Diphtheria-Tetanus-Polio, Measles-Mumps-Rubella, and Hepatitis B Vaccination Coverage and Associated Factors among Homeless Children in the Paris Region in 2013: Results from the ENFAMS Survey

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
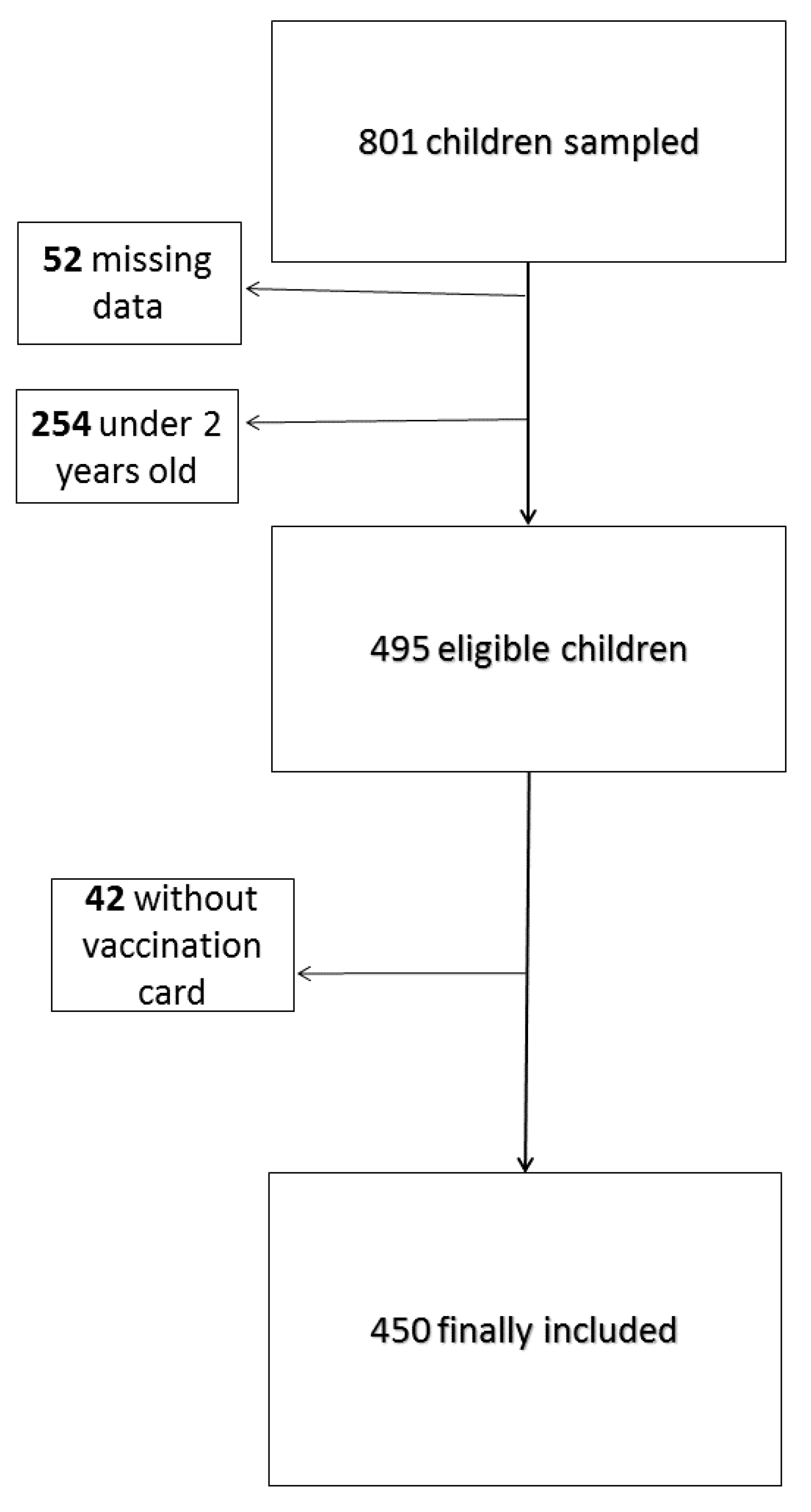
2.1. Study Population
2.2. Measures
2.2.1. Insufficient Vaccination Coverage
2.2.2. Covariates: Sociodemographic Characteristics
2.3. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics of the Population
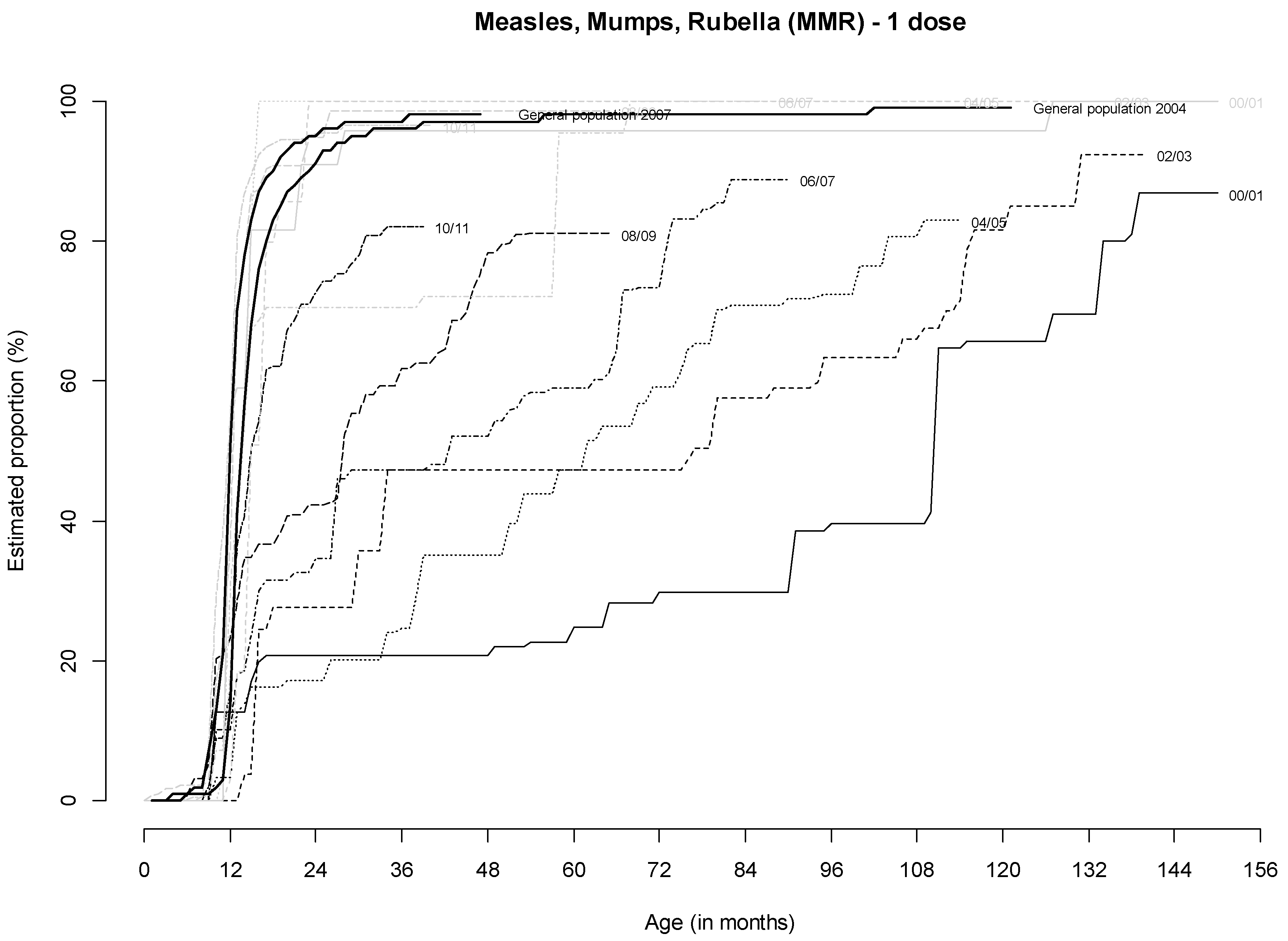
3.2. Vaccination Coverage of Homeless Children
3.3. Factors Associated with Insufficient Vaccination Coverage for DT-IPV, MMR and HepB
3.3.1. Children Born in France
3.3.2. Children Born Outside France
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bassuk, E.L.; Rubin, L.; Lauriat, A.S. Characteristics of sheltered homeless families. Am. J. Public Health 1986, 76, 1097–1101. Available online: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1646563&tool=pmcentrez&rendertype=abstract (accessed on 7 December 2015). [CrossRef] [Green Version]
- FEANTSA. Changing Faces: Homelessness Among Children, Families and Young People. Homeless Eur. 2010; (Autumn/Winter). Available online: https://www.feantsa.org/download/homeless_in_europe_autumn2010_en_final-pdf400948969711266824.pdf (accessed on 20 April 2020).
- Méner, E.L.; Guyavarch, E. Les familles sans domicile à Paris et en Île-de-France: Une population à decouvrir. Revue des Politiques Sociales et Familiales 2014, 115, 80–86. [Google Scholar]
