Effectiveness of the Validation Method in Work Satisfaction and Motivation of Nursing Home Care Professionals: A Literature Review

 , ,
, ,  and
and
Abstract
:1. Introduction
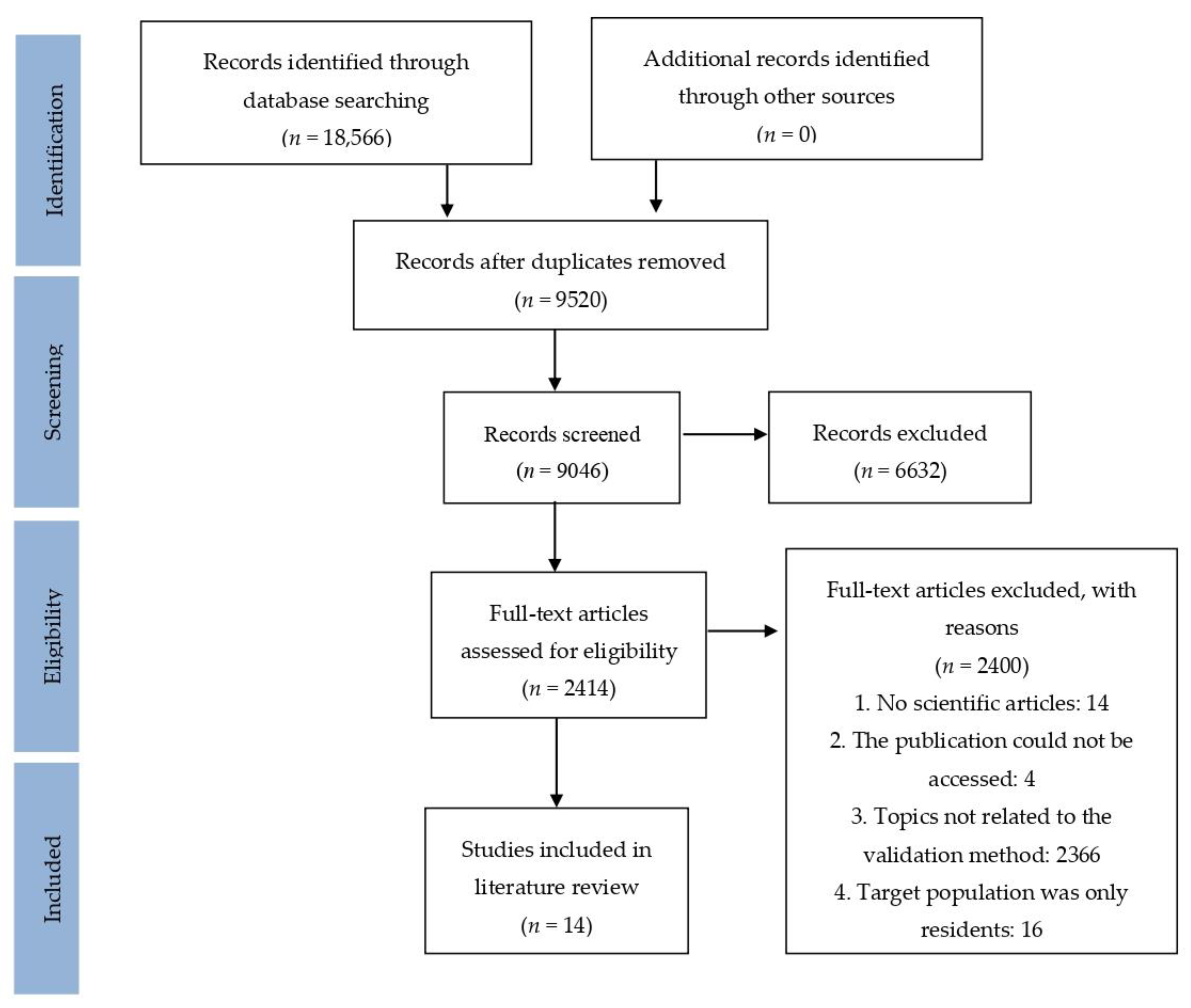
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mitchell, G.; Agnelli, J. Non-Pharmacological Approaches to Alleviate Distress in Dementia Care. Nurs. Stand. 2015, 30, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Berg-Weger, M.; Stewart, D.B. Non-pharmacologic interventions for persons with dementia. Mo. Med. 2017, 114, 116–119. [Google Scholar]
- Sikkes, S.A.; Tang, Y.; Jutten, R.J.; Wesselman, L.M.; Turkstra, L.S.; Brodaty, H.; Clare, L.; Cassidy-Eagle, E.; Cox, K.L.; Chételat, G.; et al. Toward a theory-based specification of non-pharmacological treatments in aging and dementia: Focused reviews and methodological recommendations. Alzheimer’s Dement. 2020, 1–16. [Google Scholar] [CrossRef]
- Eggenberger, E.; Heimerl, K.; Bennett, M.I. Communication Skills Training in Dementia Care: A Systematic Review of Effectiveness, Training Content, and Didactic Methods in Different Care Settings. Int. Psychogeriatr. 2013, 25, 345–358. [Google Scholar] [CrossRef] [PubMed]
- Feil, N. When Feelings Become Incontinent: Sexual Behaviors in the Resolution Phase of Life. Sex. Disabil. 1995, 13, 271–282. [Google Scholar] [CrossRef]
- Hansebo, G.; Kihlgren, M. Carers’ Interactions with Patients Suffering from Severe Dementia: A Difficult Balance to Facilitate Mutual Togetherness. J. Clin. Nurs. 2002, 11, 225–236. [Google Scholar] [CrossRef]
- Ripich, D.; Wykle, M.; Niles, S. The FOCUSED Program: A Communication Skills Training Program Helps Nursing Assistants to Give Better Care to Patients with Alzheimer’s Disease. Geriatr. Nurs. 1995, 16, 15–19. [Google Scholar] [CrossRef]
- Eton, D.T.; Ridgweway, J.L.; Linzer, M.; Boehm, D.H.; Rogers, E.A.; Yost, K.J.; Rutten, LJ.F.; Sauver, J.L.S.; Poplau, S.; Anderson, R.T. Healthcare Provider Relational Quality Is Associated with Better Self-Management and Less Treatment Burden in People with Multiple Chronic Conditions. Patient Prefer. Adherence 2017, 11, 1635–1646. [Google Scholar] [CrossRef] [Green Version]
- Savundranayagam, M.Y.; Hummert, M.L.; Montgomery, R.J. Investigating the Effects of Communication Problems on Caregiver Burden. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2005, 60, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Vasse, E.; Vernooij-Dassen, M.; Spijker, A.; Rikkert, M.O.; Koopmans, R. A Systematic Review of Communication Strategies for People with Dementia in Residential and Nursing Homes. Int. Psychogeriatr. 2010, 22, 189–200. [Google Scholar] [CrossRef] [Green Version]
- Lee, G.E.; Kim, J.Y.; Jung, J.H.; Kang, H.W.; Jung, I.C. Non-pharmacological interventions for patients with dementia. A protocol for a systematic review and meta-analysis. Medicine 2019, 98, 1–5. [Google Scholar] [CrossRef]
- Babins, L. Conceptual Analysis of Validation Therapy. Int. J. Aging Hum. Dev. 1988, 26, 161–168. [Google Scholar] [CrossRef]
- Jones, G.M. A Review of Feil’s Validation Method for Communicating with and Caring for Dementia Sufferers. Curr. Opin. Psychiatry 1997, 10, 326–332. [Google Scholar] [CrossRef]
