Food Insecurity Is Associated with Depression among a Vulnerable Workforce: Early Care and Education Workers


Abstract
:1. Introduction
2. Methods
2.1. Participants, Recruitment, and Data Collection
2.1.1. Key Exposure Variable
2.1.2. Key Outcome Variable
2.1.3. Effect Measure Modifiers and Confounders
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coleman-Jensen, A.; Rabbitt, M.P.; Gregory, C.A.; Singh, A. Household Food Security in the United States in 2019. Economic Research Service, 2020. Available online: https://www.ers.usda.gov/publications/pub-details/?pubid=99281 (accessed on 27 December 2020).
- Heflin, C.M.; Ziliak, J.P. Food Insufficiency, Food Stamp Participation, and Mental Health. Soc. Sci. Q. 2008, 89, 706–727. [Google Scholar] [CrossRef] [Green Version]
- Leung, C.W.; Epel, E.S.; Willett, W.C.; Rimm, E.B.; Laraia, B.A. Household Food Insecurity Is Positively Associated with Depression among Low-Income Supplemental Nutrition Assistance Program Participants and Income-Eligible Nonparticipants. J. Nutr. 2015, 145, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Noonan, K.; Corman, H.; Reichman, N.E. Effects of maternal depression on family food insecurity. Econ. Hum. Biol. 2016, 22, 201–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heflin, C.M.; Siefert, K.; Williams, D.R. Food insufficiency and women’s mental health: Findings from a 3-year panel of welfare recipients. Soc. Sci. Med. 2005, 61, 1971–1982. [Google Scholar] [CrossRef]
- Leung, C.W.; Stewart, A.L.; Portela-Parra, E.T.; Adler, N.E.; Laraia, B.A.; Epel, E.S. Understanding the Psychological Distress of Food Insecurity: A Qualitative Study of Children’s Experiences and Related Coping Strategies. J. Acad. Nutr. Diet. 2020, 120, 395–403. [Google Scholar] [CrossRef] [Green Version]
- Linnan, L.; Arandia, G.; Bateman, L.A.; Vaughn, A.; Smith, N.; Ward, D. The Health and Working Conditions of Women Employed in Child Care. Int. J. Environ. Res. Public Health 2017, 14, 283. [Google Scholar] [CrossRef]
- Otten, J.J.; Bradford, V.A.; Stover, B.; Hill, H.D.; Osborne, C.; Getts, K.; Seixas, N. The Culture of Health in Early Care and Education: Workers’ Wages, Health, and Job Characteristics. Health Aff. (Proj. Hope) 2019, 38, 709–720. [Google Scholar] [CrossRef] [Green Version]
- McKelvey, L.; Forsman, A.; Morrison-Ward, J. Arkansas Workforce Study: Instructional Staff in Child Care & Early Childhood Education, 2017. Good to Great. 2017. Available online: https://familymedicine.uams.edu/wp-content/uploads/sites/57/2018/04/Staff-Workforce-Study-Report_FINAL.pdf (accessed on 27 December 2020).
- Morrissey, T. The Effects of Early Care and Education on Children’s Health. Health Affairs. 2019. Available online: https://www.healthaffairs.org/do/10.1377/hpb20190325.519221/full/ (accessed on 27 December 2020).
