Demographic Assessment of Down Syndrome: A Systematic Review



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
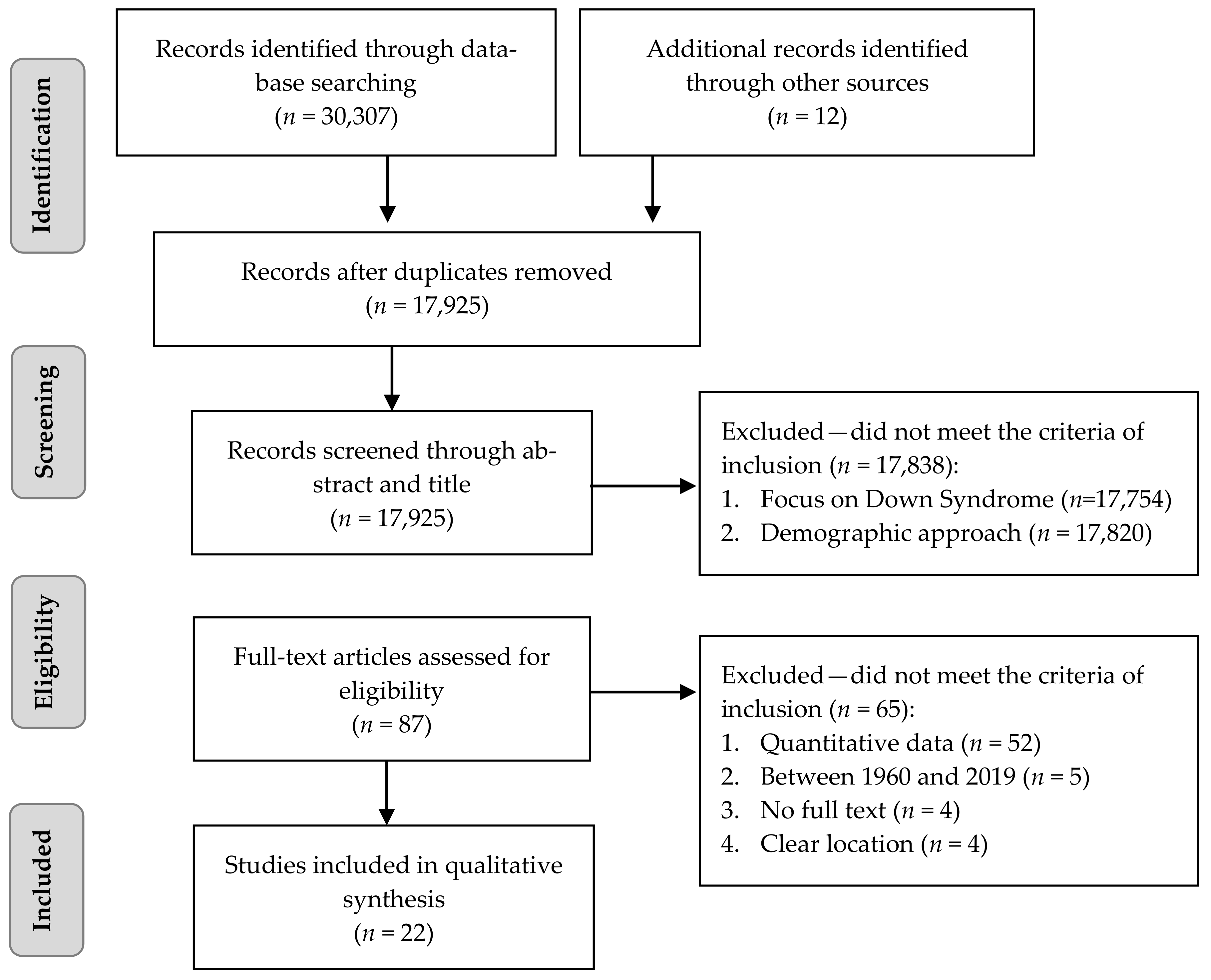
2.3. Screening and Selection Process
2.4. Quality Measurement
2.5. Data Analysis
3. Results
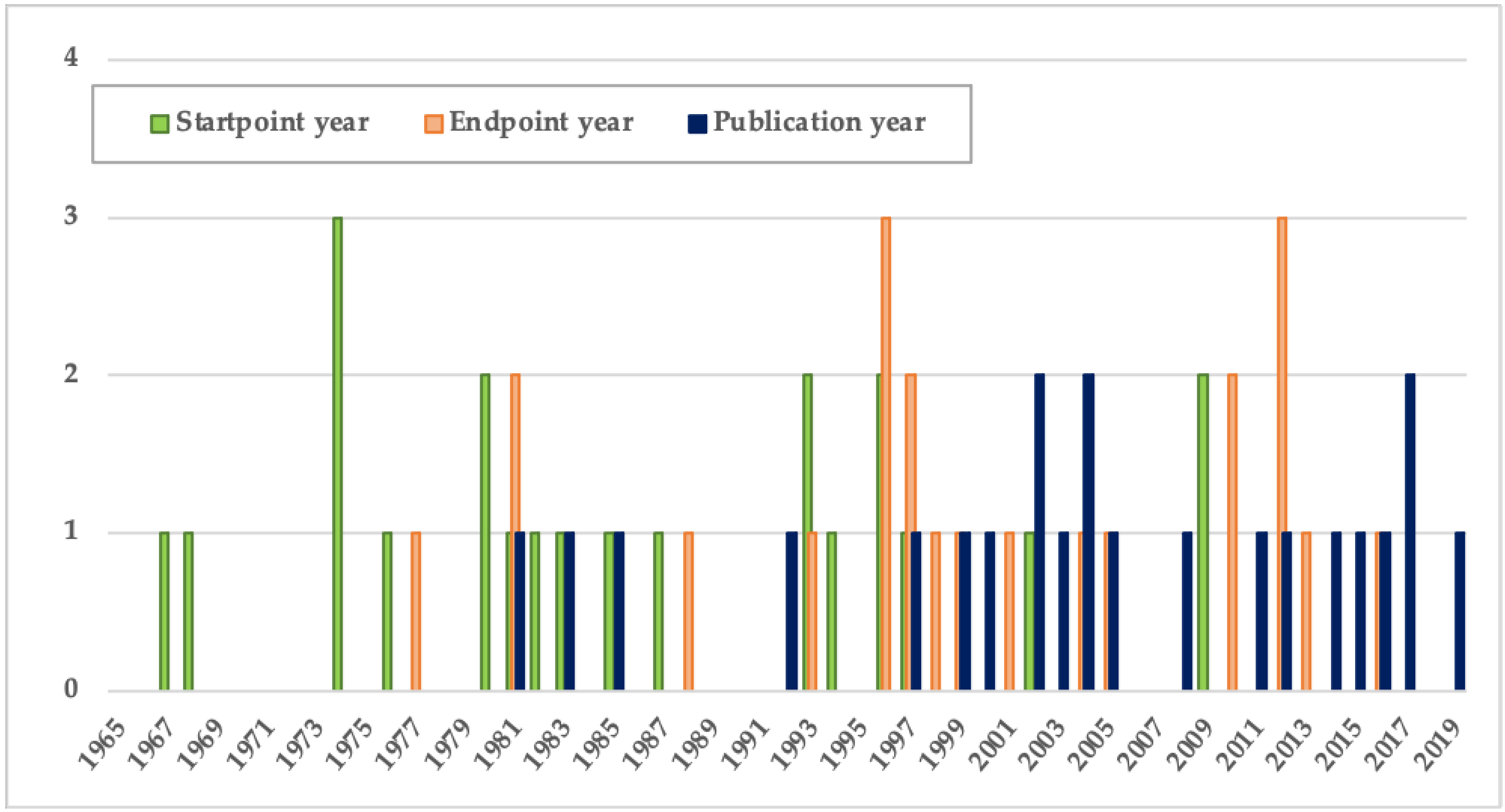
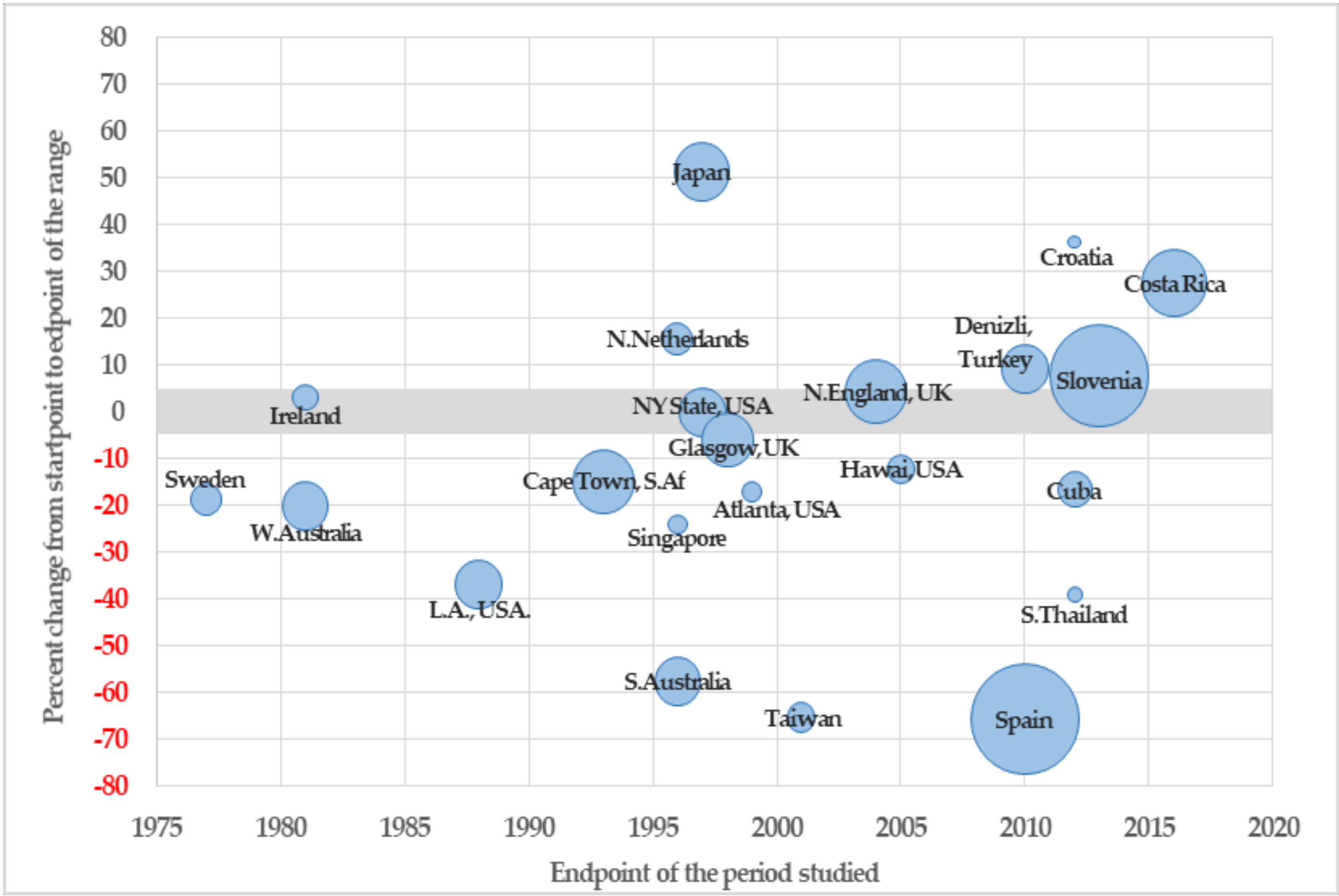
3.1. Trends in Demographics of Down Syndrome
3.2. Screening Tests and Prenatal Care
3.3. Related Variables: Maternal Age, Legal and Sociocultural Contexts
3.4. Sources for Demographic Assessment of Down Syndrome
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| S48 | S24 and S47 | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S47 | S33 or S34 or S35 or S36 or S37 or S38 or S39 or S40 or S41 or S42 or S43 or S44 or S45 | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S46 | S9 and S32 | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S45 | AB* antenatal testing | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S44 | TI** antenatal testing | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S43 | TI antenatal screening | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S42 | AB antenatal screening | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S41 | AB prenatal screening | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S40 | TI prenatal screening | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S39 | AB prenatal screening | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S38 | AB antenatal diagnosis | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S37 | TI antenatal diagnosis | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S36 | TI prenatal testing | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S35 | AB prenatal testing | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S34 | TI prenatal diagnosis | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S33 | AB prenatal diagnosis | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S32 | S26 or S27 or S28 or S29 or S30 or S31 | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S31 | antenatal testing | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S30 | antenatal diagnosis | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S29 | antenatal screening | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S28 | prenatal screening | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S27 | prenatal testing | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S26 | prenatal diagnosis | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S25 | S14 n1 S23 | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S24 | S14 and S23 | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S23 | (S15 or S16 or S17 or S18 or S19 or S20 or S21 or S22) | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S22 | TI prevalence | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S21 | AB prevalence | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S20 | AB incidence | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S19 | TI incidence | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S18 | TI demographic characteristics | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S17 | AB demographic characteristics | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S16 | AB epidemiology | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S15 | TI epidemiology | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S14 | S10 or S11 or S12 or S13 | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S13 | AB down’s syndrome | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S12 | TI down’s syndrome | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S11 | TI trisomy 21 | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S10 | AB trisomy 21 | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S9 | S7 and S8 | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S8 | S3 or S4 or S5 or S6 | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S7 | S1 or S2 | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S6 | prevalence | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S5 | incidence | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S4 | demography | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S3 | epidemiology | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S2 | trisomy 21 | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
| S1 | down’s syndrome | Expanders—Apply equivalent subjects/Search modes—Boolean/Phrase |
References
- Afzal, M. Some considerations for demographic assessment of developing countries. Pak. Dev. Rev. 1986, 25, 517–534. [Google Scholar]
- Olsen, C.L.; Cross, P.K.; Gensburg, L.J. Down syndrome: Interaction between culture, demography, and biology in determining the prevalence of a genetic trait. Hum. Biol. 2003, 75, 503–520. [Google Scholar] [CrossRef]
- Santesmases, M.J. Hacia descendencias saludables: Algunos orígenes del diagnóstico prenatal en España. Asclepio. Rev. Hist. Med. Cienc. 2008, 60, 129–150. [Google Scholar] [CrossRef] [Green Version]
- Plaja, A.; Lloveras, D.E.; Cirigliano, V.; Fernandez, D.A.; Barranco, D.L.; Laura, D.; Castells, N.; Cañellas, D.A.; Ordoñez, D.E. Diagnóstico prenatal de las anomalías cromosómicas: Pasado, presente y futuro. Rev. Latinoam. Perinat. 2014, 17, 140–147. [Google Scholar]
- Castro-Volio, I. El diagnóstico prenatal de defectos cromosómicos en Costa Rica. Rev. Biol. Trop. 2004, 54. [Google Scholar] [CrossRef] [Green Version]
- Díaz-Martínez, A.G.; De la Valdés-Abreu, M.C.; Dalmau Díaz, A. Antecedentes y actualidades en el diagnóstico prenatal. Rev. Cuba. Obstet. Ginecol. 1997, 23, 25–30. [Google Scholar]
- Smith, S.K.; Cai, A.; Wong, M.; Sousa, M.S.; Peate, M.; Welsh, A.; Meiser, B.; Kaur, R.; Halliday, J.; Lewis, S.; et al. Improving women’s knowledge about prenatal screening in the era of non-invasive prenatal testing for Down syndrome—Development and acceptability of a low literacy decision aid. BMC Pregnancy Childbirth 2018, 18, 1–14. [Google Scholar] [CrossRef]
- Gadsbøll, K.; Petersen, O.B.; Gatinois, V.; Strange, H.; Jacobsson, B.; Wapner, R.; Vermeesch, J.R.; Vogel, I. Current use of noninvasive prenatal testing in Europe, Australia and the USA: A graphical presentation. Acta Obstet. Gynecol. Scand. 2020, 99, 722–730. [Google Scholar] [CrossRef]
- Loane, M.; Morris, J.K.; Addor, M.-C.; Arriola, L.; Budd, J.; Doray, B.; Garne, E.; Gatt, M.; Haeusler, M.; Khoshnood, B.; et al. Twenty-year trends in the prevalence of Down syndrome and other trisomies in Europe: Impact of maternal age and prenatal screening. Eur. J. Hum. Genet. 2013, 21, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Mulcahy, M.T. The effect of prenatal diagnosis on the incidence of Down syndrome livebirths in the Singapore General Hospital. Aust. N. Z. J. Obstet. Gynaecol. 1983, 23, 38197–38198. [Google Scholar]