- Bleathman, C.; Morton, I. Validation Therapy: A Review of Its Contribution to Dementia Care. Br. J. Nurs. 1996, 5, 866–868. [Google Scholar] [CrossRef] [PubMed]
- Feil, N.; De Klerk-Rubin, V. Validación. In Un Método Para Ayudar a Las Personas Mayores Desorientadas; Herder: Barcelona, Spain, 2002. [Google Scholar]
- Swall, A.; Marmstål-Hammar, L.; Gransjön-Craftman, Å. Like a bridge over troubled water- a qualitative study of professional caregiver singing and music as a way to enable person-centred care for persons with dementia. Int. J. Qual. Stud. Health Well-Being 2020, 15, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Más, A.; Parra, P.; Bermejo, R.M.; Hidalgo, M.D.; Calle, J.E. Improving Quality in Healthcare: What Makes a Satisfied Patient? Rev. Calid. Asist. 2016, 31, 196–203. [Google Scholar] [CrossRef]
- Soares, C.C.; Marques, A.M.; Clarke, P.; Klein, R.; Koskinen, L.; Krasuckiene, D.; Küçükgüçlü, Ö. Older People’s Views and Expectations about the Competences of Health and Social Care Professionals: A European Qualitative Study. Eur. J. Ageing 2019, 16, 53–62. [Google Scholar] [CrossRef]
- Soares, C.C.; Marques, A.M. Communicator. In Older People: Improving Health and Social Care. Focus on the European Core Competences Framework; Dijkman, B., Mikkonen, I., Roodbol, P., Eds.; Springer Nature: Cham, Switzerland, 2019; pp. 171–192. [Google Scholar]
- Bullington, J.; Söderlund, M.; Bos Sparén, E.; Kneck, Å.; Omérov, P.; Cronqvist, A. Communication Skills in Nursing. A phenomenologically-Based Communication Training Approach. Nurse Educ. Pract. 2019, 39, 136–141. [Google Scholar] [CrossRef]
- Canon, R.L. The Effect of Validation Therapy Training on Satisfaction with Communication and Quality of Relationship between Staff and Family Caregivers and Demented Residents in Long Term Care. Ph.D. Thesis, School of Health Professions Southwest Texas State University San Marcos, San Marcos, TX, USA, 1995. Available online: https://digital.library.txstate.edu/handle/10877/4363 (accessed on 10 June 2020).
- Söderlund, M.; Norberg, A.; Hansebo, G. Implementation of the Validation Method: Nurses’ Descriptions of Caring Relationships with Residents with Dementia Disease. Dementia 2011, 11, 569–587. [Google Scholar] [CrossRef]
- Söderlund, M.; Cronqvist, A.; Norberg, A.; Ternestedt, B.M.; Hansebo, G. Conversations between Persons with Dementia Disease Living in Nursing Homes and Nurses–Qualitative Evaluation of an Intervention with the Validation Method. Scand. J. Caring Sci. 2016, 30, 37–47. [Google Scholar] [CrossRef]
- Söderlund, M.; Norberg, A.; Hansebo, G. Validation Method Training: Nurses’ Experiences and Ratings of Work Climate. Int. J. Older People Nurs. 2013, 9, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Söderlund, M.; Cronqvist, A.; Norberg, A.; Ternestedt, B.M.; Hansebo, G. Nurses’ Movements within and between Various Paths When Improving Their Communication Skills: An Evaluation of Validation Method Training. Open J. Nurs. 2013, 3, 265–273. [Google Scholar] [CrossRef] [Green Version]
- Finnema, E.J.; Dröes, R.M.; Van Der Kooij, C.H.; De Lange, J.; Rigter, H.; Van Montfort, A.P.W.P.; Van Tilburg, W. The Design of a Large-Scale Experimental Study into the Effect of Emotion-Oriented Care on Demented Elderly and Professional Careers in Nursing Homes. Arch. Gerontol. Geriatr. 1998, 26, 193–200. [Google Scholar] [CrossRef]
