
Scaling up Action Schools! BC: How Does Voltage Drop at Scale Affect Student Level Outcomes? A Cluster Randomized Controlled Trial


Abstract
:1. Introduction
2. Action Schools! BC
3. Materials and Methods
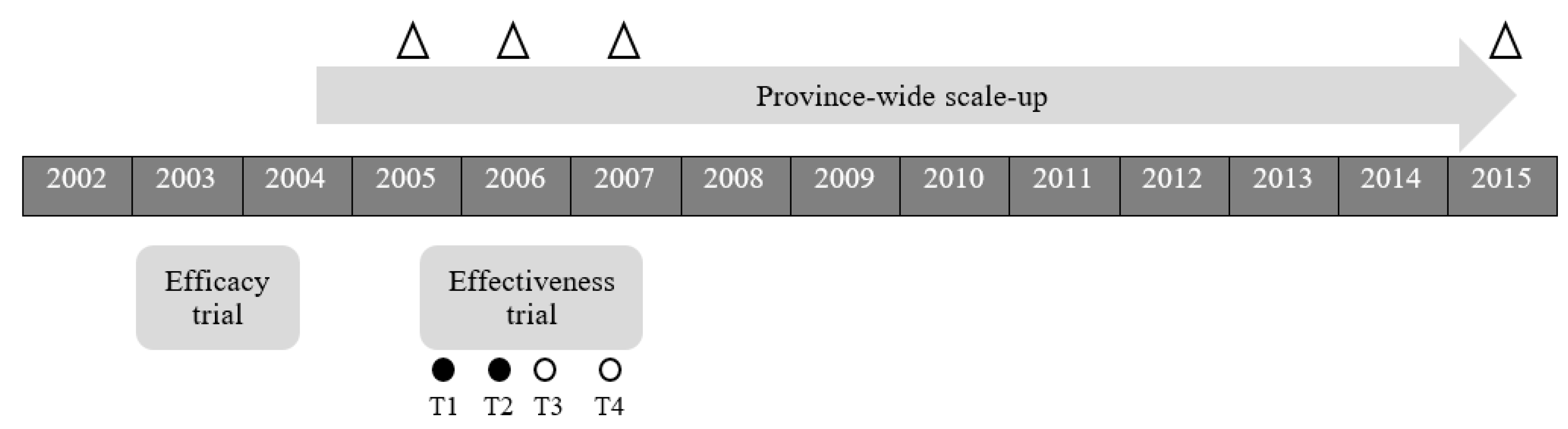
3.1. Objective 1: Implementation Strategies across 11 Years of Province-Wide Scale up (2004–2015)
3.2. Objectives 2 & 3: Randomized Control Effectiveness Trial (2005–2007)
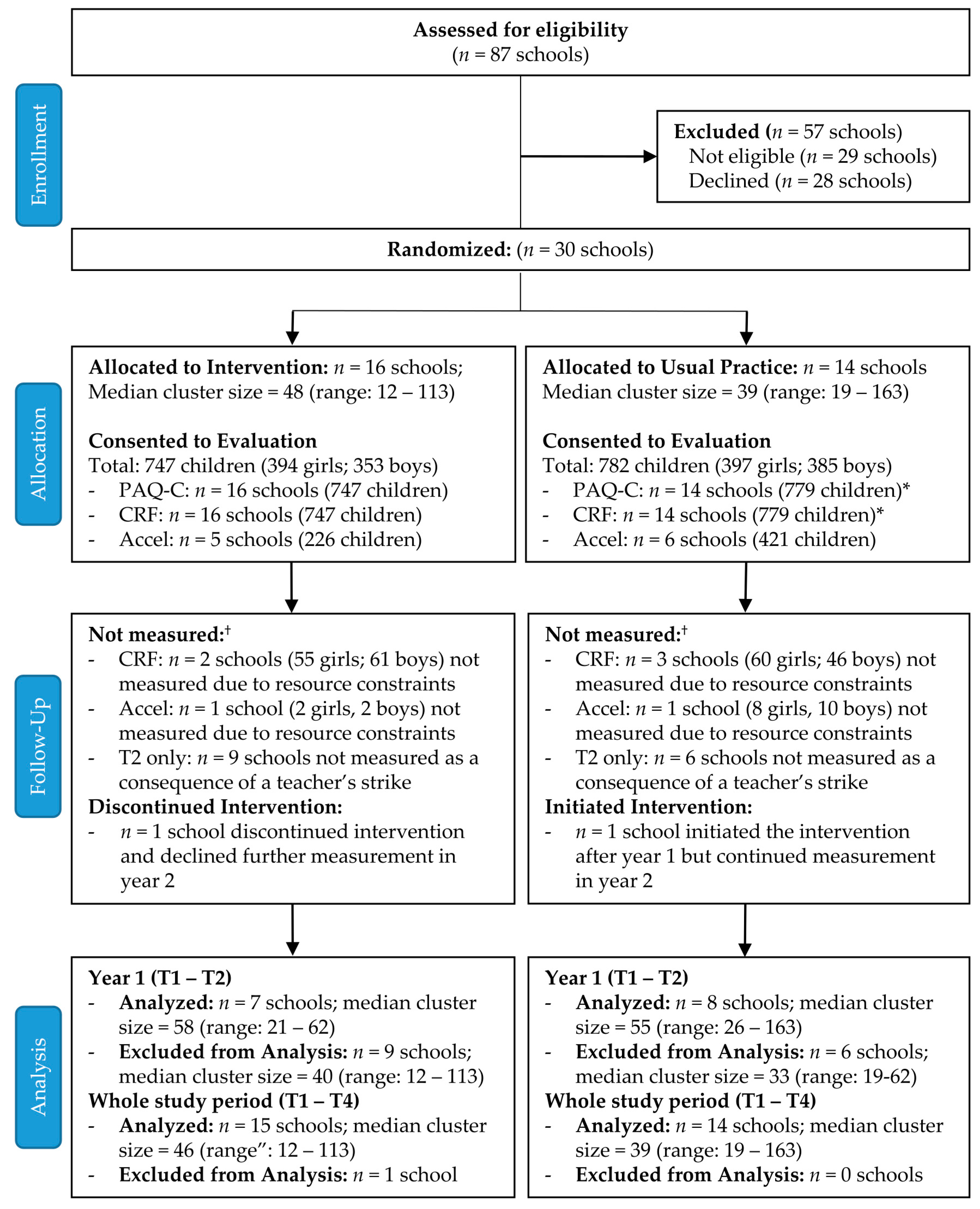
3.2.1. Study Design and Participants
3.2.2. Implementation Measures (Physical Activity Delivery by Teachers)
3.2.3. Impact Measures (Student-Level Outcomes)
3.2.4. Sample Size Calculation
3.3. Statistical Analysis
4. Results
4.1. Objective 1: Implementation Strategies across 11 Years of Province-Wide Scale up (2004–2015)
4.1.1. Implementation Process Strategies
4.1.2. Capacity-Building Strategies
4.1.3. Scale-up Strategies
4.2. Randomized Control Effectiveness Trial (2005–2007)
4.2.1. Participants
4.2.2. Physical Activity Delivery by Teachers
4.2.3. Student’s Physical Activity and Fitness
4.2.4. Link with Implementation
5. Discussion
Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chaput, J.P.; Willumsen, J.; Bull, F.; Chou, R.; Ekelund, U.; Firth, J.; Jago, R.; Ortega, F.B.; Katzmarzyk, P.T. 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5–17 years: Summary of the evidence. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 141. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjostrom, M. Physical fitness in childhood and adolescence: a powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Steele, R.M.; Brage, S.; Corder, K.; Wareham, N.J.; Ekelund, U. Physical activity, cardiorespiratory fitness, and the metabolic syndrome in youth. J. Appl. Physiol. 2008, 105, 342–351. [Google Scholar] [CrossRef] [Green Version]
