
Unified Protocol for the Transdiagnostic Treatment of Emotional Disorders in Medical Conditions: A Systematic Review




Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection
2.4. Risk of Bias Assessment
3. Results
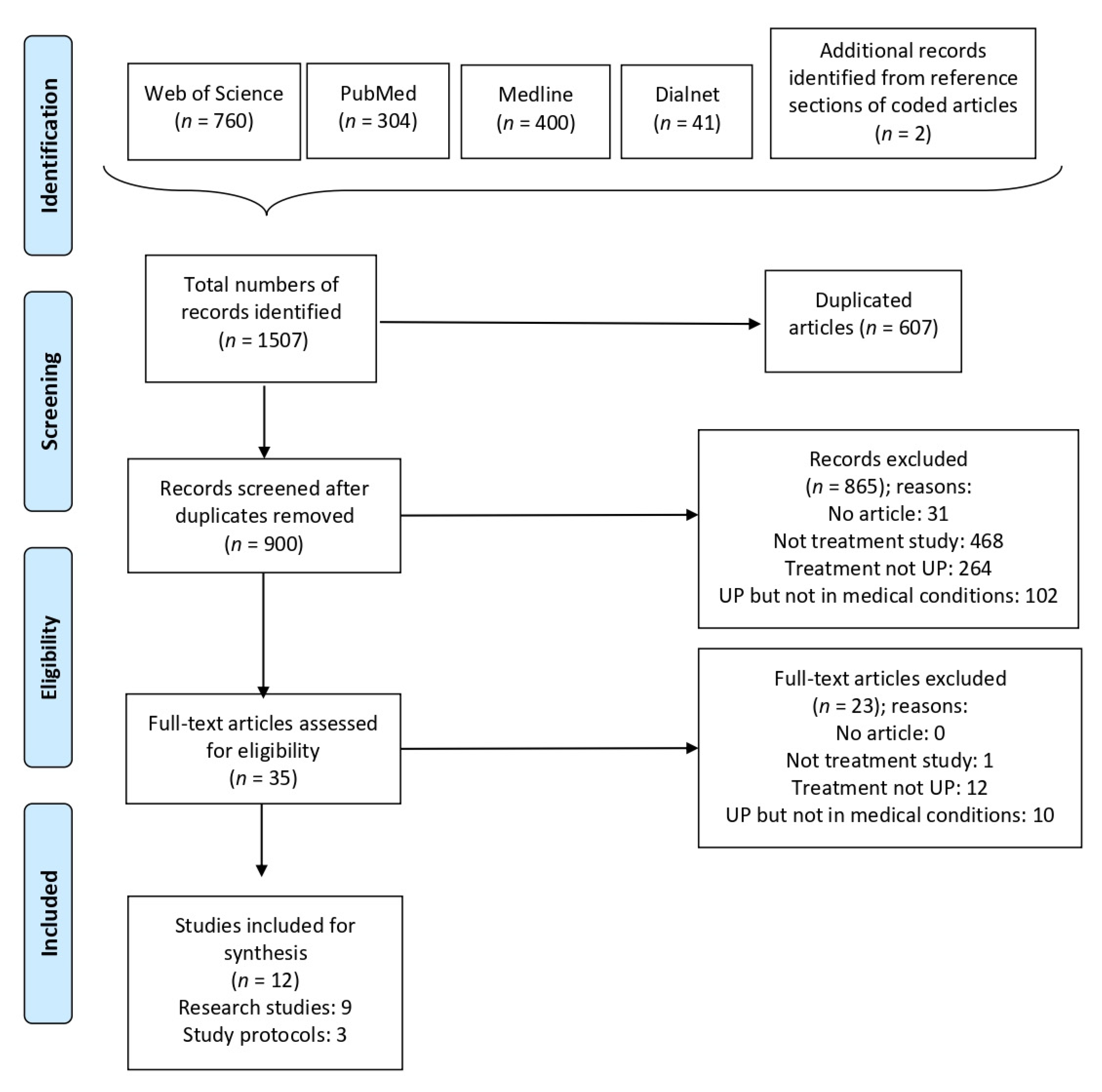
3.1. Search and Screening
3.2. Characteristics of the Included Research Studies
3.3. Modifications to UP
3.4. Clinical Effectiveness in Emotional Disorders and/or Emotional Symptomatology
3.5. Clinical Effectiveness in Medical Symptoms
3.6. Patient’s Opinion after the UP Intervention
3.7. Risk of Bias Assessment
3.8. Future Directions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A. Complete List of Search Terms and Combinations

{kind=link}
| Search | Keywords | Results |
|---|---|---|
| 1 | “Unified protocol” AND “health” | 107 |
| 2 | “Unified protocol” AND “disease” | 28 |
| 3 | “Unified protocol” AND “illness” | 17 |
| 4 | “Unified protocol” AND “syndrome” | 8 |
| 5 | “Unified protocol” AND “medical condition” | 0 |
| 6 | “Unified protocol” AND “disorder” | 190 |
| 7 | “Unified protocol” AND “sickness” | 1 |
| 8 | “Unified protocol” AND “condition” | 30 |
| 9 | “Unified protocol” AND “chronic” | 18 |
| 10 | “Unified protocol” AND “physical condition” | 0 |
| 11 | “Unified protocol” AND “physical problem” | 0 |
| 12 | “Unified protocol” AND “physical health” | 2 |
| 13 | “cognitive behavioral therapy” AND “health” AND “transdiagnostic” | 165 |
| 14 | “cognitive behavioral therapy” AND “disease” AND “transdiagnostic” | 14 |
| 15 | “cognitive behavioral therapy” AND “illness” AND “transdiagnostic” | 20 |
| 16 | “cognitive behavioral therapy” AND “syndrome” AND “transdiagnostic” | 12 |
| 17 | “cognitive behavioral therapy” AND “medical condition” AND “transdiagnostic” | 0 |
| 18 | “cognitive behavioral therapy” AND “disorder” AND “transdiagnostic” | 296 |
| 19 | “cognitive behavioral therapy” AND “sickness” AND “transdiagnostic” | 0 |
| 20 | “cognitive behavioral therapy” AND “condition” AND “transdiagnostic” | 48 |
| 21 | “cognitive behavioral therapy” AND “chronic” AND “transdiagnostic” | 24 |
| 22 | “cognitive behavioral therapy” AND “physical condition” AND “transdiagnostic” | 0 |
| 23 | “cognitive behavioral therapy” AND “physical problem” AND “transdiagnostic” | 0 |
| 24 | “cognitive behavioral therapy” AND “physical health” AND “transdiagnostic” | 11 |
| 25 | “emotion regulation” AND “health” AND “transdiagnostic” | 100 |
| 26 | “emotion regulation” AND “disease” AND “transdiagnostic” | 7 |
| 27 | “emotion regulation” AND “illness” AND “transdiagnostic” | 22 |
| 28 | “emotion regulation” AND “syndrome” AND “transdiagnostic” | 11 |
| 29 | “emotion regulation” AND “medical condition” AND “transdiagnostic” | 0 |
| 30 | “emotion regulation” AND “disorder” AND “transdiagnostic” | 235 |
| 31 | “emotion regulation” AND “sickness” AND “transdiagnostic” | 1 |
| 32 | “emotion regulation” AND “condition” AND “transdiagnostic” | 25 |
| 33 | “emotion regulation” AND “chronic” AND “transdiagnostic” | 20 |
| 34 | “emotion regulation” AND “physical condition” AND “transdiagnostic” | 0 |
| 35 | “emotion regulation” AND “physical problem” AND “transdiagnostic” | 0 |
| 36 | “emotion regulation” AND “physical health” AND “transdiagnostic” | 2 |
Appendix B. Quality Assessment of the Included Studies
| [42] | [43] | [44] | [48] | |
|---|---|---|---|---|
| 1. Was the study question or objective clearly stated? | Yes | Yes | Yes | Yes |
| 2. Were the eligibility/selection criteria for the study population prespecified and clearly described? | Yes | Yes | Yes | Yes |
| 3. Were the study participants representative of those who would be eligible for the test/service/intervention in the general or clinical population of interest? | Yes | Yes | Yes | Yes |
| 4. Were all the eligible participants who met the prespecified entry criteria enrolled? | No | Yes | Yes | Yes |
| 5. Was the sample size large enough to provide reliable findings? | NR | No | Yes | NR |
| 6. Was the test/service/intervention clearly described and delivered consistently across the study population? | Yes | Yes | Yes | Yes |
| 7. Were the outcome measures prespecified, clearly defined, valid, reliable, and assessed consistently across the study participants? | Yes | Yes | Yes | Yes |
