Dietary Constituents: Relationship with Breast Cancer Prognostic (MCC-SPAIN Follow-Up)

 ,
,  , , , , ,
, , , , ,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
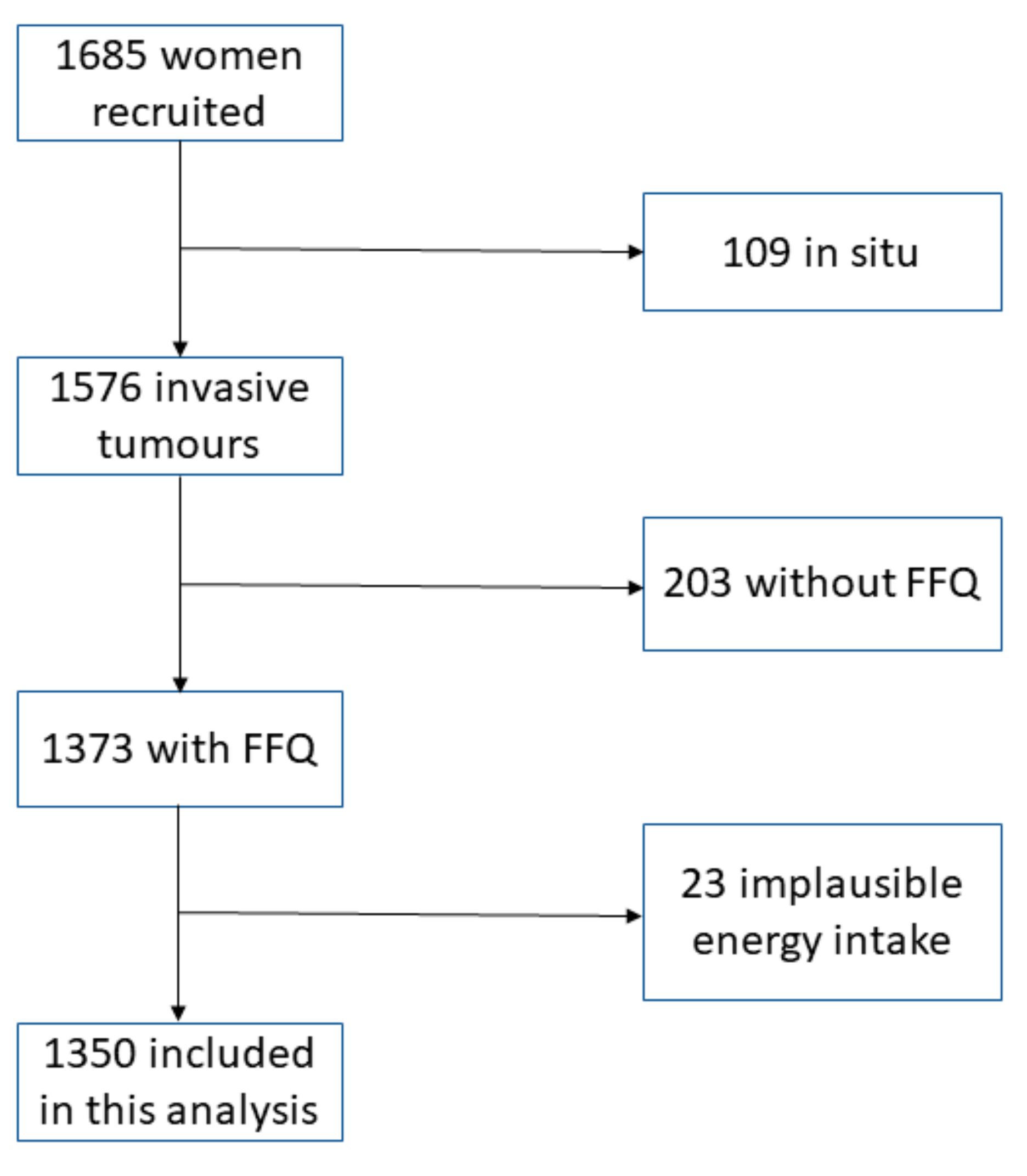
2.1. Study Population
2.2. Ethical Approval
2.3. Dietary and Prognosis Factors Assessment
2.4. Follow-Up and Ascertainment of Events
2.5. Statistical Analysis
3. Results
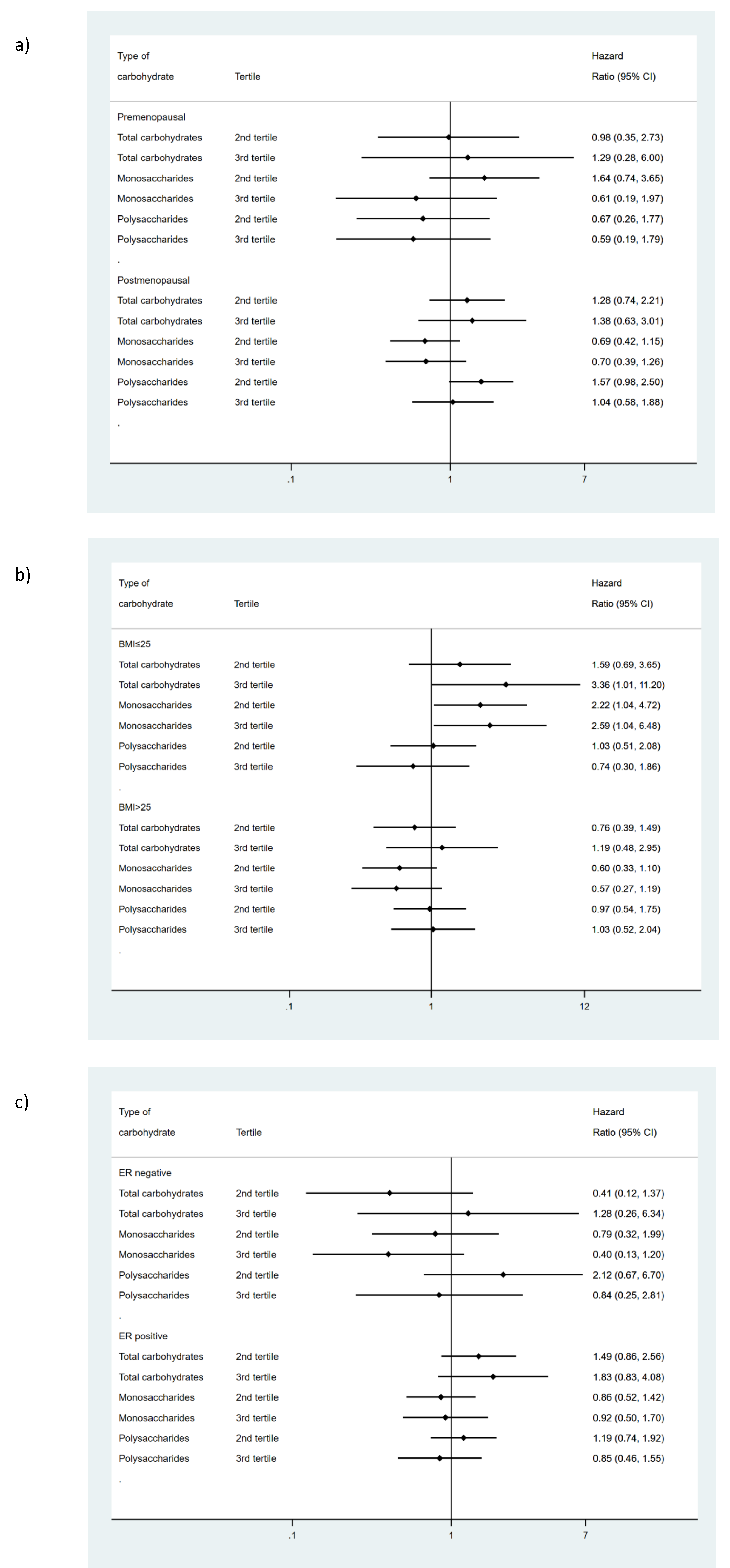
3.1. Relationship between Carbohydrate Intake and Overall Survival
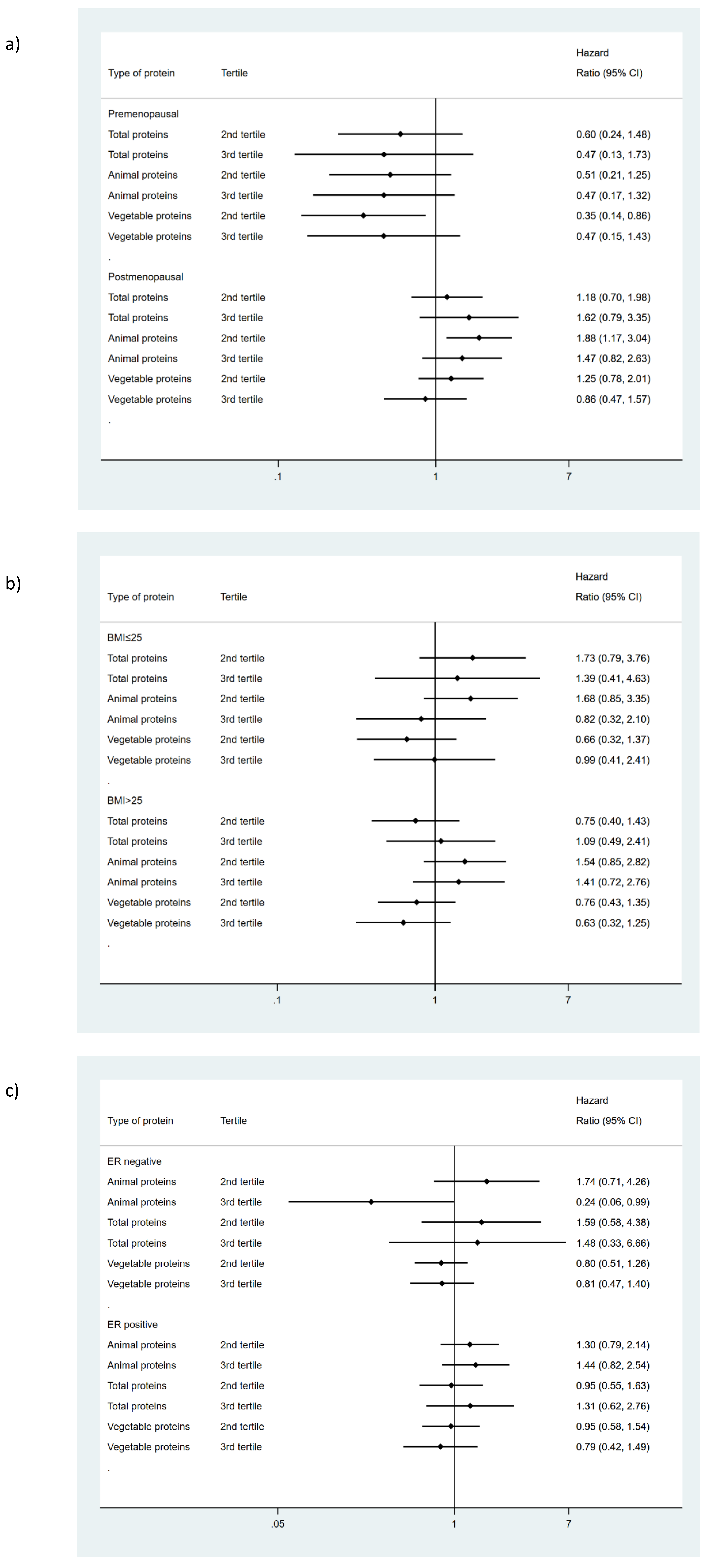
3.2. Relationship between Protein Intake and Overall Survival
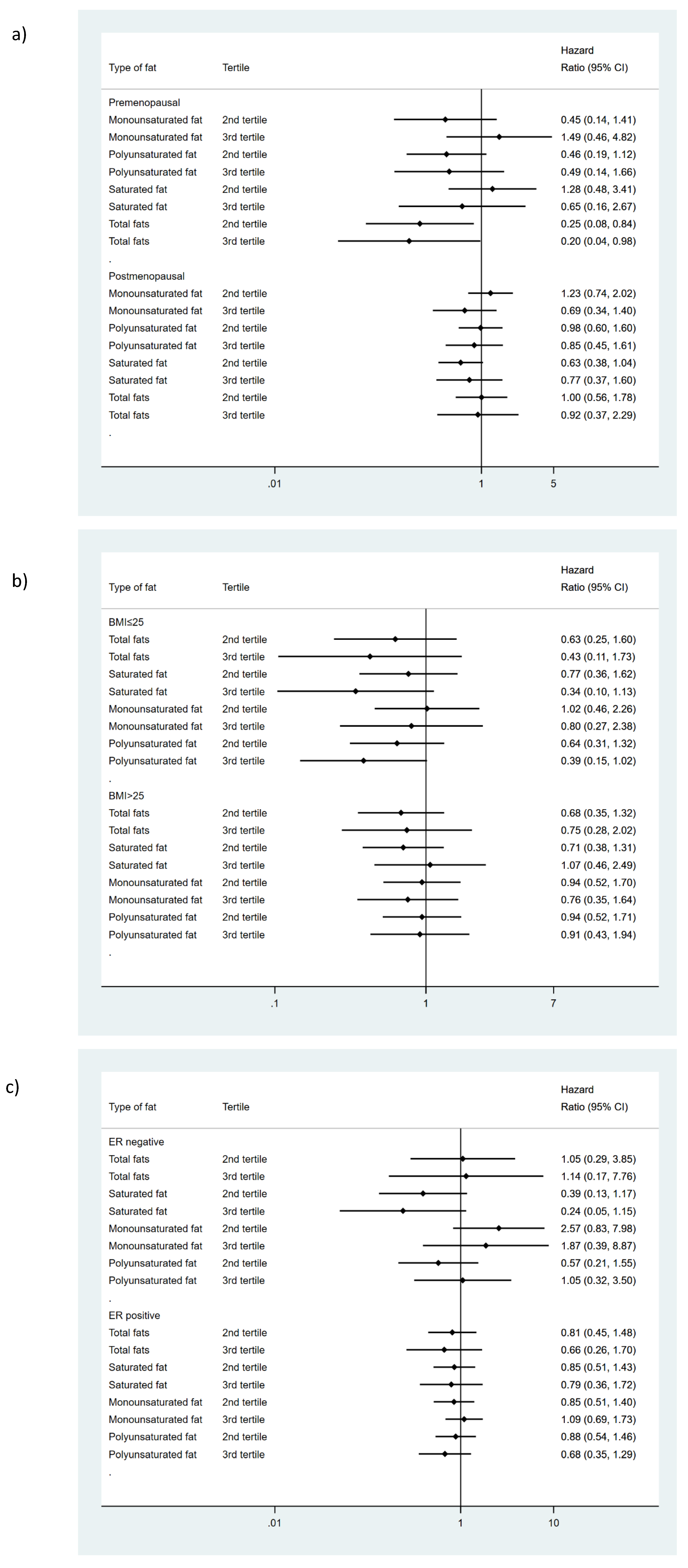
3.3. Relationship between Fat Intake and Overall Survival
3.4. Effect of Substituting a Nutrient for Another
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries and 25 major cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Siegel, R.L.; Lin, C.C.; Mariotto, A.B.; Kramer, J.L.; Rowland, J.H.; Stein, K.D.; Alteri, R.; Jemal, A. Cancer treatment and survivorship statistics, 2016. CA Cancer J. Clin. 2016, 66, 271–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saadatmand, S.; Bretveld, R.; Siesling, S.; Tilanus-Linthorst, M.M.A. Influence of tumour stage at breast cancer detection on survival in modern times: Population based study in 173 797 patients. BMJ 2015, 351. [Google Scholar] [CrossRef] [Green Version]
- Carioli, G.; Malvezzi, M.; Rodriguez, T.; Bertuccio, P.; Negri, E.; La Vecchia, C. Trends and predictions to 2020 in breast cancer mortality in Europe. Breast 2017, 36, 89–95. [Google Scholar] [CrossRef]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Alkandari, J.R.; Andersen, L.B.; Bauman, A.E.; Brownson, R.C.; et al. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Lumeng, C.N.; Bodzin, J.L.; Saltiel, A.R. Obesity induces a phenotypic switch in adipose tissue macrophage polarization. J. Clin. Investig. 2007, 117, 175–184. [Google Scholar] [CrossRef] [Green Version]
- Pierce, J.P.; Natarajan, L.; Caan, B.J.; Parker, B.A.; Greenberg, E.R.; Flatt, S.W.; Rock, C.L.; Kealey, S.; Al-Delaimy, W.K.; Bardwell, W.A.; et al. Influence of a Diet Very High in Vegetables, Fruit, and Fiber and Low in Fat on Prognosis Following Treatment for Breast Cancer. JAMA 2007, 298, 289. [Google Scholar] [CrossRef]
- Chlebowski, R.T.; Aragaki, A.K.; Anderson, G.L.; Thomson, C.A.; Manson, J.E.; Simon, M.S.; Howard, B.V.; Rohan, T.E.; Snetselar, L.; Lane, D.; et al. Low-Fat Dietary Pattern and Breast Cancer Mortality in the Women’s Health Initiative Randomized Controlled Trial. J. Clin. Oncol. 2017, 35, 2919–2926. [Google Scholar] [CrossRef] [Green Version]
- De Cicco, P.; Catani, M.V.; Gasperi, V.; Sibilano, M.; Quaglietta, M.; Savini, I. Nutrition and breast cancer: A literature review on prevention, treatment and recurrence. Nutrients 2019, 11, 1514. [Google Scholar] [CrossRef] [Green Version]
