A Long-Term Trend Study of Tuberculosis Incidence in China, India and United States 1992–2017: A Joinpoint and Age–Period–Cohort Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Statistical Analysis
2.2.1. Age–Period–Cohort Analysis
2.2.2. Joinpoint Regression Analysis
3. Results
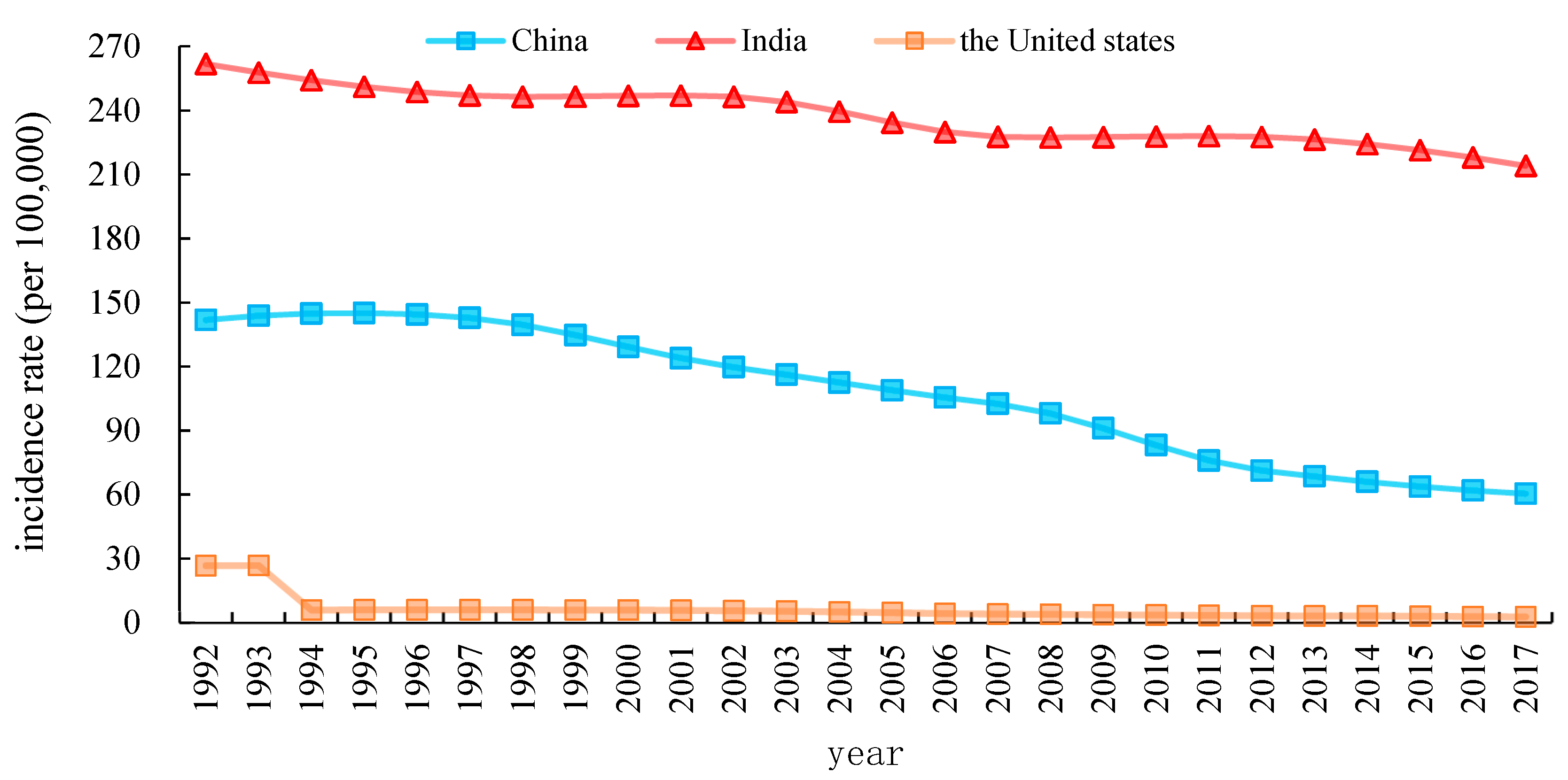
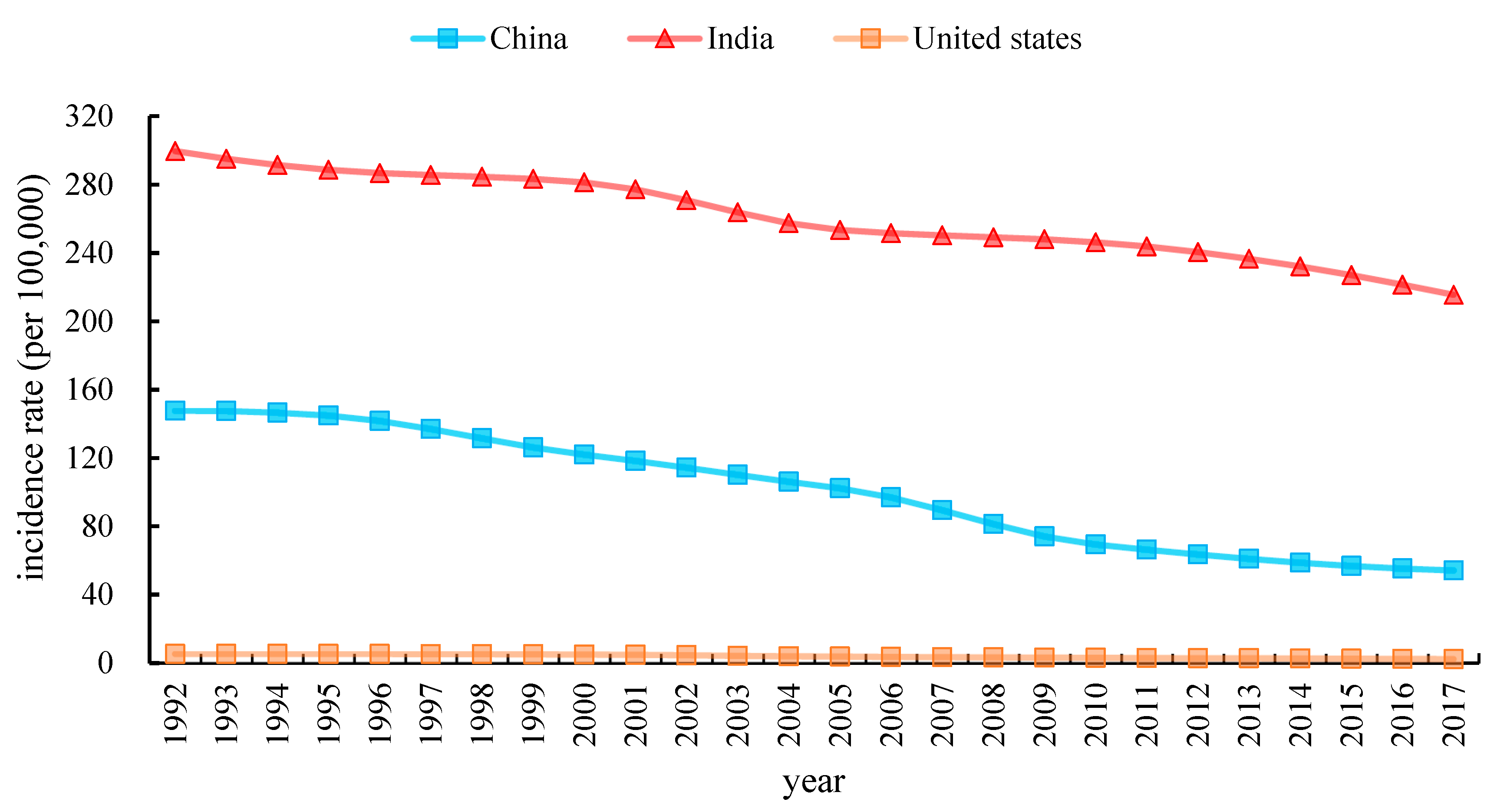
3.1. The Overall Trends in TB Incidence in China, India, and the United States
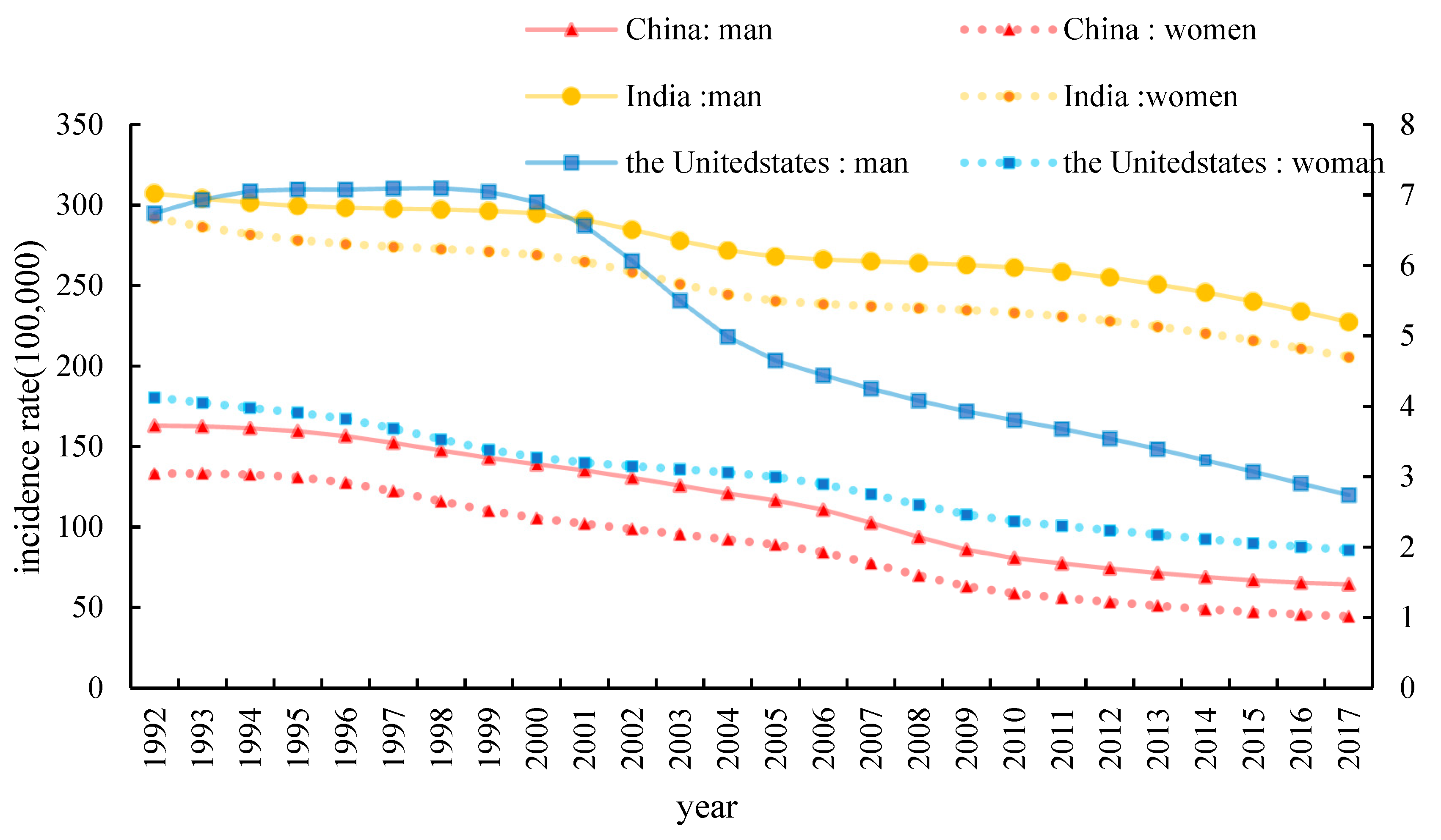
3.2. Descriptive Analysis of Gender of TB Incidence in China, India, and the United States
3.3. Trends in Age-Standardized TB Incidence Rates Using Joinpoint Regression Analysis
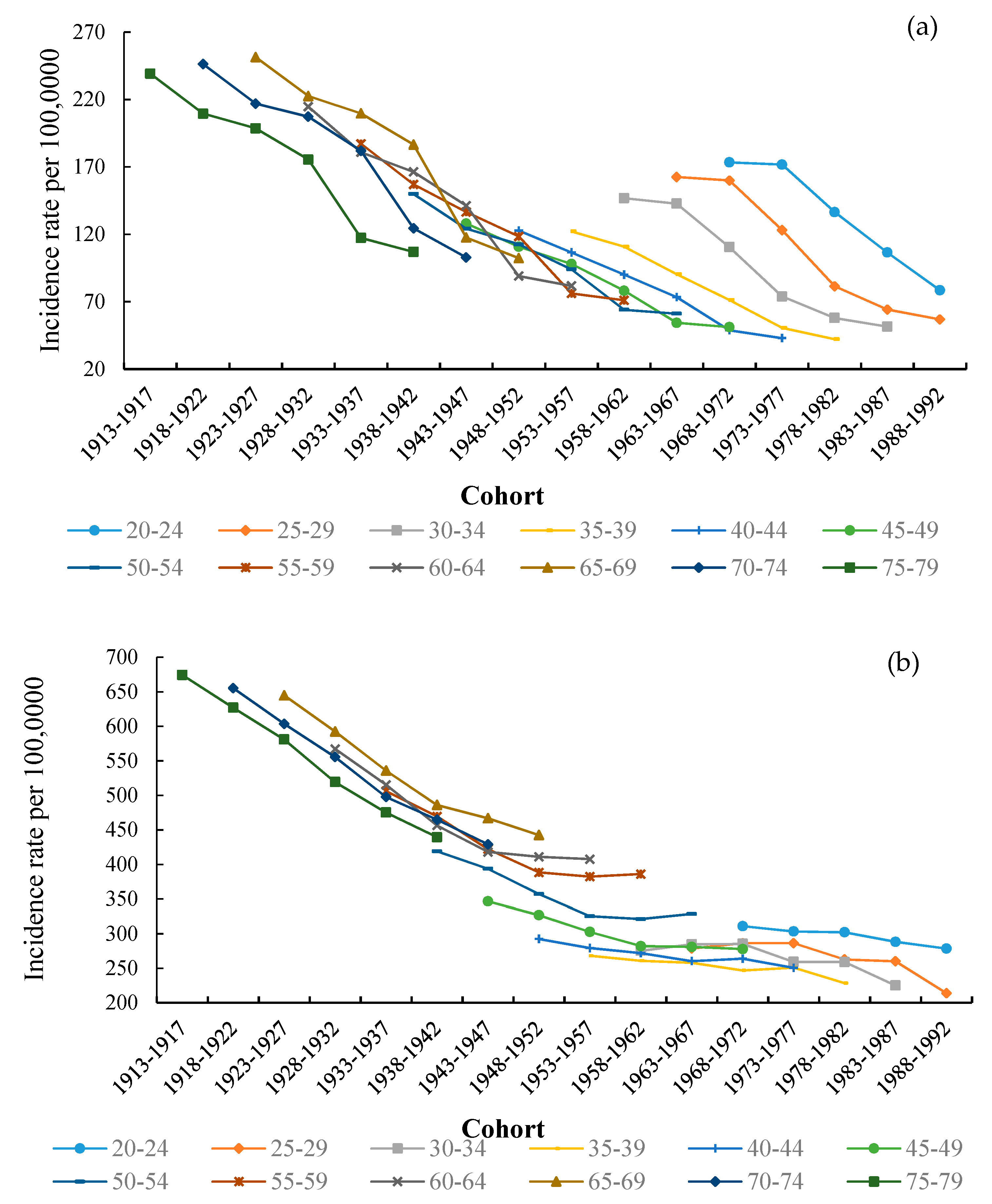
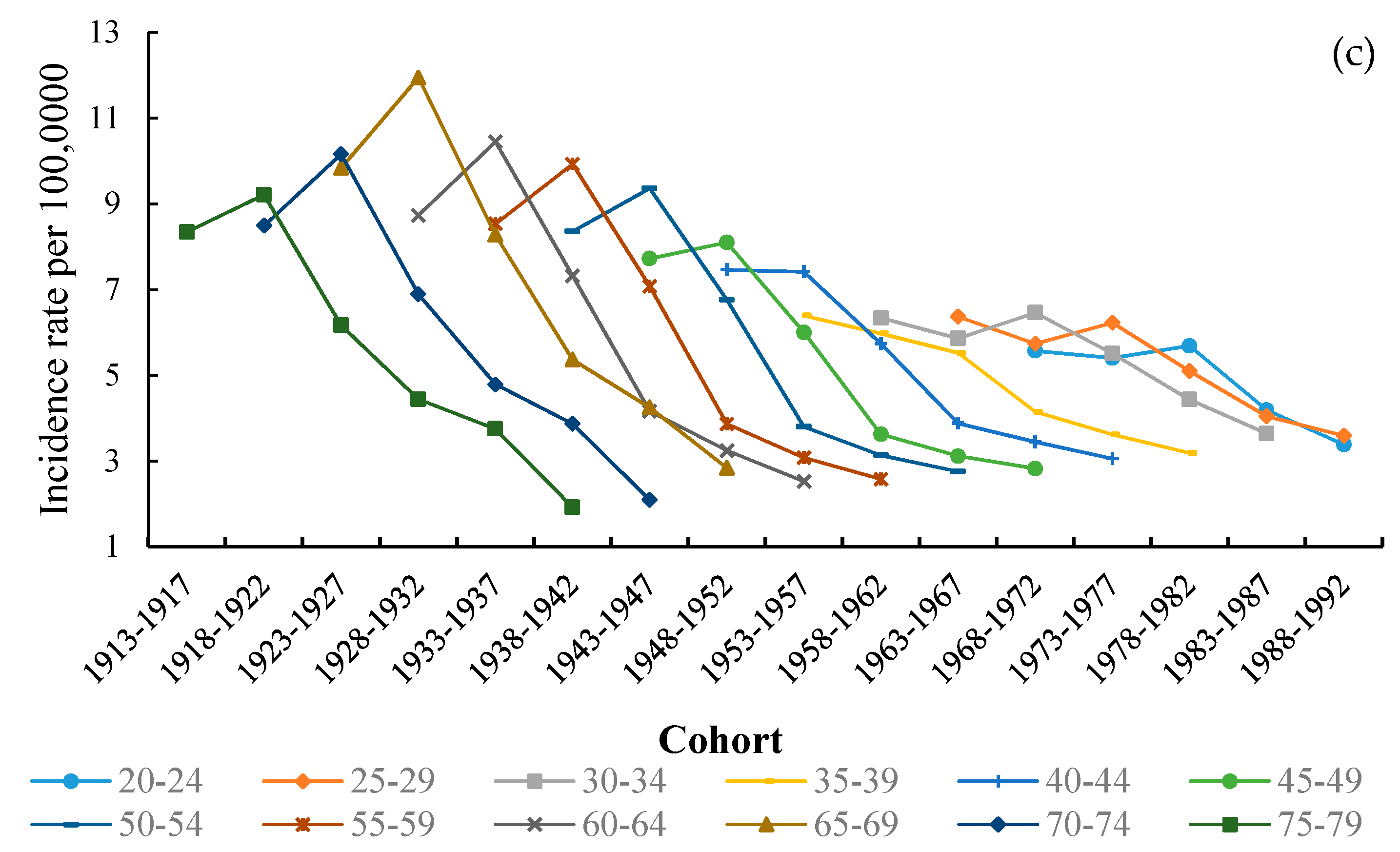
3.4. The Variation in Age, Period and Cohort on TB Incidence
3.5. The Age, Period, and Cohort Effects on TB Incidence
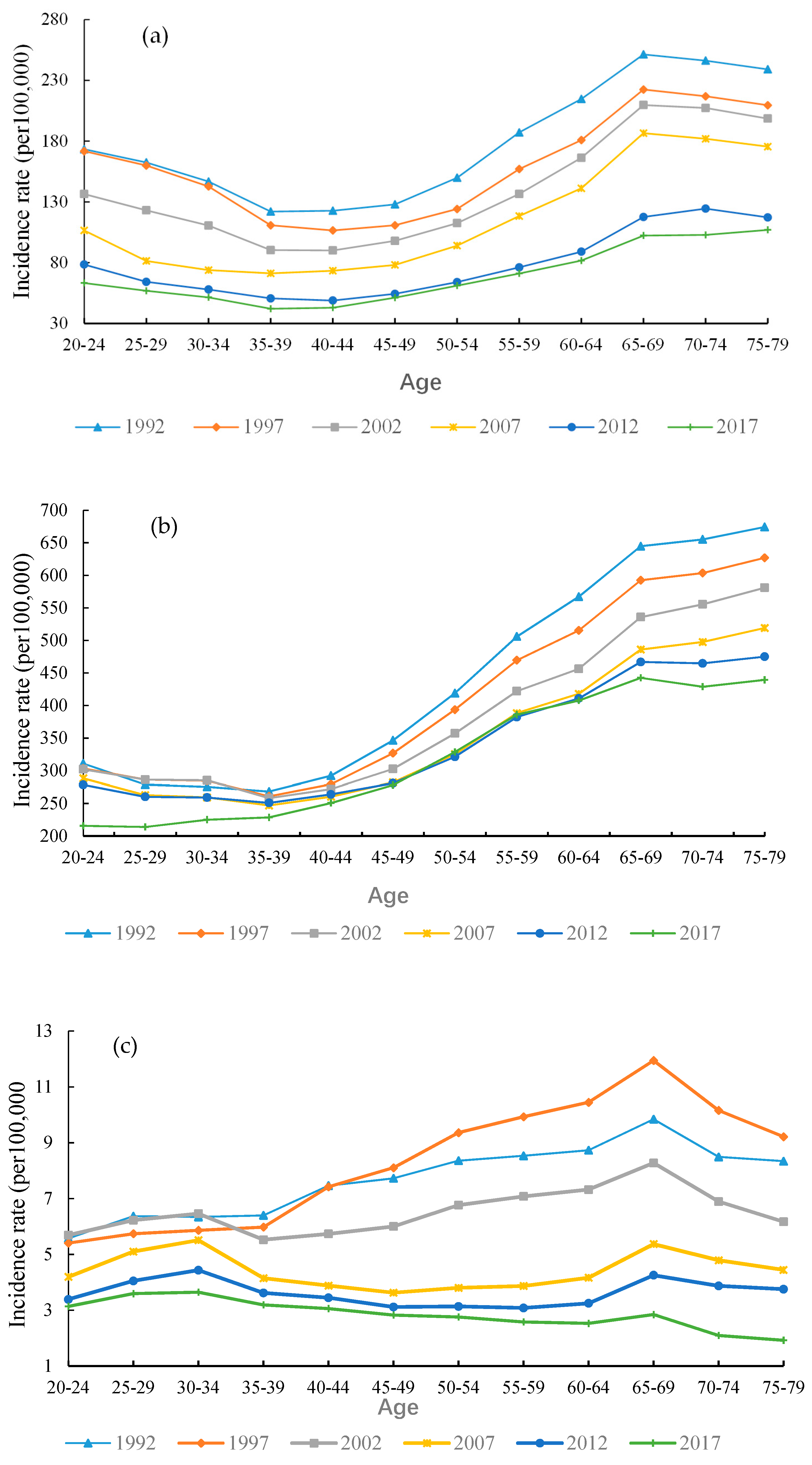
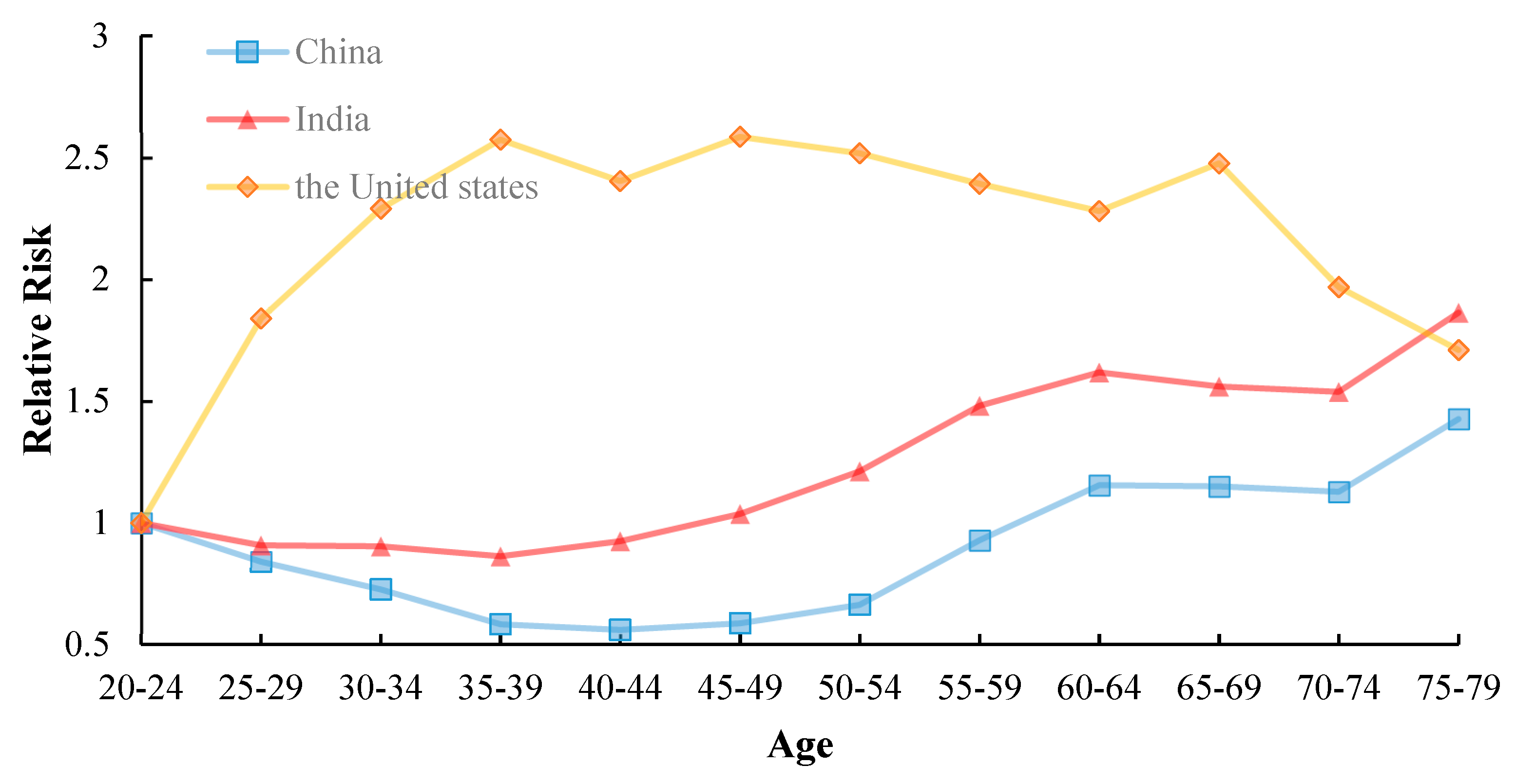
3.5.1. Age Effect
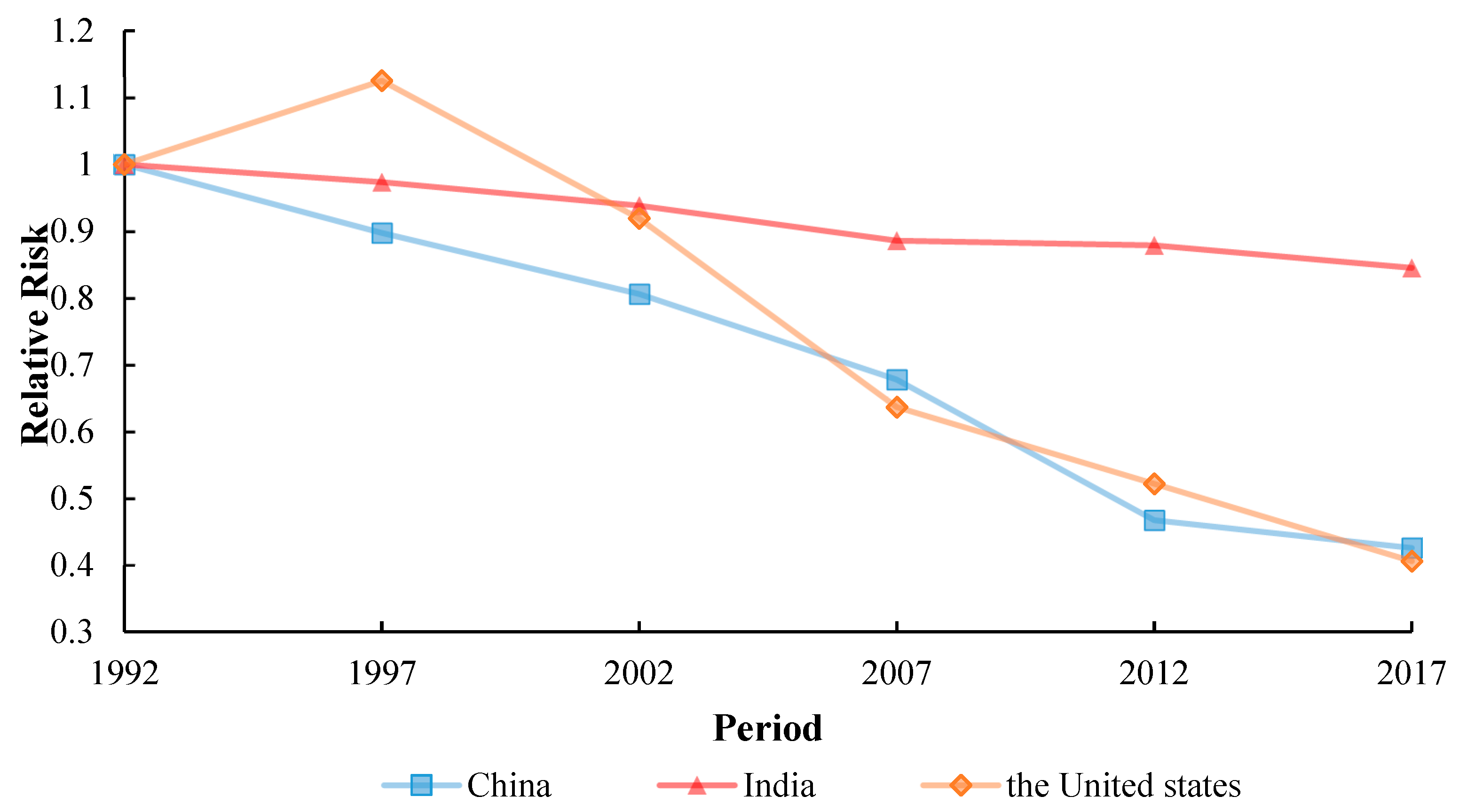
3.5.2. Period Effect
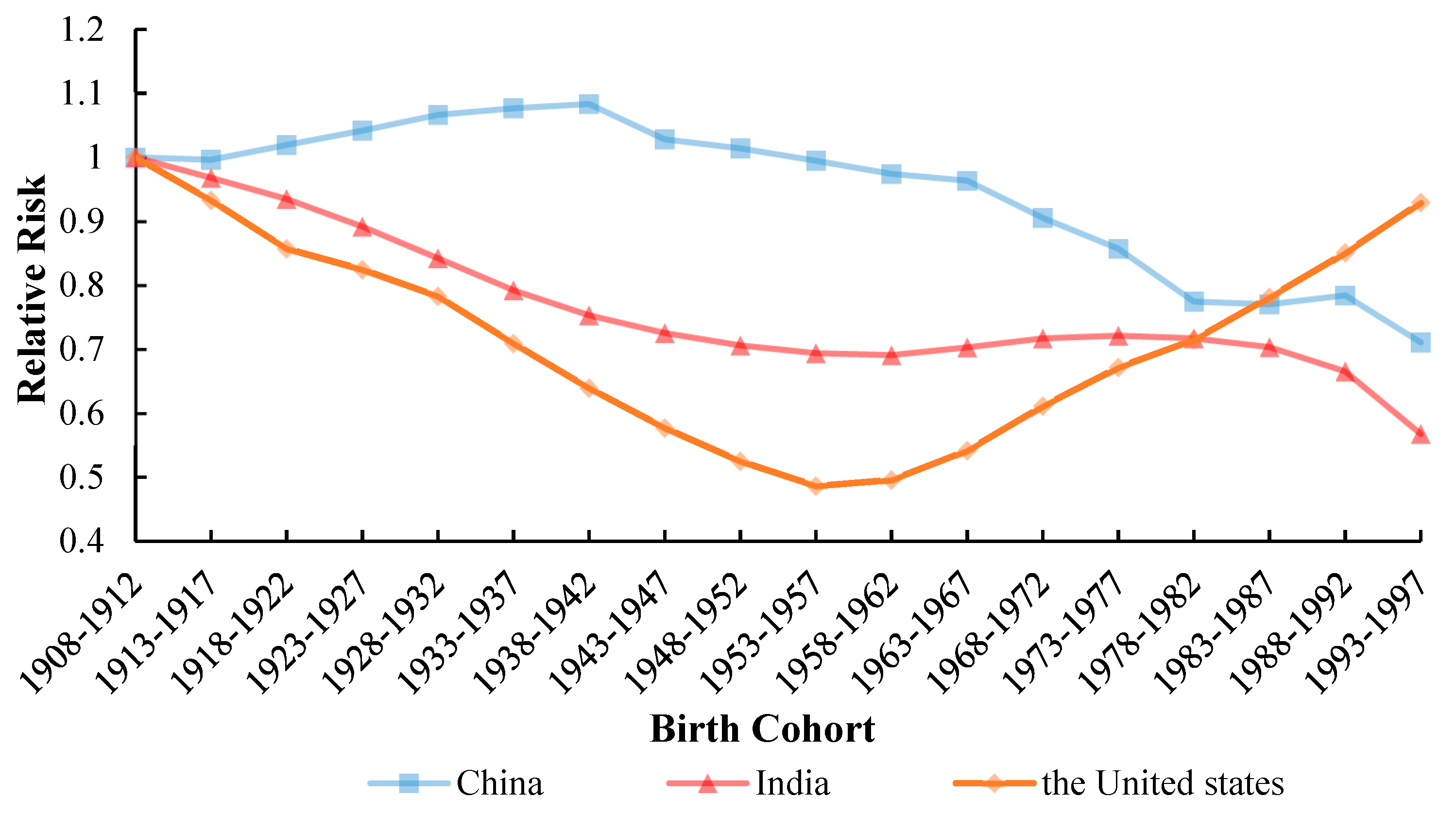
3.5.3. Cohort Effect
4. Discussion
4.1. Age Effect
4.2. Period Effect
4.3. Cohort Effect
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | China | India | The United States | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Coef (95%CI) | RR (95%CI) | P | Coef (95%CI) | RR (95%CI) | P | Coef (95%CI) | RR (95%CI) | P | |
| Intercept | 4.73 (4.70, 4.76) | 0 | 5.94 (5.93, 5.96) | 0 | 1.66 (1.52, 1.80) | 0 | |||
| Age | |||||||||
| 20–24 | 0.16 (0.08, 0.24) | 1 | 0.74 | −0.19 (−0.24, −0.14) | 1 | 0 | −0.76 (−1.21, −0.28) | 1 | 0 |
| 25–29 | −0.01 (−0.09, 0.06) | 0.84 (0.84, 0.84) | 0 | −0.29 (−0.34, −0.24) | 0.91 (0.91, 0.91) | 0 | −0.15 (−0.52, −0.22) | 1.84 (2.06, 1.64) | 0.42 |
| 30–34 | −0.16 (−0.24, −0.08) | 0.73 (0.72, 0.73) | 0 | −0.30 (−0.34, −0.25) | 0.90 (0.90, 0.90) | 0 | 0.07 (−0.29, 0.43) | 2.29 (2.60, 2.02) | 0.71 |
| 35–39 | −0.38 (−0.47, −0.29) | 0.58 (0.58, 0.59) | 0 | −0.34 (−0.39, −0.29) | 0.86 (0.86, 0.86) | 0 | 0.18 (−0.18, 0.55) | 2.57 (2.91, 2.27) | 0.32 |
| 40–44 | −0.42 (−0.51, −0.33) | 0.56 (0.55, 0.57) | 0 | −0.27 (−0.32, −0.22) | 0.93 (0.93, 0.92) | 0 | 0.12 (−0.27, 0.50) | 2.40 (2.66, 2.17) | 0.55 |
| 45–49 | −0.37 (−0.46, −0.28) | 0.59 (0.58, 0.59) | 0 | −0.16 (−0.21, 0.11) | 1.04 (1.04, 1.03) | 0 | 0.19 (−0.19, 0.57) | 2.59 (2.87, 2.33) | 0.33 |
| 50–54 | −0.25 (−0.33, −0.17) | 0.66 (0.66, 0.67) | 0.12 | 0.00 (−0.04, 0.04) | 1.21 (1.22, 1.21) | 0.94 | 0.16 (−0.22, 0.54) | 2.52 (2.80, 2.26) | 0.4 |
| 55–59 | −0.06 (−0.13, 0.02) | 0.80 (0.80, 0.80) | 0.02 | 0.15 (0.11, 0.19) | 1.41 (1.42, 1.40) | 0 | 0.18 (−0.19, 0.54) | 2.55 (2.88, 2.26) | 0.34 |
| 60–64 | 0.09 (0.02, 0.16) | 0.93 (0.94, 0.92) | 0 | 0.20 (0.16, 0.24) | 1.48 (1.50, 1.47) | 0 | 0.11 (−0.24, 0.46) | 2.39 (2.73, 2.10) | 0.53 |