- Finnema, E.J.; Dröes, R.M.; Ettema, T.; Ooms, M.; Adèr, H.; Ribbe, M.; Van Tilburg, W. The Effect of Integrated Emotion-oriented Care versus Usual Care on Elderly Persons with Dementia in the Nursing Home and on Nursing Assistants: A Randomized Clinical Trial. Int. J. Geriatr. Psychiatry A J. Psychiatry Late Life Allied Sci. 2005, 20, 330–343. [Google Scholar] [CrossRef]
- Tondi, L.; Ribani, L.; Bottazzi, M.; Viscomi, G.; Vulcano, V. Validation Therapy (VT) in Nursing Home: A Case-Control Study. Arch. Gerontol. Geriatr. 2007, 44, 407–411. [Google Scholar] [CrossRef]
- Hergue, M.; Lenesley, P.; Narme, P. Satisfaction Au Travail et Culture Managériale Empathique En EHPAD: Étude Exploratoire Dans Deux Établissements. NPG Neurol. Psychiatr. Gériatrie 2019, 19, 23–29. [Google Scholar] [CrossRef]
- Oliveira, M.P.; Sousa, L.X. VALIDA: A Validation Therapy-Training Program for Staff of a Residential Care Facility. Int. J. Aging Hum. Dev. 2020, 1–17. [Google Scholar] [CrossRef]
- Woodrow, P. Intervention for confusion and dementia. 4: Alternative approaches. Br. J. Nurs. 1998, 7, 12–25. [Google Scholar] [CrossRef]
- Neal, M.; Wright, P.B.; Briggs, M. Validation therapy for dementia. Cochrane Database Syst. Rev. 2003, 3, 1–28. [Google Scholar] [CrossRef]
- Narme, P. Épuisement Professionnel Des Soignants En Ehpad: Rôle de l’empathie et de La Formation. Gériatrie et Psychol. Neuropsychiatr. Du Vieil. 2018, 16, 2015–2222. [Google Scholar] [CrossRef]
- Van Corven, C.T.M.; Bielderman, A.; Wijnen, M.; Leontjevas, R.; Lucassen, P.L.B.J.; Graff, M.J.L.; Gerritsen, D.L. Defining empowerment for older people living with dementia from multiple perspectives. Int. J. Nurs. Stud. 2020, 114, 1–11. [Google Scholar] [CrossRef]
- Validation Training Institute, Inc. (VTI). Available online: https://vfvalidation.org/about-us/our-team/ (accessed on 20 October 2020).
- Deponte, A.; Missan, R. Effectiveness of Validation Therapy (VT) in Group: Preliminary Results. Arch. Gerontol. Geriatr. 2006, 44, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Toseland, R.W.; Diehl, M.; Freeman, K.; Manzanares, T.; Naleppa, M.; McCallion, P. The Impact of Validation Group Therapy on Nursing Home Residents with Dementia. J. Appl. Gerontol. 1997, 16, 31–50. [Google Scholar] [CrossRef]
- Fine, J.L.; Rouse-Bane, S. Using Validation Techniques to Improve Communication with Cognitively Impaired Older Adults. J. Gerontol. Nurs. 1995, 21, 39–45. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E. The Measurement of Experienced Burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Cummings, J.L.; Mega, M.; Gray, K.; Rosenberg-Thompson, S.; Carusi, D.A.; Gornbein, J. The Neuropsychiatric Inventory: Comprehensive Assessment of Psychopathology in Dementia. Neurology 1994, 44, 2308–2314. [Google Scholar] [CrossRef] [Green Version]
- Ekvall, G. Organizational Climate for Creativity and Innovation. Eur. J. Work Organ. Psychol. 1996, 5, 105–123. [Google Scholar] [CrossRef]
- Lemke, S.; Moos, R.H. Validity of the Sheltered Care Environment Scale: Conceptual and Methodological Issues. Psychol. Aging 1990, 5, 569–571. [Google Scholar] [CrossRef]
