Validation of a Short Questionnaire to Assess Healthcare Professionals’ Perceptions of Asynchronous Telemedicine Services: The Catalan Version of the Health Optimum Telemedicine Acceptance Questionnaire

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Likert Scale
2.2. Translation into Catalan and Data Collection
2.3. Scale Level Descriptive Analysis
2.4. Internal Consistency
2.5. Temporal Stability—Reliability
2.6. Factor Analysis
3. Results
3.1. Test–Retest
3.2. Descriptive Analysis of the Items
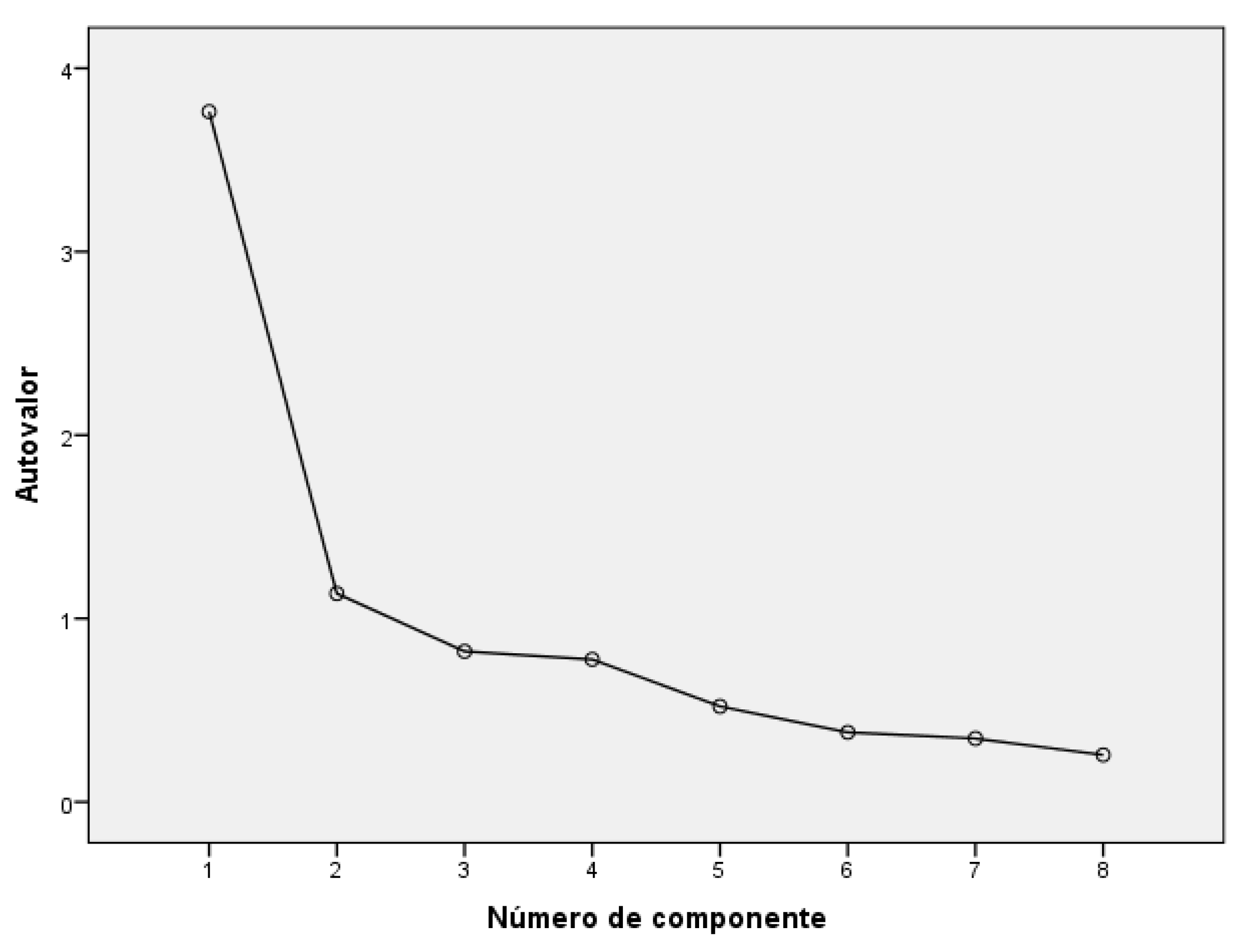
3.3. Exploratory Factor Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Original EU Project Health Optimum Telemedicine Acceptance Questionnaire
- 1. How do you rate the overall quality of the telemedicine consultation?