| 65–69 | 0.30 (0.24, 0.37) | 1.15 (1.17, 1.14) | 0 | 0.29 (0.25, 0.32) | 1.62 (1.64, 1.60) | 0 | 0.06 (−0.28, 0.40) | 2.28 (2.64, 1.97) | 0.71 |
| 70–74 | 0.30 (0.24, 0.36) | 1.15 (1.17, 1.13) | 0 | 0.25 (0.22, 0.29) | 1.56 (1.58, 1.54) | 0 | 0.15 (−0.17, 0.46) | 2.48 (2.93, 2.10) | 0.37 |
| 75–79 | 0.28 (0.22, 0.34) | 1.13 (1.14, 1.11) | 0 | 0.24 (0.20, 0.27) | 1.54 (1.56, 1.52) | 0 | −0.08 (−0.42, 0.26) | 1.97 (2.27, 1.71) | 0.63 |
| period | |||||||||
| 1992 | 0.39 (0.35, 0.43) | 1 | 0 | 0.08 (0.06, 0.11) | 1 | 0 | 0.33 (0.13, 0.53) | 1 | 0 |
| 1997 | 0.28 (0.24, 0.32) | 0.90 (0.90, 0.90) | 0 | 0.06 (0.03, 0.08) | 0.97 (0.97, 0.97) | 0 | 0.45 (0.25, 0.64) | 1.13 (1.13, 1.12) | 0 |
| 2002 | 0.17 (0.13, 0.22) | 0.81 (0.80, 0.81) | 0.96 | 0.02 (0.00, 0.05) | 0.94 (0.94, 0.94) | 0.02 | 0.24 (0.03, 0.24) | 0.92 (0.91, 0.93) | 0.02 |
| 2007 | 0.00 (−0.05, 0.05) | 0.68 (0.67, 0.68) | 0 | −0.04 (−0.06, −0.01) | 0.89 (0.88, 0.89) | 0.32 | −0.12 (−0.37, 0.12) | 0.64 (0.61, 0.66) | 0.32 |
| 2012 | −0.37 (−0.43, −0.32) | 0.47 (0.46, 0.47) | 0 | −0.04 (−0.07, −0.02) | 0.88 (0.88, 0.88) | 0.02 | −0.32 (−0.58, −0.06) | 0.52 (0.49, 0.55) | 0.02 |
| 2017 | −0.47 (−0.52, −0.41) | 0.43 (0.42, 0.43) | 0.31 | 0.08 (−0.11, −0.06) | 0.85 (0.84, 0.85) | 0 | −0.57 (−0.87, −0.27) | 0.41 (0.37, 0.45) | 0 |
| cohort | |||||||||
| 1908–1912 | 0.06 (−0.06, 0.18) | 1 | 0.21 | 0.28 (0.21, 0.35) | 1 | 0 | 0.36 (−0.35, 1.06) | 1 | 0.32 |
| 1913–1917 | 0.06 (−0.03, 0.15) | 1.00 (1.03, 0.97) | 0.04 | 0.24 (0.19, 0.30) | 0.97 (0.99, 0.95) | 0 | 0.29 (−0.20, 0.77) | 0.93 (1.16, 0.75) | 0.25 |
| 1918–1922 | 0.08 (0.00, 0.16) | 1.02 (1.06, 0.98) | 0 | 0.21 (0.16, 0.25) | 0.94 (0.96, 0.91) | 0 | 0.20 (−0.20, 0.60) | 0.86 (1.16, 0.63) | 0.32 |
| 1923–1927 | 0.10 (0.03, 0.17) | 1.04 (1.10, 0.99) | 0 | 0.16 (0.12, 0.20) | 0.89 (0.92, 0.87) | 0 | 0.16 (−0.21, 0.53) | 0.82 (1.15, 0.59) | 0.39 |
| 1928–1932 | 0.13 (0.06, 0.19) | 1.07 (1.12, 1.01) | 0 | 0.10 (0.07, 0.14) | 0.84 (0.87, 0.82) | 0 | 0.11 (−0.25, 0.47) | 0.78 (1.11, 0.55) | 0.54 |
| 1933–1937 | 0.14 (0.07, 0.20) | 1.08 (1.14, 1.02) | 0 | 0.04 (0.01, 0.08) | 0.79 (0.82, 0.77) | 0.02 | 0.01 (−0.35, 0.37) | 0.71 (1.00, 0.50) | 0.95 |
| 1938–1942 | 0.14 (0.07, 0.22) | 1.08 (1.13, 1.03) | 0.03 | −0.01 (−0.05, 0.03) | 0.75 (0.77, 0.73) | 0.73 | −0.09 (−0.48, 0.29) | 0.64(0.88, 0.46) | 0.64 |
| 1943–1947 | 0.09 (0.01, 0.17) | 1.03 (1.07, 0.99) | 0.09 | −0.04 (−0.09, 0.00) | 0.74 (0.74, 0.71) | 0.05 | −0.20 (−0.60, 0.21) | 0.58 (0.78, 0.43) | 0.34 |
| 1948–1952 | 0.08 (−0.01, 0.16) | 1.01 (1.05, 0.98) | 0.23 | −0.07 (−0.12, −0.02) | 0.71 (0.72, 0.69) | 0 | −0.29 (−0.71, 0.13) | 0.52 (0.69, 0.40) | 0.18 |
| 1953–1957 | 0.06 (−0.04, 0.15) | 0.99 (1.02, 0.97) | 0.45 | −0.09 (−0.14, −0.04) | 0.69 (0.71, 0.68) | 0 | −0.37 (−0.80, 0.06) | 0.49 (0.64, 0.37) | 0.1 |
| 1958–1962 | 0.04 (−0.06, 0.13) | 0.97 (1.00, 0.95) | 0.59 | −0.09 (−0.14, −0.04) | 0.69 (0.70, 0.68) | 0 | −0.35 (−0.77, 0.07) | 0.50 (0.66, 0.37) | 0.11 |
