The Effects of Performance of Public Sector Health System on Quality of Life in China: Evidence from the CGSS2015



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
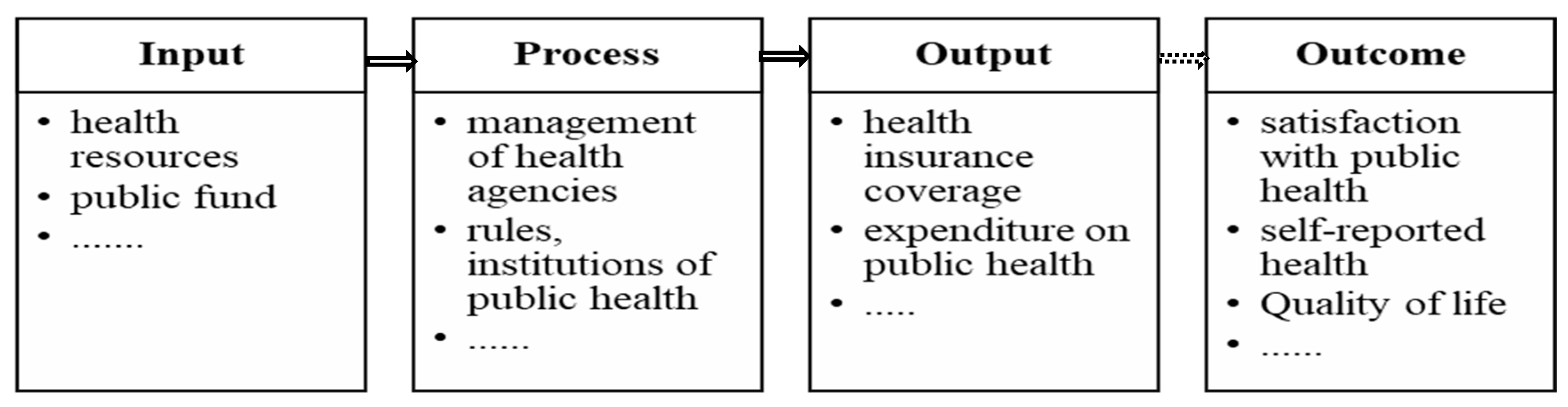
2.2. Variables Specification
2.3. Model Specification
3. Results
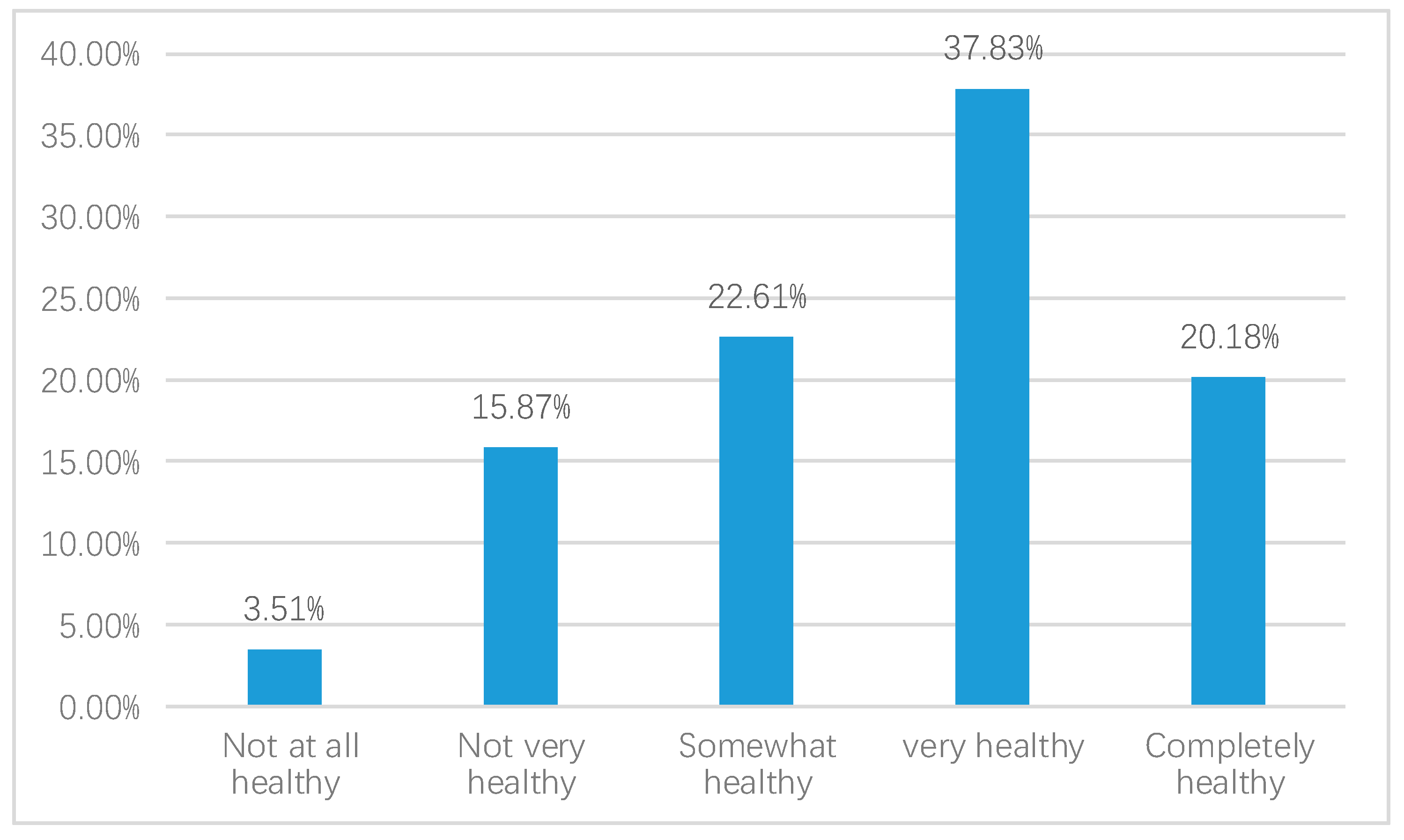
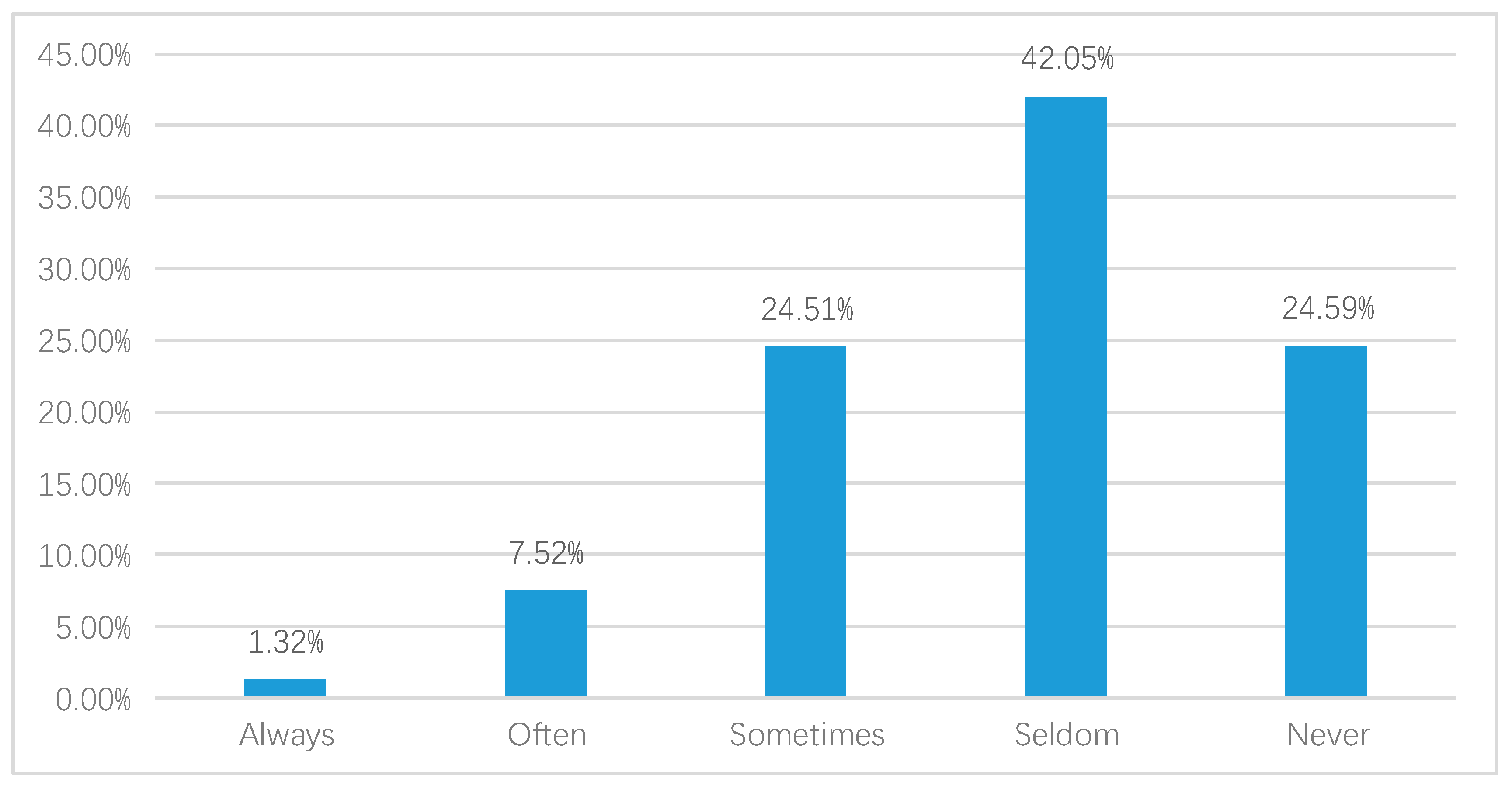
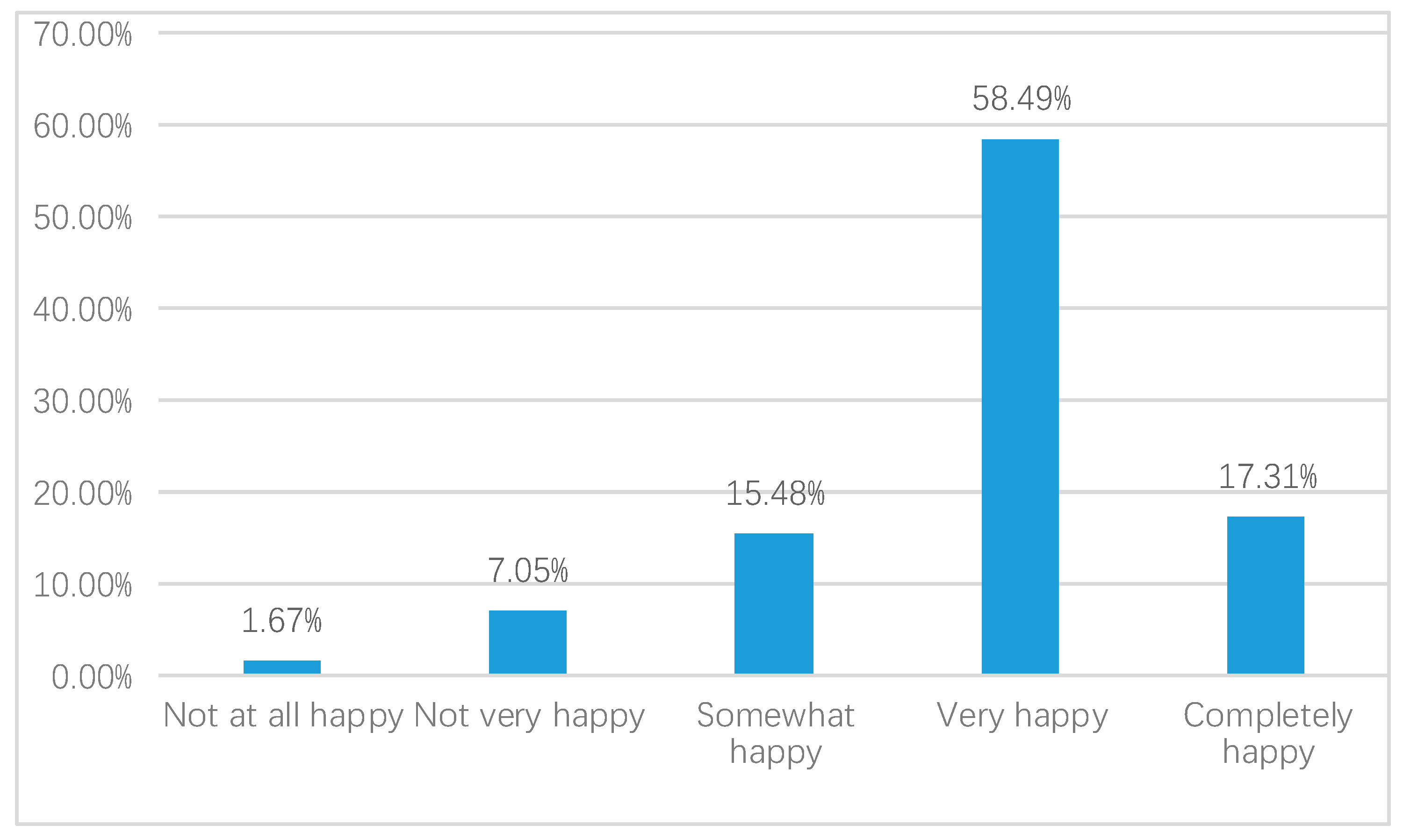
3.1. Description of Quality of Life in China
3.2. Regression Results
3.3. Robust Check
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wang, Z.; Xu, J. Association between resilience and quality of life in Wenchuan Earthquake Shidu parents: The mediating role of social support. Community Ment. Health J. 2017, 53, 859–863. [Google Scholar] [CrossRef] [PubMed]
- Ardalan, A.; Mazaheri, M.; Vanrooyen, M.; Mowafi, H.; Nedjat, S.; Holakouie Naieni, K.; Russel, M. Post-disaster quality of life among older survivors five years after the Bam earthquake: Implications for recovery policy. Ageing Soc. 2011, 31, 179–196. [Google Scholar] [CrossRef]
- Chou, F.-C.; Chou, P.; Lin, C.; Su, T.T.; Ou-Yang, W.C.; Chien, I.C.; Su, C.Y.; Lui, M.K.; Chen, M.K. The relationship between quality of life and psychiatric impairment for a Taiwanese community post-earthquake. Qual. Life Res. 2004, 13, 1089–1097. [Google Scholar] [CrossRef]
- Cui, K.; Han, Z. Association between disaster experience and quality of life: The mediating role of disaster risk perception. Qual. Life Res. 2018, 28, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.-R.; Huang, W.; Huang, C.; Hwang, H.; Tsai, L.; Chiu, Y. The impact of the Chi-Chi earthquake on quality of life among elderly survivors in Taiwan–A before and after study. Qual. Life Res. 2002, 11, 379–388. [Google Scholar] [CrossRef]
- Berlemann, M. Does hurricane risk affect individual well-being? Empirical evidence on the indirect effects of natural disasters. Ecol. Econ. 2016, 124, 99–113. [Google Scholar] [CrossRef]
- Estes, R.J.; Sirgy, M.J. Radical Islamic militancy and acts of terrorism: A quality-of-life analysis. Soc. Indic. Res. 2014, 117, 615–652. [Google Scholar] [CrossRef]
- Charyton, C.; Elliott, J.O.; Lu, B.; Moore, J. The impact of social support on health-related quality of life in persons with epilepsy. Epilepsy Behav. 2009, 16, 640–645. [Google Scholar] [CrossRef]
- Ke, X.; Liu, C.; Li, N. Social support and quality of life: A cross-sectional study on survivors eight months after the 2008 Wenchuan earthquake. BMC Public Health 2010, 10, 573. [Google Scholar] [CrossRef] [Green Version]
- Bjørnskov, C.; Dreher, A.; Fischer, J.A. The bigger the better? Evidence of the effect of government size on life satisfaction around the world. Public Choice 2007, 130, 267–292. [Google Scholar] [CrossRef] [Green Version]
