A Mixed-Method Modified Delphi Study toward Identifying Key Elements of Psychotherapy in Iran

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
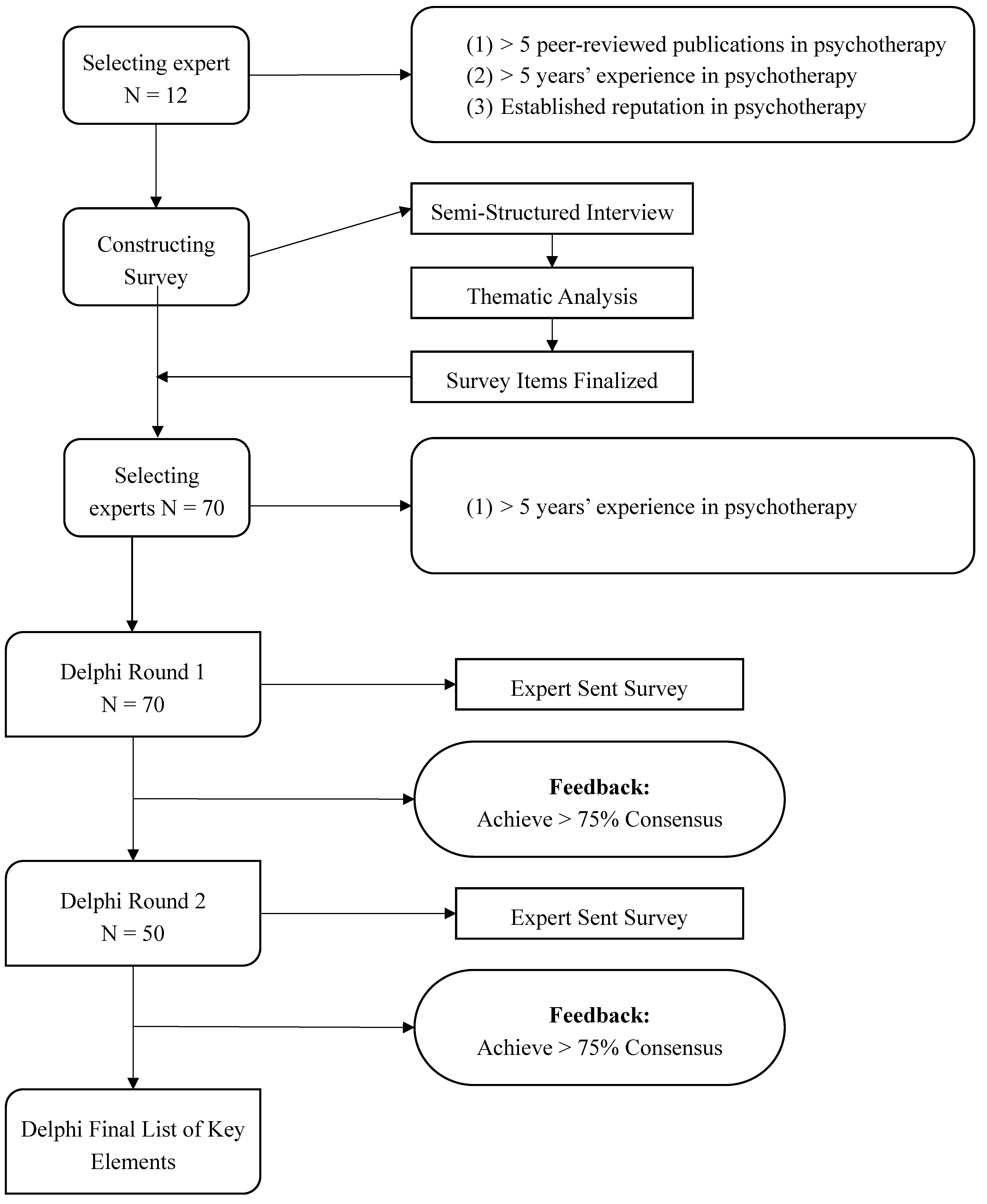
2.1. Study Design
2.2. Expert Identification and Semi-Structured Interviews
2.3. Round 1 Delphi
2.4. Round 2 Delphi
2.5. Data Analysis
2.6. Compliance with Ethical Standards
3. Results
3.1. Semi-Structured Interview
“I think the main problem is education. We need systematic education through which both psychiatry residents and clinical psychologists pass both theoretical and practical psychotherapy education. Supervision should also be emphasized by educators. Our curriculum should be revised”.(p11)
“Unfortunately, we are confronted with psychotherapists with a lack of necessary skills to do psychotherapy. Everyone who wants to do psychotherapy should have a certification of necessary training”.(p3)
“We should know what our societal problems are, and what appropriate approaches exist to solve them. We need to have an assessment from the society and plan accordingly. Our culture should not be overlooked”.(p8)
“Substrate for psychotherapy in Iran is currently not optimal. A substrate for both support and supervision to psychotherapists is necessary. A powerful syndicate should exist. The principles for psychotherapists should be clarified”.(p4)
3.2. Delphi Survey
3.3. Main Areas of Agreement
3.3.1. Education
3.3.2. Psychotherapist Competency
3.3.3. Psychotherapy Interventions
3.3.4. Substrate for Psychotherapy
4. Discussion
4.1. Strengths and Limitations
4.2. Implications and Conclusion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kanfer, F.H.; Reinecker, H.; Schmelzer, D. Sebstmanagement-Therapie (Selfmanangement-Therapy), 5th ed.; Springer: Berlin, Germany, 2011. [Google Scholar]
- Consoli, A.J.; Beutler, L.E.; Bongar, B. Comprehensive Textbook of Psychotherapy, 2nd ed.; Oxford University Press: New York, NY, USA, 2016. [Google Scholar]
- Grawe, K. Psychological Therapy; Hogrefe Publisher: Göttingen, Germany, 2004. [Google Scholar]
- Grawe, K.D.R.; Bernauer, F. Development of Pychotherapy—From the Confession to Profession; Hogrefe: Göttingen, Germany, 1994. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; DSM 5; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Jobst, A.; Brakemeier, E.L.; Buchheim, A.; Caspar, F.; Cuijpers, P.; Ebmeier, K.P.; Falkai, P.; Jan van der Gaag, R.; Gaebel, W.; Herpertz, S.; et al. European Psychiatric Association Guidance on psychotherapy in chronic depression across Europe. Eur. Psychiatry J. Assoc. Eur. Psychiatr. 2016, 33, 18–36. [Google Scholar] [CrossRef] [PubMed]
- Grawe, K. Neuropsychotherapy: How the Neurosciences Inform Effective Psychotherapy; Hogrefe Publisher: Göttingen, Germany, 2007. [Google Scholar]
- Ost, L.-G. The efficacy of Acceptance and Commitment Therapy: An updated systematic review and meta-analysis. Behav. Res. Ther. 2014, 61, 105–121. [Google Scholar] [CrossRef] [PubMed]
- Botha, E.; Gwin, T.; Purpora, C. The effectiveness of mindfulness based programs in reducing stress experienced by nurses in adult hospital settings: A systematic review of quantitative evidence protocol. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Andersson, G.; Carlbring, P. Internet-Assisted Cognitive Behavioral Therapy. Psychiatr. Clin. N. Am. 2017, 40, 689–700. [Google Scholar] [CrossRef]
- Andersson, G.; Rozental, A.; Shafran, R.; Carlbring, P. Long-term effects of internet-supported cognitive behaviour therapy. Expert Rev. Neurother. 2018, 18, 21–28. [Google Scholar] [CrossRef]
