. Am. J. Public Health 1998, 88, 1761–1766. [Google Scholar] [CrossRef]
- Tenias, J.M.; Ballester, F.; Perez-Hoyos, S.; Rivera, M.L. Air pollution and hospital emergency room admissions for chronic obstructive pulmonary disease in Valencia, Spain. Arch. Environ. Health 2002, 57, 41–47. [Google Scholar] [CrossRef]
- Peel, J.L.; Tolbert, P.E.; Klein, M.; Metzger, K.B.; Flanders, W.D.; Todd, K.; Mulholland, J.A.; Ryan, P.B.; Frumkin, H. Ambient air pollution and respiratory emergency department visits. Epidemiology 2005, 16, 164–174. [Google Scholar] [CrossRef]
- Yang, Q.Y.; Chen, Y.; Krewski, D.; Burnett, R.T.; Shi, Y.L.; McGrail, K.M. Effect of short-term exposure to low levels of gaseous pollutants on chronic obstructive pulmonary disease hospitalizations. Environ. Res. 2005, 99, 99–105. [Google Scholar] [CrossRef]
- Halonen, J.I.; Lanki, T.; Tiittanen, P.; Niemi, J.V.; Loh, M.; Pekkanen, J. Ozone and cause-specific cardiorespiratory morbidity and mortality. J. Epidemiol. Community Health 2010, 64, 814–820. [Google Scholar] [CrossRef]
- Anderson, H.R.; Bremner, S.A.; Atkinson, R.W.; Harrison, R.M.; Walters, S. Particulate matter and daily mortality and hospital admissions in the west midlands conurbation of the United Kingdom: Associations with fine and coarse particles, black smoke and sulphate. Occup. Environ. Med. 2001, 58, 504–510. [Google Scholar] [CrossRef] [Green Version]
- Hinwood, A.L.; De Klerk, N.; Rodriguez, C.; Jacoby, P.; Runnion, T.; Rye, P.; Landau, L.; Murray, F.; Feldwick, M.; Spickett, J. The relationship between changes in daily air pollution and hospitalizations in Perth, Australia 1992-1998: A case-crossover study. Int. J. Environ. Health Res. 2006, 16, 27–46. [Google Scholar] [CrossRef] [PubMed]
- Qiu, H.; Yu, I.T.S.; Wang, X.R.; Tian, L.W.; Tse, L.A.; Wong, T.W. Season and humidity dependence of the effects of air pollution on COPD hospitalizations in Hong Kong. Atmos. Environ. 2013, 76, 74–80. [Google Scholar] [CrossRef]
- Schouten, J.P.; Vonk, J.M.; deGraaf, A. Short term effects of air pollution on emergency hospital admissions for respiratory disease: Results of the APHEA project in two major cities in The Netherlands, 1977–1989. J. Epidemiol. Community Health 1996, 50, S22–S29. [Google Scholar] [CrossRef]
- Dab, W.; Medina, S.; Quenel, P.; LeMoullec, Y.; LeTertre, A.; Thelot, B.; Monteil, C.; Lameloise, P.; Pirard, P.; Momas, I.; et al. Short term respiratory health effects of ambient air pollution: Results of the APHEA project in Paris. J. Epidemiol. Community Health 1996, 50, S42–S46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, F.W.S.; Tam, W.; Wong, T.W.; Chan, D.P.S.; Tung, A.H.; Lai, C.K.W.; Hui, D.S.C. Temporal relationship between air pollutants and hospital admissions for chronic obstructive pulmonary disease in Hong Kong. Thorax 2007, 62, 780–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malig, B.J.; Pearson, D.L.; Chang, Y.B.; Broadwin, R.; Basu, R.; Green, R.S.; Ostro, B. A Time-Stratified Case-Crossover Study of Ambient Ozone Exposure and Emergency Department Visits for Specific Respiratory Diagnoses in California (2005–2008). Environ. Health Perspect. 2016, 124, 745–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arbex, M.A.; Conceicao, G.M.D.; Cendon, S.P.; Arbex, F.F.; Lopes, A.C.; Moyses, E.P.; Santiago, S.L.; Saldiva, P.H.N.; Pereira, L.A.A.; Braga, A.L.F. Urban air pollution and chronic obstructive pulmonary disease-related emergency department visits. J. Epidemiol. Community Health 2009, 63, 777–783. [Google Scholar] [CrossRef]
- Ding, P.H.; Wang, G.S.; Guo, Y.L.; Chang, S.C.; Wan, G.H. Urban air pollution and meteorological factors affect emergency department visits of elderly patients with chronic obstructive pulmonary disease in Taiwan. Environ. Pollut. 2017, 224, 751–758. [Google Scholar] [CrossRef]