- Elliott, M.; Hayward, R.D. Religion and life satisfaction worldwide: The role of government regulation. Sociol. Relig. 2009, 70, 285–310. [Google Scholar] [CrossRef]
- Cheung, C.-K.; Leung, K.-K. Enhancing life satisfaction by government accountability in China. Soc. Indic. Res. 2007, 82, 411–432. [Google Scholar] [CrossRef]
- Bouckaert, G.; Van De Walle, S. Potential for comparative public opinion research in Public Administration. Int. Rev. Adm. Sci. 2005, 2, 293–313. [Google Scholar] [CrossRef] [Green Version]
- Yang, K.; Holzer, M. The performance–trust link: Implications for performance measurement. Public Adm. Rev. 2006, 66, 114–126. [Google Scholar] [CrossRef]
- Chinese Academy of Social Sciences in December 2019. Available online: https://shareapp.cyol.com/cmsfile/News/201812/21/share166144.html?t=1545385607&nid=166144[EB/OL] (accessed on 22 February 2020). (In Chinese).
- Relative Achievements in Institutional Reform of Health Care from 1949 to 2019. Available online: http://www.xinhuanet.com/politics/2019-09/25/c_1210291935.htm (accessed on 25 January 2020). (In Chinese).
- Whiteley, P.; Clarke, H.D.; Sanders, D.; Stewart, M. Government performance and life satisfaction in contemporary Britain. J. Politics 2010, 72, 733–746. [Google Scholar] [CrossRef] [Green Version]
- Gregory, D.; Johnston, R.; Pratt, G. Quality of Life; Wiley-Blackwell: Oxford, UK, 2009. [Google Scholar]
- Mcnally, J.W. Encyclopedia of the Life Course and Human Development; Macmillan Reference: New York, NY, USA, 2009. [Google Scholar]
- Chen, T.; Wang, Y.; Luo, X.; Hua, L. Inter-provincial inequality of public health services in China: The perspective of local officials’ behavior. Int. J. Equity Health 2018, 17, 108. [Google Scholar] [CrossRef]
- National Bureau of Statistics of China. Report on the Implementation of China Children’s Development Program (2011–2014). 2015. Available online: http://www.stats.gov.cn/tjsj/zxfb/201511/t20151127_1282230.html (accessed on 25 January 2020). (In Chinese)
- National Statistics Bureau of China. China Statistical Yearbook 2015; China Statistics Press: Beijing, China, 2015. (In Chinese)
- Zhou, Z.; Fang, Y.; Zhou, Z.; Li, D.; Wang, D.; Li, Y.; Lu, L.; Gao, J.; Chen, G. Assessing income-related health inequality and horizontal inequity in China. Soc. Indic. Res. 2017, 132, 241–256. [Google Scholar] [CrossRef]
- Meng, Q.; Xu, L.; Zhang, Y.; Qian, J.; Cai, M.; Xin, Y.; Gao, J.; Xu, K.; Boerma, J.; Barber, S. Trends in access to health services and financial protection in China between 2003 and 2011: A cross-sectional study. Lancet 2012, 379, 805–814. [Google Scholar] [CrossRef]