- Excellent
- Good
- Fair
- Poor
- 2. How would you rate the technical quality of the telemedicine consultation?
- Excellent
- Good
- Fair
- Poor
- 3. How do you rate the quality of care delivered by the telemedicine service when compared to the quality of traditional care?
- Better
- About the same
- Not as good
- Not sure
- 4. Were you comfortable during the telemedicine consultation?
- Yes, very comfortable
- Yes, somewhat comfortable
- No, somewhat uncomfortable
- No, very uncomfortable
- 5. Do you feel that the telemedicine consultation service may influence the health status of your patients?
- Improved health
- No change
- Negative effects on health
- 6. Did you experience technical difficulties that might affect the quality of care delivered by the telemedicine service?
- Not at all
- Sometimes
- Often
- 7. Did you experience organisational or other difficulties that might affect the quality of care delivered by the telemedicine service?
- Not at all
- Sometimes
- Often
- 8. Would you continue to use the telemedicine service?
- Yes, in the same way as the service has be deployed
- Yes, but with improvements
- No
Appendix B. Catalan Version of the Questionnai
- 1. Com qualificaries la qualitat global de les consultes de telemedicina?
- Excel·lent
- Bona
- Normal
- Regular
- Dolenta
- 2. Com qualificaries la qualitat tècnica de les consultes de telemedicina?
- Excel·lent
- Bona
- Normal
- Regular
- Dolenta
- 3. Com qualificaries la qualitat assistencial proporcionada pels serveis de telemedicina comparant-la amb la qualitat de l’atenció habitual?
- Molt millor
- Millor
- Igual
- Pitjor
- Molt pitjor
- 4. Et sents còmode durant les consultes de telemedicina?
- Sí, molt còmode
- Sí, bastant còmode
- Ni còmode, ni incòmode
- No, bastant incòmode
- No, molt incòmode
- 5. Creus que els serveis de telemedicina poden influir en l’estat de salut dels teus pacients?
- Sí, poden millorar la seva salut
- No, no canvien la seva salut
- Sí, poden tenir efectes negatius en la seva salut
- 6. Has experimentat dificultats tècniques que poden haver afectat la qualitat de l’atenció proporcionada pels serveis de telemedicina?
- No, mai
- Alguns cops
- Sovint
- 7. Has experimentat dificultats de tipus organitzatiu o d’altres dificultats que poden haver afectat la qualitat de l’atenció proporcionada pels serveis de telemedicina?
- No
- Algunes vegades
- Sovint
- 8. Continuaràs utilitzant els serveis de telemedicina?
- Sí, igual que ara
- Sí, però amb millores
- No
References
- NICE. National Institute for Health and Care Excellence Evidence Standards Framework for Digital; NICE: London, UK, 2019. [Google Scholar]
- World Health Organization. WHO Guideline: Recommendations on Digital Interventions for Health System Strengthening; WHO: Genev, Switzerland, 2019. [Google Scholar]
- Delgoshaei, B.; Mobinizadeh, M.; Mojdekar, R.; Afzal, E.; Arabloo, J.; Mohamadi, E. Telemedicine: A systematic review of economic evaluations. Med. J. Islamic Repub. Iran 2017, 31, 754–761. [Google Scholar] [CrossRef]
- Langabeer, J.R.; Champagne-Langabeer, T.; Alqusairi, D.; Kim, J.; Jackson, A.; Persse, D.; Gonzalez, M. Cost-benefit analysis of telehealth in pre-hospital care. J. Telemed. Telecare 2017, 23, 747–751. [Google Scholar] [CrossRef] [PubMed]
- Vidal-Alaball, J.; Garcia Domingo, J.L.; Garcia Cuyàs, F.; Mendioroz Peña, J.; Flores Mateo, G.; Deniel Rosanas, J.; Sauch Valmaña, G. A cost savings analysis of asynchronous teledermatology compared to face-to-face dermatology in Catalonia. BMC Health Serv. Res. 2018, 18, 650. [Google Scholar] [CrossRef] [PubMed]
- Van Der Heijden, J.P.; De Keizer, N.F.; Bos, J.D.; Spuls, P.I.; Witkamp, L. Teledermatology applied following patient selection by general practitioners in daily practice improves efficiency and quality of care at lower cost. Br. J. Dermatol. 2011, 165, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Bashshur, R.L.; Shannon, G.W.; Tejasvi, T.; Kvedar, J.; Gates, M. The Empirical Foundations of Teledermatology: A Review of the Research Evidence. Telemed. Health 2015, 21, 10–27. [Google Scholar] [CrossRef] [PubMed]