- Colley, R.C.; Carson, V.; Garriguet, D.; Janssen, I.; Roberts, K.C.; Tremblay, M.S. Physical activity of Canadian children and youth, 2007 to 2015. Health Rep. 2017, 28, 8–16. [Google Scholar] [PubMed]
- Cameron, C.; Craig, C.L.; Bauman, A.; Tudor-Locke, C. CANPLAY study: Secular trends in steps/day amongst 5-19 year-old Canadians between 2005 and 2014. Prev. Med. 2016, 86, 28–33. [Google Scholar] [CrossRef]
- Knuth, A.G.; Hallal, P.C. Temporal trends in physical activity: a systematic review. J. Phys. Act. Health 2009, 6, 548–559. [Google Scholar] [CrossRef]
- Tomkinson, G.R.; Lang, J.J.; Tremblay, M.S. Temporal trends in the cardiorespiratory fitness of children and adolescents representing 19 high-income and upper middle-income countries between 1981 and 2014. Br. J. Sports Med. 2019, 53, 478–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, C.L.; Shields, M.; Leblanc, A.G.; Tremblay, M.S. Trends in aerobic fitness among Canadians, 1981 to 2007–2009. Appl. Physiol. Nutr. Metab. 2012, 37, 511–519. [Google Scholar] [CrossRef]
- Jones, R.A.; Hinkley, T.; Okely, A.D.; Salmon, J. Tracking physical activity and sedentary behavior in childhood: a systematic review. Am. J. Prev. Med. 2013, 44, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Janz, K.F.; Dawson, J.D.; Mahoney, L.T. Tracking physical fitness and physical activity from childhood to adolescence: the muscatine study. Med. Sci. Sports Exerc. 