- Syed, S.T.; Gerber, B.S.; Sharp, L.K. Traveling towards disease: Transportation barriers to health care access. J. Community Health 2013, 38, 976–993. [Google Scholar] [CrossRef] [Green Version]
- Atuoye, K.N.; Dixon, J.; Rishworth, A.; Galaa, S.; Boamah, S.; Luginaah, I. Can she make it? Transportation barriers to accessing maternal and child health care services in rural Ghana. BMC Health Serv. Res. 2015, 15, 333. [Google Scholar] [CrossRef] [Green Version]
- Woodward, A.; Kawachi, I. Why reduce health inequalities? J. Epidemiol. Community Health 2000, 54, 923–929. [Google Scholar] [CrossRef]
- Chzhen, Y.; Bruckauf, Z.; Ng, K.; Pavlove, D.; Torsheim, T.; De Matos, M. Inequalities in Adolescent Health and Life Satisfaction: Evidence from the Health Behavior in School-Aged Children Study; Innocenti Working Paper: Florence, Italy, 2016. [Google Scholar]
- Brown, M.G.; Svenson, R.A. Measuring r&d productivity. Res. Technol. Manag. 1988, 31, 11–15. [Google Scholar]
- Wall, T.D.; Michie, J.; Patterson, M.; Wood, S. On the validity of subjective measures of company performance. Pers. Psychol. 2004, 57, 95–118. [Google Scholar] [CrossRef]
- Boyne, G.; Day, P.; Walker, R. The evaluation of public service inspection: A theoretical framework. Urban Stud. 2002, 39, 1197–1212. [Google Scholar] [CrossRef]
- Stipak, B. Citizen satisfaction with urban services: Potential misuse as a performance indicator. Public Adm. Rev. 1979, 39, 46–52. [Google Scholar] [CrossRef] [Green Version]
- Brudney, J.L.; England, R.E. Urban policy making and subjective service evaluations: Are they compatible? Public Adm. Rev. 1982, 42, 127–135. [Google Scholar] [CrossRef]
- Van Ryzin, G.G. Expectations, performance, and citizen satisfaction with urban services. J. Policy Anal. Manag. 2004, 23, 433–448. [Google Scholar] [CrossRef]
- Zhao, D. The mandate of heaven and performance legitimation in historical and contemporary China. Am. Behav. Sci. 2009, 53, 416–433. [Google Scholar] [CrossRef]
- Zhu, Y. “Performance legitimacy” and China’s political adaptation strategy. JCPS 2011, 16, 123–140. [Google Scholar] [CrossRef]
- Lee, J.; Kim, S. Citizens’ e-participation on agenda setting in local governance: Do individual social capital and e-participation management matter? Public Manag. Rev. 2018, 20, 873–895. [Google Scholar] [CrossRef]
- Baltatescu, S. Confidence in Government and Happiness in EU and US. Presented at the International Joint Workshop: Europe and North America-Societies in Contrast, Delmenhorst, Germany, 6–9 March 2005. [Google Scholar]