| 8. Were the people assessing the outcomes blinded to participants’ exposures/interventions? | NR | NR | NR | NR |
| 9. Was loss to follow-up after the baseline 20% or less? Were those lost to follow-up accounted for in the analysis? | Yes | Yes | Yes | No |
| 10. Did the statistical methods examine changes in outcome measures from before to after the intervention? Were statistical tests that provided p values for the pre-to-post changes done? | Yes | Yes | Yes | Yes |
| 11. Were outcome measures of interest taken many times before and many times after the intervention (i.e., was an interrupted time-series design used)? | No | Yes | No | Yes |
| 12. If the intervention was conducted as a group (e.g., a whole hospital, a community, etc.), did the statistical analysis take into account the use of individual-level data to determine effects at the group level? | NA | NA | NA | NA |
| Total score (maximum 12 points) | 7 | 9 | 9 | 8 |
| [45] | [38] | [46] | [47] | |
|---|---|---|---|---|
| 1. Was the study described as randomized, a randomized trial, a randomized clinical trial, or an RCT? | No | Yes | Yes | Yes |
| 2. Was the randomization method adequate (i.e., use of randomly generated assignment)? | CD | Yes | Yes | Yes |
| 3. Was the treatment allocation concealed (so that assignments could not be predicted)? | NR | Yes | Yes | Yes |
| 4. Were the study participants and providers blinded to the treatment group assignment? | NR | Yes | Yes | Yes |
| 5. Were the people assessing the outcomes blinded to the participants’ group assignments? | NR | Yes | Yes | Yes |
| 6. Were the groups similar at the baseline for important characteristics that could affect outcomes (e.g., demographics, risk factors, co-morbid conditions)? | NR | Yes | Yes | Yes |
| 7. Was the overall drop-out rate from the study at the endpoint 20% or lower of the number allocated to treatment? | NR | Yes | No | No |
| 8. Was the differential drop-out rate (between treatment groups) at the endpoint 15% or lower? | NR | Yes | No | Yes |
| 9. Was adherence to the intervention protocols for each treatment group good? | NR | Yes | Yes | Yes |
| 10. Were other interventions avoided or similar in groups (e.g., similar background treatments)? | NR | Yes | Yes | Yes |
| 11. Were outcomes assessed by valid and reliable measures, implemented consistently across the study participants? | Yes | Yes | Yes | Yes |
| 12. Did the authors report if sample size was big enough to detect a difference in the main outcome between groups with at least 80% power? | No | No | Yes | Yes |
| 13. Were the reported outcomes or analyzed subgroups prespecified (i.e., identified before analyses were conducted)? | Yes | Yes | Yes | Yes |
| 14. Were all the randomized participants analyzed in the group to which they were originally assigned, i.e., did they use an intention-to-treat analysis? | Yes | Yes | Yes | Yes |
| Total score (maximum 14 points) | 3 | 13 | 12 | 13 |
| [37] | |
|---|---|
| 1. Was the study question or objective clearly stated? | Yes |
| 2. Was the study population clearly and fully described, including a case definition? | Yes |
| 3. Were the cases consecutive? | NR |
| 4. Were the subjects comparable? | Yes |
| 5. Was the intervention clearly described? | Yes |
| 6. Were the outcome measures clearly defined, valid, reliable, and implemented consistently across the study participants? | Yes |
| 7. Was follow-up length adequate? | No |
| 8. Were the statistical methods well-described? | No |
| 9. Were the results well-described? | Yes |
| Total score (maximum 9 points) | 6 |
References
- Porta, M. A Dictionary of Epidemiology, 5th ed.; Oxford University Press: New York, NY, USA, 2008; pp. 27–58. [Google Scholar]
- World Health Organization (WHO). Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 15 April 2021).
- World Health Organization (WHO). Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2016. Available online: https://www.who.int/data/gho/data/themes/topics/indicator-groups/indicator-group-details/GHO/life-expectancy-and-healthy-life-expectancy (accessed on 7 November 2020).
- WHO. World Health Statistics 2020: Monitoring Health for the SDGs Sustainable Development Goals; World Health Organization: Geneve, Switzerland, 2020; pp. 6–11. [Google Scholar]
