Suicidal Ideation Profiles in Patients with Fibromyalgia Using Transdiagnostic Psychological and Fibromyalgia-Associated Variables

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P. The American college of rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology Preliminary Diagnostic Criteria for Fibromyalgia and Measurement of Symptom Severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Queiroz, L.P. Worldwide Epidemiology of Fibromyalgia. Curr. Pain Headache Rep. 2013, 17, 356. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Ablin, J.; Fitzcharles, M.A.; LittleJohn, G.; Luciano, J.V.; Usui, C.; Walitt, B. Fibromyalgia. Nat. Rev. Dis. Primers 2015, 1, 15022. [Google Scholar] [CrossRef]
- Häuser, W.; Fitzcharles, M.A. Facts and myths pertaining to fibromyalgia. Dialogues Clin. Neurosci. 2018, 20, 53–62. [Google Scholar] [CrossRef]
- Rico-Villademoros, F.; Postigo-Martin, P.; Garcia-Leiva, J.M.; Ordoñez-Carrasco, J.L.; Calandre, E.P. Patterns of pharmacologic and non-pharmacologic treatment, treatment satisfaction and perceived tolerability in patients with fibromyalgia: A patients’ survey. Clin. Exp. Rheumatol. 2020, 123, 72–78. [Google Scholar]
- Cohen, H. Controversies and challenges in fibromyalgia: A review and a proposal. Ther. Adv. Musculoskelet. Dis. 2017, 9, 115–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzcharles, M.A.; Ste-Marie, P.A.; Goldenberg, D.L.; Pereira, J.X.; Abbey, S.; Choinière, M.; Ko, G.; Moulin, D.E.; Panopalis, P.; Proulx, J.; et al. 2012 Canadian Guidelines for the diagnosis and management of fibromyalgia syndrome: Executive summary. Pain Res. Manag. 2013, 18, 119–126. [Google Scholar] [CrossRef] [Green Version]
- MacFarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Flub, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef]
- Calandre, E.P.; Rico-Villademoros, F.; Slim, M. Pharmacological treatment of fibromyalgia: Is the glass half empty or half full? Pain Manag. 2017, 7, 5–10. [Google Scholar] [CrossRef] [PubMed]
- McNett, M.; Goldenberg, D.; Schaefer, C.; Hufstader, M.; Baik, R.; Chandran, A.; Zlateva, G. Treatment patterns among physician specialties in the management of fibromyalgia: Results of a cross-sectional study in the United States. Curr. Med. Res. Opin. 2011, 27, 673–683. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Qian, C.; Yang, M. Treatment Patterns Associated with ACR-Recommended Medications in the Management of Fibromyalgia in the United States. J. Manag. Care Spec. Pharm. 2016, 22, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Bennett, R.M.; Jones, J.; Turk, D.C.; Russell, I.J.; Matallana, L. An internet survey of 2596 people with fibromyalgia. BMC Musculoskelet. Disord. 2007, 9, 8–27. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.J.; Steer, M.; Ashe, S.C.; Furness, P.J.; Haywood-Small, S.; Lawson, K. Patients’ perspective of the effectiveness and acceptability of pharmacological and non-pharmacological treatments of fibromyalgia. Scand. J. Pain 2019, 19, 167–181. [Google Scholar] [CrossRef] [Green Version]
- Petzke, F.; Brückle, W.; Eidmann, U.; Heldmann, P.; Köllner, V.; Kühn, T.; Kühn-Becker, H.; Strunk-Richter, M.; Schiltenwolf, M. General treatment principles, coordination of care and patient education in fibromyalgia syndrome: Updated guidelines 2017 and overview of systematic review articles. Schmerz 2017, 31, 246–254. [Google Scholar] [CrossRef]
- Wolfe, F.; Hassett, A.L.; Walitt, B.; Michaud, K. Mortality in fibromyalgia: A study of 8186 patients over thirty-five years. Arthritis. Care Res. 2011, 63, 94–101. [Google Scholar] [CrossRef]