- Andersson, G.; Titov, N.; Dear, B.F.; Rozental, A.; Carlbring, P. Internet-delivered psychological treatments: From innovation to implementation. World Psychiatry Off. J. World Psychiatr. Assoc. 2019, 18, 20–28. [Google Scholar] [CrossRef] [Green Version]
- Carlbring, P.; Andersson, G.; Cuijpers, P.; Riper, H.; Hedman-Lagerlöf, E. Internet-based vs. face-to-face cognitive behavior therapy for psychiatric and somatic disorders: An updated systematic review and meta-analysis. Cogn. Behav. Ther. 2018, 47, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Norcross, J.C.; Alford, B.A.; De Michele, J.T. The future of psychotherapy: Delphi data and concluding observations. Psychother. Theory Res. Pract. Train. 1992, 29, 150–158. [Google Scholar] [CrossRef]
- Norcross, J.C.; Hedges, M.; Prochaska, J.O. The face of 2010: A Delphi poll on the future of psychotherapy. Prof. Psychol. Res. Pract. 2002, 33, 316–322. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Norcross, J.C. The future of psychotherapy: A Delphi poll. Prof. Psychol. 1982, 13, 620–627. [Google Scholar] [CrossRef]
- Boulkedid, R.; Abdoul, H.; Loustau, M.; Sibony, O.; Alberti, C. Using and reporting the Delphi method for selecting health care quality indicators: A systematic review. PLoS ONE 2011, 6, e20476. [Google Scholar] [CrossRef] [PubMed]
- Diamond, I.R.; Grant, R.C.; Feldman, B.M.; Pencharz, P.B.; Ling, S.C.; Moore, A.M.; Wales, P.W. Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi studies. J. Clin. Epidemiol. 2014, 67, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Hasson, F.; Keeney, S.; McKenna, H. Research guidelines for the Delphi survey technique. J. Adv. Nurs. 2000, 32, 1008–1015. [Google Scholar] [PubMed] [Green Version]
- McMillan, S.S.; King, M.; Tully, M.P. How to use the nominal group and Delphi techniques. Int. J. Clin. Pharm. 2016, 38, 655–662. [Google Scholar] [CrossRef]
- Norcross, J.C.; Pfund, R.A.; Prochaska, J.O. Psychotherapy in 2022: A Delphi poll on its future. Prof. Psychol. Res. Pract. 2013, 44, 363–370. [Google Scholar] [CrossRef] [Green Version]
- Danaei, G.; Farzadfar, F.; Kelishadi, R.; Rashidian, A.; Rouhani, O.M.; Ahmadnia, S.; Ahmadvand, A.; Arabi, M.; Ardalan, A.; Arhami, M.; et al. Iran in transition. Lancet 2019, 393, 1984–2005. [Google Scholar] [CrossRef]
- Abdoli, N.; Sadeghi Bahmani, D.; Farnia, V.; Alikhani, M.; Golshani, S.; Holsboer-Trachsler, E.; Brand, S. Among substance-abusing traffic offenders, poor sleep and poor general health predict lower driving skills but not slower reaction times. Psychol. Res. Behav. Manag. 2018, 11, 557–566. [Google Scholar] [CrossRef] [Green Version]
- Abdoli, N.; Farnia, V.; Delavar, A.; Dortaj, F.; Esmaeili, A.; Farrokhi, N.; Karami, M.; Shakeri, J.; Holsboer-Trachsler, E.; Brand, S. Mental health status, aggression, and poor driving distinguish traffic offenders from non-offenders but health status predicts driving behavior in both groups. Neuropsychiatr. Dis. Treat. 2015, 11, 2063–2070. [Google Scholar] [CrossRef] [Green Version]
- Abdoli, N.; Farnia, V.; Delavar, A.; Esmaeili, A.; Dortaj, F.; Farrokhi, N.; Karami, M.; Shakeri, J.; Holsboer-Trachsler, E.; Brand, S. Poor mental health status and aggression are associated with poor driving behavior among male traffic offenders. Neuropsychiatr. Dis. Treat. 2015, 11, 2071–2078. [Google Scholar] [CrossRef] [Green Version]
