Elaboration and Validation of Two Predictive Models of Postpartum Traumatic Stress Disorder Risk Formed by Variables Related to the Birth Process: A Retrospective Cohort Study

 , , ,
, , , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Data Collection and Information Sources
- Maternal: maternal age, education level, nationality, attendance at maternal education classes, and the use of a birth plan.
- Obstetric: previous cesarean section (CS), number of deliveries, induction of labor, type of labor, use of regional analgesia, use of general anesthesia, use of natural analgesic methods, episiotomy, and perineal tear.
- Fetal: prematurity, twin pregnancy, breastfeeding in the first hour, skin-to-skin contact, admission of the newborn to care unit, type of feeding at hospital discharge.
- Subjective variables evaluated with a Likert-type scale (scores 1–5): degree of support from the partner during pregnancy, delivery, and postpartum; respectful treatment by professionals during pregnancy, delivery, and postpartum. The different categories used for each variable are detailed in Table 1.
2.3. Statistical Analysis
3. Results
Characteristics of Participants
4. Discussion
Strengths and Limits
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
|
References
- Van der Kolk, B.A.; Pelcovitz, D.; Roth, S.; Mandel, F.S.; McFarlane, A.; Herman, J.L. Dissociation, somatization, and affect dysregulation: The complexity of adaptation of trauma. Am. J. Psychiatry 1996, 153, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Martinez, A.; Rodriguez-Almagro, J.; Molina-Alarcon, M.; Infante-Torres, N.; Donate Manzanares, M.; Martinez-Galiano, J.M. Postpartum post-traumatic stress disorder: Associated perinatal factors and quality of life. J. Affect. Disord. 2019, 249, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.; Ayers, S.; Horsch, A. Maternal posttraumatic stress disorder during the perinatal period and child outcomes: A systematic review. J. Affect. Disord. 2018, 225, 18–31. [Google Scholar] [CrossRef]
- Dikmen-Yildiz, P.; Ayers, S.; Phillips, L. Factors associated with post-traumatic stress symptoms (PTSS) 4-6 weeks and 6 months after birth: A longitudinal population-based study. J. Affect. Disord. 2017, 221, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, P.D.; Ayers, S.; Phillips, L. The prevalence of posttraumatic stress disorder in pregnancy and after birth: A systematic review and meta-analysis. J. Affect. Disord. 2017, 208, 634–645. [Google Scholar] [CrossRef]
- Geller, P.A.; Stasko, E.C. Effect of Previous Posttraumatic Stress in the Perinatal Period. J. Obstet. Gynecol. Neonatal. Nurs. 2017, 46, 912–922. [Google Scholar] [CrossRef] [Green Version]