- Campbell, G.; Darke, S.; Bruno, R.; Degenhardt, L. The prevalence and correlates of chronic pain and suicidality in a nationally representative sample. Aust. N. Z. J. Psychiatry 2015, 49, 803–811. [Google Scholar] [CrossRef]
- Stenager, E.; Christiansen, E.; Handberg, G.; Jensen, B. Suicide attempts in chronic pain patients. A register-based study. Scand. J. Pain 2014, 5, 4–7. [Google Scholar] [CrossRef]
- Calati, R.; Laglaoui-Bakhiyi, C.; Artero, S.; Ilgen, M.; Courtet, P. The impact of physical pain on suicidal thoughts and behaviors: Meta-analyses. J. Psychiatr. Res. 2015, 71, 16–32. [Google Scholar] [CrossRef]
- Tang, N.K.Y.; Crane, C. Suicidality in chronic pain: A review of the prevalence, risk factors and psychological links. Psychol. Med. 2006, 36, 575–586. [Google Scholar] [CrossRef]
- Calandre, E.P.; Navajas-Rojas, M.A.; Ballesteros, J.; García-Carrillo, J.; García-Leiva, J.; Rico-Villademoros, F. Suicidal Ideation in Patients with Fibromyalgia: A Cross-Sectional Study. Pain Pract. 2014, 15, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Posner, K.; Oquendo, M.A.; Gould, M.; Stanley, B.; Davies, M. Columbia Classification Algorithm of Suicide Assessment (C-CASA): Classification of Suicidal Events in the FDA’s Pediatric Suicidal Risk Analysis of Antidepressants. Am. J. Psychiatry 2007, 164, 1035–1043. [Google Scholar] [CrossRef] [PubMed]
- Jobes, D.A.; Joiner, T.E. Reflections on Suicidal Ideation. Crisis 2019, 40, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Franklin, J.C.; Ribeiro, J.D.; Fox, K.R.; Bentley, K.H.; Kleiman, E.M.; Huang, X.; Musacchio, K.M.; Jaroszewski, A.C.; Chang, B.P.; Nock, M.K. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychol. Bull. 2017, 143, 187–232. [Google Scholar] [CrossRef]
- Hassett, A.L.; Aquino, J.K.; Ilgen, M.A. The Risk of Suicide Mortality in Chronic Pain Patients. Curr. Pain Headache Rep. 2014, 18, 436. [Google Scholar] [CrossRef]
- Hooley, J.M.; Franklin, J.C.; Nock, M.K. Chronic Pain and Suicide: Understanding the Association. Curr. Pain Headache Rep. 2014, 18, 435. [Google Scholar] [CrossRef]
- Kirtley, O.J.; Rodham, K.; Crane, C. Understanding suicidal ideation and behaviour in individuals with chronic pain: A review of the role of novel transdiagnostic psychological factors. Lancet Psychiatry 2020, 7, 282–290. [Google Scholar] [CrossRef]
- Klonsky, E.D.; Saffer, B.Y.; Bryan, C.J. Ideation-to-action theories of suicide: A conceptual and empirical update. Curr. Opin. Psychol. 2018, 22, 38–43. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Portzky, G. Looking to the Future: A Synthesis of New Developments and Challenges in Suicide Research and Prevention. Front. Psychol. 2018, 9, 2139. [Google Scholar] [CrossRef] [Green Version]
- Joiner, T.E. Why People Die by Suicide; Harvard University Press: Cambridge, UK, 2005. [Google Scholar]
- O’Connor, R.C. The Integrated Motivational-Volitional Model of Suicidal Behavior. Crisis 2011, 32, 295–298. [Google Scholar] [CrossRef]
- Klonsky, E.D.; May, A.M. The Three-Step Theory (3ST): A New Theory of Suicide Rooted in the “Ideation-to-Action” Framework. Int. J. Cogn. Ther. 2015, 8, 114–129. [Google Scholar] [CrossRef] [Green Version]