- Kim, M.-K.; Lee, G.-G.; Lee, S.-Y.; Chun, J.; Han, Y. The Effects of Job-Seeking Stress, Appearance Recognition, Financial Distress, Trust in Government, and Locus of Control on University Students’ Happiness. J. Soc. Korea Ind. Syst. Eng. 2017, 40, 171–182. [Google Scholar] [CrossRef]
- Dankulincova Veselska, Z.; Jirasek, I.; Veselsky, P.; Jiraskova, M.; Plevova, I.; Tavel, P.; Geckova, A. Spirituality but not Religiosity Is Associated with Better Health and Higher Life Satisfaction among Adolescents. Int. J. Environ. Res. Public Health 2018, 15, 2781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kline, P. The Handbook of Psychological Testing, 2nd ed.; Routledge: London, UK, 2000. [Google Scholar]
- Zineldin, M. The quality of health care and patient satisfaction. Int. J. Health Care Qual. Assur. 2006, 19, 60–92. [Google Scholar] [CrossRef] [PubMed]
- Hussain, A.; Sial, M.S.; Usman, S.M.; Usman, S.; Hwang, J.; Jiang, Y.; Shafiq, A. What factors affect patient satisfaction in public sector hospitals: Evidence from an emerging economy. Int. J. Environ. Res. Public Health 2019, 16, 994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, L.; Lee, P.S. Multiple determinants of life quality: The roles of Internet activities, use of new media, social support, and leisure activities. Telemat. Inform. 2005, 22, 161–180. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Observation | Mean | Std. Dev. | Min | Max |
|---|---|---|---|---|---|
| Self-reported health | 10,961 | 3.608 | 1.075 | 1 | 5 |
| Depressed mood | 10,942 | 3.840 | 0.924 | 1 | 5 |
| Happiness | 10,953 | 3.867 | 0.821 | 1 | 5 |
| HCP | 10,846 | 3.365 | 0.910 | 1 | 5 |
| MCPH | 10,735 | 69.756 | 17.932 | 0 | 100 |
| Internet usage | 10,951 | 2.370 | 1.635 | 1 | 5 |
| Gender | |||||
| Female | 10,968 | 0.532 | 0.499 | 0 | 1 |
| Age | 10,968 | 50.397 | 16.898 | 18 | 95 |
| Age squared | 10,968 | 2825.388 | 1742.334 | 324 | 9025 |
| Years of education | 10,939 | 8.694 | 4.707 | 0 | 19 |
| Place of residence | |||||
| Rural area | 10,968 | 0.410 | 0.492 | 0 | 1 |
| Party status | |||||
| Youth League member | 10,921 | 0.050 | 0.218 | 0 | 1 |
| Democratic party member | 10,921 | 0.001 | 0.038 | 0 | 1 |
| CPC member | 10,921 | 0.104 | 0.305 | 0 | 1 |
| Marital status | |||||
| Married | 10,968 | 0.784 | 0.411 | 0 | 1 |
| Divorced | 10,968 | 0.021 | 0.143 | 0 | 1 |
| Widowed | 10,968 | 0.092 | 0.28 | 0 | 1 |
| Income (log) | 8722 | 9.765 | 1.271 | 3.912 | 16.118 |
| Expenditure on public health (100 million) | 28 | 348.104 | 169.954 | 65.27 | 777.55 |
| GDP per capita (yuan RMB) | 28 | 52,292.61 | 22,652.38 | 26,433 | 105,231 |
| Population (10,000) | 28 | 4740.25 | 2709.963 | 583 | 10,724 |
| Main | (1) | (2) | (3) | (4) | (5) | (6) |
|---|---|---|---|---|---|---|