- Narme, P.; Jaafari, N.; Gil, R. Echelle d’empathie Interpersonal Reactivity Index (IRI). In GREMOIRE 2: Tests Et Échelles Des Maladies Neurologiques Avec Symptomatologie Cognitive; Sellal, F., Thomas-Antérion, C., Hugonot-Diener, L., Eds.; De Boeck-Solal Éditions: Marseille, France, 2015; pp. 128–132. [Google Scholar]
- Hojat, M.; Gonnella, J.S.; Nasca, T.J.; Mangione, S.; Vergare, M.; Magee, M. Physician Empathy: Definition, Components, Measurement, and Relationship to Gender and Specialty. Am. J. Psychiatry 2002, 159, 1563–1569. [Google Scholar] [CrossRef] [Green Version]
- Hecht, M.L. Measures of Communication Satisfaction. Hum. Commun. Res. 1978, 4, 350. [Google Scholar] [CrossRef]
- Hudson, W. The Clinical Measurement Package: A Field Manual; Dorsey Press: Chicago, IL, USA, 1982; Volume 56. [Google Scholar]
- Goldberg, D.P.; Hillier, V.F. A Scaled Version of the General Health Questionnaire. Psychol. Med. 1979, 9, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Van den Broeck, A.; Vansteenkiste, M.; De Witte, H.; Soenens, B.; Lens, W. Capturing Autonomy, Competence, and Relatedness at Work: Construction and Initial Validation of the Work-related Basic Need Satisfaction Scale. J. Occup. Organ. Psychol. 2010, 83, 981–1002. [Google Scholar] [CrossRef] [Green Version]
- Nazneen, A.; Bhalla, P. A Study of Organizational Role Stress and Organizational Commitment among the Faculty Members of Public and Private Universities. Int. J. Hum. Resour. Manag. Res. 2014, 4, 69–76. [Google Scholar]
- Cohen-Mansfield, J.; Marx, M.S.; Rosenthal, A.S. A Description of Agitation in a Nursing Home. J. Gerontol. 1989, 44, 77–84. [Google Scholar] [CrossRef]
- Benjamin, B.J. Validation: A Communication Alternative. In Enhancing the Quality of Life in Advanced Dementia; Volicer, L., Bloom-Charette, L., Eds.; Taylor & Francis: Philadelphia, PA, USA, 1999; pp. 107–125. [Google Scholar]
- Gagnon, D.L. A Review of Reality Orientation (RO), Validation Therapy (VT), and Reminiscence Therapy (RT) with the Alzheimer’s Client. Phys. Occup. Ther. Geriatr. 1996, 14, 61–77. [Google Scholar] [CrossRef]
- Finnema, E.J.; Dröes, R.M.; Ribbe, M.; Van Tilburg, W. The Effects of Emotion-oriented Approaches in the Care for Persons Suffering from Dementia: A Review of the Literature. Int. J. Geriatr. Psychiatry 2000, 15, 141–161. [Google Scholar] [CrossRef]
- Schrijnemaekers, V.; Van Rossum, E.; Candel, M.; Frederiks, C.; Derix, M.; Sielhorst, H.; Van den Brandt, P. Effects of Emotion-Oriented Care on Elderly People with Cognitive impairment and Behavioral Problems. Int. J. Geriatr. Psychiatry 2002, 17, 926–937. [Google Scholar] [CrossRef] [Green Version]
- Brooker, D. What Is Person-Centred Care in Dementia? Rev. Clin. Gerontol. 2003, 13, 215–222. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Features | Inclusion Criteria |
|---|---|
| Font Type | Any type (articles, books chapters, theses, etc.) |
| End-Users | ≥than 65 years with dementia in nursing homes |
| Professionals Language | Healthcare professionals Spanish, English, French |
| Intervention | Validation method (individual or in group) |