- Siffel, C.; Correa, A.; Cragan, J.; Alverson, C.J. Prenatal diagnosis, pregnancy terminations and prevalence of Down Syndrome in Atlanta. Birth Defects Res. Part A Clin. Mol. Teratol. 2004, 70, 565–571. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability and Health: ICD; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- United Nations. Convention on the Rights of Persons with Disabilities; United Nations: New York, NY, USA, 2006. [Google Scholar]
- McDermott, H.; Johnson, J.L. Is the prevalence of Down syndrome births in Hawai’i increasing? Hawaii Med. J. 2011, 70, 72–76. [Google Scholar]
- Committe on the Rights of Persons with Disabilities. Concluding Observations on the Combined Second and Third Periodic Reports of Spain; Committe on the Rights of Persons with Disabilities: Geneva, Switzerland, 2019. [Google Scholar]
- Wilson, M.G.; Chan, L.S.; Herbert, W.S. Birth prevalence of down syndrome in a predominantly Latino population: A 15-year study. Teratology 1992, 45, 285–292. [Google Scholar] [CrossRef]
- Glivetic, T.; Rodin, U.; Milosevic, M.; Mayer, D.; Filipovic-Grcic, B.; Saric, M.S. Prevalence, prenatal screening and neonatal features in children with Down syndrome: A registry-based national study. Ital. J. Pediatr. 2015, 41, 81. [Google Scholar] [CrossRef] [Green Version]
- Benavides-lara, A.; de la Barboza-Argüello, M.P. Prevalencia al nacimiento de síndrome de Down, según edad materna en Costa Rica, 1996–2016. Acta Med. Costarric. 2019, 4, 177–182. [Google Scholar]
- Acikbas, I.; Tomatir, A.G.; Akdag, B.; Koksal, A. Retrospective analysis of live birth prevalence of children with Down syndrome in Denizli, Turkey. Genet. Mol. Res. 2012, 11, 4640–4645. [Google Scholar] [CrossRef]
- Rudolf, G.; Tul, N.; Verdenik, I.; Volk, M.; Brezigar, A.; Vokac, N.K.; Jeršin, N.; Prosenc, B.; Sršen, T.P.; Peterlin, B. Impact of prenatal screening on the prevalence of down syndrome in Slovenia. PLoS ONE 2017, 12, 1–8. [Google Scholar] [CrossRef]
- Huete García, A. Demografía e inclusión social de las personas con síndrome de Down. Rev. Síndrome Down Rev. Española Investig. Inf. Sobre Síndrome Down 2016, 33, 38–50. [Google Scholar]