| Self-Reported Health | Depressed Mood | Happiness | Self-Reported Health | Depressed Mood | Happiness | |
| HCP | 0.144 *** | 0.167 *** | 0.328 *** | |||
| (4.30) | (3.98) | (8.73) | ||||
| MCPH | 0.00921 *** | 0.00905 *** | 0.0162 *** | |||
| (5.37) | (5.75) | (9.56) | ||||
| Internet Usage | 0.0702 *** | 0.0765 *** | 0.0436 | 0.0680 *** | 0.0704 *** | 0.0326 |
| (3.49) | (4.34) | (1.66) | (3.34) | (3.75) | (1.25) | |
| Female | −0.205 *** | −0.0761 | 0.252 *** | −0.215 *** | −0.0779 | 0.243 *** |
| (−3.61) | (−1.65) | (3.83) | (−3.88) | (−1.67) | (3.75) | |
| Age | −0.0735 *** | −0.0222 | −0.0583 *** | −0.0747 *** | −0.0244 | −0.0595 *** |
| (−7.28) | (−1.50) | (−5.29) | (−7.29) | (−1.73) | (−5.41) | |
| Age Squared | 0.000329 *** | 0.000205 | 0.000668 *** | 0.000336 *** | 0.000228 | 0.000677 *** |
| (3.70) | (1.57) | (6.59) | (3.77) | (1.84) | (6.74) | |
| Years of Education | 0.0115 | 0.0345 *** | 0.0331 ** | 0.0120 | 0.0357 *** | 0.0308 ** |
| (1.42) | (4.61) | (3.12) | (1.53) | (4.84) | (2.95) | |
| Living Place | Reference group: urban | |||||
| Rural Area | 0.0105 | −0.0477 | 0.179 | 0.00107 | −0.0503 | 0.179 * |
| (0.16) | (−0.62) | (1.91) | (0.02) | (−0.66) | (1.97) | |
| Party Affiliation | The mass as reference group | |||||
| Youth League | 0.189 | −0.0747 | 0.484 *** | 0.176 | −0.107 | 0.484 *** |
| (1.26) | (−0.57) | (4.40) | (1.24) | (−0.81) | (4.37) | |
| Democratic Member | 0.359 | 0.323 | 0.0676 | 0.332 | 0.295 | 0.0562 |
| (1.19) | (0.46) | (0.08) | (1.06) | (0.42) | (0.07) | |
| CPC Member | 0.177 ** | 0.113 | 0.294 *** | 0.172 ** | 0.0882 | 0.281 *** |
| (3.04) | (1.44) | (3.87) | (2.91) | (1.09) | (3.86) | |
| Marriage Status | Unmarried as reference group | |||||
| Married | 0.302 *** | 0.134 | 0.681 *** | 0.295 *** | 0.110 | 0.637 *** |
| (3.57) | (1.30) | (5.45) | (3.55) | (1.02) | (5.03) | |
| Divorced | −0.00505 | −0.367 * | −0.329 * | 0.0220 | −0.400 * | −0.311 * |
| (−0.04) | (−2.07) | (−2.26) | (0.16) | (−2.19) | (−2.30) | |
| Widowed | 0.323 ** | 0.0213 | 0.348 ** | 0.355 *** | 0.0121 | 0.307 * |
| (3.17) | (0.16) | (2.64) | (3.37) | (0.09) | (2.16) | |
| Income per Year (ln) | 0.175 *** | 0.199 *** | 0.177 *** | 0.169 *** | 0.199 *** | 0.178 *** |
| (4.78) | (6.52) | (4.09) | (4.68) | (6.38) | (4.34) | |
| cut1 | −4.035 *** | −2.196 *** | −1.526 ** | −3.984 *** | −2.203 *** | −1.628 ** |
| (−9.42) | (−3.77) | (−2.84) | (−8.54) | (−3.88) | (−3.04) | |
| cut2 | −1.967 *** | −0.0836 | 0.308 | −1.910 *** | −0.0877 | 0.222 |
| (−4.86) | (−0.16) | (0.57) | (−4.33) | (−0.17) | (0.42) | |
| cut3 | −0.637 | 1.662 *** | 1.649 ** | −0.577 | 1.665 ** | 1.558 ** |
| (−1.65) | (3.29) | (3.17) | (−1.38) | (3.27) | (2.98) | |