- Norton, P.J.; Gorji, A.; International Scientific Committee of the International Anxiety Congress; Drummond, S.P.A.; Ward, P.B. Trauma, Anxiety, and Depression in Iran: A Report from the 3rd International Anxiety Congress in Iran. Behav. Therapist 2017, 40, 192–194. [Google Scholar]
- Mirsalimi, H. Perspectives of an Iranian psychologist practicing in America. Psychother. Theory Res. Pract. Train. 2010, 47, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Khodayarifard, M.; Rehm, L.; Khodayarifard, S. Psychotherapy in Iran: A case study of cognitive-behavioral family therapy for Mrs. A. J. Clin. Psychol. 2007, 63, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Birashk, B. Counseling and psychotherapy in Iran. In Handbook of Counseling and Psychotherapy in an International Context; Moodley, R.G., Gielen, U.P., Wu, R., Eds.; Routledge: New York, NY, USA, 2013; pp. 361–370. [Google Scholar]
- Mousavi, M.; Alavinezhad, R.; Khazaei, M. Psychotherapy approaches of Iranian psychiatrists and psychologists. J. Fundam. Ment. Health 2018, 20, 202–207. [Google Scholar] [CrossRef]
- Tavakoli, S. The place of psychotherapy in contemporary psychiatry. Iran. J. Psychiatry Behav. Sci. 2014, 8, 1–6. [Google Scholar] [PubMed]
- Khazaie, H.; Rezaie, L.; de Jong, D.M. Dropping out of out patient psychiatric treatment: A preliminary report of a 2-year follow-up of 1500 psychiatric out patients in Kermanshah, Iran. Gen. Hosp. Psychiatry 2013, 35, 314–319. [Google Scholar] [CrossRef]
- Khazaie, H.; Rezaie, L.; Shahdipour, N.; Weaver, P. Exploration of the reasons for dropping out of psychotherapy: A qualitative study. Eval. Prog. Plan. 2016, 56, 23–30. [Google Scholar] [CrossRef]
- Deva, M.P. Bringing changes to Asian mental health. Int. Rev. Psychiatry 2008, 20, 484–487. [Google Scholar] [CrossRef]
- Negri, A.; Andreoli, G.; Belotti, L.; Barazzetti, A.; Martin, H. Psychotherapy trainees’epistemiological assumptions in influencing research-practice integration. Res. Psychother. Psychopathol. Process Outcome 2019, 22, 344–358. [Google Scholar]
- Mullen, P.M. Delphi: Myths and reality. J. Health Organ. Manag. 2003, 17, 37–52. [Google Scholar] [CrossRef]
- Njuangang, S.; Liyanage, C.; Akintoye, A. Application of the Delphi technique in health care maintenance. Int. J. Health Care Qual. Assur. 2017, 30, 737–754. [Google Scholar] [CrossRef]
- Murphy, M.K.; Black, N.A.; Lamping, D.L.; McKee, C.M.; Sanderson, C.F.; Askham, J.; Marteau, T. Consensus development methods, and their use in clinical guideline development. Health Technol. Assess. 1998, 2, i-88. [Google Scholar] [CrossRef] [Green Version]
- Kovach, J.G.; Dubin, W.R.; Combs, C.J. Psychotherapy Training: Residents’ Perceptions and Experiences. Acad. Psychiatry 2015, 39, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Brittlebank, A.; Hermans, M.; Bhugra, D.; Pinto da Costa, M.; Rojnic-Kuzman, M.; Fiorillo, A.; Kurimay, T.; Hanon, C.; Wasserman, D.; van der Gaag, R.J. Training in psychiatry throughout Europe. Eur. Arch. Psychiatry Clin. Neurosci. 2016, 266, 155–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liddell, A.E.; Allan, S.; Goss, K. Therapist competencies necessary for the delivery of compassion-focused therapy: A Delphi study. Psychol. Psychother. 2017, 90, 156–176. [Google Scholar] [CrossRef]
- Epstein, R.M.; Hundert, E.M. Defining and assessing professional competence. JAMA 2002, 287, 226–235. [Google Scholar] [CrossRef]