2000, 32, 1250–1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, L.B.; Hasselstrom, H.; Gronfeldt, V.; Hansen, S.E.; Karsten, F. The relationship between physical fitness and clustered risk, and tracking of clustered risk from adolescence to young adulthood: eight years follow-up in the Danish Youth and Sport Study. Int. J. Behav. Nutr. Phys. Act. 2004, 1, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Telama, R.; Yang, X.; Leskinen, E.; Kankaanpaa, A.; Hirvensalo, M.; Tammelin, T.; Viikari, J.S.; Raitakari, O.T. Tracking of physical activity from early childhood through youth into adulthood. Med. Sci. Sports Exerc. 2014, 46, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Hogstrom, G.; Nordstrom, A.; Nordstrom, P. Aerobic fitness in late adolescence and the risk of early death: a prospective cohort study of 1.3 million Swedish men. Int. J. Epidemiol. 2016, 45, 1159–1168. [Google Scholar] [CrossRef] [Green Version]
- Hogstrom, G.; Nordstrom, A.; Nordstrom, P. High aerobic fitness in late adolescence is associated with a reduced risk of myocardial infarction later in life: a nationwide cohort study in men. Eur. Heart J. 2014, 35, 3133–3140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hogstrom, G.; Ohlsson, H.; Crump, C.; Sundquist, J.; Sundquist, K. Aerobic fitness in late adolescence and the risk of cancer and cancer-associated mortality in adulthood: A prospective nationwide study of 1.2 million Swedish men. Cancer Epidemiol. 2019, 59, 58–63. [Google Scholar] [CrossRef]
- Naylor, P.J.; McKay, H.A. Prevention in the first place: schools a setting for action on physical inactivity. Br. J. Sports Med. 2009, 43, 10–13. [Google Scholar] [CrossRef]
- International Society for Physical Activity and Health (ISPAH). Eight Investments that Work for Physical Activity. 2020. Available online: www.ISPAH.org/Resources (accessed on 30 November 2020).