| 1963–1967 | 0.02 (−0.06, 0.11) | 0.96 (0.99, 0.93) | 0.36 | −0.08 (−0.13, −0.03) | 0.70 (0.72, 0.69) | 0 | −0.26 (−0.66, 0.15) | 0.54 (0.73, 0.40) | 0.21 |
| 1968–1972 | −0.04 (−0.12,0.04) | 0.91 (0.94, 0.87) | 0.05 | −0.06 (−0.10, −0.01) | 0.72 (0.73, 0.70) | 0.02 | −0.14 (−0.53, 0.26) | 0.61 (0.83, 0.45) | 0.49 |
| 1973–1977 | −0.09 (−0.18, 0.00) | 0.86 (0.88, 0.83) | 0 | −0.05 (−0.10, 0.00) | 0.72 (0.73, 0.71) | 0.06 | −0.04 (−0.47, 0.38) | 0.67 (0.88, 0.51) | 0.84 |
| 1978–1982 | −0.19 (−0.30, −0.09) | 0.77 (0.78, 0.76) | 0 | −0.06 (−0.11, 0.00) | 0.72 (0.73, 0.71) | 0.06 | 0.02 (−0.47, 0.51) | 0.71 (0.88, 0.58) | 0.94 |
| 1983–1987 | −0.20 (−0.32, −0.08) | 0.77 (0.77, 0.77) | 0.02 | −0.08 (−0.14, −0.01) | 0.70 (0.71, 0.70) | 0.03 | 0.11 (−0.49, 0.70) | 0.78 (0.87, 0.70) | 0.72 |
| 1988–1992 | −0.18 (−0.33, −0.03) | 0.78 (0.76, 0.81) | 0.03 | −0.13 (−0.21, −0.05) | 0.67 (0.66, 0.67) | 0 | 0.19 (−0.59, 0.98) | 0.85 (0.79, 0.92) | 0.63 |
| 1993–1997 | −0.28 (−0.53, −0.03) | 0.71 (0.62, 0.81) | 0 | −0.29 (−0.43, −0.15) | 0.57 (0.53, 0.61) | 0 | 0.28 (−1.19, 1.75) | 0.93 (0.43, 2.00) | 0.71 |
| AIC | 7.68 | 8.78 | 4.35 | ||||||
| BIC | −175.66 | −180.23 | −189.74 | ||||||
| Deviance | 16.03 | 11.47 | 1.96 | ||||||
References
- World Health Organization. Global Tuberculosis Report 2013; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization. Global Tuberculosis Report 2016; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Centers for Disease Control and Prevention. Trends in tuberculosis—United States, 2008. Morb. Mortal. Wkly. Rep. 2009, 58, 249–253. [Google Scholar]
- Centers for Disease Control and Prevention. HIV Surveillance Special Report: HIV Risk, Prevention, and Testing Behaviors—National HIV Behavioral Surveillance System: Men Who Have Sex With Men; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2018. [Google Scholar]
- Stewart, R.J.; Tsang, C.A.; Pratt, R.H.; Price, S.F.; Langer, A.J. Tuberculosis—United States, 2017. Morb. Mortal. Wkly. Rep. 2018, 67, 317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doege, T.C. Tuberculosis mortality in the United States, 1900 to 1960. JAMA 1965, 192, 1045–1048. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.-T.; Chen, C.-J.; Lee, W.-C.; Luh, K.-T.; Hsieh, W.-C.; Lin, R.-S. Age-period-cohort analysis of pulmonary tuberculosis mortality in Taiwan: 1961 to 1990. J. Formos. Med. Assoc. Taiwan Yi Zhi 1994, 93, 657–662. [Google Scholar] [PubMed]
- Kyu, H.H.; Maddison, E.R.; Henry, N.J.; Mumford, J.E.; Barber, R.; Shields, C.; Brown, J.C.; Nguyen, G.; Carter, A.; Wolock, T.M. The global burden of tuberculosis: Results from the Global Burden of Disease Study 2015. Lancet Infect. Dis. 2018, 18, 261–284. [Google Scholar] [CrossRef] [Green Version]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Land, K.C. Age-Period-Cohort Analysis: New Models, Methods, and Empirical Applications; Chapman and Hall/CRC: London, UK, 2016. [Google Scholar]