- Levine, M.E.; Suarez, J.A.; Brandhorst, S.; Balasubramanian, P.; Cheng, C.W.; Madia, F.; Fontana, L.; Mirisola, M.G.; Guevara-Aguirre, J.; Wan, J.; et al. Low protein intake is associated with a major reduction in IGF-1, cancer, and overall mortality in the 65 and younger but not older population. Cell Metab. 2014, 19, 407–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maino Vieytes, C.A.; Taha, H.M.; Burton-Obanla, A.A.; Douglas, K.G.; Arthur, A.E. Carbohydrate Nutrition and the Risk of Cancer. Curr. Nutr. Rep. 2019, 230–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Cancer Research Fund; American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Breast Cancer. Available online: https://www.wcrf.org/sites/default/files/Breast-Cancer-2017-Report.pdf (accessed on 27 February 2020).
- Lajous, M.; Boutron-Ruault, M.C.; Fabre, A.; Clavel-Chapelon, F.; Romieu, I. Carbohydrate intake, glycemic index, glycemic load, and risk of postmenopausal breast cancer in a prospective study of French women. Am. J. Clin. Nutr. 2008, 87, 1384–1391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, M.; Liu, S.H.; Mitchell, C.; Fung, T.T. Associations between diet quality scores and risk of postmenopausal estrogen receptor-negative breast cancer: A systematic review. J. Nutr. 2018, 148, 100–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chlebowski, R.T.; Blackburn, G.L.; Thomson, C.A.; Nixon, D.W.; Shapiro, A.; Hoy, M.K.; Goodman, M.T.; Giuliano, A.E.; Karanja, N.; McAndrew, P.; et al. Dietary fat reduction and breast cancer outcome: Interim efficacy results from the women’s intervention nutrition study. J. Natl. Cancer Inst. 2006, 98, 1767–1776. [Google Scholar] [CrossRef] [Green Version]
- Chlebowski, R.T.; Aragaki, A.K.; Anderson, G.L.; Simon, M.S.; Manson, J.E.; Neuhouser, M.L.; Pan, K.; Stefanic, M.L.; Rohan, T.E.; Lane, D.; et al. Association of Low-Fat Dietary Pattern With Breast Cancer Overall Survival: A Secondary Analysis of the Women’s Health Initiative Randomized Clinical Trial. JAMA Oncol. 2018, 4, e181212. [Google Scholar] [CrossRef]
- Castaño-Vinyals, G.; Aragonés, N.; Pérez-Gómez, B.; Martín, V.; Llorca, J.; Moreno, V.; Altzibar, J.M.; Ardanaz, E.; de Sanjosé, S.; Jiménez-Moleón, J.J.; et al. Population-based multicase-control study in common tumors in Spain (MCC-Spain): Rationale and study design. Gac. Sanit. 2015, 29, 308–315. [Google Scholar] [CrossRef] [Green Version]
- Alonso-Molero, J.; Molina, A.; Jiménez-Moleón, J.; Pérez-Gómez, B.; Martin, V.; Moreno, V.; Amiano, P.; Ardanaz, E.; de Sanjose, S.; Salcedo, I.; et al. Cohort profile: The MCC-Spain follow-up on colorectal, breast and prostate cancers: Study design and initial results. BMJ Open 2019, 9, e031904. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Acebo, I.; Dierssen-Sotos, T.; Palazuelos-Calderón, C.; Pérez-Gómez, B.; Amiano, P.; Guevara, M.; Molina, A.J.; Domingo, L.; Fernández-Ortiz, M.; Moreno, V.; et al. Tumour characteristics and survivorship in a cohort of breast cancer: The MCC-Spain study. Breast Cancer Res. Treat. 2020, 181, 667–678. [Google Scholar] [CrossRef]