- Vandentorren, S.; Le Méner, E.; Oppenchaim, N.; Arnaud, A.; Jangal, C.; Caum, C.; Vuillermoz, C.; Martin-Fernandez, J.; Lioret, S.; Roze, M.; et al. Characteristics and health of homeless families: The ENFAMS survey in the Paris region, France 2013. Eur. J. Public Health 2016, 26, 71–76. [Google Scholar] [CrossRef] [Green Version]
- Fazel, S.; Geddes, J.R.; Kushel, M. The health of homeless people in high-income countries: Descriptive epidemiology, health consequences, and clinical and policy recommendations. Lancet 2014, 384, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Beijer, U.; Wolf, A.; Fazel, S. Prevalence of tuberculosis, hepatitis C virus, and HIV in homeless people: A systematic review and meta-analysis. Lancet Infect. Dis. 2012, 12, 859–870. [Google Scholar] [CrossRef] [Green Version]
- Grant, R.; Shapiro, A.; Joseph, S.; Goldsmith, S.; Rigual-Lynch, L.; Redlener, I. The health of homeless children revisited. Adv. Pediatr. 2007, 54, 173–187. Available online: http://www.ncbi.nlm.nih.gov/pubmed/17918471 (accessed on 7 December 2015). [CrossRef] [PubMed]
- Cutuli, J.J.; Herbers, J.E.; Lafavor, T.L.; Ahumada, S.M.; Masten, A.S.; Oberg, C.N. Asthma and adaptive functioning among homeless kindergarten-aged children in emergency housing. J. Health Care Poor Underserved 2014, 25, 717–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLean, D.E.; Bowen, S.; Drezner, K.; Rowe, A.; Sherman, P.; Schroeder, S.; Redlener, K.; Redlener, I. Asthma among homeless children: Undercounting and undertreating the underserved. Arch. Pediatr. Adolesc. Med. 2004, 158, 244–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berti, L.C.; Zylbert, S.; Rolnitzky, L. Comparison of health status of children using a school-based health center for comprehensive care. J. Pediatr. Health Care 2001, 15, 244–250. [Google Scholar] [CrossRef]