- Vidal-Alaball, J.; Franch-Parella, J.; Lopez Segui, F.; Garcia Cuyàs, F.; Mendioroz Peña, J. Impact of a Telemedicine Program on the Reduction in the Emission of Atmospheric Pollutants and Journeys by Road. Int. J. Environ. Res. Public Health 2019, 16, 4366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eedy, D.J.; Wootton, R. Teledermatology: A review. Br. J. Dermatol. 2001, 4, 696–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKoy, K.C.; DiGregorio, S.; Stira, L. Asynchronous Teledermatology in an Urban Primary Care Practice. Telemed. J. Health 2004, 10, S-70–S-80. [Google Scholar]
- MacNeill, V.; Sanders, C.; Fitzpatrick, R.; Hendy, J.; Barlow, J.; Knapp, M.; Rogers, A.; Bardsley, M.; Newman, S.P. Experiences of front-line health professionals in the delivery of telehealth: A qualitative study. Br. J. Gen. Pract. 2014, 64, 401–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thijssing, L.; Tensen, E.; Jaspers, M. Patient’s Perspective on Quality of Teleconsultation Services. Stud. Health Technol. Inf. 2016, 228, 132–136. [Google Scholar]
- Orruño Aguado, E.; Gagnon, M.P.; Asua, J.; Abdeljelil, A. Ben Evaluation of teledermatology adoption by health-care professionals using a modified Technology Acceptance Model. J. Telemed. Telecare 2011 2011, 17, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Kidholm, K.; Nielsen, A.D.; Prior, R. REgioNs of Europe WorkINg toGether for HEALTH; European Comission: Brussells, Belgium, 2011. [Google Scholar]
- Momentum Health Optimum. Available online: http://www.telemedicine-momentum.eu/health-optimum-dk/ (accessed on 15 January 2020).
- Asua, J.; Orruño Aguado, E.; Reviriego, E.; Gagnon, M.P. Healthcare professional acceptance of telemonitoring for chronic care patients in primary care. BMC Med. Inform. Decis. Mak. 2012, 12, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gagnon, M.P.; Orruño Aguado, E.; Asua, J.; Abdeljelil, A.B.; Emparanza Knör, J. Using a Modified Technology Acceptance Model to Evaluate Healthcare Professionals’ Adoption of a New Telemonitoring System. Telemed. Health 2012, 18, 54–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamieson, S. Likert Scale, in Encyclopædia Britannica. Available online: https://www.britannica.com/topic/Likert-Scale (accessed on 20 March 2018).
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillemin, F.; Bombardier, C.; Beaton, D. Cross-cultural adaptation of health-related quality of life measures: Literature review and proposed guidelines. J. Clin. Epidemiol. 1993, 46, 1417–1432. [Google Scholar] [CrossRef]
- Argimon-Pallàs, J.M.; Flores Mateo, G.; Jiménez-Villa, J.; Pujol-Ribera, E.; Foz, G.; Bund-Vidiella, M.; Juncosa, S.; Fuentes-Bellido, C.M.; Pérez-Rodríguez, B.; Margalef-Pallarès, F.; et al. Study protocol of psychometric properties of the Spanish translation of a competence test in evidence based practice: The Fresno test. BMC Health Serv. Res. 2009, 9, 37. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.E.; Gandek, B. Methods for testing data quality, scaling assumptions, and reliability: The IQOLA Project approach. J. Clin. Epidemiol. 1998, 51, 945–952. [Google Scholar] [CrossRef]
- Rattray, J.; Jones, M.C. Essential elements of questionnaire design and development. J. Clin. Nurs. 2007, 16, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Argimon-Pallàs, J.M.; Flores Mateo, G.; Jiménez-Villa, J.; Pujol-Ribera, E. Psychometric properties of a test in evidence based practice: The Spanish version of the Fresno test. BMC Med. Educ. 2010, 10, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- TiC Salut i Social. Mapa de Tendencias|TIC Salut Social. Available online: https://ticsalutsocial.cat/es/area/observatorio/ (accessed on 28 February 2020).