- Falender, C.A.; Cornish, J.A.E.; Goodyear, R.; Hatcher, R.; Kaslow, N.J.; Leventhal, G.; Shafranske, E.; Sigmon, S.T.; Stoltenberg, C.; Grus, C. Defining competencies in psychology supervision: A consensus statement. J. Clin. Psychol. 2004, 60, 771–785. [Google Scholar] [CrossRef]
- Kaslow, N.J.; Borden, K.A.; Collins, F.L., Jr.; Forrest, L.; Illfelder-Kaye, J.; Nelson, P.D.; Rallo, J.S.; Vasquez, M.J.T.; Willmuth, M.E. Competencies Conference: Future Directions in Education and Credentialing in Professional Psychology. J. Clin. Psychol. 2004, 60, 699–712. [Google Scholar] [CrossRef]
- Jalilian, F.; Mirzaei-Alavijeh, M.; Ahmadpanah, M.; Mostafaei, S.; Kargar, M.; Pirouzeh, R.; Sadeghi Bahmani, D.; Brand, S. Extension of the Theory of Planned Behavior (TPB) to Predict Patterns of Marijuana Use among Young Iranian Adults. Int. J. Environ. Res. Public Health 2020, 17, 1981. [Google Scholar] [CrossRef] [Green Version]
- Khazaie, H.; Behrouz, B.; Chehri, A.; Gerber, M.; Holsboer-Trachsler, E.; Sadeghi Bahmani, D.; Brand, S. Among adolescents, addiction susceptibility and sleep-related dysfunction have a common cognitive-emotional base and predict poor sleep quantity. J. Subst. Use 2019, 24, 426–431. [Google Scholar] [CrossRef]
- Jasbi, M.; Sadeghi Bahmani, D.; Karami, G.; Omidbeygi, M.; Peyravi, M.; Panahi, A.; Mirzaee, J.; Holsboer-Trachsler, E.; Brand, S. Influence of adjuvant mindfulness-based cognitive therapy (MBCT) on symptoms of post-traumatic stress disorder (PTSD) in veterans—Results from a randomized control study. Cogn. Behav. 2018, 47, 431–446. [Google Scholar] [CrossRef]
- Orlinsky, D.; Rønnestad, M.H. How Psychotherapists Develop: A Study of Therapeutic Work and Professional Growth. Psychodyn. Pract. 2010, 16. [Google Scholar] [CrossRef]
- Orlinsky, D.; Rønnestad, M.H.; Ambühl, H.; Willutzki, U.; Botersman, J.-F.; Cierpka, M.; John, D.; Davis, M. Psychotherapists’ assessments of their development at different career levels. Psychother. Theory Res. Pract. Train. 1999, 36, 203–215. [Google Scholar] [CrossRef]
- Rønnestad, M.H.; Orlinsky, D.; Schroder, T.; Skovholt, T.; Willutzki, U. The Professional development of counsellor and psychotherapists: Implications of empirical studies for supervision, training and practice. Couns. Psychother. Res. 2018, 19, 214–230. [Google Scholar] [CrossRef]
- Albani, C.; Blaser, G.; Geyer, M.; Borkenhagen, A.; Brähler, E. Psychotherapie und Versorgungsforschung. Psychotherapeut 2004, 49, 407–414. [Google Scholar] [CrossRef]
- Kordy, H. Psychosoziale Versorgungsforschung. Psychotherapeut 2008, 53, 245–253. [Google Scholar] [CrossRef]


{kind=link}
| Expert Number | Gender | Academic Role | Experience (Years) | Location | Number of Publications | Expert’s Area of Emphasis |
|---|---|---|---|---|---|---|
| 1 | Male | Associate professor of psychiatry | 11 | Tehran | 10 | Cognitive behavior therapy |
| 2 | Male | Assistant professor of clinical psychology | 8 | Tehran | 7 | Child and adolescence psychotherapy |
| 3 | Male | Professor of psychiatry | 20 | Shiraz | 15 | Psychoanalytical psychotherapy |
| 4 | Female | Associate professor of clinical psychology | 10 | Yazd | 9 | Child and adolescence psychotherapy |
| 5 | Female | Professor of psychiatry | 25 | Kerman | 18 | Group psychotherapy |
| 6 | Female | Professor of clinical psychology | 16 | Ahvaz | 18 | Cognitive behavior therapy |
| 7 | Male | Professor of psychiatry | 15 | Sanandaj | 22 | Transfer-based psychotherapy |
| 8 | Male | Associate professor of clinical psychology | 8 | Tehran | 9 | Cognitive behavior therapy |
