Quantitative Microbial Risk Assessment of Drinking Water Quality to Predict the Risk of Waterborne Diseases in Primary-School Children

 ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
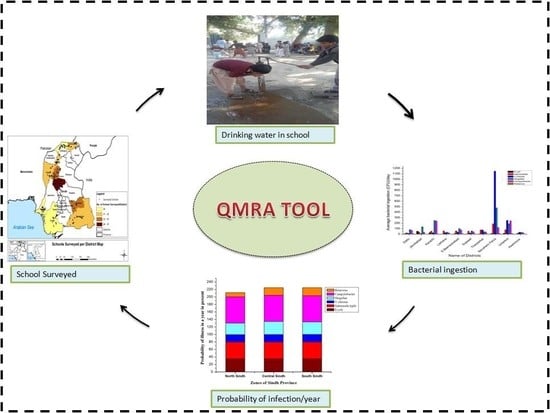
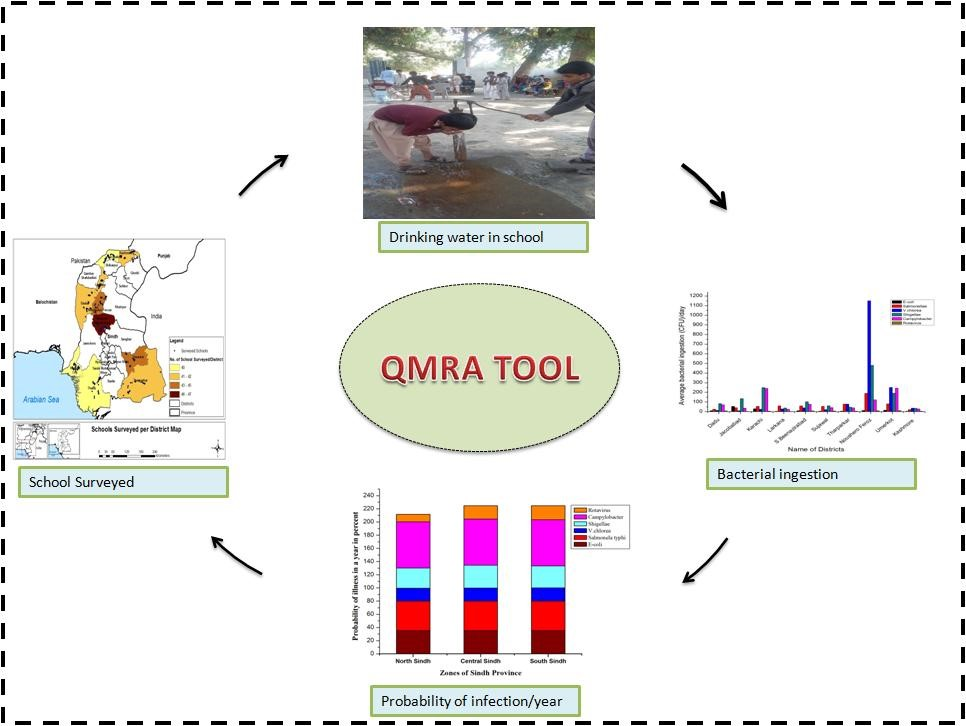
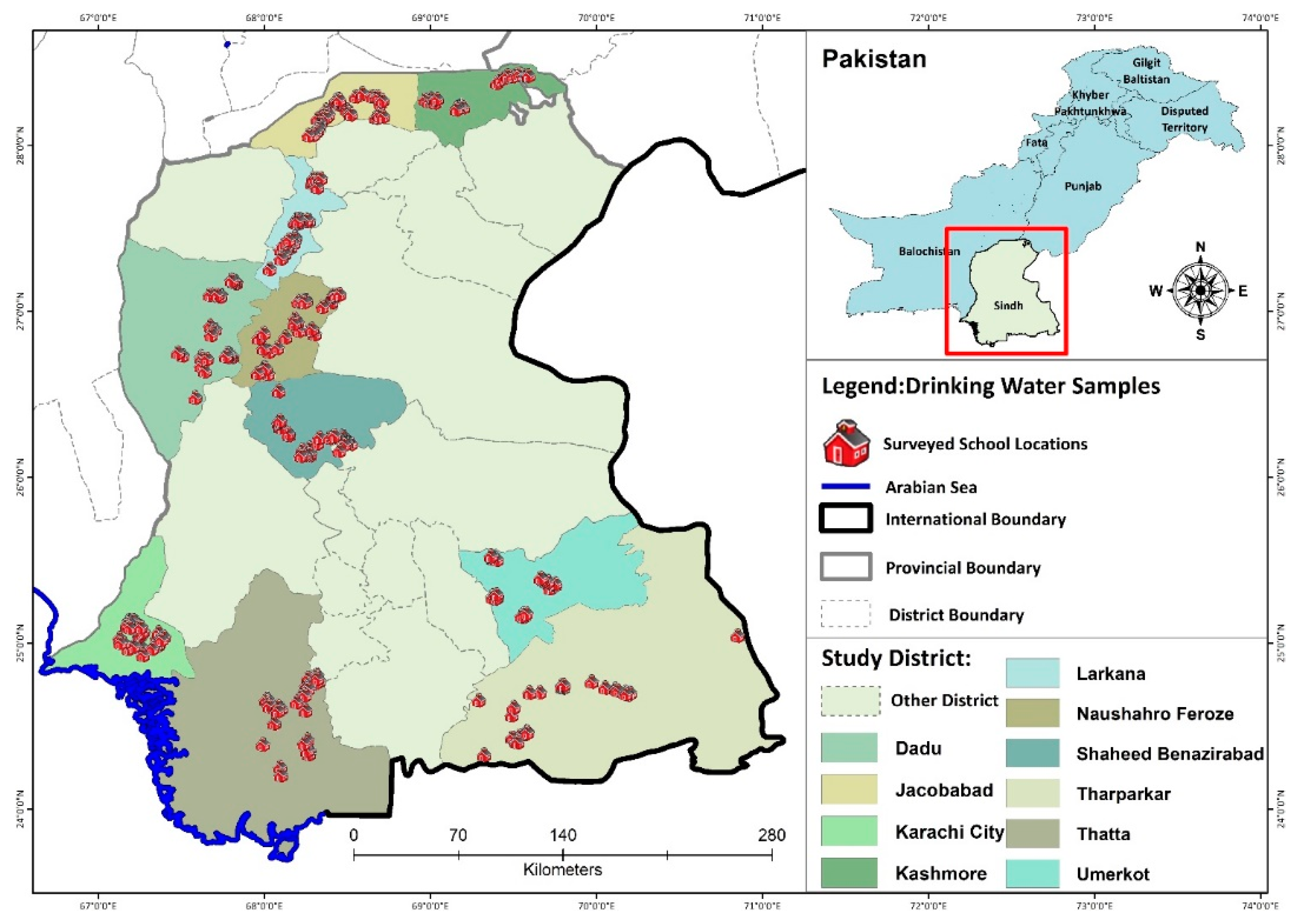
2.1. Study Area (Sindh)
2.2. Sampling
2.3. Microbial Contamination of Drinking-Water Sources
2.4. Hazard Identification
2.5. Isolation and Identification of Bacteria in Drinking Water
2.6. Dose–Response Assessment
2.7. Exposure through Drinking-Water Sources
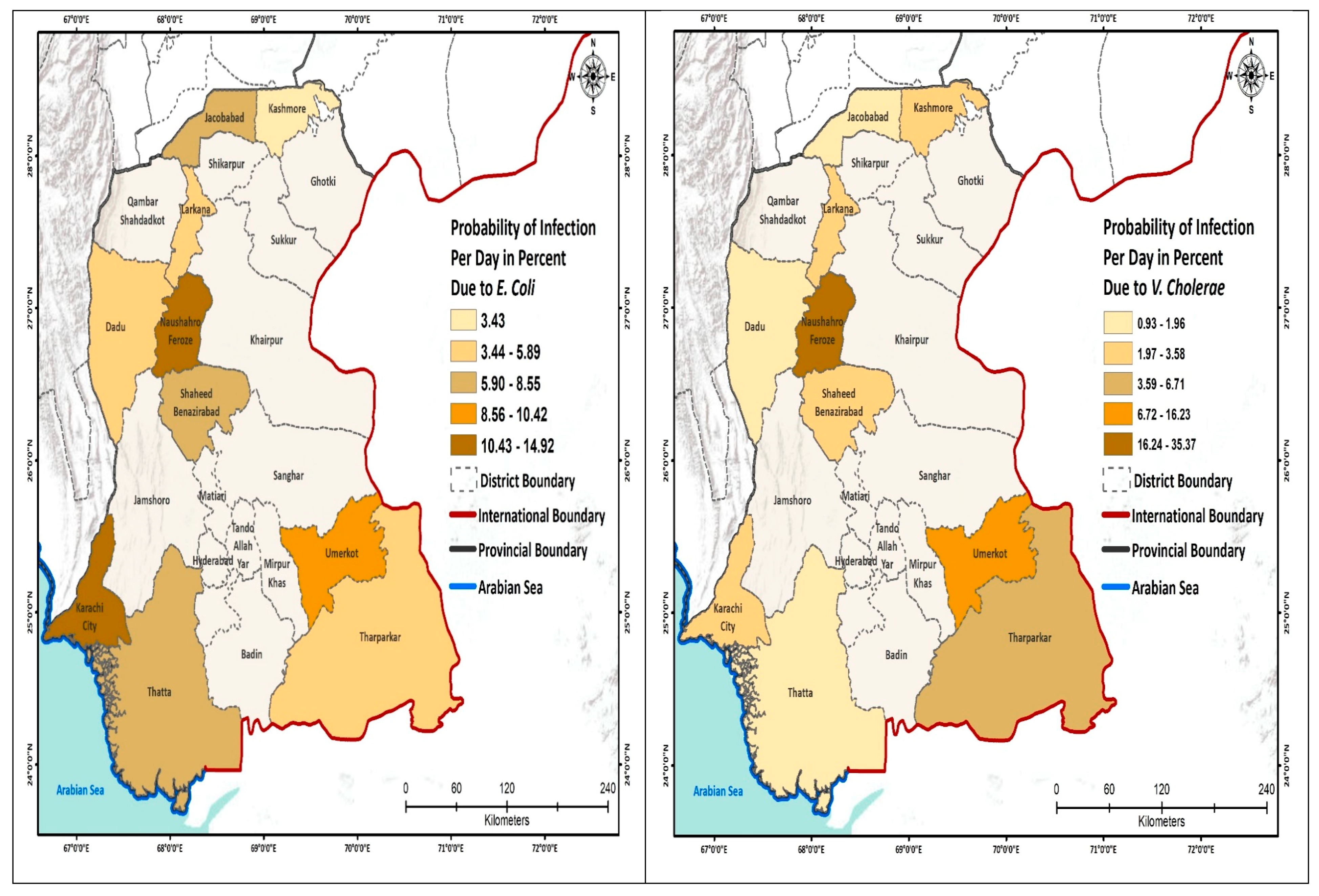
2.8. Risk Characterization
3. Results
3.1. Characterization of Water Samples
3.2. Microbial Quality of Drinking Water
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Districts of Sindh Selected for This Study | Pinf E. Coli/Day | Pinf S. Typhi/Day | Pinf V. Cholera | Pinf Shigella | Pinf Campylobacter | Pinf Rotavirus |
|---|---|---|---|---|---|---|
| Dadu | 0.0372 | 0.0788 | 0.013 | 0.0138 | 0.2861 | 3.2 × 10−4 |
| Jacobabad | 0.0202 | 0.117 | 0.0093 | 0.0221 | 0.2243 | 1.6 × 10−4 |
| Karachi | 0.1033 | 0.143 | 0.0235 | 0.0391 | 0.3969 | 10.9 × 10−4 |
| Larkana | 0.0139 | 0.1519 | 0.0261 | 0.0064 | 0.1881 | 1.1 × 10−4 |
| Nawabshah | 0.0402 | 0.1517 | 0.0358 | 0.0169 | 0.2942 | 3.5 × 10−4 |
| Sujawal | 0.0236 | 0.1455 | 0.0196 | 0.0102 | 0.2399 | 1.9 × 10−4 |
| Tharparkar | 0.0215 | 0.1797 | 0.0671 | 0.0078 | 0.2305 | 1.8 × 10−4 |
| Noushehro Feroze | 0.0472 | 0.2809 | 0.3537 | 0.0694 | 0.3111 | 6.9 × 10−4 |
| Umerkot | 0.0605 | 0.1834 | 0.1623 | 0.0305 | 0.3377 | 5.6 × 10−4 |
| Kashmore | 0.0155 | 0.0678 | 0.0343 | 0.006 | 0.1986 | 1.2 × 10−4 |
References
- WHO. Annual Report WHO/UNICEF Joint Monitoring Programme (JMP) for Water Supply and Sanitation; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Sauer, M.; Smith, S.; Clemens, B. Does it Pay to Invest in Potable Water in the Developing World? Relationships Between External Financing and Economic Development in Sustainable Community-Run Integrated Projects. J. Int. Dev. 2016, 28, 233–242. [Google Scholar] [CrossRef]
- Cairncross, S.; Feachem, R. Environmental Health Engineering in the Tropics: Water, Sanitation and Disease Control; Routledge: Abington, UK, 2018. [Google Scholar]
- Nawaz, S.; Ali, Y. Factors affecting the performance of water treatment plants in Pakistan. Water Conserv. Sci. Eng. 2018, 3, 191–203. [Google Scholar] [CrossRef]