- Yang, Y.; Fu, W.J.; Land, K.C. A methodological comparison of age-period-cohort models: The intrinsic estimator and conventional generalized linear models. Sociol. Methodol. 2004, 34, 75–110. [Google Scholar] [CrossRef]
- Li, Z.; Wang, P.; Gao, G.; Xu, C.; Chen, X. Age-period-cohort analysis of infectious disease mortality in urban-rural China, 1990–2010. Int. J. Equity Health 2016, 15, 55. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Schulhofer-Wohl, S.; Fu, W.J.; Land, K.C. The intrinsic estimator for age-period-cohort analysis: What it is and how to use it. Am. J. Sociol. 2008, 113, 1697–1736. [Google Scholar]
- Luo, L. Assessing validity and application scope of the intrinsic estimator approach to the age-period-cohort problem. Demography 2013, 50, 1945–1967. [Google Scholar]
- Clegg, L.X.; Hankey, B.F.; Tiwari, R.; Feuer, E.J.; Edwards, B.K. Estimating average annual per cent change in trend analysis. Stat. Med. 2009, 28, 3670–3682. [Google Scholar] [CrossRef] [Green Version]
- Wu, P.; Cowling, B.J.; Schooling, C.M.; Wong, I.O.; Johnston, J.M.; Leung, C.-C.; Tam, C.-M.; Leung, G.M. Age-period-cohort analysis of tuberculosis notifications in Hong Kong from 1961 to 2005. Thorax 2008, 63, 312–316. [Google Scholar] [CrossRef] [Green Version]
- Houweling, H.; Wiessing, L.G.; Hamers, F.F.; Termorshuizen, F.; Gill, O.N.; Sprenger, M. An age-period-cohort analysis of 50,875 AIDS cases among injecting drug users in Europe. Int. J. Epidemiol. 1999, 28, 1141–1148. [Google Scholar] [CrossRef] [Green Version]
- Verdecchia, A.; Mariotto, A.; Capocaccia, R.; Mariotti, S. An age and period reconstruction of the HIV epidemic in Italy. Int. J. Epidemiol. 1994, 23, 1027–1039. [Google Scholar] [CrossRef]
- Vynnycky, E.; Fine, P. The natural history of tuberculosis: The implications of age-dependent risks of disease and the role of reinfection. Epidemiol. Infect. 1997, 119, 183–201. [Google Scholar] [CrossRef]
- Cegielski, J.; McMurray, D. The relationship between malnutrition and tuberculosis: Evidence from studies in humans and experimental animals. Int. J. Tuberc. Lung Dis. 2004, 8, 286–298. [Google Scholar]
- Stevenson, C.R.; Forouhi, N.G.; Roglic, G.; Williams, B.G.; Lauer, J.A.; Dye, C.; Unwin, N. Diabetes and tuberculosis: The impact of the diabetes epidemic on tuberculosis incidence. BMC Public Health 2007, 7, 234. [Google Scholar] [CrossRef] [Green Version]
- Thomas, T.Y.; Rajagopalan, S. Tuberculosis and aging: A global health problem. Clin. Infect. Dis. 2001, 33, 1034–1039. [Google Scholar]
- Moutschen, M.; Scheen, A.; Lefebvre, P. Impaired immune responses in diabetes mellitus: Analysis of the factors and mechanisms involved, relevance to the increased susceptibility of diabetic patients to specific infections. Diabete Metab. 1992, 18, 187–201. [Google Scholar]
