The Influence of Family Caregivers’ Experience of Interprofessional Care on Their Participation in Health Checkups as Preventive Health Behavior in Japan—A Cross-Sectional Analysis


Abstract
:1. Introduction
2. Materials and Methods
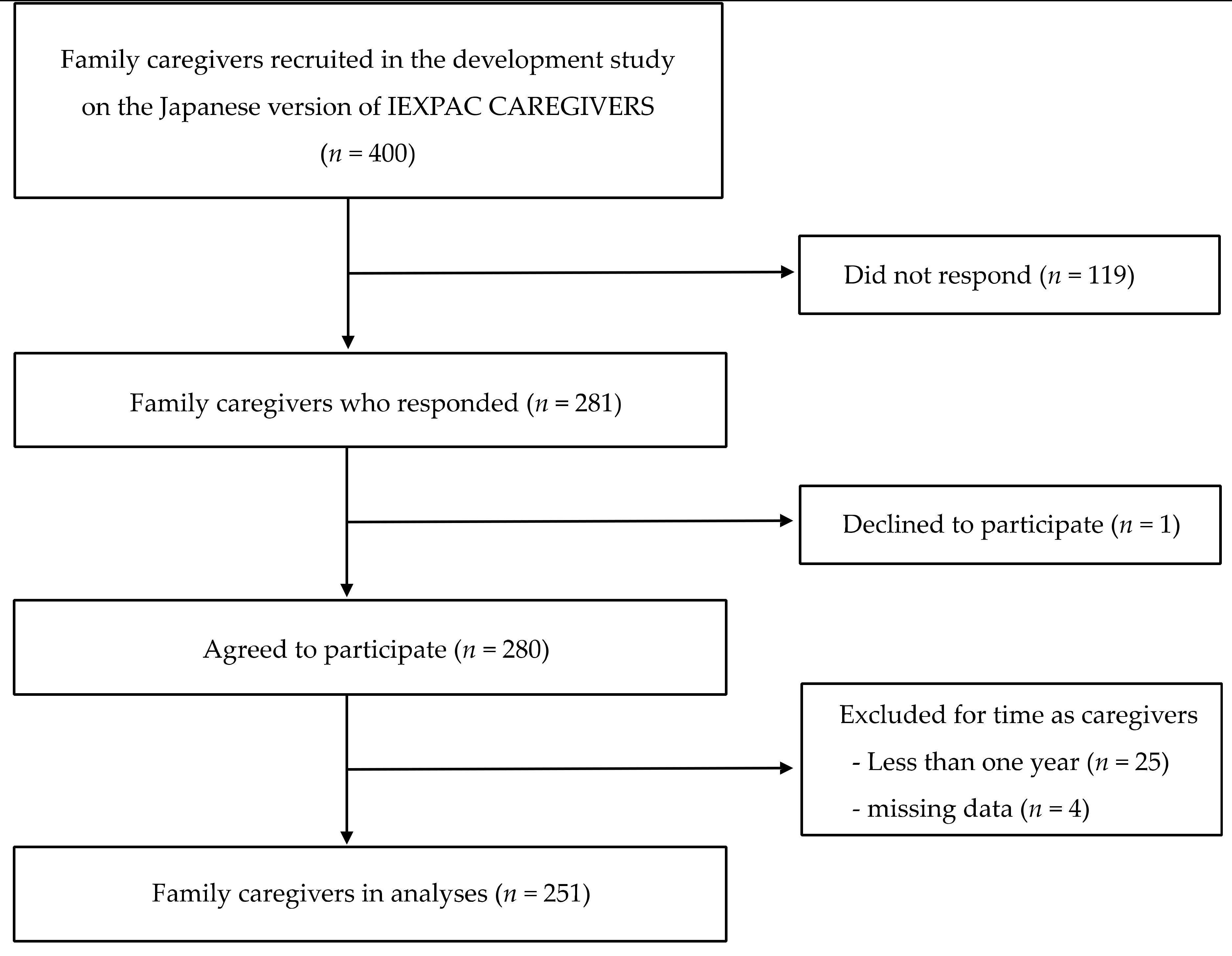
2.1. Participants and Procedures
2.2. Outcome Variable
2.3. Family Caregivers’ Experience of Interprofessional Care
2.4. Other Variables
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Collins, L.G.; Swartz, K. Caregiver care. Am. Fam. Physician 2011, 83, 1309–1317. [Google Scholar] [PubMed]
- Adelman, R.D.; Tmanova, L.L.; Delgado, D.; Dion, S.; Lachs, M.S. Caregiver burden: A clinical review. JAMA 2014, 311, 1052–1060. [Google Scholar] [CrossRef] [PubMed]
- Schulz, R.; Czaja, S.J. Family Caregiving: A Vision for the Future. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2018, 26, 358–363. [Google Scholar] [CrossRef]
- McKeown, L.P.; Porter-Armstrong, A.P.; Baxter, G.D. The needs and experiences of caregivers of individuals with multiple sclerosis: A systematic review. Clin. Rehabil. 2003, 17, 234–248. [Google Scholar] [CrossRef]
- Oliveira, D.; Sousa, L.; Orrell, M. Improving health-promoting self-care in family carers of people with dementia: A review of interventions. Clin. Interv. Aging 2019, 14, 515–523. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Caregiving for Family and Friends—A Public Health Issue. Available online: https://www.cdc.gov/aging/caregiving/caregiver-brief.html (accessed on 3 November 2020).
- Krogsbøll, L.T.; Jørgensen, K.J.; Gøtzsche, P.C. General health checks in adults for reducing morbidity and mortality from disease. Cochrane Database Syst. Rev. 2019, 1, Cd009009. [Google Scholar] [CrossRef]
- Lee, S.; Colditz, G.A.; Berkman, L.F.; Kawachi, I. Caregiving and risk of coronary heart disease in US women—A prospective study. Am. J. Prev. Med. 2003, 24, 113–119. [Google Scholar] [CrossRef]
- Miyawaki, A.; Tomio, J.; Kobayashi, Y.; Takahashi, H.; Noguchi, H.; Tamiya, N. Impact of long-hours family caregiving on non-fatal coronary heart disease risk in middle-aged people: Results from a longitudinal nationwide survey in Japan. Geriatr. Gerontol. Int. 2017, 17, 2109–2115. [Google Scholar] [CrossRef] [Green Version]