- Shinn, M.; Schteingart, J.S.; Williams, N.C.; Carlin-Mathis, J.; Bialo-Karagis, N.; Becker-Klein, R.; Weitzman, B.C. Long-Term Associations of Homelessness With Children’s Well-Being. Am. Behav. Sci. 2008, 51, 789–809. [Google Scholar] [CrossRef]
- Schwarz, K.; Garrett, B.; Lamoreux, J.; Bowser, Y.D.; Weinbaum, C.; Alter, M.J. Hepatitis B vaccination rate of homeless children in Baltimore. J. Pediatr. Gastroenterol. Nutr. 2005, 41, 225–229. Available online: http://www.ncbi.nlm.nih.gov/pubmed/16056104 (accessed on 7 December 2015). [CrossRef] [PubMed]
- Fierman, A.H.; Dreyer, B.P.; Acker, P.J.; Legano, L. Status of immunization and iron nutrition in New York City homeless children. Clin. Pediatr. 1993, 32, 151–155. Available online: http://www.ncbi.nlm.nih.gov/pubmed/8453831 (accessed on 7 December 2015). [CrossRef] [PubMed]
- Bouhamam, N.; Laporte, R.; Boutin, A.; Uters, M.; Bremond, V.; Noel, G.; Rodier, P.; Minodier, P. Relationship between precariousness, social coverage, and vaccine coverage: Survey among children consulting in pediatric emergency departments in France. Archives de Pediatrie Organe Officiel de la Societe Francaise de Pediatrie 2012, 19, 242–247. [Google Scholar] [PubMed]
- Beytout, J.; Denis, F.A.F. Description du statut vaccinal de la population adulte française. Med. Mal. Infect. 2002, 32, 678–688. [Google Scholar] [CrossRef]
- Antona, D.; Levy-Bruhl, D.; Baudon, C.; Freymuth, F.; Lamy, M.; Maine, C.; Floret, D.; Du Chatelet, I.P. Measles limination efforts and 2008–2011 outbreak, France. Emerg. Infect. Dis. 2013, 19, 357–364. [Google Scholar] [CrossRef] [Green Version]