- JMP. Progress on Drinking Water, Sanitation and Hygiene: 2017 Update and SDG Baselines; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- UNICEF. Child Survival Fact Sheet: Water and Sanitation; UNICEF: New York, NY, USA, 2018. [Google Scholar]
- Rahman, A.E.; Moinuddin, M.; Molla, M.; Worku, A.; Hurt, L.; Kirkwood, B.; Mohan, S.B.; Mazumder, S.; Bhutta, Z.; Raza, F. Childhood diarrhoeal deaths in seven low-and middle-income countries. Bull. World Health Organ. 2014, 92, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, T.; Pervez, A.; Mehtab, M.; Sherwani, S.K. Assessment of drinking water quality and its potential health impacts in academic institutions of Abbottabad (Pakistan). Desalin. Water Treat. 2015, 54, 1819–1828. [Google Scholar] [CrossRef]
- UNICEF. Water, Sanitation and Hygiene (WASH) in Public Sector Schools Strategic Plan for Sindh; UNICEF: New York, NY, USA, 2016; pp. 3–524. [Google Scholar]
- Zahid, J. Impact of Clean Drinking Water and Sanitation on Water Borne Diseases in Pakistan; Sustainable Development Policy Institute: Islamabad, Pakistan, 2018. [Google Scholar]
- WaterAid. The Water Gap—The State of the World’s Water 2018; WaterAid: London, UK, 2018. [Google Scholar]
- Amin, R.; Zaidi, M.B.; Bashir, S.; Khanani, R.; Nawaz, R.; Ali, S.; Khan, S. Microbial contamination levels in the drinking water and associated health risk in Karachi, Pakistan. J. Water Sanit. Hyg. Dev. 2019, 9, 319–328. [Google Scholar] [CrossRef]
- Azizullah, A.; Khattak, M.N.K.; Richter, P.; Häder, D.-P. Water pollution in Pakistan and its impact on public health—A review. Environ. Int. 2011, 37, 479–497. [Google Scholar] [CrossRef]
- Bosan, A.; Qureshi, H.; Bile, K.M.; Ahmad, I.; Hafiz, R. A review of hepatitis viral infections in Pakistan. JPMA J. Pak. Med. Assoc. 2010, 60, 1045. [Google Scholar]
- Daud, M.; Nafees, M.; Ali, S.; Rizwan, M.; Bajwa, R.A.; Shakoor, M.B.; Arshad, M.U.; Chatha, S.A.S.; Deeba, F.; Murad, W. Drinking water quality status and contamination in Pakistan. BioMed. Res. Int. 2017, 2017, 7908183. [Google Scholar] [CrossRef]
- Rind, A.; Mastoi, A.; Mastoi, G.; Almani, K.; Hullio, A.; Somroo, A.; Mallah, S. Quality examination of drinking water: A cause study of water filtration plants installed at Hyderabad city, Sindh, Pakistan. J. Biodivers. Environ. Sci. 2014, 4, 289–295. [Google Scholar]