- Jaruratanasirikul, S.; Kor-anantakul, O.; Chowvichian, M.; Limpitikul, W.; Dissaneevate, P.; Intharasangkanawin, N.; Sattapanyo, A.; Pathompanitrat, S.; Sriplung, H. A population-based study of prevalence of Down syndrome in Southern Thailand. World J. Pediatr. 2017, 13, 63–69. [Google Scholar] [CrossRef]
- Méndez-Rosado, L.A.; Hechavarría-Estenoz, D.; de la Torre, M.E.; Pimentel-Benitez, H.; Hernández-Gil, J.; Perez, B.; Barrios-Martínez, A.; Morales-Rodriguez, E.; Soriano-Torres, M.; Garcia, M.; et al. Current status of prenatal diagnosis in Cuba: Causes of low prevalence of Down syndrome. Prenat. Diagn. 2014, 34, 1049–1054. [Google Scholar] [CrossRef]
- Molteno, C.; Smart, R.; Viljoen, D.; Sayed, R.; Roux, A. Twenty-year birth prevalence of Down syndrome in Cape Town, South Africa. Paediatr. Perinat. Epidemiol. 1997, 11, 428–435. [Google Scholar] [CrossRef]
- Wortelboer, M.J.M.; De Wolf, B.T.H.M.; Verschuuren-Bemelmans, C.C.; Reefhuis, J.; Mantingh, A.; Beekhuis, J.R.; Cornel, M.C. Trends in live birth prevalence of Down syndrome in the Northern Netherlands 1987-96: The impact of screening and prenatal diagnosis. Prenat. Diagn. 2000, 20, 709–713. [Google Scholar] [CrossRef]
- Lindsten, J.; Marsk, L.; Berglund, K.; Iselius, L.; Ryman, N.; Annerén, G.; Kjessler, B.; Mitelman, F.; Nordenson, I.; Wahlström, J.; et al. Incidence of Down’s syndrome in Sweden during the years 1968-1977. Hum. Genet. Suppl. 1981, 2, 195–210. [Google Scholar] [CrossRef]
- Cheffins, T.; Chan, A.; Haan, E.A.; Ranieri, E.; Ryall, R.G.; Keane, R.J.; Byron-Scott, R.; Scott, H.; Gjerde, E.M.; Nguyen, A.M.; et al. The impact of maternal serum screening on the birth prevalence of Down’s syndrome and the use of amniocentesis and chorionic villus sampling in South Australia. Br. J. Obstet. Gynaecol. 2000, 107, 1453–1459. [Google Scholar] [CrossRef]
- Lai, F.M.; Woo, B.H.; Tan, K.H.; Huang, J.; Lee, S.T.; Tan, B.Y.; Tan, B.H.; Chew, S.K.; Yeo, G.S.H. Birth Prevalence of Down Syndrome in Singapore from 1993 to 1998. Singap. Med. J. 2002, 43, 70–76. [Google Scholar]
- Jou, H.J.; Kuo, Y.S.; Hsu, J.J.; Shyu, M.K.; Hsieh, T.T.A.; Hsieh, F.J. The evolving national birth prevalence of Down syndrome in Taiwan. A study on the impact of second-trimester maternal serum screening. Prenat. Diagn. 2005, 25, 665–670. [Google Scholar] [CrossRef]