- Naylor, C.; Parsonage, M.; McDaid, D.; Knapp, M.; Fossey, M.; Galea, A. Long-Term Conditions and Mental Health: The Cost of Co-Morbidities; The King’s Fund and Centre for Mental Health: London, UK, 2012; pp. 1–32. [Google Scholar]
- Daré, L.O.; Bruand, P.E.; Gérard, D.; Marin, B.; Lameyre, V.; Boumédiène, F.; Preux, P.M. Co-morbidities of mental disorders and chronic physical diseases in developing and emerging countries: A meta-analysis. BMC Public Health 2019, 19, 304. [Google Scholar] [CrossRef]
- Doherty, A.M.; Gaughran, F. The interface of physical and mental health. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Moussavi, S.; Chatterji, S.; Verdes, E.; Tandon, A.; Patel, V.; Ustun, B. Depression, chronic diseases, and decrements in health: Results from the World Health Surveys. Lancet 2017, 370, 851–858. [Google Scholar] [CrossRef]
- Prince, M.; Patel, V.; Saxena, S.; Maj, M.; Maselko, J.; Phillips, M.R.; Rahman, A. No health without mental health. Lancet 2007, 370, 859–877. [Google Scholar] [CrossRef]
- Barlow, D.H.; Farchione, T.J.; Sauer-Zavala, S.; Murray-Latin, H.; Ellard, K.K.; Bullis, J.R.; Bentley, K.H.; Boettcher, H.T.; Cassiello-Robbins, C. Unified Protocol for Transdiagnostic Treatment of Emotional Disorders: Therapist Guide, 2nd ed.; Oxford University Press: New York, NY, USA, 2018; pp. 19–27. [Google Scholar]
- Clarke, D.M.; Currie, K.C. Depression, anxiety and their relationship with chronic diseases: A review of the epidemiology, risk and treatment evidence. Med. J. Aust. 2009, 190, S54–S60. [Google Scholar] [CrossRef] [PubMed]
- Scott, K.M.; Bruffaerts, R.; Tsang, A.; Ormel, J.; Alonso, J.; Angermeyer, M.C.; Benjet, C.; Bromet, E.; de Girolamo, G.; de Graaf, R.; et al. Depression-anxiety relationships with chronic physical conditions: Results from the World Mental Health Surveys. J. Affect. Disord. 2007, 103, 113–120. [Google Scholar] [CrossRef]
- Caruso, R.; Nanni, M.G.; Riba, M.; Sabato, S.; Mitchell, A.J.; Croce, E.; Grassi, L. Depressive spectrum disorders in cancer: Prevalence, risk factors and screening for depression: A critical review. Acta Oncol. 2017, 56, 146–155. [Google Scholar] [CrossRef] [Green Version]
- Yu, M.; Zhang, X.; Lu, F.; Fang, L. Depression and risk for diabetes: A meta-analysis. Can. J. Diabetes 2015, 39, 266–272. [Google Scholar] [CrossRef] [PubMed]
- IsHak, W.W.; Wen, R.Y.; Naghdechi, L.; Vanle, B.; Dang, J.; Knosp, M.; Dascal, J.; Marcia, L.; Gohar, Y.; Eskander, L.; et al. Pain and Depression: A Systematic Review. Harv. Rev. Psychiatry 2018, 26, 352–363. [Google Scholar] [CrossRef]
- Celano, C.M.; Villegas, A.C.; Albanese, A.M.; Gaggin, H.K.; Huffman, J.C. Depression and anxiety in heart failure: A review. Harv. Rev. Psychiatry 2018, 26, 175. [Google Scholar] [CrossRef] [PubMed]
- Abou Abbas, L.; Salameh, P.; Nasser, W.; Nasser, Z.; Godin, I. Obesity and symptoms of depression among adults in selected countries of the Middle East: A systematic review and meta-analysis. Clin. Obes. 2015, 5, 2–11. [Google Scholar] [CrossRef]
- Brandt, C.; Zvolensky, M.J.; Woods, S.P.; Gonzalez, A.; Safren, S.A.; O’Cleirigh, C.M. Anxiety symptoms and disorders among adults living with HIV and AIDS: A critical review and integrative synthesis of the empirical literature. Clin. Psychol. Rev. 2017, 51, 164–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, Y.; Fang, J.; Huang, W.; Qin, S. Efficacy of Cognitive Behavioral Therapy for Heart Failure. Int. Heart J. 2019, 60, 665–670. [Google Scholar] [CrossRef] [Green Version]
- Reavell, J.; Hopkinson, M.; Clarkesmith, D.; Lane, D.A. Effectiveness of Cognitive Behavioral Therapy for Depression and Anxiety in Patients with Cardiovascular Disease: A Systematic Review and Meta-Analysis. Psychosom. Med. 2018, 80, 742–753. [Google Scholar] [CrossRef] [Green Version]
- National Clinical Guideline Centre (NICE). Depression in Adults with Chronic Physical Health Problems: Treatment and Management. Clinical Guideline 91. Available online: https://www.nice.org.uk/guidance/cg91/resources/depression-in-adults-with-a-chronic-physical-health-problem-recognition-and-management-pdf-975744316357 (accessed on 20 November 2020).
- Ye, M.; Du, K.; Zhou, J.; Zhou, Q.; Shou, M.; Hu, B.; Jiang, P.; Dong, N.; He, L.; Liang, S.; et al. A meta-analysis of the efficacy of cognitive behavior therapy on quality of life and psychological health of breast cancer survivors and patients. Psycho Oncol. 2018, 27, 1695–1703. [Google Scholar] [CrossRef]