- Halperin, O.; Sarid, O.; Cwikel, J. The influence of childbirth experiences on women’s postpartum traumatic stress symptoms: A comparison between Israeli Jewish and Arab women. Midwifery 2015, 6, 625–632. [Google Scholar] [CrossRef]
- Söderquist, J.; Wijma, K.; Wijma, B. Traumatic stress after childbirth: The role of obstetric variables. J. Psychosom. Obstet. Gynecol. 2002, 23, 1. [Google Scholar] [CrossRef]
- Adewuya, A.O.; Ologun, Y.A.; Ibigbami, O.S. Post-traumatic stress disorder after childbirth in Nigerian women: Prevalence and risk factors. BJOG 2006, 113, 284–288. [Google Scholar] [CrossRef]
- Susan, A.; Harris, R.; Sawyer, A.; Parfitt, Y.; Ford, E. Posttraumatic stress disorder after childbirth: Analysis of symptom presentation and sampling. J. Affect. Disord. 2009, 119, 200–204. [Google Scholar] [CrossRef] [Green Version]
- Andersen, L.B.; Melvaer, L.B.; Videbech, P.; Lamont, R.F.; Joergensen, J.S. Risk factors for developing post-traumatic stress disorder following childbirth: A systematic review. Acta Obstet. Gynecol. Scand. 2012, 91, 1261–1272. [Google Scholar] [CrossRef] [PubMed]
- Ayers, S.; Bond, R.; Bertullies, S.; Wijma, K. The aetiology of post-traumatic stress following childbirth: A meta-analysis and theoretical framework. Psychol. Med. 2016, 46, 1121–1134. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.M.; Ansara, D.; Schei, B.; Stuckless, N.; Stewart, D.E. Posttraumatic stress disorder after pregnancy, labor, and delivery. J. Womens. Health 2004, 13, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Srkalović Imširagić, A.; Begić, D.; Šimičević, L.; Bajić, Ž. Prediction of posttraumatic stress disorder symptomatology after childbirth—A Croatian longitudinal study. Women Birth. 2017, 30, e17–e23. [Google Scholar] [CrossRef]
- Hernández-Martínez, A.; Rodríguez-Almagro, J.; Molina-Alarcón, M.; Infante-Torres, N.; Rubio-Álvarez, A.; Martínez-Galiano, J.M. Perinatal factors related to post-traumatic stress disorder symptoms 1–5 years following birth. Women Birth. 2020, 33, e129–e135. [Google Scholar] [CrossRef]
- DeMier, R.L.; Hynan, M.T.; Harris, H.B.; Manniello, R.L. Perinatal stressors as predictors of symptoms of posttraumatic stress in mothers of infants at high risk. J. Perinatol. 1996, 16, 276–280. [Google Scholar] [PubMed]
- Elklit, A.; Hartvig, T.; Christiansen, M. Stress disorder in parents of premature neonates—Secondary publication. Ugeskr. Laeger. 2008, 170, 3643–3645. [Google Scholar] [PubMed]
- Fairbrother, N.; Woody, S.R. Fear of childbirth and obstetrical events as predictors of postnatal symptoms of depression and post-traumatic stress disorder. J. Psychosom. Obstet. Gynecol. 2007, 28, 239–242. [Google Scholar] [CrossRef]