- Carducci, A.; Donzelli, G.; Cioni, L.; Federigi, I.; Lombardi, R.; Verani, M. Quantitative microbial risk assessment for workers exposed to bioaerosol in wastewater treatment plants aimed at the choice and setup of safety measures. Int. J. Environ. Res. Public Health 2018, 15, 1490. [Google Scholar] [CrossRef] [Green Version]
- Carducci, A.; Donzelli, G.; Cioni, L.; Verani, M. Quantitative microbial risk assessment in occupational settings applied to the airborne human adenovirus infection. Int. J. Environ. Res. Public Health 2016, 13, 733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owens, C.E.; Angles, M.L.; Cox, P.T.; Byleveld, P.M.; Osborne, N.J.; Rahman, M.B. Implementation of quantitative microbial risk assessment (QMRA) for public drinking water supplies: Systematic review. Water Res. 2020, 174, 115614. [Google Scholar] [CrossRef] [PubMed]
- Kundu, A.; Wuertz, S.; Smith, W.A. Quantitative microbial risk assessment to estimate the risk of diarrheal diseases from fresh produce consumption in India. Food Microbiol. 2018, 75, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Federigi, I.; Verani, M.; Donzelli, G.; Cioni, L.; Carducci, A. The application of quantitative microbial risk assessment to natural recreational waters: A review. Mar. Pollut. Bull. 2019, 144, 334–350. [Google Scholar] [CrossRef] [PubMed]
- Verani, M.; Federigi, I.; Donzelli, G.; Cioni, L.; Carducci, A. Human adenoviruses as waterborne index pathogens and their use for Quantitative Microbial Risk Assessment. Sci. Total Environ. 2019, 651, 1469–1475. [Google Scholar] [CrossRef] [PubMed]
- Rasheduzzaman, M.; Singh, R.; Haas, C.N.; Tolofari, D.; Yassaghi, H.; Hamilton, K.A.; Yang, Z.; Gurian, P.L. Reverse QMRA as a Decision Support Tool: Setting Acceptable Concentration Limits for Pseudomonas aeruginosa and Naegleria fowleri. Water Conserv. Sci. Eng. 2019, 11, 1850. [Google Scholar] [CrossRef] [Green Version]
- Memon, M.; Soomro, M.S.; Akhtar, M.S.; Memon, K.S. Drinking water quality assessment in Southern Sindh (Pakistan). Environ. Monit. Assess. 2011, 177, 39–50. [Google Scholar] [CrossRef]
- Sindh, G.o.; Department, S.E.a.L. Government of Sindh; Pakistan: Sindh, Pakistan, 2019. Available online: http://www.sindheducation.gov.pk./ (accessed on 5 April 2020).