- Maynard, M.; Andrade, L.; Packull-McCormick, S.; Perlman, C.M.; Leos-Toro, C.; Kirkpatrick, S.I. Food Insecurity and Mental Health among Females in High-Income Countries. Int. J. Environ. Res. Public Health 2018, 15, 1424. [Google Scholar] [CrossRef] [Green Version]
- Arenas, D.J.; Thomas, A.; Wang, J.; DeLisser, H.M. A Systematic Review and Meta-analysis of Depression, Anxiety, and Sleep Disorders in US Adults with Food Insecurity. J. Gen. Intern. Med. 2019, 1–9. [Google Scholar] [CrossRef]
- Jessiman-Perreault, G.; McIntyre, L. The household food insecurity gradient and potential reductions in adverse population mental health outcomes in Canadian adults. Ssm-Popul. Health 2017, 3, 464–472. [Google Scholar] [CrossRef]
- Loopstra, R. Interventions to address household food insecurity in high-income countries. Proc. Nutr. Soc. 2018, 77, 270–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gundersen, C.; Ziliak, J.P. Food Insecurity and Health Outcomes. Health Aff. (Proj. Hope) 2015, 34, 1830–1839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brostow, D.; Gunzburger, E.; Abbate, L.; Brenner, L.; Thomas, K. Mental Illness, Not Weight Status, Predicts Increased Odds of Food Insecurity in the Health and Retirement Study (OR02-06-19). Curr. Dev. Nutr. 2019, 3. [Google Scholar] [CrossRef]
- Kim, K.; Frongillo, E.A. Participation in Food Assistance Programs Modifies the Relation of Food Insecurity with Weight and Depression in Elders. J. Nutr. 2007, 137, 1005–1010. [Google Scholar] [CrossRef] [Green Version]
- Tuthill, E.L.; Sheira, L.A.; Palar, K.; Frongillo, E.A.; Wilson, T.E.; Adedimeji, A.; Merenstein, D.; Cohen, M.H.; Wentz, E.L.; Adimora, A.A.; et al. Persistent Food Insecurity Is Associated with Adverse Mental Health among Women Living with or at Risk of HIV in the United States. J. Nutr. 2019, 149, 240–248. [Google Scholar] [CrossRef]
- Dean, J.; Keshavan, M. The neurobiology of depression: An integrated view. Asian J. Psychiatry 2017, 27, 101–111. [Google Scholar] [CrossRef]
- Rao, T.S.S.; Asha, M.R.; Ramesh, B.N.; Rao, K.S.J. Understanding nutrition, depression and mental illnesses. Indian J. Psychiatry 2008, 50, 77–82. [Google Scholar]
- Whitebook, M.; McLean, C.; Austin, L.J.E.; Edwards, B. Early Childhood Workforce Index 2018. In Center for the Study of Child Care Employment; University of California: Berkeley, CA, USA, 2018. [Google Scholar]
- Lessard, L.M.; Wilkins, K.; Rose-Malm, J.; Mazzocchi, M.C. The health status of the early care and education workforce in the USA: A scoping review of the evidence and current practice. Public Health Rev. 2020, 41, 2. [Google Scholar] [CrossRef]
- Mongeau, L. Time to Change How We Think about Early Education, International Study Finds. Available online: https://hechingerreport.org/time-to-change-how-we-think-about-early-education-international-study-finds/ (accessed on 4 December 2020).
- Bertram, T.; Pascal, C. Early Childhood Policies and Systems in Eight Countries: Findings from IEA’s Early Childhood Education Study; Springer Open: Cham, Switzerland, 2016. [Google Scholar]
- Whitaker, R.C.; Becker, B.D.; Herman, A.N.; Gooze, R.A. The Physical and Mental Health of Head Start Staff: The Pennsylvania Head Start Staff Wellness Survey, 2012. Prev. Chronic Dis. 2013, 10, E181. [Google Scholar] [CrossRef] [Green Version]
- Cumming, T. Early Childhood Educators’ Well-Being: An Updated Review of the Literature. Early Child. Educ. J. 2017, 45, 583–593. [Google Scholar] [CrossRef]
- Loh, I.H.; Oddo, V.M.; Otten, J. Food Insecurity Is Associated with Depression among a Vulnerable Workforce: Early Care and Education Workers. Curr. Dev. Nutr. 2020, 4, 228. [Google Scholar] [CrossRef]
- King County Council. King County Technical Appendix B to the 2012 Comprehensive Plan: Housing. 2016. Available online: https://www.kingcounty.gov/~/media/Council/documents/CompPlan/2016/2016-0155/AppendixBHousing.ashx?la=en (accessed on 27 December 2020).
- Department of Agriculture, Economic Research Service. U.S. Household Food Security Survey Module: Six-Item Short Form. Available online: https://www.ers.usda.gov/media/8282/short2012.pdf (accessed on 4 December 2020).
- Eaton, W.W.; Smith, C.; Ybarra, M.; Muntaner, C.; Tien, A. Center for Epidemiological Depression Scale: Review and Revision (CESD and CESD-R); Maruish, M.E., Ed.; The Use of Psychological Testing for Treatment Planning and Outcomes Assessment; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2004; pp. 363–377. [Google Scholar]
- Van Dam, N.T.; Earleywine, M. Validation of the Center for Epidemiologic Studies Depression Scale—Revised (CESD-R): Pragmatic depression assessment in the general population. Psychiatry Res. 2011, 186, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Okechukwu, C.A.; El Ayadi, A.M.; Tamers, S.L.; Sabbath, E.L.; Berkman, L. Household Food Insufficiency, Financial Strain, Work–Family Spillover, and Depressive Symptoms in the Working Class: The Work, Family, and Health Network Study. Am. J. Public Health 2012, 102, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Glymour, M.M. 16. Using Causal Diagrams to Understand Common Problems in Social Epidemiology; Methods in Social Epidemiology: San Francisco, CA, USA, 2006; pp. 393–428. Available online: http://publicifsv.sund.ku.dk/~nk/epiF14/Glymour_DAGs.pdf (accessed on 27 December 2020).