- Leon, L.; Jauffret-Roustide, M.; Le Strat, Y. Design-based inference in time-location sampling. Biostatistics 2015, 16, 565–579. [Google Scholar] [CrossRef] [Green Version]
- Bello, P.; Bloch, J.; Brouard, C.; Danet, S.; Fuhrman, C.; Gagnière, B.; Grange, D.; Haus-Cheymol, R.; Jourdan-Da Silva, N.; Lefranc, A.; et al. Le Calendrier des vaccinations et les recommandations vaccinales 2013 selon l’avis du Haut Conseil de la santé publique. Bull. Epidemiol. Hebd. 2013, 14–15, 129–132. [Google Scholar]
- Waldhoer, T.; Haidinger, G.; Vutuc, C.; Haschke, F.; Plank, R. The impact of sociodemographic variables on immunization coverage of children. Eur. J. Epidemiol. 1997, 13, 145–149. [Google Scholar] [CrossRef]
- Zou, G. A modified poisson regression approach to prospective studies with binary data. Am. J. Epidemiol. 2004, 159, 702–706. [Google Scholar] [CrossRef]
- Strine, T.W.; Barker, L.E.; Mokdad, A.H.; Luman, E.T.; Sutter, R.W.; Chu, S.Y. Vaccination coverage of foreign-born children 19 to 35 months of age: Findings from the National Immunization Survey, 1999–2000. Pediatrics 2002, 110 Pt 1, e15. Available online: http://www.ncbi.nlm.nih.gov/pubmed/12165614 (accessed on 15 December 2015). [CrossRef] [Green Version]
- WHO vaccine-preventable diseases: monitoring system. 2019 global summary. Available online: www.apps.who.int/immunization_monitoring/globalsummary/countries (accessed on 10 December 2019).
- ECDC. Vaccine schedules in all countries of the European Union. ECDC. Comparison of Vaccination Recommendation between European Countries. Available online: www.vaccine-schedule.ecdc.europa.eu/Pages/Scheduler.aspx (accessed on 20 April 2020).