- Adams, J.; Bartram, J.; Chartier, Y.; Sims, J. Water, Sanitation and Hygiene Standards for Schools in Low-Cost Settings; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Garn, J.V.; Trinies, V.; Toubkiss, J.; Freeman, M.C. The role of adherence on the impact of a school-based water, sanitation, and hygiene intervention in Mali. Am. J. Trop. Med. Hyg. 2017, 96, 984–993. [Google Scholar] [CrossRef] [Green Version]
- Haas, C.N.; Rose, J.B.; Gerba, C.P. Quantitative Microbial Risk Assessment; John Wiley & Sons: Hoboken, NJ, USA, 1999. [Google Scholar]
- Machdar, E.; Van Der Steen, N.; Raschid-Sally, L.; Lens, P. Application of quantitative microbial risk assessment to analyze the public health risk from poor drinking water quality in a low income area in Accra, Ghana. Sci. Total Environ. 2013, 449, 134–142. [Google Scholar] [CrossRef]
- Howard, G.; Pedley, S.; Tibatemwa, S. Quantitative microbial risk assessment to estimate health risks attributable to water supply: Can the technique be applied in developing countries with limited data? J. Water Health 2006, 4, 49–65. [Google Scholar] [CrossRef]
- Mara, D.; Hamilton, A.J.; Sleigh, A.; Karavarsamis, N.; Seidu, R. Tools for risk analysis: Updating the 2006 WHO guidelines. In Wastewater Irrigation and Health; Routledge: Abington, UK, 2009; pp. 115–126. [Google Scholar]
- Westrell, T. Microbial Risk Assessment and Its Implications for Risk Management in Urban Water Systems; Linköping University Electronic Press: Linköping, Switzerland, 2004. [Google Scholar]
- Abia, A.L.K.; Ubomba-Jaswa, E.; Genthe, B.; Momba, M.N.B. Quantitative microbial risk assessment (QMRA) shows increased public health risk associated with exposure to river water under conditions of riverbed sediment resuspension. Sci. Total Environ. 2016, 566, 1143–1151. [Google Scholar] [CrossRef] [PubMed]
- UNICEF; World Health Organization. Core Questions and Indicators for Monitoring WASH in Schools in the Sustainable Development Goals; WHO: Geneva, Switzerland; UNICEF: New York, NY, USA, 2016. [Google Scholar]
- Sarfraz, M.; Sultana, N.; Tariq, M.I. Assessment of groundwater quality and associated health risks in rural areas of sindh (Pakistan). Studia Univ. Babes-Bolyai Chem. 2018, 63. [Google Scholar] [CrossRef]
- Studies, N.I.o.P.; Islamabad, P. Pakistan Demographic and Health Survey 2017-18; National Institute of Population Studies (NIPS) [Pakistan]: Islamabad, Pakistan; ICF: Fairfax, VA, USA, January 2019; pp. 1–573. [Google Scholar]