- OECD. Health Check-Ups in Japan. Available online: https://doi.org/10.1787/9789264311602-7-en (accessed on 2 August 2020).
- Nakanishi, N.; Tatara, K.; Tatatorige, T.; Murakami, S.; Shinsho, F. Effects of preventive health services on survival of the elderly living in a community in Osaka, Japan. J. Epidemiol. Community Health 1997, 51, 199–204. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.M.; Goto, R.; Sonoda, T.; Sakauchi, F.; Washio, M.; Kobayashi, K.; Mori, M. Impact of health education and screening over all-cause mortality in Japan: Evidence from a cohort study during 1984-2002. Prev. Med. 2004, 38, 786–792. [Google Scholar] [CrossRef]
- Torimoto-Sasai, Y.; Igarashi, A.; Wada, T.; Ogata, Y.; Yamamoto-Mitani, N. Female family caregivers face a higher risk of hypertension and lowered estimated glomerular filtration rates: A cross-sectional, comparative study. BMC Public Health 2015, 15, 177. [Google Scholar] [CrossRef] [Green Version]
- Sugiyama, T.; Tamiya, N.; Watanabe, T.; Wakui, T.; Shibayama, T.; Moriyama, Y.; Yamaoka, Y.; Noguchi, H. Association of care recipients’ care-need level with family caregiver participation in health check-ups in Japan. Geriatr. Gerontol. Int. 2018, 18, 26–32. [Google Scholar] [CrossRef] [Green Version]
- Wills, T.A.; Ainette, M.C. Social networks and social support. In Handbook of Health Psychology, 2nd ed.; Baum, A., Revenson, T.A., Singer, J., Eds.; Psychology Press: New York, NY, USA, 2012; pp. 465–492. [Google Scholar]
- Messina, C.R.; Lane, D.S.; Glanz, K.; West, D.S.; Taylor, V.; Frishman, W.; Powell, L. Relationship of social support and social burden to repeated breast cancer screening in the women’s health initiative. Health Psychol. 2004, 23, 582–594. [Google Scholar] [CrossRef]
- Silva, I.T.E.; Griep, R.H.; Rotenberg, L. Social support and cervical and breast cancer screening practices among nurses. Rev. Lat. Am. Enferm. 2009, 17, 514–521. [Google Scholar] [CrossRef] [Green Version]
- Documet, P.; Bear, T.M.; Flatt, J.D.; Macia, L.; Trauth, J.; Ricci, E.M. The Association of Social Support and Education with Breast and Cervical Cancer Screening. Health Educ. Behav. 2015, 42, 55–64. [Google Scholar] [CrossRef] [Green Version]
- Holt-Lunstad, J.; Uchino, B.N. Social Support and Health. In Health Behavior: Theory, Research, and Practice, 5th ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2015; pp. 183–204. [Google Scholar]