- Van Orden, K.A.; Witte, T.K.; Cukrowicz, K.C.; Braithwaite, S.R.; Selby, E.A.; Joiner, T.E. The interpersonal theory of suicide. Psychol. Rev. 2010, 117, 575–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fishbain, D.A.; Bruns, D.; Bruns, A.; Gao, J.; Lewis, J.E.; Meyer, L.J.; Disorbio, J.M. The Perception of Being a Burden in Acute and Chronic Pain Patients Is Associated with Affirmation of Different Types of Suicidality. Pain Med. 2016, 17, pme12889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, K.G.; Heenan, A.; Kowal, J.; Henderson, P.; McWilliams, L.A.; Castillo, D. Testing the Interpersonal Theory of Suicide in Chronic Pain. Clin. J. Pain 2017, 33, 699–706. [Google Scholar] [CrossRef]
- Lafuente-Castro, C.P.; Ordóñez-Carrasco, J.L.; García-Leiva, J.M.; Salgueiro-Macho, M.; Calandre, E.P. Perceived burdensomeness, thwarted belongingness and suicidal ideation in patients with fibromyalgia and healthy subjects: A cross-sectional study. Rheumatol. Int. 2018, 38, 1479–1486. [Google Scholar] [CrossRef]
- Williams, J.M.G.; Pollock, L.R. Psychological Aspects of the Suicidal Process. In Understanding Suicidal Behaviour: The Suicidal Process Approach to Research, Treatment and Prevention; van Heeringen, K., Ed.; Wiley: Chichester, UK, 2001; pp. 76–94. [Google Scholar]
- Dhingra, K.; Boduszek, D.; O’Connor, R.C. Differentiating suicide attempters from suicide ideators using the Integrated Motivational–Volitional model of suicidal behaviour. J. Affect. Disord. 2015, 186, 211–218. [Google Scholar] [CrossRef]
- Dhingra, K.; Boduszek, D.; O’Connor, R.C. A structural test of the Integrated Motivational-Volitional model of suicidal behaviour. Psychiatry Res. 2016, 239, 169–178. [Google Scholar] [CrossRef] [Green Version]
- Tucker, R.P.; O’Connor, R.C.; Wingate, L.R. An Investigation of the Relationship between Rumination Styles, Hope, and Suicide Ideation Through the Lens of the Integrated Motivational-Volitional Model of Suicidal Behavior. Arch. Suicide Res. 2016, 20, 553–566. [Google Scholar] [CrossRef] [Green Version]
- Wetherall, K.; Robb, K.A.; O’Connor, R.C. An Examination of Social Comparison and Suicide Ideation through the Lens of the Integrated Motivational-Volitional Model of Suicidal Behavior. Suicide Life-Threat Behav. 2018, 49, 167–182. [Google Scholar] [CrossRef] [Green Version]
- Shneidman, E.S. Suicide as Psychache: A Clinical Approach to Self-Destructive Behavior; Aronson: New York, NY, USA, 1993. [Google Scholar]
- Elman, I.; Borsook, D.; Volkow, N.D. Pain and suicidality: Insights from reward and addiction neuroscience. Prog. Neurobiol. 2013, 109, 1–27. [Google Scholar] [CrossRef] [Green Version]
- Giesecke, T.; Williams, D.A.; Harris, R.E.; Cupps, T.R.; Tian, X.; Tian, T.X.; Gracely, R.H.; Clauw, D.J. Subgrouping of fibromyalgia patients on the basis of pressure-pain thresholds and psychological factors. Arthritis Rheum. 2003, 48, 2916–2922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turk, D.C.; Okifuji, A.; Sinclair, J.D.; Starz, T.W. Differential responses by psychosocial subgroups of fibromyalgia syndrome patients to an interdisciplinary treatment. Arthritis Care Res. 1998, 11, 397–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, H.D.; Robinson, J.P.; Turk, D.C. Toward the identification of symptom patterns in people with fibromyalgia. Arthritis Rheum. 2009, 61, 527–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Aranda, A.; Andrés-Rodríguez, L.; Feliu-Soler, A.; Núñez, C.; Stephan-Otto, C.; Pastor-Mira, M.A.; López-Roig, S.; Peñacoba, C.; Calandre, E.P.; Slim, M.; et al. Clustering a large Spanish sample of patients with fibromyalgia using the Fibromyalgia Impact Questionnaire–Revised. Pain 2019, 160, 908–921. [Google Scholar] [CrossRef] [PubMed]