- Li, C.; Xu, D.; Hu, M.; Tan, Y.; Zhang, P.; Li, G.; Chen, L. A systematic review and meta-analysis of randomized controlled trials of cognitive behavior therapy for patients with diabetes and depression. J. Psychosom. Res. 2017, 95, 44–54. [Google Scholar] [CrossRef]
- Ghielen, I.; Rutten, S.; Boeschoten, R.E.; Houniet-de Gier, M.; van Wegen, E.E.; Van den Heuvel, O.A.; Cuijpers, P. The effects of cognitive behavioral and mindfulness-based therapies on psychological distress in patients with multiple sclerosis, Parkinson’s disease and Huntington’s disease: Two meta-analyses. J. Psychosom. Res. 2019, 122, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Spurgeon, P.; Hicks, C.; Barwell, F.; Walton, I.; Spurgeon, T. Counselling in primary care: A study of the psychological impact and cost benefits for four chronic conditions. Eur. J. Psychother. Couns. 2005, 7, 269–290. [Google Scholar] [CrossRef]
- Thompson, R.D.; Delaney, P.; Flores, I.; Szigethy, E. Cognitive-Behavioral Therapy for Children with Comorbid Physical Illness. Child. Adolesc. Psychiatr. Clin. 2011, 20, 329–348. [Google Scholar] [CrossRef] [PubMed]
- McManus, F.; Shafran, R.; Cooper, Z. What does a transdiagnostic approach have to offer the treatment of anxiety disorders? Br. J. Clin. Psychol. 2010, 49, 491–505. [Google Scholar] [CrossRef]
- Brown, T.A.; Barlow, D.H. A proposal for a dimensional classification system based on the shared features of the DSM-IV anxiety and mood disorders: Implications for assessment and treatment. Psychol. Assess. 2009, 21, 256. [Google Scholar] [CrossRef] [Green Version]
- Smith, T.W.; MacKenzie, J. Personality and risk of physical illness. Annu. Rev. Clin. Psychol. 2006, 2, 435–467. [Google Scholar] [CrossRef] [Green Version]
- Suls, J.; Bunde, J. Anger, anxiety, and depression as risk factors for cardiovascular disease: The problems and implications of overlapping affective dispositions. Psychol. Bull. 2005, 131, 260–300. [Google Scholar] [CrossRef]
- Lahey, B.B. Public health significance of neuroticism. Am. Psychol. 2009, 64, 241–256. [Google Scholar] [CrossRef] [Green Version]
- Brown, T.A.; Campbell, L.A.; Lehman, C.L.; Grisham, J.R.; Mancill, R.B. Current and lifetime comorbidity of the DSM-IV anxiety and mood disorders in a large clinical sample. J. Abnorm. Psychol. 2001, 110, 585. [Google Scholar] [CrossRef] [PubMed]
- McHugh, R.K.; Murray, H.W.; Barlow, D.H. Equilibrio de fidelidad y adaptación en la difusión de tratamientos respaldados empíricamente: La promesa de las intervenciones transdiagnósticas. Investigación y Terapia del Comportamiento. 2009, 47, 946–953. [Google Scholar] [CrossRef] [Green Version]
- Sauer-Zavala, S.; Tirpak, J.W.; Eustis, E.H.; Woods, B.K.; Russell, K. Unified Protocol for the Transdiagnostic Prevention of Emotional Disorders: Evaluation of a Brief, Online Course for College Freshmen. Behav. Ther. 2021, 52, 64–76. [Google Scholar] [CrossRef] [PubMed]
- Ferreres-Galán, V.; Meseguer-Valero, M.C.; Ariza-Albinana, S.; Quilez-Orden, A.; Osma, J. Aplicación del Protocolo Unificado en el Equipo Específico de Intervención con Infancia y Adolescencia (EEIIA): Estudio piloto en mujeres víctimas de violencia intrafamiliar y de pareja. In Aplicaciones Del Protocolo Unificado Para El Tratamiento Transdiagnóstico de La Disregulación Emocional; Osma López, J., Ed.; Alianza Editorial: Madrid, Spain, 2019; pp. 203–218. [Google Scholar]
- Reinholt, N.; Aharoni, R.; Winding, C.; Rosenberg, N.; Rosenbaum, B.; Arnfred, S. Transdiagnostic group CBT for anxiety disorders: The unifed protocol in mental health services. Cogn. Behav. Ther. 2017, 46, 29–43. [Google Scholar] [CrossRef]
- Sandín, B.; García-Escalera, J.; Valiente, R.M.; Espinosa, V.; Chorot, P. Clinical Utility of an Internet-Delivered Version of the Unified Protocol for Transdiagnostic Treatment of Emotional Disorders in Adolescents (iUP-A): A Pilot Open Trial. Int. J. Environ. Res. Public Health 2020, 17, 8306. [Google Scholar] [CrossRef] [PubMed]
- Sakiris, N.; Berle, D. A systematic review and meta-analysis of the Unified Protocol as a transdiagnostic emotion regulation based intervention. Clin. Psychol. Rev. 2019, 72, 101751. [Google Scholar] [CrossRef] [PubMed]