- Strosnider, H.M.; Chang, H.H.; Darrow, L.A.; Liu, Y.; Vaidyanathan, A.; Strickland, M.J. Age-Specific Associations of Ozone and Fine Particulate Matter with Respiratory Emergency Department Visits in the United States. Am. J. Respir. Crit. Care Med. 2019, 199, 882–890. [Google Scholar] [CrossRef]
- Anderson, H.R.; Spix, C.; Medina, S.; Schouten, J.P.; Castellsague, J.; Rossi, G.; Zmirou, D.; Touloumi, G.; Wojtyniak, B.; Ponka, A.; et al. Air pollution and daily admissions for chronic obstructive pulmonary disease in 6 European cities: Results from the APHEA project. Eur. Respir. J. 1997, 10, 1064–1071. [Google Scholar] [CrossRef] [Green Version]
- Stieb, D.M.; Szyszkowicz, M.; Rowe, B.H.; Leech, J.A. Air pollution and emergency department visits for cardiac and respiratory conditions: A multi-city time-series analysis. Environ. Health 2009, 8, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medina-Ramon, M.; Zanobetti, A.; Schwartz, J. The effect of ozone and PM10 on hospital admissions for pneumonia and chronic obstructive pulmonary disease: A national multicity study. Am. J. Epidemiol. 2006, 163, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Mustafic, H.; Jabre, P.; Caussin, C.; Murad, M.H.; Escolano, S.; Tafflet, M.; Perier, M.C.; Marijon, E.; Vernerey, D.; Empana, J.P.; et al. Main Air Pollutants and Myocardial Infarction A Systematic Review and Meta-analysis. Jama J. Am. Med Assoc. 2012, 307, 713–721. [Google Scholar] [CrossRef]
- Savovic, J.; Weeks, L.; Sterne, J.A.; Turner, L.; Altman, D.G.; Moher, D.; Higgins, J.P. Evaluation of the Cochrane Collaboration’s tool for assessing the risk of bias in randomized trials: Focus groups, online survey, proposed recommendations and their implementation. Syst. Rev. 2014, 3, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.Y.; Wu, S.W.; Pan, L.; Xu, J.H.; Shan, J.; Yang, X.; Dong, W.; Deng, F.R.; Chen, Y.H.; Shima, M.; et al. Short-term effects of various ozone metrics on cardiopulmonary function in chronic obstructive pulmonary disease patients: Results from a panel study in Beijing, China. Environ. Pollut. 2018, 232, 358–366. [Google Scholar] [CrossRef]
- Yin, P.; Chen, R.J.; Wang, L.J.; Meng, X.; Liu, C.; Niu, Y.; Lin, Z.J.; Liu, Y.N.; Liu, J.M.; Qi, J.L.; et al. Ambient Ozone Pollution and Daily Mortality: A Nationwide Study in 272 Chinese Cities. Environ. Health Perspect. 2017, 125, 117006. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Chen, R.; Sera, F.; Vicedo-Cabrera, A.M.; Guo, Y.M.; Tong, S.L.; Coelho, M.S.Z.S.; Saldiva, P.H.N.; Lavigne, E.; Matus, P.; et al. Ambient Particulate Air Pollution and Daily Mortality in 652 Cities. N. Engl. J. Med. 2019, 381, 705–715. [Google Scholar] [CrossRef]
- DeVries, R.; Kriebel, D.; Sama, S. Outdoor Air Pollution and COPD-Related Emergency Department Visits, Hospital Admissions, and Mortality: A Meta-Analysis. Copd J. Chronic Obstr. Pulm. Dis. 2017, 14, 113–121. [Google Scholar] [CrossRef]
- Shah, A.S.V.; Langrish, J.P.; Nair, H.; McAllister, D.A.; Hunter, A.L.; Donaldson, K.; Newby, D.E.; Mills, N.L. Global association of air pollution and heart failure: A systematic review and meta-analysis. Lancet 2013, 382, 1039–1048. [Google Scholar] [CrossRef] [Green Version]
- Viechtbauer, W.; Cheung, M.W.L. Outlier and influence diagnostics for meta-analysis. Res. Synth. Methods 2010, 1, 112–125. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Grp, P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, C.M.; Yang, L.; Thach, T.Q.; Chau, P.Y.K.; Chan, K.P.; Thomas, G.N.; Lam, T.H.; Wong, T.W.; Hedley, A.J.; Peiris, J.S.M. Modification by Influenza on Health Effects of Air Pollution in Hong Kong. Environ. Health Perspect. 2009, 117, 248–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, P.J. Cellular and molecular mechanisms of asthma and COPD. Clin. Sci. 2017, 131, 1541–1558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.S.; Ting, W.U.; Che, F.; Wang, S.; Zhou, Y.H.; Qian, X.P. Comparison between Domestic and International Ambient Air Quality Standards. Res. Environ. Sci. 2010, 23, 253–260. [Google Scholar]