- Van Heumen, M.A.; Hollander, M.H.; van Pampus, M.G.; van Dillen, J.; Stramrood, C.A.I. Psychosocial Predictors of Postpartum Posttraumatic Stress Disorder in Women with a Traumatic Childbirth Experience. Front. Psychiatry 2018, 9, 348. [Google Scholar] [CrossRef] [Green Version]
- O’Donovan, A.; Alcorn, K.L.; Patrick, J.C.; Creedy, D.K.; Dawe, S.; Devilly, G.J. Predicting posttraumatic stress disorder after childbirth. Midwifery 2014, 30, 935–941. [Google Scholar] [CrossRef] [Green Version]
- Lopez, U.; Meyer, M.; Loures, V.; Iselin-Chaves, I.; Epiney, M.; Kern, C. Post-traumatic stress disorder in parturients delivering by caesarean section and the implication of anaesthesia: A prospective cohort study. Health Qual. Life Outcomes. 2017, 15, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shlomi Polachek, I.; Dulitzky, M.; Margolis-Dorfman, L.; Simchen, M.J. A simple model for prediction postpartum PTSD in high-risk pregnancies. Arch. Women’s Ment. Health 2016, 19, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Haagen, J.F.G.; Moerbeek, M.; Olde, E.; Van Der Hart, O.; Kleber, R.J. PTSD after childbirth: A predictive ethological model for symptom development. J. Affect. Disord. 2015, 185, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Vossbeck-Elsebusch, A.N.; Freisfeld, C.; Ehring, T. Predictors of posttraumatic stress symptoms following childbirth. BMC Psychiatry 2014, 14, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, E.; Ayers, S. Support during birth interacts with prior trauma and birth intervention to predict postnatal post-traumatic stress symptoms. Psychol. Health 2011, 26, 1553–1570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boudou, M.; Séjourné, N.; Chabrol, H. Douleur de l’accouchement, dissociation et détresse périnatales comme variables prédictives de symptômes de stress post-traumatique en post-partum. Gynecol. Obstet. Fertil. 2007, 35, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- Czarnocka, J.; Slade, P. Prevalence and predictors of post-traumatic stress symptoms following childbirth. Br. J. Clin. Psychol. 2000, 39, 35–51. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. PLoS Med. 2007, 4, e297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peduzzi, P.; Concato, J.; Kemper, E.; Holford, T.R.; Feinstem, A.R. A simulation study of the number of events per variable in logistic regression analysis. J. Clin. Epidemiol. 1996, 49, 1373–1379. [Google Scholar] [CrossRef]