- Williams, S.W.; Dilworth-Anderson, P. Systems of social support in families who care for dependent African American elders. Gerontologist 2002, 42, 224–236. [Google Scholar] [CrossRef] [Green Version]
- Shiba, K.; Kondo, N.; Kondo, K. Informal and Formal Social Support and Caregiver Burden: The AGES Caregiver Survey. J. Epidemiol. 2016, 26, 622–628. [Google Scholar] [CrossRef] [Green Version]
- Kuluski, K.; Nelson, M.L.A.; Tracy, C.S.; Alloway, C.A.; Shorrock, C.; Shearkhani, S.; Upshur, R.E.G. Experience of Care as a Critical Component of Health System Performance Measurement: Recommendations for Moving Forward. HealthcarePapers 2017, 17, 8–20. [Google Scholar] [CrossRef] [Green Version]
- Rose, J.H.; Bowman, K.F.; O’Toole, E.E.; Abbott, K.; Love, T.E.; Thomas, C.; Dawson, N.V. Caregiver objective burden and assessments of patient-centered, family-focused care for frail elderly veterans. Gerontologist 2007, 47, 21–33. [Google Scholar] [CrossRef]
- Nakayama, G.; Masumoto, S.; Haruta, J.; Maeno, T. Measuring family caregivers’ experience of interprofessional care for patients and families: Development of the Japanese version of the Caregivers’ Experience Instrument. Fam. Pract. 2020, 37, 854–861. [Google Scholar] [CrossRef]
- Guilabert, M.; Amil, P.; Gonzalez-Mestre, A.; Gil-Sanchez, E.; Vila, A.; Contel, J.C.; Ansotegui, J.C.; Solas, O.; Bacigalupe, M.T.; Fernandez-Cano, P.; et al. The Measure of the Family Caregivers’ Experience. Int. J. Environ. Res. Public Health 2018, 15. [Google Scholar] [CrossRef] [Green Version]
- Anhang Price, R.; Elliott, M.N.; Zaslavsky, A.M.; Hays, R.D.; Lehrman, W.G.; Rybowski, L.; Edgman-Levitan, S.; Cleary, P.D. Examining the role of patient experience surveys in measuring health care quality. Med. Care Res. Rev. MCRR 2014, 71, 522–554. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Innovative Care for Chronic Conditions: Building Blocks for Actions: Global Report 2002. Available online: https://apps.who.int/iris/handle/10665/42500 (accessed on 2 August 2020).
- American Academy of Family Physicians. Definition of Family 1984. Available online: https://www.aafp.org/about/policies/all/family-definition.html (accessed on 2 August 2020).