{kind=link}
| Descriptive Statistics | Item Parameter Estimates | Reliability | |||||
|---|---|---|---|---|---|---|---|
| Questionnaire’s Items | Mean | Standard Deviation | IDI 1 | Ceiling Effect (%) | Floor Effect (%) | Item-Correlation | Cronbach Alpha |
| 1. Global quality a | 3.51 | 0.85 | 1.24 | 8.3 | 1.4 | 0.79 | 0.79 |
| 2. Technical quality a | 3.47 | 0.87 | 1.13 | 5.6 | 2.8 | 0.75 | 0.80 |
| 3. Clinical quality a | 3.01 | 0.86 | 1.40 | 2.8 | 0.7 | 0.73 | 0.81 |
| 4. Convenience a | 3.67 | 0.89 | 1.36 | 16.0 | 1.4 | 0.75 | 0.80 |
| 5. Health effects b | 2.68 | 0.61 | 0.54 | 75.7 | - | 0.56 | 0.83 |
| 6. Technical difficulties b | 2.03 | 0.56 | 0.59 | - | - | 0.67 | 0.81 |
| 7. Organizational difficulties b | 2.10 | 0.57 | 0.60 | - | - | 0.64 | 0.82 |
| 8. Future use b | 2.53 | 0.51 | 0.51 | - | - | 0.54 | 0.84 |
| Questionnaire Items | Factor 1 | Factor 2 | Communalities (h2) |
|---|---|---|---|
| 1. Global quality a | 0.712 | 0.430 | 0.692 |
| 2. Technical quality a | 0.526 | 0.571 | 0.603 |
| 3. Clinical quality a | 0.785 | 0.234 | 0.671 |
| 4. Convenience a | 0.827 | 0.201 | 0.722 |
| 5. Health effects a | 0.670 | - | 0.450 |
| 6. Technical difficulties b | 0.154 | 0.836 | 0.722 |
| 7. Organizational difficulties b | - | 0.870 | 0.763 |
| 8. Future use b | 0.281 | 0.441 | 0.274 |
| Eigenvalues | 3.76 | 1.14 | |
| Average variance explained (%) | 47.04 | 14.21 | |
| Cronbach’s α reliability | 0.830 | 0.672 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vidal-Alaball, J.; Flores Mateo, G.; Garcia Domingo, J.L.; Marín Gomez, X.; Sauch Valmaña, G.; Ruiz-Comellas, A.; López Seguí, F.; García Cuyàs, F. Validation of a Short Questionnaire to Assess Healthcare Professionals’ Perceptions of Asynchronous Telemedicine Services: The Catalan Version of the Health Optimum Telemedicine Acceptance Questionnaire. Int. J. Environ. Res. Public Health 2020, 17, 2202. https://doi.org/10.3390/ijerph17072202
Vidal-Alaball J, Flores Mateo G, Garcia Domingo JL, Marín Gomez X, Sauch Valmaña G, Ruiz-Comellas A, López Seguí F, García Cuyàs F. Validation of a Short Questionnaire to Assess Healthcare Professionals’ Perceptions of Asynchronous Telemedicine Services: The Catalan Version of the Health Optimum Telemedicine Acceptance Questionnaire. International Journal of Environmental Research and Public Health. 2020; 17(7):2202. https://doi.org/10.3390/ijerph17072202
Chicago/Turabian StyleVidal-Alaball, Josep, Gemma Flores Mateo, Josep Lluís Garcia Domingo, Xavier Marín Gomez, Glòria Sauch Valmaña, Anna Ruiz-Comellas, Francesc López Seguí, and Francesc García Cuyàs. 2020. "Validation of a Short Questionnaire to Assess Healthcare Professionals’ Perceptions of Asynchronous Telemedicine Services: The Catalan Version of the Health Optimum Telemedicine Acceptance Questionnaire" International Journal of Environmental Research and Public Health 17, no. 7: 2202. https://doi.org/10.3390/ijerph17072202
APA StyleVidal-Alaball, J., Flores Mateo, G., Garcia Domingo, J. L., Marín Gomez, X., Sauch Valmaña, G., Ruiz-Comellas, A., López Seguí, F., & García Cuyàs, F. (2020). Validation of a Short Questionnaire to Assess Healthcare Professionals’ Perceptions of Asynchronous Telemedicine Services: The Catalan Version of the Health Optimum Telemedicine Acceptance Questionnaire. International Journal of Environmental Research and Public Health, 17(7), 2202. https://doi.org/10.3390/ijerph17072202