- Luciano, J.V.; Forero, C.G.; Cerdà-Lafont, M.; Peñarrubia-María, T.; Fernández-Vergel, R.; Cuesta-Vargas, A.I.; Ruíz, J.M.; Rozadilla-Sacanell, A.; Sirvent-Alierta, E.; Santo-Panero, P.; et al. Functional Status, Quality of Life, and Costs Associated with Fibromyalgia Subgroups. Clin. J. Pain 2016, 32, 829–840. [Google Scholar] [CrossRef]
- Vincent, A.; Hoskin, T.L.; Whipple, M.O.; Clauw, D.J.; Barton, D.L.; Benzo, R.P.; Williams, D.A. OMERACT-based fibromyalgia symptom subgroups: An exploratory cluster analysis. Arthritis Res. Ther. 2014, 16, 463. [Google Scholar] [CrossRef] [Green Version]
- Follick, B.T.; Cherry, B.J.; Rutledge, D.N.; Zettel-Watson, L.; Jones, J.C. Heterogeneity in fibromyalgia based upon cognitive and physical performance and psychological symptomology. J. Am. Assoc. Nurse Pract. 2016, 28, 19–30. [Google Scholar] [CrossRef]
- Gonzalez, B.; Novo, R.; Ferreira, A.S. Fibromyalgia: Heterogeneity in personality and psychopathology and its implications. Psychol. Health Med. 2019, 1–7. [Google Scholar] [CrossRef]
- Torres, X.; Bailles, E.; Valdes, M.; Gutierrez, F.; Peri, J.M.; Arias, A.; Gomez, E.; Collado, A. Personality does not distinguish people with fibromyalgia but identifies subgroups of patients. Gen. Hosp. Psychiatry 2013, 35, 640–648. [Google Scholar] [CrossRef]
- Triñanes, Y.; González-Villar, A.; Gómez-Perretta, C.; Carrillo-de-la-Peña, M.T. Suicidality in Chronic Pain: Predictors of Suicidal Ideation in Fibromyalgia. Pain Pract. 2014, 15, 323–332. [Google Scholar] [CrossRef]
- Bennett, R.M.; Friend, R.; Jones, K.D.; Ward, R.; Han, B.K.; Ross, R.L. The Revised Fibromyalgia Impact Questionnaire (FIQR): Validation and psychometric properties. Arthritis Res. Ther. 2009, 11, R120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salgueiro, M.; García-Leiva, J.M.; Ballesteros, J.; Hidalgo, J.; Molina, R.; Calandre, E.P. Validation of a Spanish version of the Revised Fibromyalgia Impact Questionnaire (FIQR). Health Qual. Life Outcomes 2013, 11, 132. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.T.; Steer, R.; Brown, G. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Sanz, J.; García-Vera, M.P. Rendimiento diagnóstico y estructura factorial del Inventario para la Depresión de Beck–II (BDI-II). An. Psicol. 2013, 29, 66–75. [Google Scholar] [CrossRef] [Green Version]
- Plutchik, R.; van Praag, H.M.; Conte, H.R.; Picard, S. Correlates of suicide and violence risk 1: The suicide risk measure. Compr. Psychiat. 1989, 30, 296–302. [Google Scholar] [CrossRef]
- Rubio, G.; Montero, I.; Jáuregui, J.; Villanueva, R.; Marin, J.J.; Santodomingo, J. Validación de la escala de riesgo suicida de Plutchik en población española. Arch. Neurobiol. 1998, 61, 143–152. [Google Scholar]
- Van Orden, K.; Cukrowicz, K.; Witte, T.; Joiner, T.E. Thwarted belongingness and perceived burdensomeness: Construct validity and psychometric properties of the Interpersonal Needs Questionnaire. Psychol. Assess. 2012, 24, 197–215. [Google Scholar] [CrossRef] [Green Version]
- Ordóñez-Carrasco, J.L.; Salgueiro, M.; Sayans-Jiménez, P.; Blanc-Molina, A.; García-Leiva, J.M.; Calandre, E.P.; Rojas, A.J. Psychometric properties of the Spanish version of the 12-item Interpersonal Needs Questionnaire in fibromyalgia syndrome patients. An. Psicol. 2018, 34, 274–282. [Google Scholar] [CrossRef] [Green Version]
- Gilbert, P.; Allan, S. The role of defeat and entrapment (arrested flight) in depression: An exploration of an evolutionary view. Psychol. Med. 1998, 28, 585–598. [Google Scholar] [CrossRef]
- Ordóñez-Carrasco, J.L.; Cuadrado, I.; Rojas, A.J. Adaptación al español de las escalas de derrota y atrapamiento en jóvenes adultos: Propiedades psicométricas. Ter. Psicol. accepted.