- Cassiello-Robbins, C.; Southward, M.W.; Tirpak, J.W.; Sauer-Zavala, S. A systematic review of Unified Protocol applications with adult populations: Facilitating widespread dissemination via adaptability. Clin. Psychol. Rev. 2020, 78, 101852. [Google Scholar] [CrossRef] [PubMed]
- Mohsenabadi, H.; Zanjani, Z.; Shabani, M.J.; Arj, A. A randomized clinical trial of the Unified Protocol for Transdiagnostic treatment of emotional and gastrointestinal symptoms in patients with irritable bowel syndrome: Evaluating efficacy and mechanism of change. J. Psychosom. Res. 2018, 113, 8–15. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- National Heart Lung and Blood Institute (NHLBI). Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 22 February 2021).
- Weihs, K.L.; McConnell, M.H.; Wiley, J.F.; Crespi, C.M.; Sauer-Zavala, S.; Stanton, A.L. A preventive intervention to modify depression risk targets after breast cancer diagnosis: Design and single-arm pilot study. Psycho Oncol. 2019, 28, 880–887. [Google Scholar] [CrossRef]
- Allen, L.B.; Tsao, J.C.; Seidman, L.C.; Ehrenreich-May, J.; Zeltzer, L.K. A unified, transdiagnostic treatment for adolescents with chronic pain and comorbid anxiety and depression. Cogn. Behav. Pract. 2012, 19, 56–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parsons, J.T.; Rendina, H.J.; Moody, R.L.; Gurung, S.; Starks, T.J.; Pachankis, J.E. Feasibility of an emotion regulation intervention to improve mental health and reduce HIV transmission risk behaviors for HIV-positive gay and bisexual men with sexual compulsivity. AIDS Behav. 2017, 21, 1540–1549. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, G.O.; Saint-Hilaire, M.; Thomas, C.A.; Barlow, D.H.; Cronin-Golomb, A. Cognitive-Behavioral Therapy for Anxiety in Parkinson’s Disease. Behav. Modif. 2020, 44, 552–579. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, E.; Hosseini, S.; Bakhtiyari, M.; Mohammadi, A.; Isfeedvajani, M.S.; Arani, A.M.; Sadaat, S.H. Comparing the effectiveness of the Unified Protocol Transdiagnostic and Mindfulness Based Stress Reduction Program on anxiety and depression in infertile women receiving in vitro fertilization. J. Res. Med. Dent. Sci. 2019, 7, 44–51. [Google Scholar]
- Nazari, N.; Aligholipour, A.; Sadeghi, M. Transdiagnostic treatment of emotional disorders for women with multiple sclerosis: A randomized controlled trial. BMC Women’s Health 2020, 20, 245. [Google Scholar] [CrossRef]
- Nazari, N.; Sadeghi, M.; Ghadampour, E.; Mirzaeefar, D. Transdiagnostic treatment of emotional disorders in people with multiple sclerosis: Randomized controlled trial. BMC Psychol. 2020, 8, 114. [Google Scholar] [CrossRef]
- Wurm, M.; Strandberg, E.K.; Lorenz, C.; Tillfors, M.; Buhrman, M.; Holländare, F.; Boersma, K. Internet delivered transdiagnostic treatment with telephone support for pain patients with emotional comorbidity: A replicated single case study. Internet Interv. 2017, 10, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Tully, P.J.; Turnbull, D.A.; Horowitz, J.D.; Beltrame, J.F.; Selkow, T.; Baune, B.T.; Markwick, E.; Sauer-Zavala, S.; Baumeister, H.; Cosh, S.; et al. Cardiovascular Health in Anxiety or Mood Problems Study (CHAMPS): Study protocol for a randomized controlled trial. Trials 2016, 17, 18. [Google Scholar] [CrossRef] [Green Version]
- Quilez-Orden, A.; Ferreres-Galán, V.; Osma, J. Feasibility and Clinical Usefulness of the Unified Protocol in Online Group Format for Bariatric Surgery Candidates: Study Protocol for a Multiple Baseline Experimental Design. Int. J. Environ. Res. Public Health 2020, 17, 6155. [Google Scholar] [CrossRef] [PubMed]
- Taple, B.J.; Griffith, J.W.; Weaver, C.; Kenton, K.S. Enhancing behavioral treatment for women with pelvic floor disorders: Study protocol for a pilot randomized controlled trial. Contemp. Clin. Trials. Commun. 2020, 17, 100514. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M.; Shen, Y. Anxiety in children and adolescents with chronic physical illnesses: A meta-analysis. Acta Paediatr. 2011, 100, 1069–1076. [Google Scholar] [CrossRef]
- Pinquart, M.; Shen, Y. Depressive symptoms in children and adolescents with chronic physical illness: An updated meta-analysis. J. Pediatr. Psychol. 2011, 36, 375–384. [Google Scholar] [CrossRef] [Green Version]