| cut4 | 1.349 *** | 3.617 *** | 4.604 *** | 1.413 ** | 3.615 *** | 4.505 *** |
| (3.34) | (7.33) | (8.42) | (3.25) | (7.34) | (8.17) | |
| N | 8561 | 8550 | 8559 | 8509 | 8503 | 8508 |
| Main | (7) | (8) | (9) |
|---|---|---|---|
| Self-Reported Health | Depressed Mood | Happiness | |
| Expenditure on Public Health (log) | 0.236 | 0.245 * | −0.276 |
| (1.80) | (2.00) | (−1.94) | |
| GDP Per Capita (log) | −0.108 | 0.403 * | 0.0592 |
| (−0.62) | (2.50) | (0.32) | |
| Internet Usage | 0.0622 *** | 0.0382 * | 0.00977 |
| (3.32) | (2.00) | (0.48) | |
| Female | −0.184 *** | −0.106 * | 0.251 *** |
| (−4.36) | (−2.50) | (5.52) | |
| Age | −0.0701 *** | −0.0260 ** | −0.0578 *** |
| (−7.97) | (−2.95) | (−6.17) | |
| Age Squared | 0.000311 *** | 0.000206 * | 0.000680 *** |
| (3.89) | (2.56) | (7.93) | |
| Years of Education | 0.0133 * | 0.0276 *** | 0.0285 *** |
| (2.07) | (4.30) | (4.13) | |
| Living Place | Reference group: urban | ||
| Rural Area | −0.0421 | 0.0534 | 0.154 ** |
| (−0.82) | (1.05) | (2.80) | |
| Party Affiliation | The mass as reference group | ||
| Youth League | 0.227 * | −0.0135 | 0.507 *** |
| (1.84) | (−0.11) | (3.86) | |
| Democratic Member | 0.288 | 0.271 | 0.0706 |
| (0.61) | (0.53) | (0.13) | |
| CPC Member | 0.189 ** | 0.154 * | 0.291 *** |
| (2.84) | (2.28) | (4.09) | |
| Marriage Status | Unmarried as reference group | ||
| Married | 0.224 * | 0.190 * | 0.607 *** |
| (2.51) | (2.11) | (6.46) | |
| Divorced | −0.0585 | −0.382 ** | −0.358 * |
| (−0.37) | (−2.35) | (−2.16) | |
| Widowed | 0.263 * | 0.0913 | 0.243 * |
| (2.26) | (0.78) | (1.95) | |
| Income per Year (ln) | 0.207 *** | 0.160 *** | 0.179 *** |
| (9.51) | (7.51) | (7.76) | |
| cut1 | −4.005 * | 2.398 | −3.780 |
| (−2.00) | (1.28) | (−1.74) | |
| cut2 | −1.931 | 4.498 * | −1.956 |
| (−0.96) | (2.40) | (−0.90) | |
| cut3 | −0.580 | 6.265 *** | −0.611 |
| (−0.29) | (3.35) | (−0.28) | |
| cut4 | 1.451 | 8.241 *** | 2.377 |
| (0.72) | (4.40) | (1.10) | |
| Variance (province) | |||
| Constant | 0.115 *** | 0.0977 ** | 0.135 *** |
| (3.37) | (3.05) | (3.33) | |
| N | 8649 | 8639 | 8648 |
| Main | (10) | (11) | (12) | (13) | (14) | (15) |
|---|---|---|---|---|---|---|
| Self-Reported Health | Depressed Mood | Happiness | Self-Reported Health | Depressed Mood | Happiness | |
| HCP | 0.160 *** | 0.176 *** | 0.363 *** | |||
| (5.89) | (6.32) | (11.96) | ||||
| MCPH | 0.0100 *** | 0.0102 *** | 0.0169 *** | |||
| (7.15) | (6.94) | (10.77) | ||||
| Internet Usage | 0.0604 ** | 0.0756 *** | 0.0402 | 0.0583 ** | 0.0711 ** | 0.0267 |
| (2.91) | (3.35) | (1.72) | (2.78) | (3.15) | (1.13) | |
| Female | −0.215 *** | −0.0861 | 0.249 *** | −0.235 *** | −0.0925 | 0.234 *** |