| Design Types | Experimental, quasi-experimental, qualitative, quantitative, mixed method, single case series, literature review |
| Time Period | Unlimited |
| Study | Target Population | n | Mean Age (Years) (SD) | Women (%) | Professional Profile | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| P | R | F | P | R | P | R | P | R | |||
| Deponte, Missan (2006) [36] | x | x | P: NR | R: 30 | P: NR (NR) | R: 86.8 (NR) | P: NR | R: >80% * | Nursing Staff | ||
| Tondi et al., (2007) [28] | x | x | P: NR | R: 50 | P: NR (NR) | R: 88.2 (NR) | P: NR | R: 82% | Nursing Staff | ||
| GCr: 88.5 (NR) | |||||||||||
| GEr: 87.8 (NR) | |||||||||||
| Toseland et al., (1997) [37] | x | x | P: NR | R: 88 | P: NR (NR) | R: 88 (NR) | P: (NR) * | R: 75% | Licensed practical nurses, caregivers * | ||
| GEr: 87.8 (6.0) | |||||||||||
| GEr: 87.3 (6.1) | |||||||||||
| GCr: 87.8 (7.6) | |||||||||||
| Feil, (1995) [5] | x | P: 3 | R: 3 | P: NR (NR) | R: 89.5 (NR) | P: 66.6 % | R: 67% | Validation therapist | |||
| Finnema et al., (2005) [27] | x | x | P: 99 | R:146 | P: NR | R: 83 (NR) | P: 87% | R: 81% | Nursing aides, nurse, ward assistant, team leader | ||
| GEp: 30.8 (8.0) | GEr: 83.8 (5.3) | ||||||||||
| GCp: 30.2 (7.4) | GEr: 83.6 (5.8) | ||||||||||
| Söderlund et al., (2013a) [24] | x | x | P: 68 | R: 11 | P: 45.3 (NR) | R: 85.5 (NR) | P: 91.2% * | R: 81.8% | Registered nurses, licensed practical nurses, nurse aides | ||
| Söderlund et al., (2013b) [25] | x | x | P: 8 | R: 11 | P: 49.5 (NR) | R: 85.5 (NR) | P: 100% | R: 81.8% | Registered nurses, licensed practical nurses, nurse aides | ||
| Sördelund et al., (2011) [22] | x | x | P(A/B): 23 | R: 29 | P(A/B): 44.3 (NR) | R: 88 (NR) | P (A/B): 100% | R: 79.3% | Registered nurses, licensed practical nurses, nurse aides | ||
| Sördelund et al., (2016) [23] | x | x | P: 4 | R: 4 | P: 50.5 (NR) | R: 86.5 (NR) | P: 100% | R: 100% | Licensed practical nurses, nurse aides | ||
| Hergue et al., (2019) [29] | x | P: 29 | NA | P: NR | NA | Caregivers, nurses, doctors, manager. | |||||
| GEp: 40.5 (9.8) | P: 80% | ||||||||||
| GEp: 40.2 (9.4) | P: 100% * | ||||||||||
| Narme, (2018) [33] | Study 1 (S1) | x | P: 124 | NA | P: 38.4 (11.3) | NA | P: 92.7% | NA | Caregivers and Nurses | ||
| Study 2 (S2) | P: 122 | NA | P: 39.2 (9.9) | NA | P: 95% | NA | |||||
| Fine, Rouse-Bane, (1995) [38] | x | x | P: NR | R:35 | P: NR (NR) | P: NR (NR) | NR | NR | Nursing staff | ||
| Canon (1995) [21] | x | x | P/F: 58 | NA | P/F: NR (NR) | P/F: 86% | Caregivers, resident’s family | ||||
| Oliveira, Sousa (2020) [30] | x | P: 22 | NA | P: 46 (11.9) | P: 95.5% | Direct care worker, care-home manager, administrative assistant, psychologist and animator | |||||
| Study | Country | Methodology | Conclusions | |||
|---|---|---|---|---|---|---|
| Design | Outcome Measures | Intervention Group | Intervention Type | |||
| Deponte, Missan, (2006) [36] | Italy | Quantitative Design | MMSE, BANSS, NPI | Residents (r): RCT 1 GEr: VM implementation 1 GEr: SR group 1 GCr: no VM implementation Professionals (p): 1 GCp was formed by professionals | The GErs were conducted by two different facilitators, 2 days a week, at the same time. Each session lasted 45–60 min for 3 months. After 3 months, it was evaluated by the same battery test as the pre-treatment. For the GCp the intervention type was not specified. | (P): increased effect on the caregiver’s feelings, giving meaning to the residents behaviours. |