| 9 | Female | Associate professor of psychiatry | 6 | Tabriz | 10 | Psychoanalytical psychotherapy |
| 10 | Male | Professor of clinical psychology | 13 | Tehran | 12 | Cognitive behavior therapy |
| 11 | Male | Associate professor of psychiatry | 10 | Tehran | 7 | Psychoanalytical psychotherapy |
| 12 | Female | Professor of clinical psychology | 17 | Hamadan | 20 | Psychoanalytical psychotherapy |
| Education Elements | Round 1 Agreement (%) | Round 2 Agreement (%) |
|---|---|---|
| There should be a psychotherapy unit in each psychiatric department. | No Consensus | 92% |
| In each psychiatric group, experienced psychotherapists should be present. | 81.4% | |
| In each psychiatric group, at least one clinical psychologist should be present in the psychotherapy unit. | No Consensus | 92% |
| In the psychotherapy unit, there should be a room suitable for psychotherapy. | 77.1% | |
| In psychiatric departments, each university should communicate with other universities in Iran about psychotherapy. | 84.3% | |
| In each psychiatric group, each university should communicate with universities in other countries about psychotherapy. | No Consensus | 91.9% |
| Inter-university interactions and communication should lead to workshops also with adjunct professors in the field of psychotherapy. | 84.3% | |
| The curriculum in teaching psychotherapy should change in terms of content and time. | No Consensus | 88% |
| In each psychiatric group, a weekly morning report should be devoted to psychotherapy. | No Consensus | 91% |
| Psychiatric residents should be familiar with some of the psychotherapy concepts from the beginning of their courses. | 87.1% | |
| In the second year of residency, residents should attend classes devoted to psychotherapy theory. | 77.2% | |
| During the third year, residents should practice conducting psychotherapy with a qualified professor’s supervision. | 77.1% | |
| Psychiatric residents should learn life skills in their courses. | 80% | |
| Psychiatric residents should experience long-term (analytical) psychotherapy in their trainings, totaling at least two cases. | No Consensus | 89.8% |
| Psychiatry residents should learn short-term psychotherapy (such as CBT). | 75.7% | |
| Membership of a professional body of psychotherapy should be essential for the completion of training for long-term psychotherapy. | No Consensus | 86% |
| Psychiatric residents should be familiar with the research methods in psychotherapy. | No Consensus | 92.8% |
| Clinical psychologists should study at universities affiliated with (and under supervision of) the Ministry of Health. | No Consensus | 83.6% |
| Clinical psychologists should study practical psychotherapy alongside theoretical training during their education. | 82.8% | |
| Clinical psychologists should carry out psychotherapy under supervision with a certain number of cases. | 77.1% | |
| Psychotherapists should assess psychiatry residents and clinical psychologists during the training period and focus on individual characteristics appropriate to different types of psychotherapists. | 81.4% | |
| Psychiatric therapists should guide psychiatry residents and clinical psychology students throughout the course of their education on the basis of individual characteristics and a variety of psychotherapists. | No Consensus | 87.7% |
| Competency Elements | Round 1 Agreement (%) | Round 2 Agreement (%) |
|---|---|---|
| 1. The psychotherapist should be a psychiatrist or clinical psychologist. | No Consensus | 80% |