- Hahné, S.J.; Veldhuijzen, I.K.; Wiessing, L.; Lim, T.A.; Salminen, M.; van de Laar, M. Infection with hepatitis B and C virus in Europe: A systematic review of prevalence and cost-effectiveness of screening. BMC Infect. Dis. 2013, 13, 181. [Google Scholar] [CrossRef] [Green Version]
- Martin-Fernandez, J.; Lioret, S.; Vuillermoz, C.; Chauvin, P.; Vandentorren, S. Food Insecurity in Homeless Families in the Paris Region (France): Results from the ENFAMS Survey. Int. J. Environ. Res. Public Health 2018, 15, 420. [Google Scholar] [CrossRef] [Green Version]
- Roze, M.; Vandentorren, S.; van der Waerden, J.; Melchior, M. Factors associated with depression among homeless mothers. Results of the ENFAMS survey. J. Affect. Disord. 2018, 229, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Partouche, H.; Gilberg, S.; Renard, V.; Saint-Lary, O. Mandatory vaccination of infants in France: Is that the way forward? Eur. J. Gen. Pract. 2019, 25, 49–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bocquier, A.; Ward, J.; Raude, J.; Peretti-Watel, P.; Verger, P. Socioeconomic differences in childhood vaccination in developed countries: A systematic review of quantitative studies. Expert Rev. Vaccines 2017, 16, 1107–1118. [Google Scholar] [CrossRef] [PubMed]
- Akmatov, M.K.; Mikolajczyk, R.T. Timeliness of childhood vaccinations in 31 low and middle-income countries. J. Epidemiol. Community Health 2012, 66, e14. [Google Scholar] [CrossRef]
- Vandermeulen, C.; Roelants, M.; Theeten, H.; Van Damme, P.; Hoppenbrouwers, K. Vaccination coverage and sociodemographic determinants of measles-mumps-rubella vaccination in three different age groups. Eur. J. Pediatr. 2008, 167, 1161–1168. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Public Health Guidance on Screening and Vaccination for Infectious Diseases in Newly Arrived Migrants within the EU/EEA; ECDC: Stockholm, Sweden, 2018. [Google Scholar]
- Haute Autorité de Santé. Quel Rattrapage Proposer en Cas de Statut Vaccinal Inconnu ou Incomplet ? La HAS Met en Consultation Publique Un Projet de Recommandation; HAS: Paris, France, 12 June 2019; Available online: https://www.has-sante.fr/jcms/prd1_2989799/fr/quel-rattrapage-proposer-en-cas-de-statut-vaccinal-inconnu-ou-incomplet-la-has-met-en-consultation-publique-un-projet-de-recommandation (accessed on 20 April 2020).
- Smith, P.J.; Chu, S.Y.; Barker, L.E. Children who have received no vaccines: Who are they and where do they live? Pediatrics 2004, 114, 187–195. Available online: http://www.ncbi.nlm.nih.gov/pubmed/15231927 (accessed on 15 December 2015). [CrossRef]
- Commission Technique des Vaccinations de la Haute Autorité de Santé (HAS). Calendrier des Vaccinations et Recommandations Vaccinales 2019; Ministère des Solidarités et de la Santé: Paris, France, 2019; 73p.