| Tondi et al., (2007) [28] | Italy | Quantitative Design | MMSE, BANSS, NPI | Residents (r): 1 GEr: VM implementation 1 GCr: no VM implementation Professionals (p): 1 GEp was formed by professionals | GEr carried out individual sessions in VM of 20 min, 3 times a week, and group sessions once a week of 50 min for 4 months. The GCr did not receive the VM intervention The GEp participated in the individual and group sessions. A follow-up was carried out for 1 week at the end of the intervention. | (P): reduction of stress levels in professionals. |
| Feil, (1995) [5] | United States of America | Single unique cases series design | MMSE | 3 case studies | Weekly individual and group sessions | (P): The use of validation techniques helps professionals to grasp the reason for, and give value to, the emotions expressed by the residents. |
| Söderlund et al., (2013b) [25] | Sweden | Qualitative design | CPS | 2-arm trial VM training programme | Individual sessions for 12 months, 2–3 times a week, at the beginning they lasted between 3–14 min and, at the end of the training, from 5 to 36 min. | (P): VM training of caregivers improves their response to the needs and behaviours expressed by residents. The programme contributes to improving the communication skills of caregivers with residents, increasing quality care. |
| Söderlund et al., (2016) [23] | Sweden | Qualitative design | CPS | 1-arm trial VM training programme | Individual sessions 2–3 times a week for 5 months. | (P): Improvements in communication skills, increased conversations with residents from 3 min (at the beginning of the programme) to 36 min (at the end of the programme). |
| Hergue et al., (2019) [29] | France | Quantitative design | MBI, Karasek’s Scale | 2-arm trial VM training programme | Burnout and social support questionnaires were sent to the heads of two residences. One group was formed in VM and the other group was not. | (P): The group formed in VM, the caregivers, feel more listened to, understood and supported; burnout is reduced and productivity, motivation, professional competence, satisfaction and commitment to the organisation are increased. |
| Study | Country | Methodology | Conclusions | ||||
|---|---|---|---|---|---|---|---|
| Design | Outcome Measures | Intervention Group | Intervention Types | Evaluation | |||
| Finnema et al., (2005) [27] | Netherlands | Mixed Design |
| RCT Residents (r): 1 GEr: emotion-oriented care 1 GCr: usual care Professional (p): 1 GEp: emotion-oriented care training 1 GCp: usual care training | Training sessions in Model-Care Plan for 2.5 days for 7 months at GEp, combining the Model-Care Plan with the Emotion-oriented care based on VM. The GCp and GCr combined the Model-Care Plan with Usual Care | Follow-up and supervision 4 times for 1 day on empathic skills for the GE and usual care to GC. Pre-post training assessment, at 4 and 7 months. | (P): Reduction of stress levels and increased knowledge of tools that facilitate care. No differences in absenteeism and job competence were found in either group. |