- García-Closas, R.; García-Closas, M.; Kogevinas, M.; Malats, N.; Silverman, D.; Serra, C.; Tardón, A.; Carrato, A.; Castaño-Vinyals, G.; Dosemeci, M.; et al. Food, nutrient and heterocyclic amine intake and the risk of bladder cancer. Eur. J. Cancer 2007, 43, 1731–1740. [Google Scholar] [CrossRef]
- CESNID. Tablas de Composición de Alimentos; Ediciones de la Universitat de Barcelona, Ed.; McGraw Hill-Interamericana de España S.A.: Barcelona, Spain, 2008. [Google Scholar]
- Calvert, C.; Cade, J.; Barrett, J.H.; Woodhouse, A. Using cross-check questions to address the problem of mis-reporting of specific food groups on Food Frequency Questionnaires. UKWCS Steering Group. United Kingdom Women’s Cohort Study Steering Group. Eur. J. Clin. Nutr. 1997, 51, 708–712. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.E.; Edge, S.B.; Hortobagyi, G.N. Eighth Edition of the AJCC Cancer Staging Manual: Breast Cancer. Ann Surg Oncol. 2018, 25, 1783–1785. [Google Scholar] [CrossRef]
- Navarro, C. El Índice Nacional de Defunciones: Un avance en la accesibilidad de los datos de mortalidad largamente esperado. Gac. Sanit. 2006, 20, 421–423. [Google Scholar] [CrossRef] [Green Version]
- Willett, W.C.; Howe, R. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S. [Google Scholar] [CrossRef] [PubMed]
- Mekary, R.A.; Willett, W.C.; Hu, F.B.; Ding, E.L. Isotemporal substitution paradigm for physical activity epidemiology and weight change. Am. J. Epidemiol. 2009, 170, 519–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dam, R.M.; Li, T.; Spiegelman, D.; Franco, O.H.; Hu, F.B. Combined impact of lifestyle factors on mortality: Prospective cohort study in US women. BMJ 2008, 337, 742–745. [Google Scholar] [CrossRef] [Green Version]
- MacMahon, S.; Baigent, C.; Duffy, S.; Rodgers, A.; Tominaga, S.; Chambless, L.; De Backer, G.; De Bacquer, D.; Kornitzer, M.; Whincup, P.; et al. Body-mass index and cause-specific mortality in 900 000 adults: Collaborative analyses of 57 prospective studies. Lancet 2009, 373, 1083–1096. [Google Scholar] [CrossRef] [Green Version]
- Leturque, A.; Brot-Laroche, E.; Le Gall, M. Carbohydrate intake. In Progress in Molecular Biology and Translational Science; Elsevier: Amsterdam, The Netherlands, 2012; Volume 108, pp. 113–127. [Google Scholar]
- Saxe, G.A.; Rock, C.L.; Wicha, M.S.; Schottenfeld, D. Diet and risk for breast cancer recurrence and survival. Breast Cancer Res. Treat. 1999, 53, 241–253. [Google Scholar] [CrossRef] [Green Version]
- Goodwin, P.J.; Ennis, M.; Pritchard, K.I.; Koo, J.; Trudeau, M.E.; Hood, N. Diet and breast cancer: Evidence that extremes in diet are associated with poor survival. J. Clin. Oncol. 2003, 21, 2500–2507. [Google Scholar] [CrossRef]