{kind=link}
{kind=link}
{kind=link}
| Children Born in France | Children Born outside France | Comparison between Children Born in and Outside France | |||||
|---|---|---|---|---|---|---|---|
| Sample Size. n | Estimated Proportion (%) | 95% CI | Sample Size. n | Estimated Proportion (%) | 95% CI | p Value | |
| Gender | 214 | 236 | 0.9392 | ||||
| Male | 105 | 48.9 | 40.3–57.5 | 111 | 49.3 | 41.2–57.5 | |
| Female | 109 | 51.1 | 42.5–59.7 | 125 | 50.7 | 42.5–58.8 | |
| Birthplace | 214 | 236 | |||||
| France | 214 | 100 | |||||
| Europe (except France) | 100 | 46.7 | 38.2–55.4 | ||||
| Africa | 93 | 40.1 | 31.7–49.1 | ||||
| Asia | 40 | 12.3 | 8.7–17.3 | ||||
| America | 3 | 0.9 | 0.2–3.2 | ||||
| Age (years) | 214 | 236 | 0.0008 | ||||
| 2–5 | 153 | 66.1 | 55.9–75.0 | 110 | 45.2 | 38.1–52.6 | |
| 6–9 | 48 | 27.0 | 19.3–36.4 | 80 | 34.0 | 26.8–42.1 | |
| ≥10 | 13 | 6.9 | 3.5–13.2 | 46 | 20.7 | 14.2–29.2 | |
| School attendance | 159 | 217 | 0.0005 | ||||
| No | 8 | 3.1 | 1.3–7.2 | 38 | 16.2 | 11.0–23.3 | |
| Yes | 151 | 96.9 | 92.8–98.7 | 179 | 83.8 | 76.7–89.0 | |
| Child in contact with healthcare at least once in previous year | 211 | 236 | 0.0018 | ||||
| No | 9 | 3.1 | 1.5–6.3 | 27 | 13.5 | 8.8–20.0 | |
| Yes | 202 | 96.9 | 93.7–98.5 | 209 | 86.5 | 80.0–91.2 | |
| Family structure | 212 | 229 | 0.8512 | ||||
| Single-parent family | 118 | 42.2 | 33.9–51.0 | 101 | 43.3 | 35.7–51.2 | |
| Two-parent family | 94 | 57.8 | 49.0–66.1 | 128 | 56.7 | 48.8–64.3 | |
| Variables for parent/family | |||||||
| Age (years) | 214 | 235 | 0.7249 | ||||
| 17–24 | 23 | 11.1 | 5.6–20.8 | 20 | 8.5 | 5.2–13.8 | |
| 25–34 | 99 | 44.0 | 35.2–53.1 | 125 | 46.9 | 37.8–56.3 | |
| 35–44 | 78 | 39.1 | 30.9–48.1 | 69 | 37.3 | 27.7–48.1 | |
| 45–57 | 14 | 5.8 | 3.3–10.0 | 21 | 7.2 | 4.2–11.9 | |
| Birthplace | 214 | 236 | 0.0670 | ||||
| France | 16 | 5.0 | 2.6–9.1 | 1 | 0.7 | 0.1–5.0 | |
| Not in France | 198 | 95.0 | 90.9–97.4 | 235 | 99.3 | 95.0–99.9 | |
| Parent’s length of time living in France | 214 | 236 | <0.0001 | ||||
| <10% | 18 | 7.5 | 3.3–16.1 | 183 | 70.3 | 58.6–79.9 | |
| ≥10% | 196 | 92.5 | 83.9–96.7 | 53 | 29.7 | 20.1–41.4 | |
| Difficulties in understanding/speaking French (parent) | 213 | 236 | 0.0827 | ||||
| No | 158 | 66.1 | 56.2–74.7 | 120 | 53.4 | 43.8–62.7 | |
| Yes | 55 | 33.9 | 25.3–43.8 | 116 | 46.6 | 37.3–56.2 | |
| Other family members in the greater Paris area | 214 | 235 | 0.0002 | ||||
| No | 85 | 32.4 | 25.0–40.8 | 144 | 60.6 | 49.8–70.5 | |
| Yes | 129 | 67.6 | 59.2–75.0 | 91 | 39.4 | 29.5–50.2 | |
| Educational level | 211 | 229 | 0.0044 | ||||
| None | 103 | 47.3 | 39.1–55.7 | 79 | 31.8 | 24.0–40.7 | |
| Primary/Middle school | 46 | 25.9 | 18.3–35.2 | 47 | 26.5 | 17.1–38.7 | |
| High school/University | 62 | 26.8 | 19.3–35.9 | 103 | 41.7 | 33.9–50.0 | |
| Monthly household income (euros) | 204 | 232 | <0.0001 | ||||
| <500 | 89 | 31.7 | 23.8–40.8 | 152 | 59.6 | 51.3–67.3 | |