- Klemm, E.; Shakoor, S.; Page, A.; Qamar, F.; Judge, K.; Saeed, D.; Wong, V.; Dallman, T.; Nair, S.; Baker, S. Emergence of an extensively drug-resistant Salmonella enterica serovar Typhi clone harboring a promiscuous plasmid encoding resistance to fluoroquinolones and thirdgeneration cephalosporins. mBio 2018, 9, e00105-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Emergencies Preparedness, Response; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Jasper, C.L.T.; Bartram, J. Water and sanitation in schools: A systematic review of the health and educational outcomes. Int. J. Environ. Res. Public Health 2012, 9, 2772–2787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pande, G.; Kwesiga, B.; Bwire, G.; Kalyebi, P.; Riolexus, A.; Matovu, J.K.; Makumbi, F.; Mugerwa, S.; Musinguzi, J.; Wanyenze, R.K. Cholera outbreak caused by drinking contaminated water from a lakeshore water-collection site, Kasese District, south-western Uganda, June–July 2015. PLoS ONE 2018, 13, e0198431. [Google Scholar] [CrossRef]
- Chanachai, K.; Pittayawonganon, C.; Areechokchai, D.; Suchatsoonthorn, C.; Pokawattana, L.; Jiraphongsa, C. A food borne outbreak of gastroenteritis due to Shigella and possibly Salmonella in a school. Southeast Asian J. Trop. Med. Public Health 2008, 39, 297. [Google Scholar]
- Schaetti, C.; Khatib, A.M.; Ali, S.M.; Hutubessy, R.; Chaignat, C.-L.; Weiss, M.G. Social and cultural features of cholera and shigellosis in peri-urban and rural communities of Zanzibar. Infect. Dis. 2010, 10, 339. [Google Scholar] [CrossRef] [Green Version]
- Habib, M.I.; Kazi, S.G.; Khan, K.M.A.; Zia, N. Rota virus diarrhea in hospitalized children. J. Coll. Physicians Surg. Pak. 2014, 24, 114. [Google Scholar]
- Miles, M.G.; Lewis, K.D.; Kang, G.; Parashar, U.D.; Steele, A.D. A systematic review of rotavirus strain diversity in India, Bangladesh, and Pakistan. Vaccine 2012, 30, A131–A139. [Google Scholar] [CrossRef]
- Pitkänen, T. Review of Campylobacter spp. in drinking and environmental waters. J. Microbiol. Methods 2013, 95, 39–47. [Google Scholar] [CrossRef]