- Jaiswal McEligot, A.; Largent, J.; Ziogas, A.; Peel, D.; Anton-Culver, H. Dietary Fat, Fiber, Vegetable, and Micronutrients Are Associated with Overall Survival in Postmenopausal Women Diagnosed with Breast Cancer. Nutr. Cancer 2006, 55, 132–140. [Google Scholar] [CrossRef] [Green Version]
- Norat, T.; Chan, D.; Vieira, A.R.; Aune, D.; Navarro Rosenblatt, D.; Vingeliene, S.; Abar, L.; Vieira, R.; Thompson, R.; Greenwood, D.C. Systematic Review on Diet, Nutrition, Physical Activity and Survival and Second Cancers in Breast Cancer Survivors; Imperial College London: London, UK, 2014; p. 459. [Google Scholar]
- Wang, J.; Luo, X.-X.; Tang, Y.-L.; Xu, J.-X.; Zeng, Z.-G. The prognostic values of insulin-like growth factor binding protein in breast cancer. Medicine 2019, 98, e15561. [Google Scholar] [CrossRef] [PubMed]
- Krone, C.A.; Ely, J.T.A. Controlling hyperglycemia as an adjunct to cancer therapy. Integr. Cancer Ther. 2005, 4, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Endogenous Hormones and Breast Cancer Collaborative Group; Key, T.J.; Appleby, P.N.; Reeves, G.K.; Roddam, A.W. Insulin-like growth factor 1 (IGF1), IGF binding protein 3 (IGFBP3), and breast cancer risk: Pooled individual data analysis of 17 prospective studies. Lancet Oncol. 2010, 11, 530–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dal Maso, L.; Zucchetto, A.; Talamini, R.; Serraino, D.; Stocco, C.F.; Vercelli, M.; Falcini, F.; Franceschi, S. Prospective Analysis of Case-control studies on Environmental factors and health (PACE) study group Effect of obesity and other lifestyle factors on mortality in women with breast cancer. Int. J. Cancer 2008, 123, 2188–2194. [Google Scholar] [CrossRef] [PubMed]
- Jain, M.; Miller, A.B.; To, T. Premorbid Diet and the Prognosis of Women with Breast Cancer. JNCI J. Natl. Cancer Inst. 1994, 86, 1390–1397. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Zeng, R.; Huang, J.; Li, X.; Zhang, J.; Ho, J.; Zheng, Y. Dietary Protein Sources and Incidence of Breast Cancer: A Dose-Response Meta-Analysis of Prospective Studies. Nutrients 2016, 8, 730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, S.; Folsom, A.R.; Sellers, T.A.; Kushi, L.H.; Potter, J.D. Better breast cancer survival for postmenopausal women who are less overweight and eat less fat. The Iowa women’s health study. Cancer 1995, 76, 275–283. [Google Scholar] [CrossRef]
- Holmes, M.D.; Wang, J.; Hankinson, S.E.; Tamimi, R.M.; Chen, W.E. Protein intake and breast cancer survival in the Nurses’ Health Study. J. Clin. Oncol. 2017, 35, 325–333. [Google Scholar] [CrossRef] [Green Version]
- Borugian, M.J.; Dunn, B.; Gallagher, R.P.; Hislop, T.G.; Kim-Sing, C.; Van Patten, C.; Potter, J.D.; Sheps, S.B. Insulin, macronutrient intake, and physical activity: Are potential indicators of insulin resistance associated with mortality from breast cancer? Cancer Epidemiol. Biomarkers Prev. 2004, 13, 1163–1172. [Google Scholar]