- Iliyasu, Z.; Gilmour, W.; Stone, D. Prevalence of Down Syndrome in Glasgow, 1980-96-the growing impact of prenatal diagnosis on younger mothers. Health Bull. 2002, 60, 60. [Google Scholar]
- Hoshi, N.; Hattori, R.; Hanatani, K.; Okuyama, K.; Yamada, H.; Kishida, T.; Yamada, T.; Sagawa, T.; Sumiyoshi, Y.; Fujimoto, S. Recent trends in the prevalence of Down syndrome in Japan, 1980–1997. Am. J. Med. Genet. 1999, 84, 340–345. [Google Scholar] [CrossRef]
- Irving, C.; Basu, A.; Richmond, S.; Burn, J.; Wren, C. Twenty-year trends in prevalence and survival of Down syndrome. Eur. J. Hum. Genet. 2008, 16, 1336–1340. [Google Scholar] [CrossRef] [Green Version]
- Carothers, A.D.; Hecht, C.A.; Hook, E.B. International variation in reported livebirth prevalence rates of Down syndrome, adjusted for maternal age. J. Med. Genet. 1999, 36, 386–393. [Google Scholar]
- Berastegui, A.; Corral, S. La “ventaja del síndrome de Down” en la Calidad de Vida de Jóvenes con Discapacidad Intelectual. Siglo Cero 2020, 50, 39–51. [Google Scholar]



| N | Study | Region | Years (Range) | Startpoint Birthrate | Endpoint Birthrate | Percent Change | Main Result (*) | Main Cause (**) | Main Source (***) |
|---|---|---|---|---|---|---|---|---|---|
| 1. | Lindsten et al. (1981) | Sweden | 1968–1977 (10) | 14.6 | 11.9 | −18.5 | Descent | Screening | Registry |
| 2. | Mulcahy (1983) | Western Australia | 1967–1981 (15) | 11.4 | 9.1 | −20.2 | Descent | Screening | Registry |
| 3. | Mulcahy (1985) | Ireland | 1974–1981 (8) | 10 | 10.3 | 3.0 | Unclear | - | Registry |
| 4. | Wilson et al. (1992) | Los Angeles (USA) | 1974–1988 (15) | 19.0 | 12.0 | −36.8 | Descent | Screening | Record |
| 5. | Molteno et al. (1997) | Cape Town (S.Africa) | 1974–1993 (20) | 14.2 | 12.1 | −14.8 | Descent | Unclear | Record |
| 6. | Hoshi et al. (1999) | Japan | 1980–1997 (18) | 5.6 | 8.5 | 51.3 | Ascent | Maternal Age | Registry |
| 7. | Cheffins et al. (2000) | South Australia | 1982–1996 (15) | 9.9 | 4.2 | −57.6 | Descent | Screening | Registry |
| 8. | Iliyasu (2002) | Glasgow (UK) | 1980–1996 (17) | 6.7 | 6.3 | −6.0 | Unclear | - | Registry |
| 9. | Lai et al. (2002) | Singapore | 1993–1998 (6) | 11.7 | 8.9 | −23.9 | Descent | Screening | Registry |
| 10. | Olsen et al. (2003) | New York State (USA) | 1983–1997 (15) | 9.9 | 9.9 | 0.0 | Unclear | - | Registry |