- National Institute of Mental Health Major Depression. Available online: https://www.nimh.nih.gov/health/statistics/major-depression.shtml (accessed on 27 December 2020).
- Montgomery, M.J.; Lu, D.J.; Ratliff, M.S.; Mezuk, D.B. Food Insecurity and Depression among Adults with Diabetes: Results from the National Health and Nutrition Examination Survey (NHANES). Diabetes Educ. 2017, 43, 260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silverman, J.; Krieger, J.; Kiefer, M.; Hebert, P.; Robinson, J.; Nelson, K. The Relationship between Food Insecurity and Depression, Diabetes Distress and Medication Adherence among Low-Income Patients with Poorly-Controlled Diabetes. J. Gen. Intern. Med. 2015, 30, 1476–1480. [Google Scholar] [CrossRef] [PubMed]
- Oddo, V.M.; Mabli, J. Association of Participation in the Supplemental Nutrition Assistance Program and Psychological Distress. Am. J. Public Health 2015, 105, e30–e35. [Google Scholar] [CrossRef] [PubMed]
- Texas Health and Human Services SNAP Food Benefits. Available online: https://hhs.texas.gov/services/food/snap-food-benefits (accessed on 27 December 2020).
- Washington State Legislature WAC 388-444-0030. Available online: https://app.leg.wa.gov/WAC/default.aspx?cite=388-444-0030 (accessed on 27 December 2020).
- Keith-Jennings, B.; Llobrera, J.; Dean, S. Links of the Supplemental Nutrition Assistance Program with Food Insecurity, Poverty, and Health: Evidence and Potential. Am. J. Public Health (1971) 2019, 109, 1636–1640. [Google Scholar] [CrossRef]
- Gaines-Turner, T.; Simmons, J.C.; Chilton, M. Recommendations From SNAP Participants to Improve Wages and End Stigma. Am. J. Public Health (1971) 2019, 109, 1664–1667. [Google Scholar] [CrossRef]
- Alberdi, G.; McNamara, A.; Lindsay, K.; Scully, H.; Horan, M.; Gibney, E.; McAuliffe, F. The association between childcare and risk of childhood overweight and obesity in children aged 5 years and under: A systematic review. Eur. J. Pediatr. 2016, 175, 1277–1294. [Google Scholar] [CrossRef]
- Kaphingst, K.M.; Story, M. Child care as an untapped setting for obesity prevention: State child care licensing regulations related to nutrition, physical activity, and media use for preschool-aged children in the United States. Prev. Chronic Dis. 2009, 6, A11. [Google Scholar]
- Economic Opportunity Institute Washington State Career and Wage Ladder Evaluation. Available online: http://www.opportunityinstitute.org/research/post/washington-state-career-and-wage-ladder-evaluation/ (accessed on 27 December 2020).
- Bartlett, S.; Burstein, N.; Hamilton, W.; Kling, R. Food Stamp Program Access STUDY Final Report; E-FAN; Economic Research Service: Washington, DC, USA, 2004; Volume 3-013-3.
- Hungry Harvest about Produce in a SNAP. Available online: https://www.produceinasnap.com/our-roots (accessed on 23 November 2019).
- Good Food Bags. Available online: http://www.tilthalliance.org/about/good-food-bags (accessed on 23 November 2019).