- Fox, K.R.; Cooper, A.; McKenna, J. The School and Promotion of Children’s Health-Enhancing Physical Activity: Perspectives from the United Kingdom. J. Teach Phys. Educ. 2004, 23, 338–358. [Google Scholar] [CrossRef]
- Reis, R.S.; Salvo, D.; Ogilvie, D.; Lambert, E.V.; Goenka, S.; Brownson, R.C. Scaling up physical activity interventions worldwide: stepping up to larger and smarter approaches to get people moving. Lancet 2016, 388, 1337–1348. [Google Scholar] [CrossRef] [Green Version]
- Naylor, P.J.; Nettlefold, L.; Race, D.; Hoy, C.; Ashe, M.C.; Higgins, J.W.; McKay, H. Implementation of school based physical activity interventions: A systematic review. Prev. Med. 2015, 72, 95–115. [Google Scholar] [CrossRef]
- Cassar, S.; Salmon, J.; Timperio, A.; Naylor, P.J.; van Nassau, F.; Contardo Ayala, A.M.; Koorts, H. Adoption, implementation and sustainability of school-based physical activity and sedentary behaviour interventions in real-world settings: a systematic review. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 120. [Google Scholar] [CrossRef] [Green Version]
- Love, R.; Adams, J.; van Sluijs, E.M.F. Are school-based physical activity interventions effective and equitable? A meta-analysis of cluster randomized controlled trials with accelerometer-assessed activity. Obes. Rev. 2019, 20, 859–870. [Google Scholar] [CrossRef]
- Durlak, J.A.; DuPre, E.P. Implementation matters: a review of research on the influence of implementation on program outcomes and the factors affecting implementation. Am. J. Community Psychol. 2008, 41, 327–350. [Google Scholar] [CrossRef] [PubMed]
- Lane, C.; McCrabb, S.; Nathan, N.; Naylor, P.J.; Bauman, A.; Milat, A.; Lum, M.; Sutherland, R.; Byaruhanga, J.; Wolfenden, L. How effective are physical activity interventions when they are scaled-up: a systematic review. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 16. [Google Scholar] [CrossRef]
- Herlitz, L.; MacIntyre, H.; Osborn, T.; Bonell, C. The sustainability of public health interventions in schools: a systematic review. Implement. Sci. 2020, 15, 4. [Google Scholar] [CrossRef]
- Milat, A.J.; King, L.; Newson, R.; Wolfenden, L.; Rissel, C.; Bauman, A.; Redman, S. Increasing the scale and adoption of population health interventions: experiences and perspectives of policy makers, practitioners, and researchers. Health Res. Policy Syst. 2014, 12, 18. [Google Scholar] [CrossRef] [Green Version]
- Naylor, P.J.; Macdonald, H.; Reed, K.E.; McKay, H. Action Schools! BC: A Socioecological Approach to Modifying Chronic Disease Risk Factors in Elementary School Children. Prev. Chronic Dis. 2006, 3, A60. [Google Scholar]
- Naylor, P.J.; Macdonald, H.M.; Zebedee, J.A.; Reed, K.E.; McKay, H.A. Lessons learned from Action Schools! BC--an ‘active school’ model to promote physical activity in elementary schools. J. Sci. Med. Sport 2006, 9, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Naylor, P.J.; Macdonald, H.M.; Warburton, D.E.; Reed, K.E.; McKay, H.A. An active school model to promote physical activity in elementary schools: Action Schools! BC. Br. J. Sports Med. 2008, 42, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Reed, K.E.; Warburton, D.E.R.; Macdonald, H.M.; Naylor, P.J.; McKay, H.A. Action Schools! BC: A school-based physical activity intervention designed to decrease cardiovascular disease risk factors in children. Prev. Med. 2008, 46, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, H.M.; Kontulainen, S.A.; Petit, M.A.; Beck, T.J.; Khan, K.M.; McKay, H.A. Does a novel school-based physical activity model benefit femoral neck bone strength in pre- and early pubertal children? Osteoporos. Int. 2008, 19, 1445–1456. [Google Scholar] [CrossRef] [PubMed]
- Ahamed, Y.; Macdonald, H.; Reed, K.; Naylor, P.J.; Liu-Ambrose, T.; McKay, H. School-based physical activity does not compromise children’s academic performance. Med. Sci. Sports Exerc. 2007, 39, 371–376. [Google Scholar] [CrossRef]
- Indig, D.; Lee, K.; Grunseit, A.; Milat, A.; Bauman, A. Pathways for scaling up public health interventions. BMC Public Health 2018, 18, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKay, H.A.; Macdonald, H.M.; Nettlefold, L.; Masse, L.C.; Day, M.; Naylor, P.J. Action Schools! BC implementation: from efficacy to effectiveness to scale-up. Br. J. Sports Med. 2015, 49, 210–218. [Google Scholar] [CrossRef] [Green Version]