- Holmes, M.D.; Stampfer, M.J.; Colditz, G.A.; Rosner, B.; Hunter, D.J.; Willett, W.C. Dietary factors and the survival of women with breast carcinoma. Cancer 1999, 86, 826–835. [Google Scholar] [CrossRef]
- Rohan, T.E.; Hiller, J.E.; McMichael, A.J. Dietary factors and survival from breast cancer. Nutr. Cancer 1993, 20, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, H.E.K.; Voutilainen, S.; Koskinen, T.T.; Mursu, J.; Kokko, P.; Ylilauri, M.P.T.; Tuomainen, T.P.; Salonen, J.T.; Virtanen, J.K. Dietary proteins and protein sources and risk of death: The Kuopio ischaemic heart disease risk factor study. Am. J. Clin. Nutr. 2019, 109, 1462–1471. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Fung, T.T.; Hu, F.B.; Willett, W.C.; Longo, V.D.; Chan, A.T.; Giovannucci, E.L. Association of animal and plant protein intake with all-cause and cause-specific mortality. JAMA Intern. Med. 2016, 176, 1453–1463. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Alonso, P.; Salas-Salvadó, J.; Ruiz-Canela, M.; Corella, D.; Estruch, R.; Fitó, M.; Arós, F.; Gómez-Gracia, E.; Fiol, M.; Lapetra, J.; et al. High dietary protein intake is associated with an increased body weight and total death risk. Clin. Nutr. 2016, 35, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, F.; Lavigne, C.; Jacques, H.; Marette, A. Role of Dietary Proteins and Amino Acids in the Pathogenesis of Insulin Resistance. Annu. Rev. Nutr. 2007, 27, 293–310. [Google Scholar] [CrossRef]
- Gregorio, D.I.; Emrich, L.J.; Graham, S.; Marshall, J.R.; Nemoto, T. Dietary fat consumption and survival among women with breast cancer. J. Natl. Cancer Inst. 1985, 75, 37–41. [Google Scholar]
- Boeke, C.E.; Eliassen, A.H.; Chen, W.Y.; Cho, E.; Holmes, M.D.; Rosner, B.; Willett, W.C.; Tamimi, R.M. Dietary fat intake in relation to lethal breast cancer in two large prospective cohort studies. Breast Cancer Res. Treat. 2014, 146, 383–392. [Google Scholar] [CrossRef] [Green Version]
- Beasley, J.M.; Newcomb, P.A.; Trentham-Dietz, A.; Hampton, J.M.; Bersch, A.J.; Passarelli, M.N.; Holick, C.N.; Titus-Ernstoff, L.; Egan, K.M.; Holmes, M.D.; et al. Post-diagnosis dietary factors and survival after invasive breast cancer. Breast Cancer Res. Treat. 2011, 128, 229–236. [Google Scholar] [CrossRef] [Green Version]
- Sieri, S.; Krogh, V.; Ferrari, P.; Berrino, F.; Pala, V.; Thiébaut, A.C.M.; Tjønneland, A.; Olsen, A.; Overvad, K.; Jakobsen, M.U.; et al. Dietary fat and breast cancer risk in the European Prospective Investigation into Cancer and Nutrition 1–3. Am. J. Clin. Nutr. 2008, 88, 1304–1312. [Google Scholar] [CrossRef]
- Kroenke, C.H.; Kwan, M.L.; Sweeney, C.; Castillo, A.; Caan, B.J. High-and low-fat dairy intake, recurrence, and mortality after breast cancer diagnosis. J. Natl. Cancer Inst. 2013, 105, 616–623. [Google Scholar] [CrossRef] [Green Version]