- Li, X. Fresh Blood in the Labor Market: Challenges and Rewards of China’s Returning Millennial Generation. Master’s Thesis, The University of San Francisco, San Francisco, CA, USA, March 2019. [Google Scholar]
- Fang, E.F.; Scheibye-Knudsen, M.; Jahn, H.J.; Li, J.; Ling, L.; Guo, H.; Zhu, X.; Preedy, V.; Lu, H.; Bohr, V.A. A research agenda for aging in China in the 21st century. Ageing Res. Rev. 2015, 24, 197–205. [Google Scholar] [CrossRef] [Green Version]
- Gavazzi, G.; Krause, K.-H. Ageing and infection. Lancet Infect. Dis. 2002, 2, 659–666. [Google Scholar] [CrossRef]
- Zhu, S.; Xia, L.; Yu, S.; Chen, S.; Zhang, J. The burden and challenges of tuberculosis in China: Findings from the Global Burden of Disease Study 2015. Sci. Rep. 2017, 7, 14601. [Google Scholar] [CrossRef] [Green Version]
- Lönnroth, K.; Williams, B.G.; Stadlin, S.; Jaramillo, E.; Dye, C. Alcohol use as a risk factor for tuberculosis—A systematic review. BMC Public Health 2008, 8, 289. [Google Scholar] [CrossRef] [Green Version]
- Rehm, J.; Samokhvalov, A.V.; Neuman, M.G.; Room, R.; Parry, C.; Lönnroth, K.; Patra, J.; Poznyak, V.; Popova, S. The association between alcohol use, alcohol use disorders and tuberculosis (TB). A systematic review. BMc Public Health 2009, 9, 450. [Google Scholar] [CrossRef]
- World Health Organization. WHO TB Burden Estimates. Available online: https://www.who.int/tb/country/data/download/en/ (accessed on 5 October 2016).
- Imtiaz, S.; Shield, K.D.; Roerecke, M.; Samokhvalov, A.V.; Lönnroth, K.; Rehm, J. Alcohol consumption as a risk factor for tuberculosis: Meta-analyses and burden of disease. Eur. Respir. J. 2017, 50. [Google Scholar] [CrossRef]
- Iqbal, S.A.; Winston, C.A.; Bardenheier, B.H.; Armstrong, L.R.; Navin, T.R. Age-period-cohort analyses of tuberculosis incidence rates by Nativity, United States, 1996–2016. Am. J. Public Health 2018, 108, S315–S320. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Reported Tuberculosis in the United States, 2014; US Department of Health and Human Services: Atlanta, GA, USA, 2015.
- Qian, X.; Nguyen, D.T.; Lyu, J.; Albers, A.E.; Bi, X.; Graviss, E.A. Risk factors for extrapulmonary dissemination of tuberculosis and associated mortality during treatment for extrapulmonary tuberculosis. Emerg. Microbes Infect. 2018, 7, 1–14. [Google Scholar] [CrossRef]
- Gonzalez, O.; Adams, G.; Teeter, L.; Bui, T.; Musser, J.M.; Graviss, E. Extra-pulmonary manifestations in a large metropolitan area with a low incidence of tuberculosis. Int. J. Tuberc. Lung Dis. 2003, 7, 1178–1185. [Google Scholar]
- Wang, L.; Liu, J.; Chin, D.P. Progress in tuberculosis control and the evolving public-health system in China. Lancet, 2007; 369, 691–696. [Google Scholar] [CrossRef]
- Wen, J. Government work report. In Proceedings of the National People’s Congress Meeting, Beijing, China, 5 March 2006. [Google Scholar]