- Bresee, S.; Caruso, B.; Sales, J.; Lupele, J.; Freeman, M. ‘A child is also a teacher’: Exploring the potential for children as change agents in the context of a school-based WASH intervention in rural Eastern Zambia. Health Educ. Res. 2016, 31, 521–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katukiza, A.; Ronteltap, M.; Van Der Steen, P.; Foppen, J.; Lens, P. Quantification of microbial risks to human health caused by waterborne viruses and bacteria in an urban slum. J. Appl. Microbiol. 2014, 116, 447–463. [Google Scholar] [CrossRef] [PubMed]
- Gadgil, A. Drinking water in developing countries. Annu. Rev. Energy environ. 1998, 23, 253–286. [Google Scholar] [CrossRef] [Green Version]
- Siddiqui, N.; Gorard, S. Comparing government and private schools in Pakistan: The way forward for universal education. Int. J. Educ. Res. 2017, 82, 159–169. [Google Scholar] [CrossRef] [Green Version]




| Location | Districts | N Primary Schools | Sources of Drinking Water |
|---|---|---|---|
| North Sindh | Larkana | 42 | Ground (88%), Surface (12%) |
| Jacobabad | 40 | Ground (67%), Surface (33%) | |
| Kashmore | 42 | Ground (83%), Surface (16%) | |
| Central Sindh | S. Benazirabad | 47 | Ground (87%), Surface (13%) |
| Dadu | 42 | Ground (83%), Surface (17) | |
| Naushahro Feroze | 45 | Ground (94%), Surface (6%) | |
| South Sindh | Tharparkar | 42 | Surface (55%), Ground (45%) |
| Sujawal | 40 | Surface (85%), Ground (15%) | |
| Karachi | 40 | Surface (98%) Ground (2%) | |
| Umerkot | 45 | Ground (58%), Surface (42%) | |
| Total samples | 425 | ||
| Organisms | Parameters | Type of Model | Reference |
|---|---|---|---|
| Escherichia coli | α = 0.2099 N50 = 1120 PDi = 0.35 | β-Poisson model | [28,29,30,32] |
| Campylobacter * | α = 0.145 N50 = 896 PDi = 0.7 | β-Poisson model | [29,32] |
| Rotavirus * | α = 0.2531 N50 = 6.17 PDi = 0.5 | β-Poisson model | [28,29] |
| Salmonella spp. | α = 0.21 β ** = 49.78 N50 = 1.11 × 106 PDi = 0.45 | β-Poisson model | [33] |
| Shigella spp. | α = 0.265 β ** =1480 PDi = 0.35 | β-Poisson model | [33] |
| Vibrio cholerae | α = 0.250 β ** = 243 PDi = 0.2 | β-Poisson model | [33] |
| Districts | N Schools | % with Contaminated Water Sources | |||
|---|---|---|---|---|---|
| E. Coli | Salmonellae spp. | V. Cholerae | Shigella | ||
| Dadu | 42 | 50.0 | 47.6 | 31.0 | 54.8 |
| Jacobabad | 40 | 42.5 | 37.5 | 22.5 | 67.5 |
| Karachi | 40 | 60.0 | 42.5 | 27.5 | 90.0 |
| Larkana | 42 | 21.4 | 69.0 | 57.1 | 45.2 |
| S. Benazirabad | 47 | 57.4 | 55.3 | 55.3 | 76.6 |
| Sujawal | 40 | 57.5 | 47.5 | 30.0 | 57.5 |