- United Nations Organization. Transforming Our World: The 2030 Agenda for Sustainable Development. Available online: https://sustainabledevelopment.un.org/post2015/transformingourworld/publication (accessed on 22 February 2021).
- WHO. Plan de Acción Mundial para la Prevención y el Control de las Enfermedades No Transmisibles 2013–2020; World Health Organization: Geneve, Switzerland, 2013; pp. 1–44. [Google Scholar]
- Hader, J.M.; White, R.; Lewis, S.; Foreman, J.L.; McDonald, P.W.; Thompson, L.G. Doctors’ views of clinical practice guidelines: A qualitative exploration using innovation theory. J. Eval. Clin. 2007, 13, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Geers, A.L.; Rose, J.P.; Fowler, S.L.; Rasinski, H.M.; Brown, J.A.; Helfer, S.G. Why does choice enhance treatment effectiveness? Using placebo treatments to demonstrate the role of personal control. J. Pers. Soc. Psychol. 2013, 105, 549–566. [Google Scholar] [CrossRef]
- Whitfield, G. Group cognitive-behavioural therapy for anxiety and depression. Adv. Psychiatr. Treat. 2010, 16, 219–227. [Google Scholar] [CrossRef]
- Osma, J.; Castellano, C.; Crespo, E.; García-Palacios, A. The unified protocol for transdiagnostic treatment of emotional disorders in group format in a spanish public mental health setting. Behav. Psychol. Psicol. Conduct. 2015, 23, 447–466. [Google Scholar] [CrossRef] [Green Version]
- Andersson, G. Internet-Delivered Psychological Treatments. Annu. Rev. Clin. Psychol. 2016, 12, 157–179. [Google Scholar] [CrossRef] [PubMed]
- Wind, T.R.; Rijkeboer, M.; Andersson, G.; Riper, H. The COVID-19 pandemic: The ’black swan’ for mental health care and a turning point for e-health. Internet Interv. 2020, 20, 100317. [Google Scholar] [CrossRef] [PubMed]

| Reference, Country and Publication Year | Sample (N) | Study Design and Setting | Medical Condition | Emotional Disorder | Length/Session Frequency | Primary and Secondary Measures | Results |
|---|---|---|---|---|---|---|---|
| [44] USA, 2012 | 2 Tx Age: 14, 17 Gender: 1 woman and 1 man | Case study/ Individual—Outpatient | Chronic pain | SAD, MDD | 12 and 17 sessions/50 min/1 per week | CSI: somatization; EESC: emotional awareness and expression; FPS-R: pain intensity; FDI: functional disability; RCADS (total anxiety and depression, social anxiety and depression subscales). | Case 1: improvements pre-to-post in FDI, RCADS (total and social anxiety), EESC, CSI and pain level maintained (FPS-R = 8). Case 2: slight improvement in RCADS (total) at post-, with no changes in RCADS (depression) and worse EESC, CSI and FPS-R levels. At the 3-month follow-up, significant improvements in all the levels were observed in both cases (RCADStotal from 31 to 17 and from 44 to 37; EESCce from 18 to 14 and 22 to 14; EESCee from 22 to 18 and from 36 to 28; CSI from 12 to 9 and from 32 to 18; FPS-R from 8 to 6 and from 6 to 2). |
| [47] Iran, 2019 | 45 (15 Tx1. + 15 Tx2 + 15 Cont.) Age: 20–45 Gender: 100% woman | RCT/Group—Outpatient | Infertility | Anxious and depressive symp. | UP (Tx): 10 sessions/2 h/1 per week MBSR (Cont.): 8 sessions/2 h/1 per week | BAI: anxious symptoms; BDI-II: depressive symptoms; DERS: emotional dysregulation; IUS-12: intolerance to uncertainty. | Improved anxious and depressive symp. at post- and 3-month follow-up for the UP condition and in MBSR. Reported results do not explain if there was any significant difference between both conditions. Significantly better improvements in the UP group compared to the waiting list condition (anxious and depressive symp. increased at post- and 3-month follow-up in the latter). |
| [40] Iran, 2018 | 64 (32 cont. + 32 Tx) Age: 30.9 Gender: 59.38% woman 40.63% man | RCT/Individual—Outpatient | Irritable bowel syndrome | Anxious and depressive symp. | 12 sessions/2 h/1 per week | DASS-42: anxious, depressive and stress symptoms; ERQ: emotional regulation strategies; GSRS: severity of intestinal symp. | Significant decrease in depression, anxiety, stress, gastrointestinal symp., and significant improvement in cognitive reappraisal and emotional suppression strategies with a marked effect sizes: between-group comparison (Cohen’s d between 0.97 and 1.34) and under the UP condition (Cohen’s d between 0.92 and 1.18). No significant differences found for the waiting list condition from pre- to post-treatment for any measure. Mediation analyses indicated that changes in emotional regulation mediated the effect of UP on emotional and gastrointestinal symptomatology. |