- Holden, R.R.; Mehta, K.; Cunningham, E.J.; McLeod, L.D. Development and preliminary validation of a scale of psychache. Can. J. Behav. Sci. 2001, 33, 224–232. [Google Scholar] [CrossRef]
- Ordóñez-Carrasco, J.L.; Cuadrado, I.; Rojas, A.J. Escala de dolor psicológico: Adaptación de la Psychache Scale al español en jóvenes adultos. Rev. Psiquiatr. Salud Ment. 2019. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Weissman, A.; Lester, D.; Trexler, L. The measurement of pessimism: The hopelessness scales. J. Consult. Clin. Psychol. 1974, 42, 861–865. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, E.J.; Hidalgo, M.D.; Cano, R.; López, J.; Campillo, M.; Hernández, J. Estudio prospectivo de la desesperanza en pacientes psicóticos: Características psicométricas de la Escala de Desesperanza de Beck. An. Psiquiatr. 1995, 11, 121–125. [Google Scholar]
- Salaffi, F.; Mozzani, F.; Draghessi, A.; Atzeni, F.; Catellani, R.; Ciapetti, A.; Di Carlo, M.; Sarzi-Puttini, P. Identifying the symptom and functional domains in patients with fibromyalgia: Results of a cross-sectional Internet-based survey in Italy. J. Pain Res. 2016, 9, 279–286. [Google Scholar] [CrossRef] [Green Version]
- Calandre, E.P.; Vilchez, J.S.; Molina-Barea, R.; Tovar, M.I.; García-Leiva, J.M.; Hidalgo, J.; Rodríguez-López, C.M.; Rico-Villademoros, F. Suicide attempts and risk of suicide in patients with fibromyalgia: A survey in Spanish patients. Rheumatology 2011, 50, 1889–1893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, C.; Buchman-Schmitt, J.M.; Stanley, I.H.; Hom, M.A.; Tucker, R.P.; Hagan, C.R.; Rogers, M.L.; Podlogar, M.C.; Chiurliza, B.; Ringer, F.B.; et al. The interpersonal theory of suicide: A systematic review and meta-analysis of a decade of cross-national research. Psychol. Bull. 2017, 143, 1313–1345. [Google Scholar] [CrossRef]
- Ma, J.; Batterham, P.J.; Calear, A.L.; Han, J. A systematic review of the predictions of the Interpersonal–Psychological Theory of Suicidal Behavior. Clin. Psychol. Rev. 2016, 46, 34–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hazeldine-Baker, C.E.; Salkovskis, P.M.; Osborn, M.; Gauntlett-Gilbert, J. Understanding the link between feelings of mental defeat, self-efficacy and the experience of chronic pain. Br. J. Pain 2018, 12, 87–94. [Google Scholar] [CrossRef]