- Samoli, E.; Zanobetti, A.; Schwartz, J.; Atkinson, R.; LeTertre, A.; Schindler, C.; Perez, L.; Cadum, E.; Pekkanen, J.; Paldy, A.; et al. The temporal pattern of mortality responses to ambient ozone in the APHEA project. J. Epidemiol. Community Health 2009, 63, 960–966. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Location | Published | Period | Study Design | Data Source | Population | Definition of Outcome | Influenza |
|---|---|---|---|---|---|---|---|---|
| Malig et al. | USA | 2016 | 2005–2008 | Case crossover | EDVs | All | ICD-9 | Adjust |
| Pothirat et al. | Thailand | 2019 | 2016–2017 | Time series | EDVs & HAs | All | ICD-10 | No |
| Szyszkowicz et al. | Canada | 2018 | 2004–2011 | Case crossover | EDVs | ≥55 years | ICD-10 | Adjust |
| Lee et al. | China | 2007 | 1996–2003 | Case crossover | HAs | All | ICD-9 | No |
| Fusco et al. | Italy | 2001 | 1995–1997 | Time series | HAs | All | ICD-9 | Adjust |
| Schwartz et al. | USA | 1994 | 1986–1989 | Time series | HAs | ≥65 years | ICD-9 | No |
| Morgan et al. | Australia | 1998 | 1990–1994 | Time series | HAs | ≥65 years | ICD-9 | No |
| Tenias et al. | Spain | 2002 | 1994–1995 | Time series | EDVs | ≥14 years | ICD-9 | No |
| Peel et al. | USA | 2005 | 1993–2000 | Time series | EDVs | All | ICD-9 | Adjust |
| Liang et al. | China | 2019 | 2013–2017 | Time series | HAs | ≥18 years | ICD-10 | No |
| Reid et al. | USA | 2019 | 2008 | Time series | EDVs & HAs | All | ICD-9 | No |
| Yang et al. | Canada | 2005 | 1994–1998 | Time series | EDVs | ≥65 years | ICD-9 | No |
| Halonen et al. | Finland | 2010 | 1998–2004 | Time series | EDVs & HAs | ≥65 years | ICD-10 | Adjust |
| Anderson et al. | UK | 2001 | 1994–1996 | Time series | HAs | ≥65 years | ICD-9 | Adjust |
| Qiu et al. | China | 2013 | 1998–2007 | Time series | EDVs | All | ICD-9 | Adjust |
| Dab et al. | France | 1996 | 1987–1992 | Time series | HAs | All | ICD-9 | Adjust |
| Ko et al. | China | 2007 | 2000–2004 | Time series | EDVs | All | ICD-9 | No |
| Hinwood et al. | Australia | 2006 | 1992–1998 | Case crossover | HAs | All | ICD-9 | No |
| Arbex et al. | Brazil | 2009 | 2001–2003 | Time series | EDVs | ≥40 years | ICD-10 | No |
| Ding et al. | China | 2017 | 2000–2013 | Case crossover | EDVs | 65–79 years | ICD-9 | No |
| Yang et al. | China | 2007 | 1996–2003 | Case crossover | HAs | All | ICD-9 | No |
| Schouten et al. | Netherlands | 1996 | 1977–1989 | Time series | EDVs | All | ICD-9 | Adjust |
| Strosnider et al. | USA | 2018 | 2000–2014 | Time series | EDVs | ≥19 years | ICD-9 | No |
| Anderson et al. | Europe | 1997 | 1977–1992 | Time series | EDVs | All | ICD-9 | Adjust |
| Stieb et al. | Canada | 2009 | 1992–2003 | Time series | EDVs | All | ICD-9/ICD-10 | No |
| Medina-Ramon et al. | USA | 2006 | 1986–1999 | Case crossover | HAs | ≥65 years | ICD-9 | No |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, H.; Wang, K.; W. Au, W.; Zhao, W.; Xia, Z.-l. A Systematic Review and Meta-Analysis of Short-Term Ambient Ozone Exposure and COPD Hospitalizations. Int. J. Environ. Res. Public Health 2020, 17, 2130. https://doi.org/10.3390/ijerph17062130
Gao H, Wang K, W. Au W, Zhao W, Xia Z-l. A Systematic Review and Meta-Analysis of Short-Term Ambient Ozone Exposure and COPD Hospitalizations. International Journal of Environmental Research and Public Health. 2020; 17(6):2130. https://doi.org/10.3390/ijerph17062130
Chicago/Turabian StyleGao, Hui, Kan Wang, William W. Au, Wensui Zhao, and Zhao-lin Xia. 2020. "A Systematic Review and Meta-Analysis of Short-Term Ambient Ozone Exposure and COPD Hospitalizations" International Journal of Environmental Research and Public Health 17, no. 6: 2130. https://doi.org/10.3390/ijerph17062130
APA StyleGao, H., Wang, K., W. Au, W., Zhao, W., & Xia, Z. -l. (2020). A Systematic Review and Meta-Analysis of Short-Term Ambient Ozone Exposure and COPD Hospitalizations. International Journal of Environmental Research and Public Health, 17(6), 2130. https://doi.org/10.3390/ijerph17062130