| Tharparkar | 42 | 23.8 | 57.1 | 59.5 | 52.4 |
| Naushahro Feroze | 45 | 64.4 | 64.4 | 93.3 | 82.2 |
| Umerkot | 45 | 68.9 | 64.4 | 60.0 | 55.6 |
| Kashmore | 42 | 45.2 | 50.0 | 57.1 | 52.4 |
| Overall | 425 | 49.4 | 53.9 | 50.1 | 63.5 |
| Districts | Average Bacterial Ingestion Colony Forming Unit (CFU)/Day | |||||
|---|---|---|---|---|---|---|
| E. Coli | Salmonella spp. | V. Cholerae | Shigella | Campylobacter | Rotavirus | |
| Dadu | 0.8476 × 101 | 2.381 × 101 | 1.3095 × 101 | 8.2619 × 101 | 6.9928 × 101 | 10.5 × 10−4 |
| Jacobabad | 0.4375 × 101 | 4.025 × 101 | 0.925 × 101 | 1.3475 × 102 | 3.6135 × 101 | 54.7 × 10−5 |
| Karachi | 2.916 × 101 | 5.4 × 101 | 2.425 × 101 | 2.49.5 × 102 | 2.405 × 102 | 36.01 × 10−4 |
| Larkana | 0.295 × 101 | 5.9286 × 101 | 2.7143 × 101 | 3.7381 × 101 | 2.4357 × 101 | 36.9 × 10−5 |
| S. Benazirabad | 0.925 × 101 | 5.9167 × 101 | 3.8125 × 101 | 1.01667 × 102 | 7.631 × 101 | 11.56 ×10−4 |
| Sujawal | 0.518 × 101 | 5.55 × 101 | 2.0 × 101 | 6.025 × 101 | 4.273 × 101 | 64.7 × 10−5 |
| Tharparkar | 0.468 × 101 | 7.8095 × 101 | 7.7857 × 101 | 4.619 × 101 | 3.868 × 101 | 58.5 × 10−5 |
| Naushahro Feroze | 1.109 × 101 | 1.89556 × 102 | 1.149556 × 103 | 4.80 × 102 | 9.154 × 101 | 13.8 × 10−5 |
| Umerkot | 1.484 × 101 | 8.0889 × 101 | 2.5044 × 102 | 1.9022 × 102 | 1.222 × 102 | 18.5 × 10−4 |
| Kashmore | 0.331 × 101 | 1.976 × 101 | 3.6429 × 101 | 3.5238 × 101 | 2.734 × 101 | 41.4 × 10−5 |
| District | Probability of Infection per Year (%) | Probability of Illness per Year (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| E. Coli | Salmonella spp. | V. Cholerae | Shigella | Campylobacter | Rotavirus | E. Coli | Salmonella spp. | V. Cholerae | Shigella | Campylobacter | Rotavirus | |
| Dadu | 100.0 | 100.0 | 97.3 | 97.8 | 100.0 | 1.61 | 35.0 | 45.0 | 19.5 | 34.2 | 70.0 | 8.0 |
| Jacobabad | 99.6 | 100.0 | 92.3 | 99.8 | 100.0 | 8.6 | 34.9 | 45.0 | 18.5 | 34.9 | 70.0 | 4.3 |
| Karachi | 100.0 | 100.0 | 99.9 | 100.0 | 100.0 | 45.1 | 35.0 | 45.0 | 20.0 | 35.0 | 70.0 | 22.6. |
| Larkana | 97.9 | 100.0 | 99.9 | 82.9 | 100.0 | 5.9 | 34.3 | 45.0 | 20.0 | 29.0 | 70.0 | 3.0 |
| S. Benazirabad | 100.0 | 100.0 | 100.0 | 99.1 | 100.0 | 17.4 | 35.0 | 45.0 | 20.0 | 34.7 | 70.0 | 8.7 |
| Sujawal | 99.9 | 100.0 | 99.6 | 94.0 | 100.0 | 10.1 | 35.0 | 45.0 | 19.9 | 32.9 | 70.0 | 5.1 |
| Tharparkar | 99.8 | 100.0 | 100.0 | 88.4 | 100.0 | 92.0 | 34.9 | 45.0 | 20.0 | 31.0 | 70.0 | 4.6 |