- Callahan, J.L.; Borja, S.E.; Hynan, M.T. Modification of the Perinatal PTSD Questionnaire to enhance clinical utility. J. Perinatol. 2006, 9, 533–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosmer, D.W., Jr.; Lemeshow, S.; Sturdivant, R.X. Model-Building Strategies and Methods for Logistic Regression; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2013; pp. 89–151. [Google Scholar]
- Mickey, R.M.; Greenland, S. The impact of confounder selection criteria on effect estimation. Am. J. Epidemiol. 1989, 129, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Swets, J.A. Measuring the accuracy of diagnostic systems. Sci. Sci. 1988, 240, 1285–1293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, E.; Ayers, S.; Bradley, R. Exploration of a cognitive model to predict post-traumatic stress symptoms following childbirth. J. Anxiety Disord. 2010, 24, 353–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdollahpour, S.; Khosravi, A.; Bolbolhaghighi, N. The effect of the magical hour on post-traumatic stress disorder (PTSD) in traumatic childbirth: A clinical trial. J. Reprod. Infant. Psychol. 2016, 34, 403–412. [Google Scholar] [CrossRef]
- Silveira, M.F.; Mesenburg, M.A.; Bertoldi, A.D.; De Mola, C.L.; Bassani, D.G.; Domingues, M.R. The association between disrespect and abuse of women during childbirth and postpartum depression: Findings from the 2015 Pelotas birth cohort study. J. Affect. Disord. 2019, 256, 441–447. [Google Scholar] [CrossRef]
- De Schepper, S.; Vercauteren, T.; Tersago, J.; Jacquemyn, Y.; Raes, F.; Franck, E. Post-Traumatic Stress Disorder after childbirth and the influence of maternity team care during labour and birth: A cohort study. Midwifery 2016, 32, 87–92. [Google Scholar] [CrossRef]
- World Health Organization. Global Status Report on Violence Prevention; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- United Nations. A Human Rights-Based Approach to Mistreatment and Violence against Women in Reproductive Health Services with a Focus on Childbirth and Obstetric Violence. 2019. Available online: https://digitallibrary.un.org/record/3823698 (accessed on 23 December 2020).
- Martínez-Galiano, J.M.; Martinez-Vazquez, S.; Rodríguez-Almagro, J.; Hernández-Martinez, A. The magnitude of the problem of obstetric violence and its associated factors: A cross-sectional study. Women Birth 2020. [Google Scholar] [CrossRef]


| Predictor | PTSD (Score PPQ) Derivation Cohort | p-Value | |
|---|---|---|---|
| <19 Points n (%) | ≥19 Points n (%) | ||
| Maternal age | 0.199 | ||
| 35 years | 638 (84.6) | 116 (15.4) | |
| >35 years | 886 (86.8) | 132 (13.2) | |
| Education level | 0.401 | ||
| Primary school | 22 (75.9) | 7 (24.1) | |
| Secondary school | 77 (87.5) | 11 (12.5) | |
| High school | 323 (85.0) | 57 (15.0) | |
| University | 1082 (86.2) | 173 (13.8) | |
| Nationality | 0.986 | ||