- Powell, B.J.; Fernandez, M.E.; Williams, N.J.; Aarons, G.A.; Beidas, R.S.; Lewis, C.C.; McHugh, S.M.; Weiner, B.J. Enhancing the Impact of Implementation Strategies in Healthcare: A Research Agenda. Front. Public Health 2019, 7, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wandersman, A.; Duffy, J.; Flaspohler, P.; Noonan, R.; Lubell, K.; Stillman, L.; Blachman, M.; Dunville, R.; Saul, J. Bridging the gap between prevention research and practice: The interactive systems framework for dissemination and implementation. Am. J. Community Psychol. 2008, 41, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Simmons, R.; Shiffman, J. Chapter 1: Scaling up health service innovations: a framework for action. In Scaling up Health Service Delivery: From Pilot Innovations to Policies and Programmes; Simmons, R., Fajans, P., Ghiron, L., Eds.; World Health Organization: Geneva, Switzerland, 2007; pp. 1–30. [Google Scholar]
- Day, M.E.; Strange, K.S.; McKay, H.A.; Naylor, P.J. Action schools! BC--Healthy Eating: effects of a whole-school model to modifying eating behaviours of elementary school children. Can. J. Public Health 2008, 99, 328–331. [Google Scholar] [CrossRef]
- Powell, B.J.; Waltz, T.J.; Chinman, M.J.; Damschroder, L.J.; Smith, J.L.; Matthieu, M.M.; Proctor, E.K.; Kirchner, J.E. A refined compilation of implementation strategies: results from the Expert Recommendations for Implementing Change (ERIC) project. Implement. Sci. 2015, 10, 21. [Google Scholar] [CrossRef] [Green Version]
- Leeman, J.; Birken, S.A.; Powell, B.J.; Rohweder, C.; Shea, C.M. Beyond "implementation strategies": classifying the full range of strategies used in implementation science and practice. Implement. Sci. 2017, 12, 125. [Google Scholar] [CrossRef]
- Proctor, E.K.; Powell, B.J.; McMillen, J.C. Implementation strategies: recommendations for specifying and reporting. Implement. Sci. 2013, 8, 139. [Google Scholar] [CrossRef] [Green Version]
- Curran, G.M.; Bauer, M.; Mittman, B.; Pyne, J.M.; Stetler, C. Effectiveness-implementation hybrid designs: combining elements of clinical effectiveness and implementation research to enhance public health impact. Med. Care 2012, 50, 217–226. [Google Scholar] [CrossRef] [Green Version]
- Crocker, P.R.; Bailey, D.A.; Faulkner, R.A.; Kowalski, K.C.; McGrath, R. Measuring general levels of physical activity: preliminary evidence for the Physical Activity Questionnaire for Older Children. Med. Sci. Sports Exerc. 1977, 29, 1344–1349. [Google Scholar] [CrossRef] [PubMed]
- Mackelvie, K.J.; McKay, H.A.; Khan, K.M.; Crocker, P.R. A school-based exercise intervention augments bone mineral accrual in early pubertal girls. J. Pediatr. 2001, 139, 501–508. [Google Scholar] [CrossRef]
- Trost, S.G.; Loprinzi, P.D.; Moore, R.; Pfeiffer, K.A. Comparison of accelerometer cut points for predicting activity intensity in youth. Med. Sci. Sports Exerc. 2011, 43, 1360–1368. [Google Scholar] [CrossRef]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Leger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef]
- Olds, T.; Tomkinson, G.; Leger, L.; Cazorla, G. Worldwide variation in the performance of children and adolescents: an analysis of 109 studies of the 20-m shuttle run test in 37 countries. J. Sports Sci. 2006, 24, 1025–1038. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.A.; McKay, H.A.; Macdonald, H.; Nettlefold, L.; Baxter-Jones, A.D.; Cameron, N.; Brasher, P.M. Enhancing a Somatic Maturity Prediction Model. Med. Sci. Sports Exerc. 2015, 47, 1755–1764. [Google Scholar] [CrossRef]
- Ip, F. Ethnicity and Visible Minority Characteristics of BC’s Population. 2006 Census Fast Facts. 2006-12; BC Stats: Victoria, BC, Canada, 2008. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Linden, A. ESIZEREG: Stata Module for Computing the Effect Size Based on a Linear Regression Coefficient; Boston College Department of Economics: Chestnut Hill, MA, USA, 2019. [Google Scholar]
- Sullivan, G.M.; Feinn, R. Using Effect Size-or Why the P Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef] [Green Version]
- Global Advocacy for Physical Activity (GAPA); The Advocacy Council of the International Society for Physical Activity and Health (ISPAH). NCD Prevention: Investments that work for physical activity. Br. J. Sports Med.