- Ministry of Health, Labour and Welfare. Comprehensive Survey of Living Conditions: Health of Household Members. 2016. Available online: https://www.mhlw.go.jp/toukei/chousahyo/koku28ke.pdf (accessed on 2 August 2020).
- Mira, J.J.; Nuno-Solinis, R.; Guilabert-Mora, M.; Solas-Gaspar, O.; Fernandez-Cano, P.; Gonzalez-Mestre, M.A.; Contel, J.C.; Del Rio-Camara, M. Development and Validation of an Instrument for Assessing Patient Experience of Chronic Illness Care. Int. J. Integr. Care 2016, 16, 13. [Google Scholar] [CrossRef] [Green Version]
- Miyawaki, A.; Tanaka, H.; Kobayashi, Y.; Kawachi, I. Informal caregiving and mortality―Who is protected and who is not? A prospective cohort study from Japan. Soc. Sci. Med. 2019, 223, 24–30. [Google Scholar] [CrossRef]
- Arai, Y.; Tamiya, N.; Yano, E. The short version of the Japanese version of the Zarit Caregiver Burden Interview (J-ZBI_8): Its reliability and validity. Nihon Ronen Igakkai Zasshi Jpn. J. Geriatr. 2003, 40, 497–503. [Google Scholar] [CrossRef] [Green Version]
- Arai, Y.; Zarit, S.H. Determining a cutoff score of caregiver burden for predicting depression among family caregivers in a large population-based sample. Int. J. Geriatr. Psychiatry 2014, 29, 1313–1315. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Long-Term Care Insurance System of Japan 2016. Available online: https://www.mhlw.go.jp/english/policy/care-welfare/care-welfare-elderly/dl/ltcisj_e.pdf (accessed on 3 November 2020).
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstein, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Tang, Y.Y.; Chen, S.P. Health promotion behaviors in Chinese family caregivers of patients with stroke. Health Promot. Int. 2002, 17, 329–339. [Google Scholar] [CrossRef] [Green Version]
- McDaniel, S.H.; Campbell, T.L.; Hepworth, J.; Lorenz, A. Family-Oriented Primary Care, 2nd ed.; Springer: New York, NY, USA, 2005; pp. 242–260. [Google Scholar]
- Aoki, T.; Inoue, M. Primary care patient experience and cancer screening uptake among women: An exploratory cross-sectional study in a Japanese population. Asia Pac. Fam. Med. 2017, 16, 3. [Google Scholar] [CrossRef] [Green Version]
- Flocke, S.A.; Stange, K.C.; Zyzanski, S.J. The association of attributes of primary care with the delivery of clinical preventive services. Med. Care 1998, 36, AS21–AS30. [Google Scholar] [CrossRef]
- Van Stralen, K.J.; Dekker, F.W.; Zoccali, C.; Jager, K.J. Confounding. Nephron Clin. Pract. 2010, 116, c143–c147. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Total | Participation in Health Checkups | |||||
|---|---|---|---|---|---|---|---|
| (n = 251) | Yes (n = 182) | No (n = 69) | p Value | ||||
| Caregivers | |||||||
| Gender | |||||||
| Men | 56 | (22.3%) | 41 | (22.5%) | 15 | (21.7%) | 0.893 |
| Women | 195 | (77.7%) | 141 | (77.5%) | 54 | (78.3%) | |
| Data missing | 0 | ||||||
| Education | |||||||
| Less than high school | 21 | (8.4%) | 10 | (5.5%) | 11 | (15.9%) | 0.019 |