- Rose, D.P.; Connolly, J.M. Regulation of Tumor Angiogenesis by Dietary Fatty Acids and Eicosanoids. Nutr. Cancer 2000, 37, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Engeset, D.; Alsaker, E.; Lund, E.; Welch, A.; Khaw, K.T.; Clavel-Chapelon, F.; Thiébaut, A.; Chajès, V.; Key, T.J.; Allen, N.E.; et al. Fish consumption and breast cancer risk. The European Prospective Investigation into Cancer and Nutrition (EPIC). Int. J. Cancer 2006, 119, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Welch, A.; Lund, E.; Amiano, P.; Dorronsoro, M.; Brustad, M.; Kumle, M.; Rodriguez, M.; Lasheras, C.; Janzon, L.; Jansson, J.; et al. Variability of fish consumption within the 10 European countries participating in the European Investigation into Cancer and Nutrition (EPIC) study. Public Health Nutr. 2002, 5, 1273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eilander, A.; Harika, R.K.; Zock, P.L. Intake and sources of dietary fatty acids in Europe: Are current population intakes of fats aligned with dietary recommendations? Eur. J. Lipid Sci. Technol. 2015, 117, 1370–1377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, A.G.; Ford, N.A.; Hu, F.B.; Zelman, K.M.; Mozaffarian, D.; Kris-Etherton, P.M. A healthy approach to dietary fats: Understanding the science and taking action to reduce consumer confusion. Nutr. J. 2017, 16, 53. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.-S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef] [PubMed]
- Custódio, I.D.D.; Marinho, E.d.C.; Gontijo, C.A.; Pereira, T.S.S.; Paiva, C.E.; Maia, Y.C.d.P. Impact of Chemotherapy on Diet and Nutritional Status of Women with Breast Cancer: A Prospective Study. PLoS ONE 2016, 11, e0157113. [Google Scholar] [CrossRef]
- Velentzis, L.S.; Keshtgar, M.R.; Woodside, J.V.; Leathem, A.J.; Titcomb, A.; Perkins, K.A.; Mazurowska, M.; Anderson, V.; Wardell, K.; Cantwell, M.M. Significant changes in dietary intake and supplement use after breast cancer diagnosis in a UK multicentre study. Breast Cancer Res. Treat. 2011, 128, 473–482. [Google Scholar] [CrossRef] [Green Version]
- Salminen, E.; Bishop, M.; Poussa, T.; Drummond, R.; Salminen, S. Dietary attitudes and changes as well as use of supplements and complementary therapies by Australian and Finnish women following the diagnosis of breast cancer. Eur. J. Clin. Nutr. 2004, 58, 137–144. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Nutrient | 1st Tertile | HR (95% CI) 2nd Tertile | HR (95% CI) 3rd Tertile | p Trend | |
|---|---|---|---|---|---|
| Total carbohydrates | Deaths/woman-years | 52/2933 | 53/2946 | 66/2913 | |
| Model 1 | 1(ref.) | 1.10 (0.72 to 1.68) | 1.36 (0.80 to 2.33) | 0.27 | |
| Model 2 | 1(ref.) | 1.09 (0.71 to 1.67) | 1.31 (0.76 to 2.26) | 0.34 | |
| Model 3 * | 1(ref.) | 1.12 (0.71 to 1.75) | 1.42 (0.75 to 2.69) | 0.30 | |
| Monosaccharides | Deaths/woman-years | 56/2910 | 55/2943 | 60/2939 | |
| Model 1 | 1(ref.) | 0.86 (0.58 to 1.29) | 0.76 (0.47 to 1.24) | 0.28 | |
| Model 2 | 1(ref.) | 0.86 (0.58 to 1.30) | 0.75 (0.45 to 1.22) | 0.24 | |