| Spanish | 1443 (85.8) | 238 (14.2) | |
| Other | 61 (85.9) | 10 (14.1) | |
| Parity | <0.001 | ||
| Primiparous | 1004 (83.0) | 205 (17.0) | |
| Multiparous | 499 (92.1) | 43 (7.9) | |
| Live newborn | 0.056 | ||
| No | 8 (66.7) | 4 (33.3) | |
| Yes | 1496 (86.0) | 244 (14.0) | |
| Twin pregnancy | 0.319 | ||
| No | 1471 (86.0) | 240 (14.0) | |
| Yes | 33 (80.5) | 8 (19.5) | |
| Previous cesarean section | <0.001 | ||
| No | 1102 (89.7) | 126 (10.3) | |
| Yes | 402 (76.7) | 122 (23.3) | |
| Place of birth | 0.099 | ||
| Public hospital | 1210 (86.2) | 194 (13.8) | |
| Private hospital | 262 (83.2) | 53 (16.8) | |
| Midwife-led hospital | 6 (85.7) | 1 (14.3) | |
| Home | 26 (100.0) | 0 (0.0) | |
| Labor induction | 0.007 | ||
| No | 913 (87.7) | 128 (12.3) | |
| Yes | 591 (83.1) | 120 (16.9) | |
| Regional analgesia | 0.001 | ||
| No | 442 (90.4) | 47 (9.6) | |
| Yes | 1062 (84.1) | 201 (15.9) | |
| General anesthesia | <0.001 | ||
| No | 1461 (86.5) | 228 (13.5) | |
| Yes | 43 (68.3) | 20 (31.7) | |
| Natural analgesia | 0.139 | ||
| No | 1214 (85.3) | 210 (14.7) | |
| Yes | 290 (88.4) | 38 (11.6) | |
| Type of birth | <0.001 | ||
| Normal vaginal delivery | 912 (91.6) | 84 (8.4) | |
| Instrumental | 273 (84.0) | 52 (16.0) | |
| Elective CS | 109 (84.5) | 20 (15.5) | |
| Emergency CS | 210 (69.5) | 92 (30.5) | |
| Episiotomy | 0.925 | ||
| No | 1069 (85.8) | 177 (14.2) | |
| Yes | 435 (86.0) | 71 (14.0) | |
| Perineal tear | <0.001 | ||
| No | 940 (83.9) | 180 (16.1) | |
| Mild | 512 (90.9) | 51 (9.1) | |
| Severe (III–IV) | 52 (75.4) | 17 (24.6) | |
| Prematurity | 0.023 | ||
| No | 1141 (86.4) | 223 (13.6) | |
| Yes | 93 (78.8) | 25 (21.2) | |
| Maternal antenatal classes | 0.123 | ||
| No | 295 (87.5) | 42 (12.5) | |
| Yes (less than 5 classes) | 208 (81.9) | 46 (18.1) | |
| Yes (more than 5 classes) | 1001 (86.2) | 160 (13.8) | |
| Breastfeeding 1 h after childbirth | <0.001 | ||
| No | 338 (76.0) | 107 (24.0) | |
| Yes | 1166 (89.2) | 141 (10.8) | |
| Skin-to-skin contact | <0.001 | ||
| No | 302 (73.1) | 111 (26.9) | |
| Yes | 1202 (89.8) | 137 (10.2) | |
| Birth plan | <0.001 | ||
| No | 803 (87.8) | 112 (12.2) | |
| Yes, but not respected | 164 (65.3) | 87 (34.7) | |
| Yes, and was respected | 537 (91.6) | 49 (8.4) | |
| Admission of the newborn to care unit | <0.001 | ||
| No | 1324 (87.6) | 187 (12.4) | |
| Yes | 180 (74.7) | 61 (25.3) | |
| Hospital length of stay | <0.001 | ||
| 1 day | 122 (91.0) | 12 (9.0) | |
| 2 day | 779 (90.2) | 85 (9.8) | |
| 3 day | 365 (82.4) | 78 (17.6) | |
| 4 days or more | 238 (76.5) | 73 (23.5) | |
| Infant feeding on discharge | <0.001 | ||
| Maternal | 1226 (88.2) | 164 (11.8) | |