| (−4.49) | (−1.78) | (4.67) | (−4.90) | (−1.91) | (4.38) | |
| Age | −0.0796 *** | −0.0110 | −0.0584 *** | −0.0804 *** | −0.0121 | −0.0584 *** |
| (−8.06) | (−1.07) | (−5.34) | (−8.02) | (−1.18) | (−5.31) | |
| Age Squared | 0.000376 *** | 0.0000992 | 0.000658 *** | 0.000379 *** | 0.000109 | 0.000657 *** |
| (4.17) | (1.06) | (6.56) | (4.13) | (1.16) | (6.52) | |
| Years of Education | 0.00958 | 0.0297 *** | 0.0291 *** | 0.0114 | 0.0313 *** | 0.0281 *** |
| (1.33) | (4.22) | (3.72) | (1.56) | (4.43) | (3.55) | |
| Living Place | Reference group: urban | |||||
| Rural Area | −0.0281 | −0.117 * | 0.145 * | −0.0316 | −0.120 * | 0.156 * |
| (−0.50) | (−2.13) | (2.39) | (−0.56) | (−2.16) | (2.55) | |
| Party Affiliation | The mass as reference group | |||||
| Youth League | 0.100 | −0.0482 | 0.559 *** | 0.0689 | −0.0820 | 0.563 *** |
| (0.66) | (−0.35) | (3.82) | (0.46) | (−0.62) | (3.86) | |
| Democratic Member | 0.822 | 0.555 | 0.823 | 0.761 | 0.506 | 0.706 |
| (1.62) | (0.77) | (1.18) | (1.46) | (0.69) | (1.11) | |
| CPC member | 0.145 * | 0.112 | 0.327 *** | 0.135 | 0.0852 | 0.308 *** |
| (1.98) | (1.45) | (4.26) | (1.83) | (1.10) | (3.96) | |
| Marriage Status | Unmarried as reference group | |||||
| Married | 0.329 *** | 0.140 | 0.819 *** | 0.325 *** | 0.127 | 0.767 *** |
| (3.51) | (1.35) | (7.34) | (3.41) | (1.23) | (6.98) | |
| Divorced | −0.0205 | −0.391 | −0.318 | −0.00328 | −0.435 * | −0.320 |
| (−0.12) | (−1.88) | (−1.68) | (−0.02) | (−2.12) | (−1.67) | |
| Widowed | 0.351 ** | 0.0722 | 0.398 ** | 0.394 ** | 0.0762 | 0.354 * |
| (2.82) | (0.54) | (2.72) | (3.14) | (0.57) | (2.42) | |
| Income per year (ln) | 0.179 *** | 0.195 *** | 0.178 *** | 0.171 *** | 0.195 *** | 0.181 *** |
| (7.08) | (8.28) | (6.78) | (6.70) | (8.22) | (6.90) | |
| cut1 | −4.141 *** | −1.818 *** | −1.153 ** | −4.115 *** | −1.750 *** | −1.278 ** |
| (−11.49) | (−4.71) | (−2.86) | (−11.23) | (−4.50) | (−3.14) | |
| cut2 | −2.089 *** | 0.188 | 0.559 | −2.040 *** | 0.249 | 0.467 |
| (−5.91) | (0.52) | (1.43) | (−5.67) | (0.68) | (1.19) | |
| cut3 | −0.750 * | 1.892 *** | 1.871 *** | −0.694 | 1.968 *** | 1.774 *** |
| (−2.13) | (5.23) | (4.79) | (−1.94) | (5.40) | (4.51) | |
| cut4 | 1.220 *** | 3.831 *** | 4.784 *** | 1.280 *** | 3.906 *** | 4.676 *** |
| (3.47) | (10.52) | (12.11) | (3.58) | (10.65) | (11.78) | |
| N | 8536 | 8526 | 8534 | 8485 | 8479 | 8484 |
| Main | (16) | (17) | (18) |
|---|---|---|---|
| Self-Reported Health | Depressed Mood | Happiness | |
| Expenditure on Public Health (log) | 0.211 * | 0.188 * | −0.322 |
| (1.99) | (2.48) | (−1.16) | |
| GDP Per Capita (log) | −0.108 | 0.370 * | 0.0539 |
| (−0.66) | (2.20) | (0.29) | |
| Internet usage | 0.0534 ** | 0.0417 | 0.00669 |