- Wang, H.; Gusmano, M.K.; Cao, Q. An evaluation of the policy on community health organizations in China: Will the priority of new healthcare reform in China be a success? Health Policy 2011, 99, 37–43. [Google Scholar] [CrossRef]
- Shen, G. Changes from traditional solid fuels to clean household energies—Opportunities in emission reduction of primary PM2.5 from residential cookstoves in China. Biomass Bioenergy 2016, 86, 28–35. [Google Scholar] [CrossRef]
- Cowling, K.; Dandona, R.; Dandona, L. Improving the estimation of the tuberculosis burden in India. Bull. World Health Organ. 2014, 92, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Khatri, G.; Frieden, T.R. Controlling tuberculosis in India. N. Engl. J. Med. 2002, 347, 1420–1425. [Google Scholar] [CrossRef]
- Global, W. Tuberculosis Report 2017; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Brudney, K.; Dobkin, J. Resurgent tuberculosis in New York City: Human immunodeficiency virus, homelessness, and the decline of tuberculosis control programs. J. Public Health Policy 1992, 13, 435–450. [Google Scholar] [CrossRef]
- Manthey, J.; Shield, K.D.; Rylett, M.; Hasan, O.S.; Probst, C.; Rehm, J. Global alcohol exposure between 1990 and 2017 and forecasts until 2030: A modelling study. Lancet 2019, 393, 2493–2502. [Google Scholar] [CrossRef]
- Chaves, F. Tuberculosis trends in Madrid, 1994–2003: Impact of immigration and HIV infection. Off. J. Int. Union Against Tuberc. Lung Dis. 2006, 10, 550. [Google Scholar]
- Winston, C.A.; Navin, T.R. Birth cohort effect on latent tuberculosis infection prevalence, United States. BMC Infect. Dis. 2010, 10, 206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, W.; Long, H.; Li, J.; Tao, S.; Zheng, P.; Tang, S.; Abdullah, A.S. Delivery of public health services by community health workers (CHWs) in primary health care settings in China: A systematic review (1996–2016). Glob. Health Res. Policy 2018, 3, 18. [Google Scholar] [CrossRef]
- Wang, F.; Liang, Y. China’s rural cooperative medical scheme: A type of health insurance or a type of health cooperative? Prim. Health Care Res. Dev. 2017, 18, 194–199. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Mauzerall, D.L.; Zhu, T.; Liang, S.; Ezzati, M.; Remais, J.V. Environmental health in China: Progress towards clean air and safe water. Lancet 2010, 375, 1110–1119. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Yang, J.; Wang, S. China has reached the Lewis turning point. China Econ. Rev. 2011, 22, 542–554. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Fu, H. China’s health care system reform: Progress and prospects. Int. J. Health Plan. Manag. 2017, 32, 240–253. [Google Scholar] [CrossRef] [PubMed]