- Tang, N.K.Y.; Beckwith, P.; Ashworth, P. Mental Defeat Is Associated with Suicide Intent in Patients with Chronic Pain. Clin. J. Pain 2016, 32, 411–419. [Google Scholar] [CrossRef] [Green Version]
- Tang, N.K.Y.; Salkovskis, P.M.; Hanna, M. Mental Defeat in Chronic Pain: Initial Exploration of the Concept. Clin. J. Pain 2007, 23, 222–232. [Google Scholar] [CrossRef]
- Ducasse, D.; Holden, R.R.; Boyer, L.; Artéro, S.; Calati, R.; Guillaume, S.; Courtet, P.; Olié, E. Psychological Pain in Suicidality: A Meta-Analysis. J. Clin. Psychiatry 2018, 79, 16r10732. [Google Scholar] [CrossRef] [PubMed]
- Verrocchio, M.C.; Carrozzino, D.; Marchetti, D.; Andreasson, K.; Fulcheri, M.; Bech, P. Mental Pain and Suicide: A Systematic Review of the Literature. Front. Psychiatry 2016, 7, 108. [Google Scholar] [CrossRef]
- Smith, M.T.; Edwards, R.R.; Robinson, R.C.; Dworkin, R.H. Suicidal ideation, plans, and attempts in chronic pain patients: Factors associated with increased risk. Pain 2004, 111, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Kivimaki, M.; Leino-Arjas, P.; Kaila-Kangas, L.; Virtanen, M.; Elovainio, M.; Puttonen, S.; Keltikangas-Järvinen, L.; Pentti, J.; Vahtera, J. Increased absence due to sickness among employees with fibromyalgia. Ann. Rheum. Dis. 2006, 66, 65–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, A.T.; Brown, G.K.; Steer, R.A. Psychometric characteristics of the Scale for Suicide Ideation with psychiatric outpatients. Behav. Res. Ther. 1997, 35, 1039–1046. [Google Scholar] [CrossRef]
- Green, J.; Berry, K.; Danquah, A.; Pratt, D. The role of psychological and social factors in the relationship between attachment and suicide: A systematic review. Clin. Psychol. Psychother. 2020, 27, 463–488. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Galynker, I.I.; Briggs, J.; Duffy, M.; Frechette-Hagan, A.; Kim, H.J.; Cohen, L.J.; Yaseen, Z.S. Attachment style and suicide behaviors in high risk psychiatric inpatients following hospital discharge: The mediating role of entrapment. Psychiatry Res. 2017, 257, 309–314. [Google Scholar] [CrossRef]
- Romeo, A.; Di Tella, M.; Ghiggia, A.; Tesio, V.; Fusaro, E.; Geminiani, G.C.; Castelli, L. Attachment style and parental bonding: Relationships with fibromyalgia and alexithymia. PLoS ONE 2020, 15, e0231674. [Google Scholar] [CrossRef]
- Sechi, C.; Vismara, L.; Brennstuhl, M.J.; Tarquinio, C.; Lucarelli, L. Adult attachment styles, self-esteem, and quality of life in women with fibromyalgia. Health Psychol. Open 2020, 7. [Google Scholar] [CrossRef]