| ≥500 | 115 | 68.3 | 59.2–76.2 | 80 | 40.4 | 32.7–48.7 | |
| Health insurance | 214 | 236 | 0.0001 | ||||
| None or application in progress | 20 | 9.2 | 5.2–15.6 | 65 | 27.4 | 21.3–34.5 | |
| Standard health insurance or specific coverage | 194 | 90.8 | 84.4–94.8 | 171 | 72.6 | 65.5–78.7 | |
| Number of changes of residence in the previous year | 211 | 234 | 0.0096 | ||||
| 0–1 | 172 | 79.1 | 69.9–86.1 | 145 | 63.5 | 54.0–72.1 | |
| ≥2 | 39 | 20.9 | 13.9–30.1 | 89 | 36.5 | 27.9–46.0 | |
| Vaccine | General Population, Greater Paris Area | Children Born in France (n = 214) | Children Born Outside France (n = 236) | Comparison between Children Born in France and Those Born Outside France | ||||
|---|---|---|---|---|---|---|---|---|
| Estimated Vaccination Coverage % | 95%CI | Estimated Vaccination Coverage % | 95%CI | Estimated Vaccination Coverage Ratio % | 95%CI | p Value | ||
| DT-IPV 3 doses | 99.1 | 98.6 | 96.1–99.5 | 47.7 | 39.4–56.1 | 2.1 | 1.7–2.5 | <0.0001 |
| MMR 1 dose | 92.0 | 90.1 | 81.6–95.0 | 33.7 | 25.4–43.1 | 2.7 | 2.0–3.5 | <0.0001 |
| HepB 3 doses | 60.9 | 73.6 | 65.4–80.4 | 26.3 | 20.6–32.8 | 2.8 | 2.2–3.6 | <0.0001 |
| DT-IPV Vaccine (n = 211) * | MMR Vaccine (n = 157) † | HepB Vaccine (n = 159) ‡ | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Adjusted Proportion Ratio | 95%CI | p Value | Adjusted Proportion Ratio | 95%CI | p Value | Adjusted Proportion Ratio | 95%CI | p Value | |
| Gender | 0.031 | ||||||||
| Male | 1 (ref) | ||||||||
| Female | 0.29 | 0.09–0.89 | |||||||
| Age (years) | 0.001 | ||||||||
| 2—5 | 1 (ref) | ||||||||
| 6—9 | 4.00 | 1.87–8.59 | |||||||
| ≥ 10 | 2.55 | 0.87–10.31 | |||||||
| School attendance | 0.006 | <0.001 | |||||||
| No | 1 (ref) | 1 (ref) | |||||||
| Yes | 0.19 | 0.06–0.61 | 0.23 | 0.11–0.49 | |||||
| Contact with healthcare at least once in the previous year (child) | 0.042 | 0.032 | |||||||
| No | 1 (ref) | 1 (ref) | |||||||
| Yes | 0.30 | 0.09–0.96 | 0.18 | 0.04–0.86 | |||||
| Variables for parent/family | |||||||||
| Birthplace | 0.001 | 0.006 | |||||||
| France | 1(ref) | 1 (ref) | |||||||
| Outside France | 4.93 | 2.01–12.07 | 5.54 | 1.67–18.37 | |||||
| Other family members in the greater Paris area | 0.025 | ||||||||
| No | 1 (ref) | ||||||||
| Yes | 0.37 | 0.15–0.88 | |||||||
| Health insurance | 0.010 | ||||||||
| None or application in progress | 1 (ref) | ||||||||
| Standard health insurance or specific coverage | 0.36 | 0.16–0.77 | |||||||
| DT-IPV Vaccine (n = 234) * | MMR Vaccine (n = 227) † | HepB Vaccine (n = 232) ‡ | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Adjusted Proportion Ratio | 95%CI | p Value | Adjusted Proportion Ratio | 95%CI | p Value | Adjusted Proportion Ratio | 95%CI | p Value | |
| Age (years) | 0.014 | 0.017 | |||||||
| 2—5 | 1 (ref) | 1 (ref) | |||||||
| 6—9 | 1.42 | 1.11–1.82 | 1.43 | 1.11–1.82 | |||||
| ≥10 | 0.99 | 0.73–1.35 | 1.30 | 0.93–1.82 | |||||