| Mixed | 233 (78.5) | 64 (21.5) | |
| Artificial | 45 (69.2) | 20 (30.8) | |
| Postpartum surgical intervention | 0.001 | ||
| No | 1449 (86.5) | 227 (13.5) | |
| Yes | 55 (72.4) | 21 (27.6) | |
| Hospital readmission | <0.001 | ||
| No | 1474 (86.4) | 232 (13.6) | |
| Yes | 30 (65.2) | 16 (34.8) | |
| Mean (SD) | Mean (SD) | ||
| Perception of adequate treatment by health professionals during pregnancy, childbirth and the puerperium. Likert scale 1–5 | 3.4 (0.93) | 2.88 (1.28) | <0.001 * |
| Perception of support by the couple during pregnancy, childbirth and the puerperium. Likert scale 1–5 | 2.99 (0.97) | 1.67 (1.22) | <0.001 * |
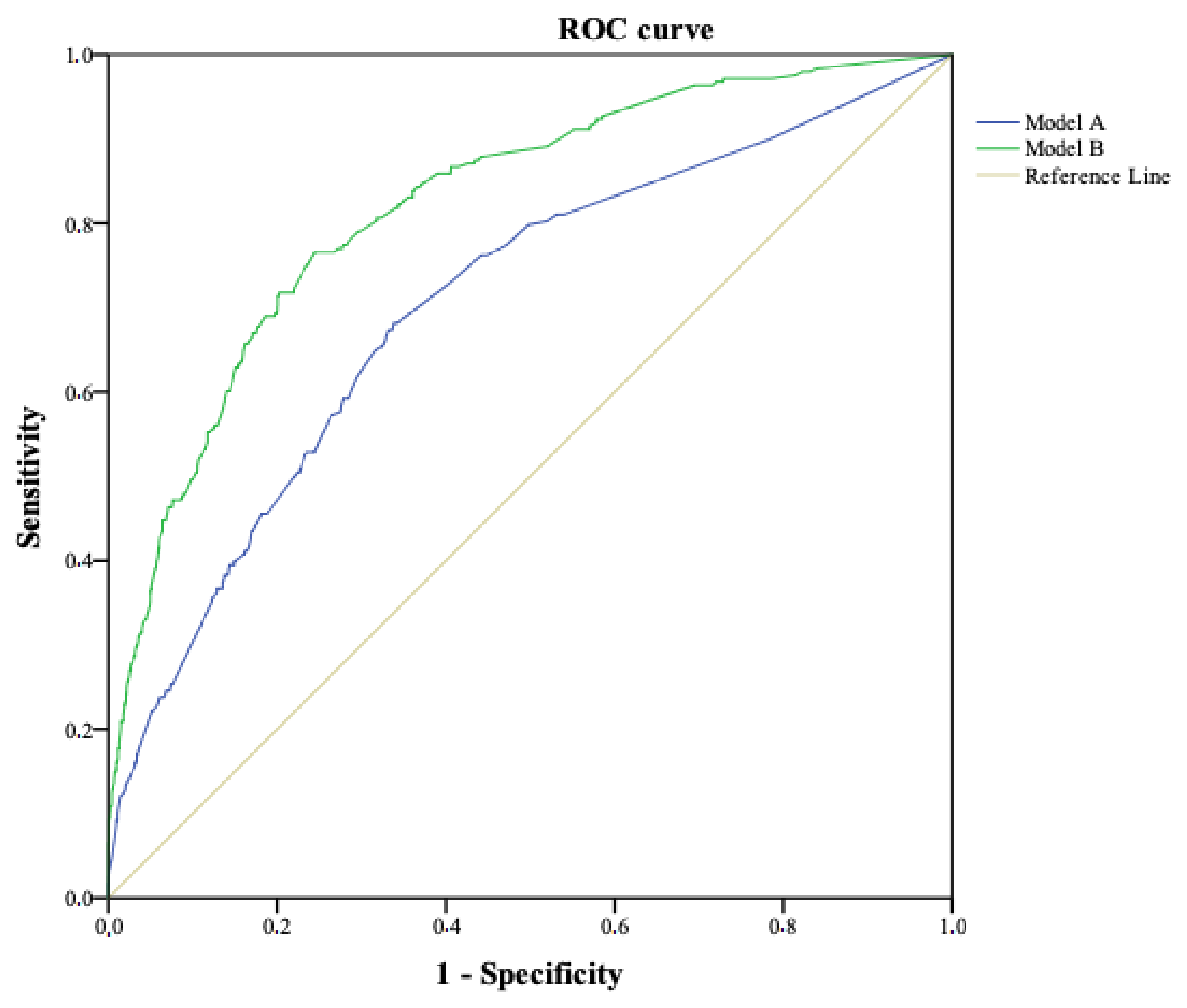
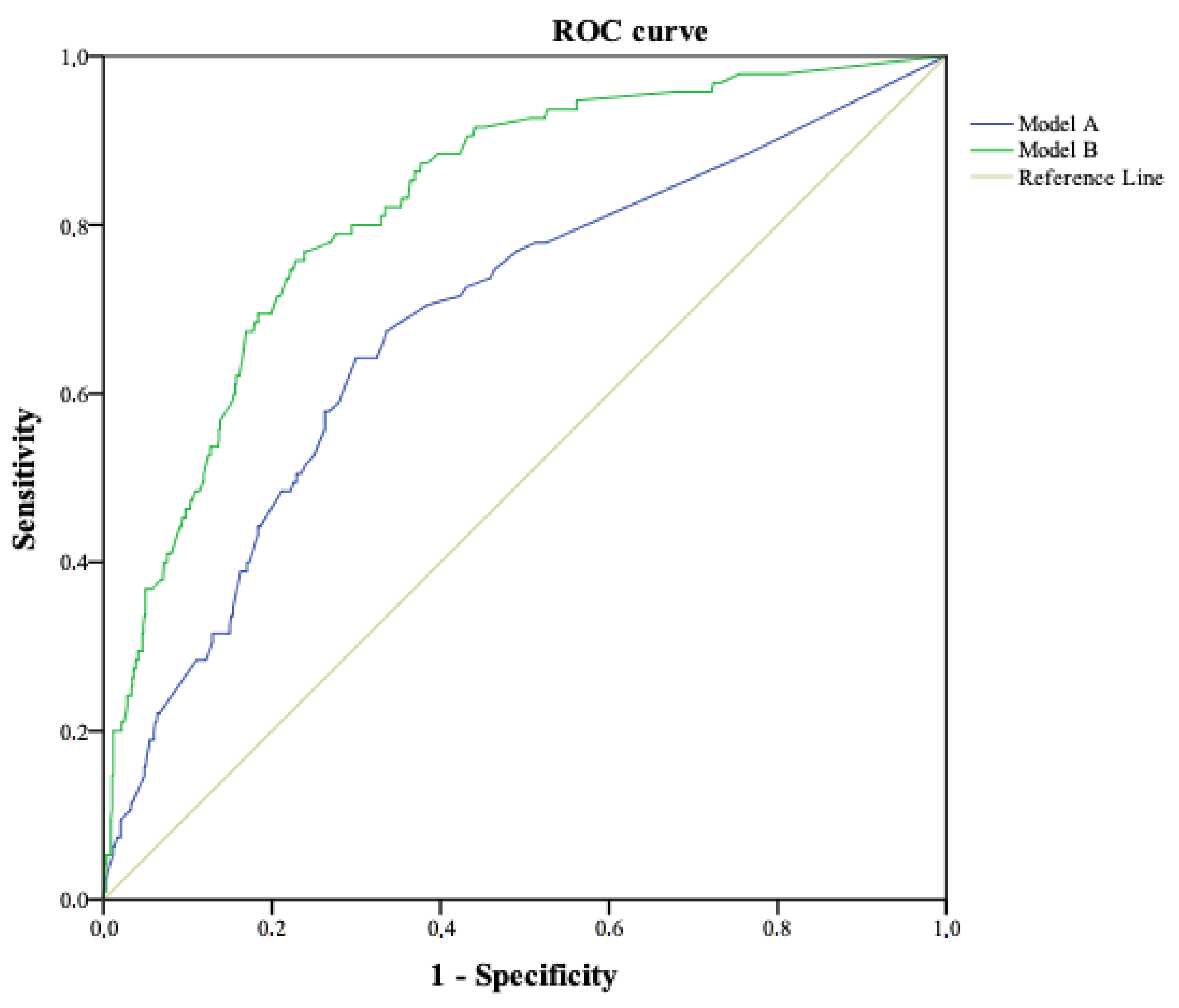
| Model Properties | Model A | Model B | ||||
|---|---|---|---|---|---|---|
| Number of Events in Derivation Cohort | 248 (14.2%) | |||||
| Number of Events in Validation Cohort | 95 (10.9%) | |||||
| Nagerlkerkes R-Square | 0.127 | 0.310 | ||||
| Hosmer–Lemeshow Test p-Value | 0.133 | 0.732 | ||||
| Risk Factor | Coef * Beta Value | OR (95% CI) | p-Value | Coef * Beta Value | OR (95% CI) | p-Value |
| Type of birth | ||||||
| Normal vaginal delivery | 1 (Ref) | 1 (Ref) | ||||
| Instrumental | 0.484 | 1.62 (1.10–2.41) | 0.016 | 0.344 | 1.22 (0.81–1.86) | 0.344 |
| Elective CS | 0.341 | 1.41 (0.77–2.57) | 0.267 | 0.200 | 1.22 (0.68–2.18) | 0.499 |
| Emergency CS | 1.121 | 3.07 (1.96–4.80) | <0.001 | 0.827 | 2.29 (1.56–3.35) | <0.001 |
| Initiate skin-to-skin contact | −0.428 | 0.65 (0.45–0.96) | 0.028 | |||
| Admission of the newborn to care unit | ||||||
| No | 1 (Ref) | 1 (Ref) | ||||
| Yes | 0.452 | 1.57 (1.26–2.87) | 0.015 | 0.503 | 1.65 (1.12–2.44) | 0.012 |
| Perineal tear | ||||||
| No | 1 (Ref) | |||||
| Type I–II | −0.020 | 0.98 (0.67–1.44) | 0.919 | |||
| Type III–IV | 0.795 | 2.21 (1.17–4.19) | 0.015 | |||
| Infant feeding on discharge | ||||||
| Maternal | 1 (Ref) | 1 (Ref) | ||||
| Mixed | 0.404 | 1.50 (1.06–2.12) | 0.022 | 0.122 | 1.13 (0.77–1.65) | 0.530 |
| Artificial | 0.740 | 2.10 (1.16–3.79) | 0.014 | 0.803 | 2.23 (1.13–4.04) | 0.021 |
| Hospital readmission | 0.934 | 2.55 (1.30–5.00) | 0.007 | 1.160 | 3.19 (1.43–7.11) | 0.005 |
| Partner’s perception of support (Likert scale 1–5) | −0.234 | 0.79 (0.69–0.91) | 0.001 | |||
| Perception of respect by professionals (Likert scale 1–5) | −0.863 | 0.42 (0.37–0.48) | <0.001 | |||
| Constant | −2.177 | 0.545 | ||||
| AUC-ROC derivation cohort | 0.70 (0.67–0.74) | <0.001 | 0.82 (0.79–0.85) | <0.001 | ||
| AUC-ROC validation cohort | 0.69 (0.63–0.75) | <0.001 | 0.83 (0.78–0.87) | <0.001 | ||
| Characteristics | Derivation Cohort N = 1752 n (%) | Validation Cohort N = 875 n (%) | p-Value * |