- Oxlade, O.; Murray, M. Tuberculosis and poverty: Why are the poor at greater risk in India? PLoS ONE 2012, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padmapriyadarsini, C.; Shobana, M.; Lakshmi, M.; Beena, T.; Swaminathan, S. Undernutrition & tuberculosis in India: Situation analysis & the way forward. Indian J. Med Res. 2016, 144, 11. [Google Scholar]
- Marimuthu, P. Tuberculosis prevalence and socio-economic differentials in the slums of four metropolitan cities of India. Indian J. Tuberc. 2016, 63, 167–170. [Google Scholar] [CrossRef]
- Prasad, R.; Suryakant, R.G.; Singhal, S.; Dawar, R.; Agarwal, G. A case-control study of tobacco smoking and tuberculosis in India. Ann. Thorac. Med. 2009, 4, 208. [Google Scholar] [CrossRef]
- Dasgupta, P.R.; Jain, M.K.; John, T.J. Government response to HIV/AIDS in India. AIDS (Lond. Engl.) 1994, 8, S83–S90. [Google Scholar]
- Zevallos, M.; Justman, J.E. Tuberculosis in the elderly. Clin. Geriatr. Med. 2003, 19, 121–138. [Google Scholar] [CrossRef]
- Frost, W.H. How much control of tuberculosis? Am. J. Public Health Nations Health 1937, 27, 759. [Google Scholar] [CrossRef]
- MacIntyre, C.; Plant, A. Preventability of incident cases of tuberculosis in recently exposed contacts. Int. J. Tuberc. Lung Dis. 1998, 2, 56–61. [Google Scholar]
- Behr, M.A.; Hopewell, P.C.; Antonio Paz, E.; Masae Kawamura, L.; Schecter, G.F.; Small, P.M. Predictive value of contact investigation for identifying recent transmission of Mycobacterium tuberculosis. Am. J. Respir. Crit. Care Med. 1998, 158, 465–469. [Google Scholar] [CrossRef]
- Lobato, M.N.; Wang, Y.-C.; Becerra, J.E.; Simone, P.M.; Castro, K.G. Improved program activities are associated with decreasing tuberculosis incidence in the United States. Public Health Rep. 2006, 121, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Van Zyl Smit, R.N.; Pai, M.; Yew, W.-W.; Leung, C.; Zumla, A.; Bateman, E.; Dheda, K. Global lung health: The colliding epidemics of tuberculosis, tobacco smoking, HIV and COPD. Eur. Respir. J. 2010, 35, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Webb, G.B. The effect of the inhalation of cigarette smoke on the lungs: A clinical study. Am. Rev. Tuberc. 1918, 2, 25–27. [Google Scholar]
- Slama, K.; Chiang, C.; Enarson, D.; Hassmiller, K.; Fanning, A.; Gupta, P.; Ray, C. Tobacco and tuberculosis: A qualitative systematic review and meta-analysis. Int. J. Tuberc. Lung Dis. 2007, 11, 1049–1061. [Google Scholar] [PubMed]
- Lin, H.-H.; Ezzati, M.; Murray, M. Tobacco smoke, indoor air pollution and tuberculosis: A systematic review and meta-analysis. PLoS Med. 2007, 4. [Google Scholar] [CrossRef]
- Bates, M.N.; Khalakdina, A.; Pai, M.; Chang, L.; Lessa, F.; Smith, K.R. Risk of tuberculosis from exposure to tobacco smoke: A systematic review and meta-analysis. Arch. Intern. Med. 2007, 167, 335–342. [Google Scholar] [CrossRef] [Green Version]
- Pai, M.; Mohan, A.; Dheda, K.; Leung, C.C.; Yew, W.W.; Christopher, D.J.; Sharma, S.K. Lethal interaction: The colliding epidemics of tobacco and tuberculosis. Expert Rev. Anti-Infect. Ther. 2007, 5, 385–391. [Google Scholar] [CrossRef]