| 11. | Siffel et al. (2004) | Atlanta (USA) | 1994–1999 (6) | 12.1 | 10.0 | −17.0 | Descent | Screening | Record/Registry |
| 12. | Wortelboer et al. (2004) | Northern Netherlands | 1987–1996 (10) | 12.8 | 14.8 | 15.6 | Ascent | Maternal Age/Healthcare | Registry |
| 13. | Hei-Jen et al. (2005) | Taiwan | 1993–2001 (9) | 4.6 | 1.6 | −65.2 | Descent | Screening | Registry |
| 14. | Irving et al. (2008) | Northern England (UK) | 1985–2004 (20) | 11.6 | 12.1 | 4.3 | Unclear | - | Survey |
| 15. | McDermott et al. (2011) | Hawaii (USA) | 1997–2005 (9) | 9.0 | 7.9 | −12.2 | Descent | Unclear | Registry |
| 16. | Acikibas et al. (2012) | Denizli (Turkey) | 1996–2010 (15) | 9.1 | 9.9 | 9.2 | Ascent | Healthcare | Record/Survey |
| 17. | Mendez-R. et al. (2014) | Cuba | 2002–2012 (11) | 8.4 | 7.0 | −16.7 | Descent | Screening/Maternal Age | Record |
| 18. | Glivetic et al. (2015) | Croatia | 2009–2012 (4) | 7.4 | 10.1 | 36.3 | Ascent | Unclear | Registry |
| 19. | Huete-García (2016) | Spain | 1976–2010 (35) | 16.0 | 5.5 | −65.6 | Descent | Screening | Registry |
| 20. | Gorazd et al. (2017) | Slovenia | 1981–2012 (32) | 5.1 | 5.5 | 7.8 | Ascent | Unclear | Record |
| 21. | Jarurata-nasirikul (2017) | Southern Thailand | 2009–2013 (5) | 9.5 | 5.8 | −38.9 | Descent | Screening/Maternal age | Survey |
| 22. | Benavides (2019) | Costa Rica | 1996–2016 (21) | 9.1 | 11.6 | 27.5 | Ascent | Maternal age/Healthcare | Registry |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huete-García, A.; Otaola-Barranquero, M. Demographic Assessment of Down Syndrome: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 352. https://doi.org/10.3390/ijerph18010352
Huete-García A, Otaola-Barranquero M. Demographic Assessment of Down Syndrome: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(1):352. https://doi.org/10.3390/ijerph18010352
Chicago/Turabian StyleHuete-García, Agustín, and Mónica Otaola-Barranquero. 2021. "Demographic Assessment of Down Syndrome: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 1: 352. https://doi.org/10.3390/ijerph18010352
APA StyleHuete-García, A., & Otaola-Barranquero, M. (2021). Demographic Assessment of Down Syndrome: A Systematic Review. International Journal of Environmental Research and Public Health, 18(1), 352. https://doi.org/10.3390/ijerph18010352