- Kleiman, E.M. Suicidal thinking as a valuable clinical endpoint. EClinicalMedicine 2020, 23, 100399. [Google Scholar] [CrossRef]
- Luoma, J.B.; Martin, C.E.; Pearson, J.L. Contact with mental health and primary care providers before suicide: A review of the evidence. Am. J. Psychiatry 2002, 159, 909–916. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total [N (%)] | Cluster 1 (Low Vulnerability) [N (%)] | Cluster 2 (High Vulnerability) [N (%)] | p-Value (Cluster 1 vs. Cluster 2) | |
|---|---|---|---|---|
| Age | M = 49.82; SD = 10.10 | M = 50.25; SD = 11.15 | M = 49.45; SD = 9.13 | 0.634 * |
| Sex | 0.144 ** | |||
| Woman | 134 (91.2%) | 64 (92.8%) | 70 (89.7%) | |
| Man | 13 (8.8%) | 5 (7.2%) | 8 (10.3%) | |
| Completed education level | 0.278 ** | |||
| No studies | 3 (2%) | 1 (1.4%) | 2 (2.6%) | |
| Primary education | 20 (13.6%) | 8 (11.6%) | 12 (15.4%) | |
| Secondary education | 80 (54.4%) | 34 (49.3%) | 46 (59.0%) | |
| Higher education | 44 (29.9%) | 26 (37.7%) | 18 (23.1%) | |
| Work activity | 0.005 ** | |||
| Unemployed | 29 (19.7%) | 9 (13.0%) | 20 (25.6%) | |
| Student | 4 (2.7%) | 2 (2.9%) | 2 (2.6%) | |
| Homemaker | 20 (13.6%) | 8 (11.6%) | 12 (15.4%) | |
| Employee | 55 (37.4%) | 30 (43.5%) | 25 (32.1%) | |
| Sick leaved | 14 (9.5%) | 2 (2.9%) | 12 (15.4%) | |
| Retired/Pensioner/Rentist | 25 (17.0%) | 18 (26.1%) | 7 (9.0%) | |
| Civil status | 0.291 ** | |||
| Single | 28 (20.1%) | 13 (19.4%) | 15 (20.8%) | |
| Stable partner | 15 (10.8%) | 6 (9.0%) | 9 (12.5%) | |
| Married | 76 (54.7%) | 42 (62.7%) | 34 (47.2%) | |
| Divorced | 18 (12.9%) | 5 (7.5%) | 13 (18.1%) | |
| Widowed | 2 (1.4%) | 1 (1.5%) | 1 (1.4%) | |
| Religion | 0.192 ** | |||
| Catholic | 76 (53.9%) | 36 (52.9%) | 40 (54.8%) | |
| Orthodox | 2 (1.4%) | 2 (2.9%) | - | |
| Protestant | 2 (1.4%) | 2 (2.9%) | - | |
| Agnostic | 13 (9.2%) | 8 (11.8%) | 5 (6.8%) | |
| Atheist | 24 (17.0%) | 8 (11.8%) | 16 (21.9%) | |
| Indifferent | 24 (17.0%) | 12 (17.6%) | 12 (16.4%) |
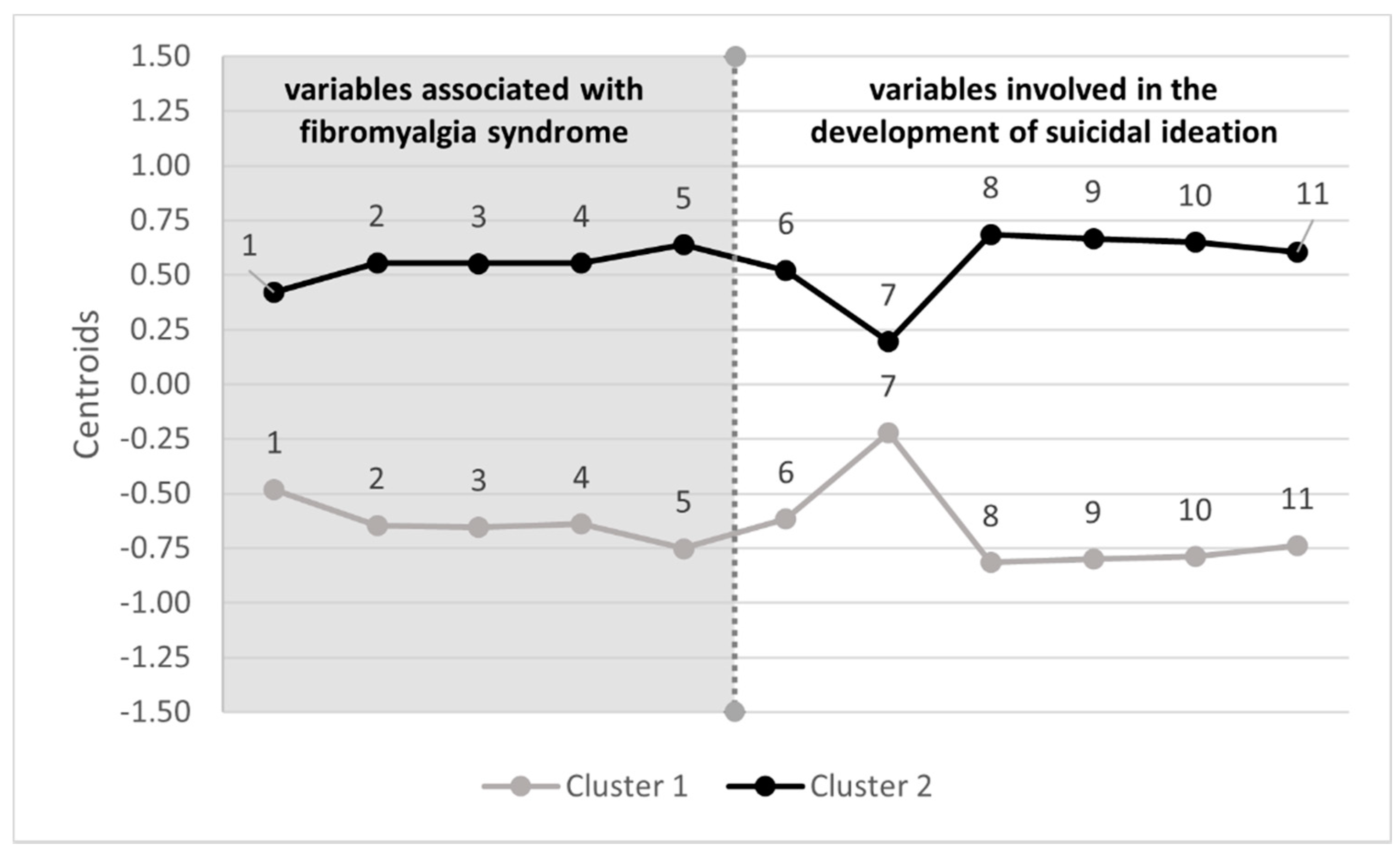
| Variables | Cluster 1 (Low Vulnerability) | Cluster 2 (High Vulnerability) | F | p-Value | ||
|---|---|---|---|---|---|---|
| Centroids | Mean (Standard Deviation) | Centroids | Mean (Standard Deviation) | |||
| Physical function difficulty (FIQ-R) | −0.48 | 15.38 (7.08) | 0.42 | 21.69 (5.39) | 38.526 | <0.001 |