- Menzies, N.A.; Cohen, T.; Hill, A.N.; Yaesoubi, R.; Galer, K.; Wolf, E.; Marks, S.M.; Salomon, J.A. Prospects for tuberculosis elimination in the United States: Results of a transmission dynamic model. Am. J. Epidemiol. 2018, 187, 2011–2020. [Google Scholar] [CrossRef]
- Menzies, N.; Hill, A.; Cohen, T.; Salomon, J. The impact of migration on tuberculosis in the United States. Int. J. Tuberc. Lung Dis. 2018, 22, 1392–1403. [Google Scholar] [CrossRef]
- Onorato, I. Tuberculosis outbreaks in the United States. Int. J. Tuberc. Lung Dis. 2000, 4, 121–126. [Google Scholar]









| Segments | China | India | The United States | |||
|---|---|---|---|---|---|---|
| Year | APC * (95% CI) | Year | APC * (95% CI) | Year | APC * (95% CI) | |
| ASIR | ||||||
| trend1 | 1992–1995 | −0.3 (−0.9, 0.2) | 1992−1995 | −1.3 * (−1.5, −1.0) | 1992–1995 | 0.4 (−0.5, 1.2) |
| trend2 | 1995–2006 | −3.5 * (−3.6, −3.5) | 1995−2000 | −0.4 * (−0.6, −0.2) | 1995–2000 | −1.3 (−1.8, −0.8) |
| trend3 | 2006–2009 | −9.2 * (−10.1, −8.3) | 2000−2005 | −2.1 * (−2.3, −1.9) | 2000–2005 | −5.6 * (−6.1, −5.1) |
| trend4 | 2009–2013 | −4.8 * (−5.3, −4.3) | 2005−2008 | −0.6 * (−0.7, −0.5) | 2005–2012 | −4.4 (−5.9, −2.9) |
| trend5 | 2013–2017 | −2.8 (−3.1, −2.5) | 2008−2017 | −2.3 * (−2.4, −2.1) | 2012–2017 | −3.7 (−3.8, −3.6) |
| AAPC * | 1992–2017 | −4.0 * (−4.1, −3.8) | 1992−2017 | −1.3 * (−1.4, −1.2) | 1992–2017 | −3.2 * (−3.4, −3.0) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, Y.; Shen, H.; Wang, F.; Wen, H.; Zeng, Z.; Wang, Y.; Yu, C. A Long-Term Trend Study of Tuberculosis Incidence in China, India and United States 1992–2017: A Joinpoint and Age–Period–Cohort Analysis. Int. J. Environ. Res. Public Health 2020, 17, 3334. https://doi.org/10.3390/ijerph17093334
Cui Y, Shen H, Wang F, Wen H, Zeng Z, Wang Y, Yu C. A Long-Term Trend Study of Tuberculosis Incidence in China, India and United States 1992–2017: A Joinpoint and Age–Period–Cohort Analysis. International Journal of Environmental Research and Public Health. 2020; 17(9):3334. https://doi.org/10.3390/ijerph17093334
Chicago/Turabian StyleCui, Yiran, Hui Shen, Fang Wang, Haoyu Wen, Zixin Zeng, Yafeng Wang, and Chuanhua Yu. 2020. "A Long-Term Trend Study of Tuberculosis Incidence in China, India and United States 1992–2017: A Joinpoint and Age–Period–Cohort Analysis" International Journal of Environmental Research and Public Health 17, no. 9: 3334. https://doi.org/10.3390/ijerph17093334
APA StyleCui, Y., Shen, H., Wang, F., Wen, H., Zeng, Z., Wang, Y., & Yu, C. (2020). A Long-Term Trend Study of Tuberculosis Incidence in China, India and United States 1992–2017: A Joinpoint and Age–Period–Cohort Analysis. International Journal of Environmental Research and Public Health, 17(9), 3334. https://doi.org/10.3390/ijerph17093334