| High school | 126 | (50.2%) | 90 | (50.0%) | 36 | (52.2%) | |
| Junior college or vocational college | 61 | (24.3%) | 46 | (25.6%) | 15 | (21.7%) | |
| College or graduate school | 40 | (15.9%) | 34 | (18.9%) | 6 | (8.7%) | |
| Data missing | 3 | ||||||
| Equivalent income (million Japanese yen) | |||||||
| Q1 (<1.06) | 62 | (24.7%) | 30 | (16.5%) | 32 | (46.4%) | <0.001 |
| Q2 (1.06–2.01) | 59 | (23.5%) | 43 | (23.6%) | 16 | (23.2%) | |
| Q3 (2.02–3.16) | 56 | (22.3%) | 41 | (22.5%) | 15 | (21.7%) | |
| Q4 (≥3.17) | 66 | (26.3%) | 61 | (33.5%) | 5 | (7.2%) | |
| Data missing | 8 | ||||||
| Patients | |||||||
| Care-need level | |||||||
| Lower (support required 1 and 2) | 36 | (14.3%) | 25 | (13.7%) | 11 | (15.9%) | 0.277 |
| Middle (care required 1–3) | 155 | (61.8%) | 118 | (64.8%) | 37 | (53.6%) | |
| Higher (care required 4 and 5) | 55 | (21.9%) | 36 | (19.8%) | 19 | (27.5%) | |
| Data missing | 5 | ||||||
| Caregivers | Median (IQR) | ||||||
| Age (years, n = 251) | 64 | (58–70) | 63 | (58–69) | 66 | (57–72.5) | 0.078 |
| Caregiver burden score (points, n = 247) | 11 | (6–17) | 11 | (6–16) | 10.5 | (5–18) | 0.834 |
| Family Caregiver Participation in Health Checkups | 95% CI | p | |||
|---|---|---|---|---|---|
| Total (n = 234) | Yes (n = 170) | No (n = 64) | |||
| J-IEXPAC CAREGIVERS Total score 2 | 40.5 (8.8) | 41.3 (8.5) | 38.4 (9.1) | 0.4–5.4 | 0.025 |
| Total (n = 241) | Yes (n = 175) | No (n = 66) | |||
| Domain score Attention for the patient 3 | 25.6 (5.3) | 26.1 (5.1) | 24.3 (5.6) | 0.3–3.3 | 0.019 |
| Total (n = 247) | Yes (n = 179) | No (n = 68) | |||
| Domain score Attention for the caregiver 4 | 12.9 (3.3) | 13.2 (3.3) | 12.2 (3.3) | 0.1–2.0 | 0.032 |
| OR | (95% CI) | p Value | |
|---|---|---|---|
| J-IEXPAC CAREGIVERS total score 1 | 1.05 | (1.01–1.09) | 0.013 |
| Gender | |||
| Men | Reference | ||
| Women | 1.07 | (0.49–2.35) | 0.864 |
| Age (years) | 1.01 | (0.97–1.05) | 0.683 |
| Education | |||
| Less than high school | Reference | ||
| High school | 1.63 | (0.58–4.57) | 0.357 |
| Junior college or vocational college | 1.19 | (0.35–4.04) | 0.785 |
| College or graduate school | 2.35 | (0.60–9.87) | 0.244 |
| Equivalent income (million Japanese yen) | |||
| Q1 (<1.06) | Reference | ||
| Q2 (1.06–2.01) | 2.54 | (1.12–5.74) | 0.026 |
| Q3 (2.02–3.16) | 2.76 | (1.21–6.32) | 0.016 |
| Q4 (≥3.17) | 15.21 | (4.71–49.15) | <0.001 |
| Caregiver burden score 1 | 0.99 | (0.95–1.04) | 0.732 |
| Care-need level | |||
| Lower (support required 1 and 2) | Reference | ||
| Middle (care required 1–3) | 1.41 | (0.57–3.51) | 0.457 |
| Higher (care required 4 and 5) | 0.59 | (0.21–1.66) | 0.317 |
| OR | (95% CI) | p Value | |
|---|---|---|---|
| Attention for the patient 1 | 1.08 | (1.01–1.15) | 0.016 |
| Gender | |||
| Men | Reference | ||
| Women | 1.07 | (0.49–2.33) | 0.874 |
| Age (years) | 1.01 | (0.97–1.05) | 0.662 |
| Education | |||
| Less than high school | Reference | ||
| High school | 1.58 | (0.56–4.45) | 0.386 |