| Overall FM impact (FIQ-R) | −0.64 | 9.54 (4.88) | 0.56 | 15.80 (3.48) | 84.251 | <0.001 |
| Intensity of associated symptoms (FIQ-R) | −0.65 | 22.30 (8.75) | 0.55 | 33.54 (6.24) | 84.291 | <0.001 |
| Physical pain (FIQ-R) | −0.64 | 5.71 (2.38) | 0.56 | 8.60 (1.46) | 83.429 | <0.001 |
| Severity depressive symptomatology (BDI-II) | −0.75 | 19.74 (6.91) | 0.64 | 34.89 (8.67) | 137.259 | <0.001 |
| Perceived burdensomeness (INQ) | −0.62 | 10.52 (4.81) | 0.52 | 22.33 (10.79) | 70.676 | <0.001 |
| Thwarted belongingness (INQ) | −0.22 | 13.80 (6.53) | 0.19 | 16.49 (6.19) | 6.730 | 0.010 |
| Defeat (DS) | −0.82 | 21.13 (10.12) | 0.69 | 42.77 (9.17) | 189.687 | <0.001 |
| Entrapment (ES) | −0.80 | 18.87 (11.07) | 0.67 | 42.46 (11.00) | 171.460 | <0.001 |
| Psychological Pain (PS) | −0.79 | 32.94 (9.12) | 0.65 | 49.80 (7.27) | 159.770 | <0.001 |
| Hopelessness (BHS) | −0.74 | 5.59 (4.32) | 0.61 | 13.55 (4.46) | 122.793 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ordóñez-Carrasco, J.L.; Sánchez-Castelló, M.; Calandre, E.P.; Cuadrado-Guirado, I.; Rojas-Tejada, A.J. Suicidal Ideation Profiles in Patients with Fibromyalgia Using Transdiagnostic Psychological and Fibromyalgia-Associated Variables. Int. J. Environ. Res. Public Health 2021, 18, 209. https://doi.org/10.3390/ijerph18010209
Ordóñez-Carrasco JL, Sánchez-Castelló M, Calandre EP, Cuadrado-Guirado I, Rojas-Tejada AJ. Suicidal Ideation Profiles in Patients with Fibromyalgia Using Transdiagnostic Psychological and Fibromyalgia-Associated Variables. International Journal of Environmental Research and Public Health. 2021; 18(1):209. https://doi.org/10.3390/ijerph18010209
Chicago/Turabian StyleOrdóñez-Carrasco, Jorge L., María Sánchez-Castelló, Elena P. Calandre, Isabel Cuadrado-Guirado, and Antonio J. Rojas-Tejada. 2021. "Suicidal Ideation Profiles in Patients with Fibromyalgia Using Transdiagnostic Psychological and Fibromyalgia-Associated Variables" International Journal of Environmental Research and Public Health 18, no. 1: 209. https://doi.org/10.3390/ijerph18010209
APA StyleOrdóñez-Carrasco, J. L., Sánchez-Castelló, M., Calandre, E. P., Cuadrado-Guirado, I., & Rojas-Tejada, A. J. (2021). Suicidal Ideation Profiles in Patients with Fibromyalgia Using Transdiagnostic Psychological and Fibromyalgia-Associated Variables. International Journal of Environmental Research and Public Health, 18(1), 209. https://doi.org/10.3390/ijerph18010209