|---|---|---|---|
| PPQ | 0.018 | ||
| <19 | 1504 (85.8) | 780 (89.1) | |
| ≥19 | 248 (14.2) | 95 (10.9) | |
| Maternal age | 0.930 | ||
| ≤35 years | 754 (43.0) | 375 (42.9) | |
| >35 years | 998 (57.0) | 500 (57.1) | |
| Education level | 0.478 | ||
| Primary school | 29 (1.7) | 9 (28.6) | |
| Secondary school | 88 (5.0) | 37 (4.2) | |
| High school | 380 (21.7) | 193 (22.1) | |
| University | 1255 (71.6) | 636 (72.7) | |
| Nationality | 0.351 | ||
| Spanish | 1681 (95.9) | 846 (96.7) | |
| Other | 71 (4.1) | 29 (3.3) | |
| Parity | 0.092 | ||
| Primiparous | 1209 (69.0) | 575 (65.8) | |
| Multiparous | 542 (31.0) | 299 (34.2) | |
| Live newborn | 0.130 | ||
| No | 12 (0.7) | 2 (0.2) | |
| Yes | 1740 (86.0) | 873 (99.8) | |
| Twin pregnancy | 0.333 | ||
| No | 1711 (97.7) | 849 (97.0) | |
| Yes | 41 (2.3) | 26 (3.0) | |
| Previous cesarean section | 0.167 | ||
| No | 1228 (70.1) | 636 (72.7) | |
| Yes | 524 (29.9) | 239 (27.3) | |
| Place of birth | 0.526 | ||
| Public hospital | 1404 (80.1) | 697 (79.7) | |
| Private hospital | 315 (18.0) | 155 (17.7) | |
| Midwife-led hospital | 7 (0.4) | 3 (0.3) | |
| Home | 26 (1.5) | 20 (2.3) | |
| Labor induction | 0.213 | ||
| No | 1041 (59.4) | 542 (61.9) | |
| Yes | 711 (40.6) | 333 (38.1) | |
| Regional analgesia | 0.413 | ||
| No | 489 (27.9) | 231 (26.4) | |
| Yes | 1263 (72.1) | 644 (73.6) | |
| General anesthesia | 0.404 | ||
| No | 1689 (96.4) | 849 (97.0) | |
| Yes | 63 (3.6) | 26 (3.0) | |
| Natural analgesia | 0.768 | ||
| No | 1424 (81.3) | 707 (80.8) | |
| Yes | 328 (18.7) | 168 (19.2) | |
| Type of birth | 0.152 | ||
| Normal vaginal delivery | 996 (56.8) | 536 (61.3) | |
| Instrumental | 325 (18.6) | 146 (16.7) | |
| Elective CS | 129 (7.4) | 64 (7.3) | |
| Emergency CS | 302 (17.2) | 129 (314.7) | |
| Episiotomy | 0.965 | ||
| No | 1246 (71.1) | 623 (71.2) | |
| Yes | 506 (28.9) | 252 (28.8) | |
| Perineal tear | 0.157 | ||
| No | 1120 (63.9) | 529 (60.5) | |
| Mild | 563 (32.1) | 314 (35.9) | |
| Severe (III–IV) | 69 (3.9) | 32 (3.7) | |
| Prematurity | 0.821 | ||
| No | 1634 (93.3) | 814 (93.0) | |
| Yes | 118 (6.7) | 61 (7.0) | |
| Maternal antenatal classes | 0.133 | ||
| No | 337 (19.2) | 185 (21.1) | |
| Yes (less than 5 classes) | 254 (14.5) | 104 (11.9) | |
| Yes (more than 5 classes) | 1161 (66.3) | 586 (67.0) | |
| Breastfeeding 1 h after childbirth | 0.556 | ||
| No | 445 (25.4) | 213 (24.3) | |
| Yes | 1307 (74.6) | 662 (75.7) | |
| Skin-to-skin contact | 0.422 | ||
| No | 413 (23.6) | 194 (22.2) | |
| Yes | 1339 (76.4) | 681 (77.8) | |
| Birth plan | 0.739 | ||
| No | 915 (52.2) | 459 (52.5) | |
| Yes, but not respected | 251 (14.3) | 116 (13.3) | |