| Junior college or vocational college | 1.13 | (0.33–3.84) | 0.847 |
| College or graduate school | 2.10 | (0.50–8.77) | 0.313 |
| Equivalent income (million Japanese yen) | |||
| Q1 (<1.06) | Reference | ||
| Q2 (1.06–2.01) | 2.61 | (1.15–5.92) | 0.026 |
| Q3 (2.02–3.16) | 2.91 | (1.27–6.64) | 0.016 |
| Q4 (≥3.17) | 15.50 | (4.79–49.99) | <0.001 |
| Caregiver burden score 1 | 0.99 | (0.95–1.04) | 0.723 |
| Care-need level | |||
| Lower (support required 1 and 2) | Reference | ||
| Middle (care required 1–3) | 1.40 | (0.56–3.46) | 0.470 |
| Higher (care required 4 and 5) | 0.58 | (0.21–1.64) | 0.307 |
| Attention for the caregiver 1 | 1.12 | (1.02–1.24) | 0.023 |
| Gender | |||
| Men | Reference | ||
| Women | 1.10 | (0.50–2.40) | 0.819 |
| Age (years) | 1.01 | (0.97–1.05) | 0.708 |
| Education | |||
| Less than high school | Reference | ||
| High school | 1.68 | (0.60–4.73) | 0.323 |
| Junior college or vocational college | 1.20 | (0.35–4.11) | 0.768 |
| College or graduate school | 2.60 | (0.61–10.98) | 0.195 |
| Equivalent income (million Japanese yen) | |||
| Q1 (<1.06) | Reference | ||
| Q2 (1.06–2.01) | 2.51 | (1.11–5.67) | 0.026 |
| Q3 (2.02–3.16) | 2.64 | (1.15–6.06) | 0.016 |
| Q4 (≥3.17) | 15.01 | (4.66–48.36) | <0.001 |
| Caregiver burden score1 | 0.99 | (0.95–1.04) | 0.731 |
| Care-need level | |||
| Lower (support required 1 and 2) | Reference | ||
| Middle (care required 1–3) | 1.39 | (0.56–3.45) | 0.473 |
| Higher (care required 4 and 5) | 0.61 | (0.22–1.70) | 0.344 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakayama, G.; Masumoto, S.; Haruta, J.; Maeno, T. The Influence of Family Caregivers’ Experience of Interprofessional Care on Their Participation in Health Checkups as Preventive Health Behavior in Japan—A Cross-Sectional Analysis. Int. J. Environ. Res. Public Health 2021, 18, 223. https://doi.org/10.3390/ijerph18010223
Nakayama G, Masumoto S, Haruta J, Maeno T. The Influence of Family Caregivers’ Experience of Interprofessional Care on Their Participation in Health Checkups as Preventive Health Behavior in Japan—A Cross-Sectional Analysis. International Journal of Environmental Research and Public Health. 2021; 18(1):223. https://doi.org/10.3390/ijerph18010223
Chicago/Turabian StyleNakayama, Gen, Shoichi Masumoto, Junji Haruta, and Tetsuhiro Maeno. 2021. "The Influence of Family Caregivers’ Experience of Interprofessional Care on Their Participation in Health Checkups as Preventive Health Behavior in Japan—A Cross-Sectional Analysis" International Journal of Environmental Research and Public Health 18, no. 1: 223. https://doi.org/10.3390/ijerph18010223
APA StyleNakayama, G., Masumoto, S., Haruta, J., & Maeno, T. (2021). The Influence of Family Caregivers’ Experience of Interprofessional Care on Their Participation in Health Checkups as Preventive Health Behavior in Japan—A Cross-Sectional Analysis. International Journal of Environmental Research and Public Health, 18(1), 223. https://doi.org/10.3390/ijerph18010223