| Naushahro Feroze | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 20.5 | 35.0 | 45.0 | 20.0 | 35.0 | 70.0 | 10.2 |
| Umerkot | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 26.4 | 35.0 | 45.0 | 20.0 | 35.0 | 70.0 | 13.0 |
| Kashmore | 98.7 | 100.0 | 100.0 | 80.9 | 100.0 | 6.6 | 34.5 | 45.0 | 20.0 | 28.3 | 70.0 | 3.3 |
| Overall | 99.6 | 100.0 | 98.9 | 94.3 | 100.0 | 23.4 | 34.8 | 45.0 | 19.8 | 33.0 | 70.0 | 6.7 |
| E. Coli | V. Cholerae | Shigella | Campylobacter | Rotavirus | Salmonella spp. | |
|---|---|---|---|---|---|---|
| E. coli | 1 | |||||
| V. Cholerae | 0.118 | 1 | ||||
| Shigella | 0.525 | 0.878 * | 1 | |||
| Campylobacter | 1.000 * | 0.118 | 0.525 | 1 | ||
| Rotavirus | 1.000 * | 0.118 | 0.525 | 1.000 * | 1 | |
| Salmonella spp. | 0.156 | 0.942 * | 0.833 ** | 0.156 | 0.156 | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, J.; Wong, L.P.; Chua, Y.P.; Channa, N.; Mahar, R.B.; Yasmin, A.; VanDerslice, J.A.; Garn, J.V. Quantitative Microbial Risk Assessment of Drinking Water Quality to Predict the Risk of Waterborne Diseases in Primary-School Children. Int. J. Environ. Res. Public Health 2020, 17, 2774. https://doi.org/10.3390/ijerph17082774
Ahmed J, Wong LP, Chua YP, Channa N, Mahar RB, Yasmin A, VanDerslice JA, Garn JV. Quantitative Microbial Risk Assessment of Drinking Water Quality to Predict the Risk of Waterborne Diseases in Primary-School Children. International Journal of Environmental Research and Public Health. 2020; 17(8):2774. https://doi.org/10.3390/ijerph17082774
Chicago/Turabian StyleAhmed, Jamil, Li Ping Wong, Yan Piaw Chua, Najeebullah Channa, Rasool Bux Mahar, Aneela Yasmin, James A. VanDerslice, and Joshua V. Garn. 2020. "Quantitative Microbial Risk Assessment of Drinking Water Quality to Predict the Risk of Waterborne Diseases in Primary-School Children" International Journal of Environmental Research and Public Health 17, no. 8: 2774. https://doi.org/10.3390/ijerph17082774
APA StyleAhmed, J., Wong, L. P., Chua, Y. P., Channa, N., Mahar, R. B., Yasmin, A., VanDerslice, J. A., & Garn, J. V. (2020). Quantitative Microbial Risk Assessment of Drinking Water Quality to Predict the Risk of Waterborne Diseases in Primary-School Children. International Journal of Environmental Research and Public Health, 17(8), 2774. https://doi.org/10.3390/ijerph17082774