| 2. The psychotherapist should have a certificate from a valid source (university or institution). | No Consensus | 82% |
| 3. The psychotherapist should undergo psychotherapy himself/herself. | No Consensus | 87.4% |
| 4. The psychotherapist should have the personal qualities necessary for psychotherapy (e.g., ability to communicate, empathy). | 82.8% | |
| 5. Individual psychotherapist features should be approved by several experts in psychotherapy. | No Consensus | 88% |
| 6. The psychotherapist should adhere to the principle of supervision in psychotherapy. | 82.8% | |
| 7. Psychotherapists should adhere to the principle of teamwork in psychotherapy. | 77.1% | |
| 8. The psychotherapist should be a member of a psychotherapy association. | No Consensus | 95.9% |
| 9. The psychotherapist should be aware of changes in the community. | 84.3% | |
| 10. The psychotherapist should be aware of the literature in the community regarding communication. | 85.7% |
| Psychotherapy Intervention Elements | Round 1 Agreement (%) | Round 2 Agreement (%) |
|---|---|---|
| 1. The types of psychotherapy interventions should be based on community-based needs assessments. | 81.4% | |
| 2. Psychotherapists should use short-term psychotherapy interventions. | 81.4% | |
| 3. Psychotherapists should use group psychotherapy interventions. | 82.9% | |
| 4. Psychotherapy interventions should be offered as primary care. | No Consensus | 90% |
| 5. Psychotherapy interventions should be addressed at nursery and primary schools. | No Consensus | 90% |
| 6. Short-term evidence-based psychotherapy packages should be provided. | 80% | |
| 7. The effectiveness of provided psychotherapy packages should be examined in well-controlled studies. | No Consensus | 98% |
| 8. Internet-based methods are not suitable for psychotherapy. | No Consensus | 91.8% |
| 9. Use of new methods such as mindfulness should be considered. | No Consensus | 84% |
| 10. Long-term psychotherapy is suitable for psychologically-minded people. | No Consensus | 88% |
| 11. In psychotherapy interventions, cultural sensitivities should be considered. | 82.2% | |
| 12. Psychotherapy interventions should be structured. | No Consensus | 88% |
| 13. For each psychotherapy session, reports on the content of the meeting should be provided. | 77.6% | |
| 14. Psychotherapy interventions should gradually begin for referrals. | No Consensus | 88% |
| 15. Initial psychotherapy sessions should aim solely to motivate the patient. | No Consensus | 80% |
| 16. Increase in number of psychotherapy sessions per week should be based on consideration of the client’s condition. | 77.1% | |
| 17. Psychotherapy interventions should be used in combination with medication. | 83.8% |
| Elements of Substrate for Psychotherapy | Round 1 Agreement (%) | Round 2 Agreement (%) |
|---|---|---|
| A psychotherapy branch board should exist under the psychiatric board. | No Consensus | 96.4% |
| The board of psychiatrists should develop and apply precise, continuous monitoring criteria for psychotherapy education in psychiatry residency. | 77.1% | |
| A syndicate for psychotherapy should exist in the Ministry of Health. | No Consensus | 97.9% |
| Significant communication between the associations of psychology and psychiatry should exist. | 82.9% | |
| Trade associations should have strict supervision over the license to work in psychotherapy. | 82.9% | |
| Trade associations should require an internship in order to get a license to for work in psychotherapy. | No Consensus | 85.7% |