- Snelling, A.; Maroto, M.; Jacknowitz, A.; Waxman, E. Key Factors for School-Based Food Pantries: Perspectives from Food Bank and School Pantry Personnel. J. Hunger Environ. Nutr. 2014, 9, 350–361. [Google Scholar] [CrossRef]


{kind=link}
| Demographic Factor * | Food Secure (n = 185) | Low Food Security (n = 64) | Very Low Food Security (n = 64) |
|---|---|---|---|
| Age, mean (SD) | 39.5 (13) | 35.5 (13) | 33.3 (12) |
| Females, n (%) | 171 (93%) | 59 (92%) | 61 (97%) |
| U.S. Born, n (%) | 155 (84%) | 55 (86%) | 58 (91%) |
| Study Site, n (%) | |||
| Seattle, WA | 81 (44%) | 26 (41%) | 19 (30%) |
| South King County, WA | 50 (27%) | 16 (25%) | 15 (23%) |
| Austin, TX | 54 (29%) | 22 (34%) | 30 (47%) |
| Race/Ethnicity, n (%) | |||
| Non-Hispanic White | 118 (64%) | 30 (47%) | 27 (42%) |
| Non-Hispanic Black/African-American | 17 (9%) | 10 (16%) | 14 (22%) |
| Non-Hispanic, Other | 27 (15%) | 3 (5%) | 6 (9%) |
| Hispanic | 23 (12%) | 21 (33%) | 17 (27%) |
| No Children (<18) in Household, n (%) | 125 (68%) | 32 (50%) | 40 (63%) |
| Highest Level of Education, n (%) | |||
| ≤High School or GED | 17 (9%) | 18 (28%) | 16 (25%) |
| Some college, Associate’s degree, ECE certificate | 65 (35%) | 23 (36%) | 32 (50%) |
| Bachelor’s degree or higher | 103 (56%) | 23 (36%) | 16 (25%) |
| ECE Job Title, n (%) | |||
| Center Director | 20 (11%) | 3 (5%) | 3 (5%) |
| Lead Teacher or Instructor | 55 (30%) | 24 (38%) | 28 (44%) |
| Teacher or Instructor | 50 (27%) | 14 (22%) | 14 (22%) |
| Assistant Teacher or Instructor | 41 (22%) | 12 (19%) | 13 (20%) |
| Other | 19 (10%) | 11 (17%) | 6 (9%) |
| Average Paid Hours of Work Per Week, mean (SD) | 37.7 (8) | 37.2 (7) | 36.5 (8) |
| Individual Annual Income ($), median (25th–75th percentile) | 31,340 (25,480–37,502) | 25,935 (17,160–31,221) | 26,000 (15,600–30,000) |
| Household income, n (%) | |||
| Below $25,000 | 22 (12%) | 20 (31%) | 20 (31%) |
| $25,000–$49,999 | 55 (30%) | 20 (31%) | 28 (43%) |
| $50,000 or more | 96 (52%) | 18 (28%) | 15 (23%) |
| Don’t know | 12 (7%) | 6 (9%) | 1 (2%) |
| Hourly Wage in Comparison to Median Site Wage, n (%) | |||
| Below median | 73 (41%) | 34 (55%) | 41 (66%) |
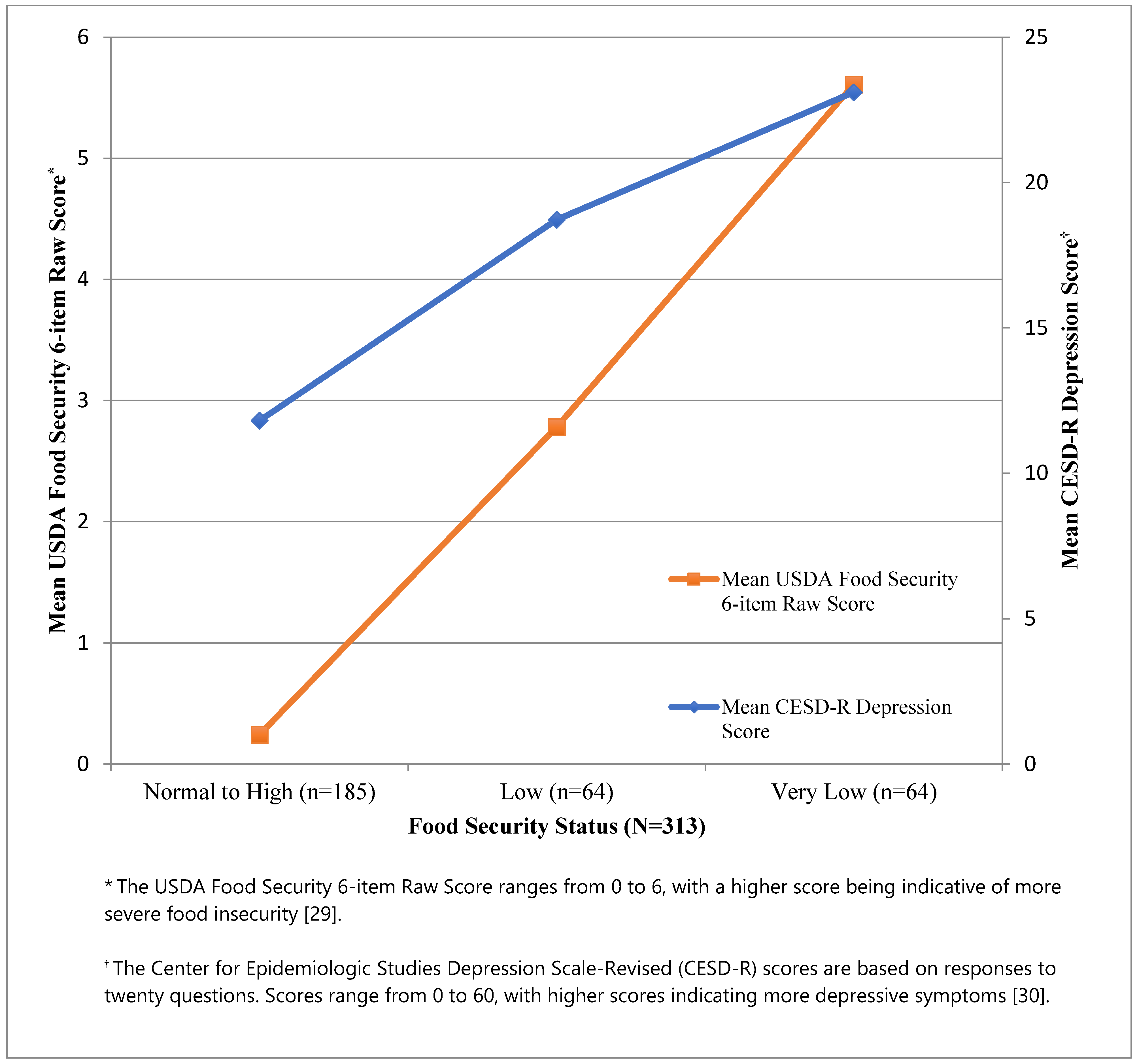
| Depression CESD-R Score †, mean (SD) | 11.8 (8) | 18.7 (12) | 23.1 (12) |
| Non-clinical Depression ‡, n (%) | 138 (75%) | 31 (48%) | 21 (33%) |
| USDA Food Security 6-item Raw Score §, mean (SD) | 0.2 (0.4) | 2.8 (0.8) | 5.6 (0.5) |