| Contact with healthcare at least once in the previous year (child) | 0.014 | 0.035 | <0.001 | ||||||
| No | 1 (ref) | 1 (ref) | 1 (ref) | ||||||
| Yes | 0.72 | 0.56–0.93 | 0.70 | 0.50–0.97 | 0.66 | 0.53–0.81 | |||
| Variables for parent/family | |||||||||
| Difficulties with understanding/speaking French (parent) | <0.001 | 0.044 | |||||||
| No | 1 (ref) | 1 (ref) | |||||||
| Yes | 1.47 | 1.15–1.88 | 1.51 | 1.01–2.27 | |||||
| Educational level | 0.046 | ||||||||
| None | 1 (ref) | ||||||||
| Primary/Middle school | 0.59 | 0.36–0.96 | |||||||
| High school/University | 0.80 | 0.59–1.07 | |||||||
| Monthly household income (euros) | 0.010 | ||||||||
| <500 | 1 (ref) | ||||||||
| ≥500 | 0.67 | 0.49–0.90 | |||||||
| Health insurance | 0.035 | ||||||||
| None or application in progress | 1 (ref) | ||||||||
| Standard health insurance or specific coverage | 0.58 | 0.40–0.86 | |||||||
| Number of changes of residence in the previous year | 0.013 | 0.015 | |||||||
| 0–1 | 1 (ref) | 1 (ref) | |||||||
| ≥2 | 1.29 | 1.06–1.58 | 1.64 | 1.10–2.45 | |||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mansor-Lefebvre, S.; Le Strat, Y.; Bernadou, A.; Vignier, N.; Guthmann, J.-P.; Arnaud, A.; Lévy-Bruhl, D.; Vandentorren, S. Diphtheria-Tetanus-Polio, Measles-Mumps-Rubella, and Hepatitis B Vaccination Coverage and Associated Factors among Homeless Children in the Paris Region in 2013: Results from the ENFAMS Survey. Int. J. Environ. Res. Public Health 2020, 17, 2854. https://doi.org/10.3390/ijerph17082854
Mansor-Lefebvre S, Le Strat Y, Bernadou A, Vignier N, Guthmann J-P, Arnaud A, Lévy-Bruhl D, Vandentorren S. Diphtheria-Tetanus-Polio, Measles-Mumps-Rubella, and Hepatitis B Vaccination Coverage and Associated Factors among Homeless Children in the Paris Region in 2013: Results from the ENFAMS Survey. International Journal of Environmental Research and Public Health. 2020; 17(8):2854. https://doi.org/10.3390/ijerph17082854
Chicago/Turabian StyleMansor-Lefebvre, Samreen, Yann Le Strat, Anne Bernadou, Nicolas Vignier, Jean-Paul Guthmann, Amandine Arnaud, Daniel Lévy-Bruhl, and Stéphanie Vandentorren. 2020. "Diphtheria-Tetanus-Polio, Measles-Mumps-Rubella, and Hepatitis B Vaccination Coverage and Associated Factors among Homeless Children in the Paris Region in 2013: Results from the ENFAMS Survey" International Journal of Environmental Research and Public Health 17, no. 8: 2854. https://doi.org/10.3390/ijerph17082854
APA StyleMansor-Lefebvre, S., Le Strat, Y., Bernadou, A., Vignier, N., Guthmann, J. -P., Arnaud, A., Lévy-Bruhl, D., & Vandentorren, S. (2020). Diphtheria-Tetanus-Polio, Measles-Mumps-Rubella, and Hepatitis B Vaccination Coverage and Associated Factors among Homeless Children in the Paris Region in 2013: Results from the ENFAMS Survey. International Journal of Environmental Research and Public Health, 17(8), 2854. https://doi.org/10.3390/ijerph17082854