| Trade associations should closely monitor the observance of principles in the work of psychotherapists. | No Consensus | 89.8% |
| Association guidelines should require psychotherapy centers to submit monthly reports and statistics. | No Consensus | 87.8% |
| Trade associations should have the authority to pursue legal remedies in cases of psychiatric violations. | No Consensus | 89.9% |
| Trade unions should set out the appropriate tariffs for psychotherapy sessions. | 78.6% | |
| Precise and fairly defined concepts of psychotherapeutic intervention should be required for trade associations to accept insurance coverage. | 80% | |
| Trade associations should define and review the cost for psychotherapy services in the Book of Health tariffs. | 82.2% | |
| Universities and trade associations should be committed to providing information and raising the level of information about community-based psychotherapy. | 84.3% | |
| Universities and trade associations should be required to establish a comprehensive database of psychotherapists. | 80% | |
| Universities and trade associations should monitor the distribution of psychotherapists nationwide. | No Consensus | 94.8% |
| The guilds should commit to establishing branches throughout the country. | No Consensus | 94.8% |
| Universities and trade associations should set out guidelines for psychotherapy intervention accepted by insurers. | 77.1% | |
| Universities and guilds should be committed to developing guidelines for referring patients to psychotherapy. | 77.1% | |
| Universities and trade associations should supervise the holding of workshops related to psychotherapy. | 81.5% | |
| Universities and trade associations should provide access to psychotherapy services in government centers at government cost. | 81.5% | |
| Universities and trade associations should monitor and promote the development of psychotherapists of both genders. | 82.8% | |
| Universities and trade associations should monitor and promote the development of child psychotherapists. | 84.3% | |
| Universities and trade associations should provide co-consulting facilities for psychotherapists. | 82.9% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rezaie, L.; Heydari, S.; Paschall, E.; Khazaie, H.; Sadeghi Bahmani, D.; Brand, S. A Mixed-Method Modified Delphi Study toward Identifying Key Elements of Psychotherapy in Iran. Int. J. Environ. Res. Public Health 2020, 17, 2514. https://doi.org/10.3390/ijerph17072514
Rezaie L, Heydari S, Paschall E, Khazaie H, Sadeghi Bahmani D, Brand S. A Mixed-Method Modified Delphi Study toward Identifying Key Elements of Psychotherapy in Iran. International Journal of Environmental Research and Public Health. 2020; 17(7):2514. https://doi.org/10.3390/ijerph17072514
Chicago/Turabian StyleRezaie, Leeba, Shima Heydari, Ethan Paschall, Habibolah Khazaie, Dena Sadeghi Bahmani, and Serge Brand. 2020. "A Mixed-Method Modified Delphi Study toward Identifying Key Elements of Psychotherapy in Iran" International Journal of Environmental Research and Public Health 17, no. 7: 2514. https://doi.org/10.3390/ijerph17072514
APA StyleRezaie, L., Heydari, S., Paschall, E., Khazaie, H., Sadeghi Bahmani, D., & Brand, S. (2020). A Mixed-Method Modified Delphi Study toward Identifying Key Elements of Psychotherapy in Iran. International Journal of Environmental Research and Public Health, 17(7), 2514. https://doi.org/10.3390/ijerph17072514