| [48] Iran, 2020 | 64 (32 Cont + 32 Tx) Age: 35.13 Gender: 100% woman | RCT/Group- Outpatient | Multiple sclerosis | Anxiety and/or depressive disorder | UP: 14 sessions/2 h/1 per week TAU: 14 sessions/2 h/1 per week | DERS: emotional dysregulation; HADS: anxious and depressive symptoms; PANAS: positive and negative affect; PSWQ: tendency to worry. | Significant improvement for the UP condition of depressive symp., anxious symp., tendency to worry, emotional dysregulation, and positive and negative affect compared to the control group (Cohen’s d ranged from 0.45 to 2.34). |
| [49] Iran, 2020 | 70 (35 Cont. + 35 Tx.) Age: 35.30 Gender: 61.43% woman 38.57% man | RCT/Group—Outpatient | Multiple sclerosis | GAD, SAD, MDD and PDD | UP: 12 sessions/2 h/1 per week TAU: 12 sessions/2 h/1 per week | DERS: emotional dysregulation; HADS: anxious and depressive symptoms; PANAS: positive and negative affect; PSWQ: tendency to worry. | At post-treatment, significant improvement in the UP condition of depressive symp, anxious symp., positive and negative affect, emotional dysregulation, and tendency to worry compared to the control condition (Cohen’s d ranged from 0.44 to 2.16). Improvements remained at the 3-month follow-up. |
| [45] USA, 2017 | 11 Tx Age: 34.4 Gender: 100% man | Single-condition pilot study/Individual—Outpatient | HIV | Anxious and depressive symp. | 10 sessions/1 per week | CES-D: depressive symptoms; DERS: emotional dysregulation; OASIS: anxious symptoms; ODSIS: depressive symptoms; PSWQ: GAD symptoms; SCS: sexual compulsivity; SIP-DU: frequency of negative consequences of drug use; TLFB: sexual behavior and substance use; YBOCS: obsessive-compulsive symptoms. | Significant reduction with large effect sizes of anxious, depressive, and obsessive-compulsive symptomatology from the baseline to the 3-month follow-up (Cohen’s d ranged from 0.83 to 1.68). Reduced medium effect sizes, albeit not significant, in emotional dysregulation, functional impairment in relation to anxiety, and number of male sexual partners and condomless anal sex (Cohen’s d ranged from 0.49 to 0.61). Reduction in small to medium, but not significant, effect sizes of sexual compulsivity, functional impairment in relation to depression, drug use, and problems with drug use (Cohen’s d ranged from 0.21 to 0.41). |
| [46] USA, 2019 | 9 Tx Age: 61.22 Sex: 55.56% woman 44.44% man | SCED/Individual—Outpatient or the Internet | Idiopathic Parkinson’s disease | AG, GAD, SAD, MDD, PD and PDD | 12 sessions/50–60 min/1 per week | ADIS-V: ED; AS: apathy; BAI: anxious symp.; BDI-II: depressive symp.; CSQ-8: satisfaction with treatment; Telepresence on Videoconference Scale; FES: self-efficacy and worry about falling; GDS: depressive symp.; OASIS: anxious symp.; ODSIS: depressive symp.; STAI: anxious symp. | Statistically significant decrease in anxious and depressive symp. in 7 of the 9 participants at the post- and 6-week follow-up. Significant reduction in fear of falling in two participants (with high scores in the pre-) at post- and follow-up. Significant reduction in apathy in two participants at post- and follow-up, and increase in one participant. High satisfaction with treatment (M CSQ-8 = 30.9). The results did not differ for session modality (online or face-to-face). |
| [43] USA, 2019 | 15 Tx Age: 57 Gender: 100% woman | Single-condition pilot study/Individual—Outpatient and telephone | Breast cancer | Depressive symp. | 4 sessions/2 h (face-to-face) 45 min (telephone)/1 per week with 2 weeks between sessions | ACS: fear of depression; CES-D: depressive symp.; COPE ACCEPTANCE: cancer-related acceptance; COPE AVOID: cancer-related avoidance; DTS: discomfort tolerance; EAC: emotional expression; FFMQ: description of emotions and thoughts and nonjudgment; MEAQ: experiential avoidance; RRQ: rumination; UP CSQ: cognitive skills. | Large effect size on cancer-related acceptance strategy (Cohen’s d = 0.82); medium effect on cancer-related emotional expression (Cohen’s d = 0.65) and smaller effects on cancer-related avoidance (Cohen’s d = 0.32) and depressive symp. (Cohen’s d = 0.42). |