| Participates in Food Assistance Program ◊, n (%) | 32 (17%) | 20 (31%) | 20 (31%) |
| Food Security Status | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Low Food Security (N = 64) | 2.69 | (1.29, 5.63) | 0.011 |
| Very Low Food Security (N = 64) | 4.95 | (2.29, 10.67) | 0.000 |
| Food Security Status | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Sensitivity Analysis 1: Primary Model + Sex (N = 311) † | |||
| Low Food Security (n = 64) | 2.75 | (1.32, 5.79) | 0.009 |
| Very Low Food Security (n = 63) | 5.00 | (2.31, 10.83) | 0.000 |
| Sensitivity Analysis 2: Primary Model, replacing Annual Household Income with Annual Individual Income (N = 299) ‡ | |||
| Low Food Security (n = 61) | 3.06 | (1.49, 6.27) | 0.002 |
| Very Low Food Security (n = 62) | 5.49 | (2.63, 11.46) | 0.000 |
| Food Security Status | Food Assistance Program Participation (N = 313) † | Individual Wage (N = 303) † | ||
|---|---|---|---|---|
| Yes (n = 72) | No (n = 241) | Below Site Median (n = 146) ‡ | At or Above Site Median (n = 155) | |
| Low Food Security | 2.58 (0.41, 16.35) | 2.73 (1.17, 6.38) | 1.62 (0.52, 5.04) | 4.11 (1.28, 13.24) |
| Very Low Food Security | 6.77 (1.02, 44.80) | 6.11 (2.48, 15.02) | 6.67 (2.19, 20.38) | 5.18 (1.32, 20.32) |
| Global p value | 0.71 | 0.41 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loh, I.H.; Oddo, V.M.; Otten, J. Food Insecurity Is Associated with Depression among a Vulnerable Workforce: Early Care and Education Workers. Int. J. Environ. Res. Public Health 2021, 18, 170. https://doi.org/10.3390/ijerph18010170
Loh IH, Oddo VM, Otten J. Food Insecurity Is Associated with Depression among a Vulnerable Workforce: Early Care and Education Workers. International Journal of Environmental Research and Public Health. 2021; 18(1):170. https://doi.org/10.3390/ijerph18010170
Chicago/Turabian StyleLoh, Ivory H., Vanessa M. Oddo, and Jennifer Otten. 2021. "Food Insecurity Is Associated with Depression among a Vulnerable Workforce: Early Care and Education Workers" International Journal of Environmental Research and Public Health 18, no. 1: 170. https://doi.org/10.3390/ijerph18010170
APA StyleLoh, I. H., Oddo, V. M., & Otten, J. (2021). Food Insecurity Is Associated with Depression among a Vulnerable Workforce: Early Care and Education Workers. International Journal of Environmental Research and Public Health, 18(1), 170. https://doi.org/10.3390/ijerph18010170