| Model 3 # | 1(ref.) | 0.89 (0.59 to 1.35) | 0.74 (0.45 to 1.23) | 0.25 | |
| Polysaccharides | Deaths/woman-years | 54/2984 | 65/2870 | 52/2937 | |
| Model 1 | 1(ref.) | 1.25 (0.85 to 1.85) | 0.94 (0.58 to 1.52) | 0.84 | |
| Model 2 | 1(ref.) | 1.23 (0.83 to 1.83) | 0.96 (0.59 to 1.55) | 0.91 | |
| Model 3 $ | 1(ref.) | 1.24 (0.83 to 1.84) | 0.92 (0.56 to 1.50) | 0.77 | |
| Total proteins | Deaths/woman-years | 60/2888 | 52/2956 | 59/2948 | |
| Model 1 ** | 1(ref.) | 0.89 (0.59 to 1.34) | 0.96 (0.56 to 1.62) | 0.84 | |
| Model 2 | 1(ref.) | 0.88 (0.58 to 1.33) | 0.96 (0.56 to 1.64) | 0.84 | |
| Model 3 | 1(ref.) | 0.94 (0.61 to 1.45) | 1.12 (0.61 to 2.06) | 0.77 | |
| Animal proteins | Deaths/woman-years | 52/2928 | 64/2902 | 55/2962 | |
| Model 1 | 1(ref.) | 1.37 (0.92 to 2.04) | 1.13 (0.70 to 1.82) | 0.60 | |
| Model 2 | 1(ref.) | 1.37 (0.91 to 2.06) | 1.09 (0.68 to 1.76) | 0.72 | |
| Model 3 ¥ | 1(ref.) | 1.35 (0.89 to 2.03) | 1.05 (0.64 to 1.71) | 0.84 | |
| Vegetable proteins | Deaths/woman-years | 62/2894 | 52/2965 | 57/2932 | |
| Model 1 | 1(ref.) | 0.88 (0.59 to 1.32) | 0.75 (0.46 to 1.23) | 0.26 | |
| Model 2 | 1(ref.) | 0.91 (0.61 to 1.37) | 0.79 (0.48 to 1.30) | 0.35 | |
| Model 3 £ | 1(ref.) | 0.90 (0.60 to 1.35) | 0.77 (0.46 to 1.28) | 0.32 | |
| Total fats | Deaths/woman-years | 59/2902 | 59/2913 | 53/2976 | |
| Model 1 | 1(ref.) | 0.77 (0.51 to 1.17) | 0.70 (0.37 to 1.30) | 0.22 | |
| Model 2 | 1(ref.) | 0.80 (0.52 to 1.22) | 0.73 (0.39 to 1.37) | 0.30 | |
| Model 3 ** | 1(ref.) | 0.73 (0.45 to 1.19) | 0.63 (0.30 to 1.34) | 0.22 | |
| Saturated fats | Deaths/woman-years | 63/2909 | 56/2909 | 52/2974 | |
| Model 1 | 1(ref.) | 0.79 (0.52 to 1.20) | 0.76 (0.41 to 1.40) | 0.33 | |
| Model 2 | 1(ref.) | 0.78 (0.51 to 1.18) | 0.73 (0.39 to 1.36) | 0.27 | |
| Model 3 § | 1(ref.) | 0.74 (0.48 to 1.14) | 0.70 (0.37 to 1.31) | 0.22 | |
| Monounsaturated fats | Deaths/woman-years | 56/2901 | 64/2926 | 51/2965 | |
| Model 1 | 1(ref.) | 0.95 (0.63 to 1.43) | 0.74 (0.43 to 1.28) | 0.29 | |
| Model 2 | 1(ref.) | 0.99 (0.65 to 1.49) | 0.77 (0.44 to 1.33) | 0.36 | |
| Model 3 ¶ | 1(ref.) | 1.00 (0.66 to 1.53) | 0.78 (0.44 to 1.38) | 0.41 | |
| Polyunsaturated fats | Deaths/woman-years | 60/2855 | 61/2984 | 50/2952 | |
| Model 1 | 1(ref.) | 0.87 (0.58 to 1.30) | 0.76 (0.45 to 1.28) | 0.3 | |
| Model 2 | 1(ref.) | 0.90 (0.59 to 1.35) | 0.81 (0.48 to 1.37) | 0.44 | |
| Model 3 ß | 1(ref.) | 0.86 (0.56 to 1.31) | 0.77 (0.45 to 1.32) | 0.34 |
| Substituted Nutrient | |||
|---|---|---|---|
| Carbohydrates | Proteins | Fats | |
| HR 95% CI | HR 95% CI | HR 95% CI | |
| Carbohydrates | 1.09 (0.78 to 1.52) | 1.02 (0.90 to 1.16) | |
| Proteins | 0.94 (0.67 to 1.33) | 0.96 (0.68 to 1.35) | |
| Fats | 0.99 (0.87 to 1.12) | 1.07 (0.77 to 1.49) | |
| Substituted Nutrient | ||||||
|---|---|---|---|---|---|---|
| Premenopausal Women | Menopausal Women | |||||
| Carbohydrates | Proteins | Fats | Carbohydrates | Proteins | Fats | |