| [50] Sweden, 2017 | 5 Tx Age: 46.40 Gender: 60% woman 40% man | SCED/Individual—Internet + telephone | Chronic pain | AG, GAD, SAD and MDD | 10 sessions/self-applied; approx. 1 module per week | MINI: DSM-V diagnosis; OASIS: anxious symp.; ODSIS: depressive symp.; ÖMPSQ-sv: pain intensity and coping problems. Satisfaction with treatment, treatment completion and compliance, and self-report improvement in strategies trained by PU. | Improvements in anxious and/or depressive symp., in four of the five participants, with medium to large effects, but only significant in two participants. At post-, P3 and P5 continued to meet the criteria for the same ED diagnosis, but P1 and P4 no longer met the criteria for any ED. In pain intensity, increases or no change at post- and 3-month follow up. High satisfaction with treatment. Patients reported improvements in each PU strategy. |
| Reference, Country and Publication Year | Sample (N) | Study Design and Setting | Medical Condition | Emotional Disorder | Length/Session Frequency | Primary Measures | Secondary Measures |
|---|---|---|---|---|---|---|---|
| [52] Spain, 2020 | 60 | SCED/Group—Internet | Obesity | Anxious and/or depressive symp. or at least a diagnosis of ED | UP: 12 sessions/2 h/1 per week | BAI: anxious symp.; BDI-II: depressive symp.; BMI: weight gain or loss; MINI: primary and secondary diagnosis of ED. | PANAS: positive and negative affect; NEO-FFI: extraversion and neuroticism; QLI: quality of life; EuroQol: health-related quality of life; MI: negative impact of health problem and ED in areas of daily life; DERS: emotional dysregulation; BEAQ: experiential avoidance; PHLMS: present awareness and acceptance; ERQ: cognitive reappraisal and expressive suppression; BITE: bulimia symp. and signs and symp. associated with binge eating; BSQ: fear of gaining weight, low self-esteem in relation to appearance, desire to lose weight, and body dissatisfaction; EES: tendency to use food to cope with negative affect; STQ: satisfaction with treatment. |
| [53] USA, 2020 | 40 (20 Tx + 20 Cont.) | RCT/Individual—outpatient | Urinary problems | Anxious symp. or Anxiety disorder | UP (Tx): 12 sessions/45 min./1 x week Supportive ther.: 12 sessions/45 min/1 x week | PROMIS-29 (Anxiety subscale); UDI-6: urinary problems. | Mini-IPIP: big 5 personality traits; PCL-5: trauma history; PGI-I: improvement of urinary symp.; PROMIS-29 (depression, fatigue, pain, physical functioning, sleep disturbances, social roles subscales); RRS: ruminative style. |
| [51] Australia, 2016 | 200 (25 Tx + 25 Cont. + 150 Comparative cohort) | RCT/lndividual—outpatient | Cardiovascular diseases | AG, GAD, SAD, MDD, PDD, PTSD, PD | UP (Tx): 12–18 sessions/1 per week EUC (Cont.): Educational package | GAD-7: GAD symp.; OASIS: anxious symp.; PHQ-9: depressive symp.; and SF-12: quality of life. | AUDIT-C: alcohol use; DASS-21: stress; GATS: tobacco use, CVE; MINI: ED diagnosis; MOS SAS: adherence to treatment. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osma, J.; Martínez-García, L.; Quilez-Orden, A.; Peris-Baquero, Ó. Unified Protocol for the Transdiagnostic Treatment of Emotional Disorders in Medical Conditions: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 5077. https://doi.org/10.3390/ijerph18105077
Osma J, Martínez-García L, Quilez-Orden A, Peris-Baquero Ó. Unified Protocol for the Transdiagnostic Treatment of Emotional Disorders in Medical Conditions: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(10):5077. https://doi.org/10.3390/ijerph18105077
Chicago/Turabian StyleOsma, Jorge, Laura Martínez-García, Alba Quilez-Orden, and Óscar Peris-Baquero. 2021. "Unified Protocol for the Transdiagnostic Treatment of Emotional Disorders in Medical Conditions: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 10: 5077. https://doi.org/10.3390/ijerph18105077
APA StyleOsma, J., Martínez-García, L., Quilez-Orden, A., & Peris-Baquero, Ó. (2021). Unified Protocol for the Transdiagnostic Treatment of Emotional Disorders in Medical Conditions: A Systematic Review. International Journal of Environmental Research and Public Health, 18(10), 5077. https://doi.org/10.3390/ijerph18105077