| Toseland et al., (1997) [37] | United States of America | Quantitative Design | SPMSQ, VSI, MOSES SCES, CMAI, GIPB MDS | 3-arm trial with RCT Residents (r): 1 GEr: VM implementation 1 GEr: SC group 1 GCr: no VM implementation, usual care (UC) Professionals (p): 1 GEp was formed by professionals | 4-day training in the VM. 30 min group sessions of VM, SC, UC were held for 13 months, conducted by leading professionals from each group. | Weekly telephone follow-up and monthly physical supervision by a validation therapist. Pre-intervention assessment at 2 weeks after start of intervention and post intervention at 3 and 12 months. | (P): Professionals trained in VM have a positive increase in the management of problem behaviours at 3 and 12 months, understand the meaning of residents’ behaviours better, and have a more positive work environment. |
| Sördelund et al., (2011) [22] | Sweden | Qualitative Design | RAI, MDS, CPS | 2-arm trial VM training programme | 10 VM training sessions with supervision, spaced over one year, and practical VM training for at least 6 months between lesson blocks. 2–3 times a week. | Pre-post training assessment where participants received feedback from an accredited VM trainer throughout the year. Follow-up for 1 year. | (P): Improves the relationship with the resident, who improves the work environment. (P): VM is useful for handling difficult caregiving situations. Professionals were happier, less stressed and more confident. |
| Söderlund et al., (2013a) [24] | Sweden | Mixed Design | CCQ | 2-arm trial VM training programme | Individual interviews after finishing the VM training programme after 12 months. | Analysis of the content of the interviews. Assessment of the work environment pre-post training. | (P): Increase in positive work climate scores. (P): The VM developed their communication skills and better handling of complex situations in care. |
| Fine, Rose-Bane, (1995) [38] | United States of America | Quasi-Experimental Design | QO | 3-arm trial Residents (r): 2 GEr: VM implementation Professionals (p): 1 GEp was formed by professionals with VM training | The GEp carried out 6-h VM training sessions for 2 weeks. | Weekly follow-up sessions for workers for 3 months and pre-post intervention assessment. | (P): They found a 73% reduction in problem behaviours with the use of the appropriate technique for the disorientation phase and reduction of work stress. |
| Canon, (1995) [21] | United States of America | Quasi-Experimental Mixed Design | ICSI, DCQRI, CAM/CAF, VS | Non-RCT 1 GE: formed by caregivers and resident’s family. 1GC: formed by caregivers and resident’s family. | VM training sessions were held in 2 days of 7 h and pre-post training questionnaires were administered. | The pre-assessment was carried out before the training. The post-test assessment was carried out at the end of the training, up to 2 weeks after. There was no follow-up. | (P): increase in satisfaction with professional-resident communication after VM training. (F): the training gave them communication tools, a greater understanding of the expressions of their relatives and greater satisfaction in communication with their family member. |