| (2.60) | (1.67) | (0.18) | |
| Gender | Male as reference | ||
| Female | −0.192 *** | −0.120 * | 0.259 *** |
| (−3.39) | (−2.23) | (4.37) | |
| Age | −0.0748 *** | −0.0147 | −0.0573 *** |
| (−5.73) | (−1.03) | (−5.84) | |
| Age Squared | 0.000351 ** | 0.000102 | 0.000672 *** |
| (3.05) | (0.80) | (7.23) | |
| Years of Education | 0.0135 | 0.0230 ** | 0.0279 ** |
| (1.36) | (3.08) | (3.01) | |
| Living Place | Reference group: urban | ||
| Rural Area | −0.0567 | 0.0216 | 0.170 * |
| (−1.04) | (0.35) | (2.46) | |
| Party Affiliation | The mass as reference group | ||
| Youth League | 0.139 | 0.0151 | 0.584 *** |
| (0.81) | (0.09) | (4.41) | |
| Democratic Member | 0.652 | 0.497 | 0.717 |
| (1.46) | (0.54) | (1.08) | |
| CPC member | 0.154 | 0.167 * | 0.342 *** |
| (1.91) | (2.04) | (3.36) | |
| Marriage status | Unmarried as reference group | ||
| Married | 0.265 ** | 0.221 | 0.749 *** |
| (2.84) | (1.86) | (6.06) | |
| Divorced | −0.0322 | −0.392 * | −0.316 * |
| (−0.20) | (−1.98) | (−2.01) | |
| Widowed | 0.313 ** | 0.163 | 0.315 * |
| (2.90) | (1.14) | (2.03) | |
| Income per year (ln) | 0.219 *** | 0.161 *** | 0.188 *** |
| (8.13) | (6.57) | (5.47) | |
| cut1 | −4.148 * | 2.172 | −3.656 |
| (−2.11) | (1.08) | (−1.77) | |
| cut2 | −2.086 | 4.164 * | −1.957 |
| (−1.08) | (2.09) | (−0.92) | |
| cut3 | −0.728 | 5.891 ** | −0.645 |
| (−0.39) | (2.95) | (−0.31) | |
| cut4 | 1.278 | 7.848 *** | 2.285 |
| (0.67) | (3.93) | (1.07) | |
| Variance (Province) | |||
| constant | 0.110 *** | 0.0993 ** | 0.125 *** |
| (4.62) | (3.28) | (4.44) | |
| N | 8624 | 8615 | 8623 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, Z.; Li, J. The Effects of Performance of Public Sector Health System on Quality of Life in China: Evidence from the CGSS2015. Int. J. Environ. Res. Public Health 2020, 17, 2896. https://doi.org/10.3390/ijerph17082896
Sun Z, Li J. The Effects of Performance of Public Sector Health System on Quality of Life in China: Evidence from the CGSS2015. International Journal of Environmental Research and Public Health. 2020; 17(8):2896. https://doi.org/10.3390/ijerph17082896
Chicago/Turabian StyleSun, Zongfeng, and Jintao Li. 2020. "The Effects of Performance of Public Sector Health System on Quality of Life in China: Evidence from the CGSS2015" International Journal of Environmental Research and Public Health 17, no. 8: 2896. https://doi.org/10.3390/ijerph17082896
APA StyleSun, Z., & Li, J. (2020). The Effects of Performance of Public Sector Health System on Quality of Life in China: Evidence from the CGSS2015. International Journal of Environmental Research and Public Health, 17(8), 2896. https://doi.org/10.3390/ijerph17082896