| Yes, and was respected | 586 (33.4) | 300 (34.3) | |
| Admission of the newborn to care unit | 0.886 | ||
| No | 1511 (86.2) | 753 (86.1) | |
| Yes | 241 (13.8) | 122 (13.9) | |
| Hospital length of stay | 0.987 | ||
| 1 day | 134 (7.6) | 69 (7.9) | |
| 2 day | 864 (49.3) | 434 (49.6) | |
| 3 day | 443 (25.3) | 216 (24.7) | |
| 4 days or more | 311 (17.8) | 156 (17.8) | |
| Infant feeding on discharge | |||
| Maternal | 1390 (79.3) | 681 (77.8) | 0.563 |
| Mixed | 297 (17.0) | 163 (18.6) | |
| Artificial | 65 (3.7) | 31 (3.5) | |
| Postpartum surgical intervention | |||
| No | 1676 (95.7) | 844 (96.5) | 0.331 |
| Yes | 76 (4.3) | 31 (3.5) | |
| Hospital readmission | |||
| No | 1706 (97.4) | 128 (12.3) | 0.480 |
| Yes | 46 (2.6) | 19 (2.2) | |
| Mean (SD) | Mean (SD) | ||
| Perception of adequate treatment by health professionals during pregnancy, childbirth, and the puerperium. Likert scale 1–5 | 3.33 (1.00) | 3.28 (1.04) | 0.334 |
| Perception of support by the couple during pregnancy, childbirth, and the puerperium. Likert scale 1–5 | 2.80 (1.11) | 2.83 (1.26) | 0.493 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Martínez, A.; Martínez-Vazquez, S.; Rodríguez-Almagro, J.; Delgado-Rodríguez, M.; Martínez-Galiano, J.M. Elaboration and Validation of Two Predictive Models of Postpartum Traumatic Stress Disorder Risk Formed by Variables Related to the Birth Process: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 92. https://doi.org/10.3390/ijerph18010092
Hernández-Martínez A, Martínez-Vazquez S, Rodríguez-Almagro J, Delgado-Rodríguez M, Martínez-Galiano JM. Elaboration and Validation of Two Predictive Models of Postpartum Traumatic Stress Disorder Risk Formed by Variables Related to the Birth Process: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(1):92. https://doi.org/10.3390/ijerph18010092
Chicago/Turabian StyleHernández-Martínez, Antonio, Sergio Martínez-Vazquez, Julián Rodríguez-Almagro, Miguel Delgado-Rodríguez, and Juan Miguel Martínez-Galiano. 2021. "Elaboration and Validation of Two Predictive Models of Postpartum Traumatic Stress Disorder Risk Formed by Variables Related to the Birth Process: A Retrospective Cohort Study" International Journal of Environmental Research and Public Health 18, no. 1: 92. https://doi.org/10.3390/ijerph18010092
APA StyleHernández-Martínez, A., Martínez-Vazquez, S., Rodríguez-Almagro, J., Delgado-Rodríguez, M., & Martínez-Galiano, J. M. (2021). Elaboration and Validation of Two Predictive Models of Postpartum Traumatic Stress Disorder Risk Formed by Variables Related to the Birth Process: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health, 18(1), 92. https://doi.org/10.3390/ijerph18010092