| Oliveira, Sousa, (2020) [30] | Portugal | Qualitative Design | Own questionnaire about functioning session. Semi-structured interview. Focus Group. | 1-arm trial VM training programme | 4 group training sessions were held on the MV of 60–90 min for 6 months. | Content analysis on the effectiveness of training after each session and at 6 months through Focus Group. There was no follow-up. | (P): Increased empowerment, self-confidence and reduction in stress levels and the use of therapeutic lying. |
| Narme, (2018) [33] | France | Quantitative Design | MBI, IRI, JSE | S1: 2-arm trial 1 GE: formed by nurses. 1 GE: formed by caregivers. | Burnout, interpersonal reactivity and empathy questionnaire administered. | Correlation between the risk of burnout and the scores on the empathy scale and its comparison between nurses and aides. | (P) S1: The different cognitive and emotional aspects of empathy do not contribute in the same way to the appearance of professional burnout. There are no differences in empathy scores based on professional status. |
| MBI, IRI | S2: 1-arm trial VM training programme | There were 3 days of MV training, 2 months of practical sessions, 2 days to discuss observed changes and 1 day to fill in post questionnaires. | Pre-evaluation before the start of the training. At 2 months there was a session to discuss changes observed in VM practice. After 6 months, the post questionnaires were administered. There was no follow-up. | (P) S2: Training brings benefits to workers, the quality of care and institutional functioning. Training contributes to burnout and stress prevention. | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Martínez, I.; Vilar, R.; Irujo, J.; Ulsamer, D.; Cano, D.; Casaca Soares, C.; Acevedo, Á.; Jerez-Roig, J.; Celdrán, M. Effectiveness of the Validation Method in Work Satisfaction and Motivation of Nursing Home Care Professionals: A Literature Review. Int. J. Environ. Res. Public Health 2021, 18, 201. https://doi.org/10.3390/ijerph18010201
Sánchez-Martínez I, Vilar R, Irujo J, Ulsamer D, Cano D, Casaca Soares C, Acevedo Á, Jerez-Roig J, Celdrán M. Effectiveness of the Validation Method in Work Satisfaction and Motivation of Nursing Home Care Professionals: A Literature Review. International Journal of Environmental Research and Public Health. 2021; 18(1):201. https://doi.org/10.3390/ijerph18010201
Chicago/Turabian StyleSánchez-Martínez, Iván, Raül Vilar, Javier Irujo, Duna Ulsamer, Dolors Cano, Celia Casaca Soares, Ángel Acevedo, Javier Jerez-Roig, and Montserrat Celdrán. 2021. "Effectiveness of the Validation Method in Work Satisfaction and Motivation of Nursing Home Care Professionals: A Literature Review" International Journal of Environmental Research and Public Health 18, no. 1: 201. https://doi.org/10.3390/ijerph18010201
APA StyleSánchez-Martínez, I., Vilar, R., Irujo, J., Ulsamer, D., Cano, D., Casaca Soares, C., Acevedo, Á., Jerez-Roig, J., & Celdrán, M. (2021). Effectiveness of the Validation Method in Work Satisfaction and Motivation of Nursing Home Care Professionals: A Literature Review. International Journal of Environmental Research and Public Health, 18(1), 201. https://doi.org/10.3390/ijerph18010201