| HR 95% CI | HR 95% CI | HR 95% CI | HR 95% CI | HR 95% CI | HR 95% CI | |
| Carbohydrates | 1.34 (0.68 to 2.71) | 0.83 (0.63 to 1.10) | 0.84 (0.56 to 1.27) | 1.03 (0.89 to 1.19) | ||
| Proteins | 0.63 (0.30 to 1.32) | 0.58 (0.27 to 1.24) | 1.16 (0.77 to 1.73) | 1.19 (0.80 to 1.76) | ||
| Fats | 1.21 (0.90 to 1.63) | 1.61 (0.77 to 3.37) | 0.97 (0.84 to 1.13) | 0.83 (0.56 to 1.25) | ||
| BMI ≤ 25 | BMI > 25 | |||||
| Carbohydrates | 1.11 (0.60 to 2.08) | 1.30 (1.01 to 1.68) | 0.94 (0.60 to 1.49) | 0.94 (0.80 to 1.10) | ||
| Proteins | 0.85 (0.45 to 1.63) | 1.12 (0.59 to 2.16) | 1.11 (0.70 to 1.76) | 1.04 (0.66 to 1.63) | ||
| Fats | 0.76 (0.59 to 0.98) | 0.85 (0.45 to 1.60) | 1.07 (0.91 to 1.25) | 1.00 (0.65 to 1.56) | ||
| ER negative | ER positive | |||||
| Carbohydrates | 1.87 (0.80 to 4.38) | 0.96 (0.76 to 1.22) | 0.92 (0.63 to 1.36) | 0.97 (0.83 to 1.30) | ||
| Proteins | 0.56 (0.24 to 1.34) | 0.54 (0.23 to 1.24) | 1.12(0.75 to 1.66) | 1.08 (0.72 to 1.61) | ||
| Fats | 1.04 (0.83 to 1.31) | 1.92 (0.86 to 4.30) | 1.04 (0.88 to 1.21) | 0.96 (0.65 to 1.42) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dierssen-Sotos, T.; Gómez-Acebo, I.; Gutiérrez-Ruiz, N.; Aragonés, N.; Amiano, P.; Molina de la Torre, A.J.; Guevara, M.; Alonso-Molero, J.; Obon-Santacana, M.; Fernández-Tardón, G.; et al. Dietary Constituents: Relationship with Breast Cancer Prognostic (MCC-SPAIN Follow-Up). Int. J. Environ. Res. Public Health 2021, 18, 84. https://doi.org/10.3390/ijerph18010084
Dierssen-Sotos T, Gómez-Acebo I, Gutiérrez-Ruiz N, Aragonés N, Amiano P, Molina de la Torre AJ, Guevara M, Alonso-Molero J, Obon-Santacana M, Fernández-Tardón G, et al. Dietary Constituents: Relationship with Breast Cancer Prognostic (MCC-SPAIN Follow-Up). International Journal of Environmental Research and Public Health. 2021; 18(1):84. https://doi.org/10.3390/ijerph18010084
Chicago/Turabian StyleDierssen-Sotos, Trinidad, Inés Gómez-Acebo, Nuria Gutiérrez-Ruiz, Nuria Aragonés, Pilar Amiano, Antonio José Molina de la Torre, Marcela Guevara, Jessica Alonso-Molero, Mireia Obon-Santacana, Guillermo Fernández-Tardón, and et al. 2021. "Dietary Constituents: Relationship with Breast Cancer Prognostic (MCC-SPAIN Follow-Up)" International Journal of Environmental Research and Public Health 18, no. 1: 84. https://doi.org/10.3390/ijerph18010084
APA StyleDierssen-Sotos, T., Gómez-Acebo, I., Gutiérrez-Ruiz, N., Aragonés, N., Amiano, P., Molina de la Torre, A. J., Guevara, M., Alonso-Molero, J., Obon-Santacana, M., Fernández-Tardón, G., Molina-Barceló, A., Alguacil, J., Marcos-Gragera, R., Rodríguez-Cundín, P., Castaño-Vinyals, G., Canseco Fernandez, R., Castilla, J., Molinuevo, A., Pérez-Gómez, B., ... Llorca, J. (2021). Dietary Constituents: Relationship with Breast Cancer Prognostic (MCC-SPAIN Follow-Up). International Journal of Environmental Research and Public Health, 18(1), 84. https://doi.org/10.3390/ijerph18010084