- Keshavarz, N.; Nutbeam, D.; Rowling, L.; Khavarpour, F. Schools as social complex adaptive systems: A new way to understand the challenges of introducing the health promoting schools concept. Soc. Sci. Med. 2010, 70, 1467–1474. [Google Scholar] [CrossRef]
- Lee, K.; van Nassau, F.; Grunseit, A.; Conte, K.; Milat, A.; Wolfenden, L.; Bauman, A. Scaling up population health interventions from decision to sustainability - a window of opportunity? A qualitative view from policy-makers. Health Res. Policy Syst. 2020, 18, 118. [Google Scholar] [CrossRef]
- Neely, K.C.; Montemurro, G.R.; Storey, K.E. A Canadian-wide perspective on the essential conditions for taking a comprehensive school health approach. BMC Public Health 2020, 20, 1907. [Google Scholar] [CrossRef] [PubMed]
- Flaspohler, P.; Duffy, J.; Wandersman, A.; Stillman, L.; Maras, M.A. Unpacking prevention capacity: an intersection of research-to-practice models and community-centered models. Am. J. Community Psychol. 2008, 41, 182–196. [Google Scholar] [CrossRef]
- Leeman, J.; Calancie, L.; Hartman, M.A.; Escoffery, C.T.; Herrmann, A.K.; Tague, L.E.; Moore, A.A.; Wilson, K.M.; Schreiner, M.; Samuel-Hodge, C. What strategies are used to build practitioners’ capacity to implement community-based interventions and are they effective? A systematic review. Implement. Sci. 2015, 10, 80. [Google Scholar] [CrossRef] [Green Version]
- Johnson, S.M. Where Teachers Thrive: Organizing Schools for Success; Harvard Education Press: Cambridge, MA, USA, 2019. [Google Scholar]
- Jones, M.; Defever, E.; Letsinger, A.; Steele, J.; Mackintosh, K.A. A mixed-studies systematic review and meta-analysis of school-based interventions to promote physical activity and/or reduce sedentary time in children. J. Sport Health Sci. 2020, 9, 3–17. [Google Scholar] [CrossRef]
- Hartwig, T.B.; Sanders, T.; Vasconcellos, D.; Noetel, M.; Parker, P.D.; Lubans, D.R.; Andrade, S.; Avila-Garcia, M.; Bartholomew, J.; Belton, S. School-based interventions modestly increase physical activity and cardiorespiratory fitness but are least effective for youth who need them most: an individual participant pooled analysis of 20 controlled trials. Br. J. Sports Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Kriemler, S.; Meyer, U.; Martin, E.; van Sluijs, E.M.F.; Andersen, L.B.; Martin, B.W. Effect of school-based interventions on physical activity and fitness in children and adolescents: a review of reviews and systematic update. Br. J. Sports Med. 2011, 45, 923–930. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, N.; Welsman, J.O. Traditional and New Perspectives on Youth Cardiorespiratory Fitness. Med. Sci. Sports Exerc. 2020, 52, 2563–2573. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.N.; Kohl, H.W., 3rd; Barlow, C.E.; Paffenbarger, R.S., Jr.; Gibbons, L.W.; Macera, C.A. Changes in physical fitness and all-cause mortality. A prospective study of healthy and unhealthy men. JAMA 1995, 273, 1093–1098. [Google Scholar] [CrossRef]
- McCrabb, S.; Lane, C.; Hall, A.; Milat, A.; Bauman, A.; Sutherland, R.; Yoong, S.; Wolfenden, L. Scaling-up evidence-based obesity interventions: A systematic review assessing intervention adaptations and effectiveness and quantifying the scale-up penalty. Obes. Rev. 2019, 20, 964–982. [Google Scholar] [CrossRef] [PubMed]
- Welsh, B.C.; Sullivan, C.J.; Olds, D.L. When early crime prevention goes to scale: a new look at the evidence. Prev. Sci. 2010, 11, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Tommeraas, T.; Ogden, T. Is There a Scale-up Penalty? Testing Behavioral Change in the Scaling up of Parent Management Training in Norway. Adm. Policy Ment. Health 2017, 44, 203–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilbourne, A.M.; Neumann, M.S.; Pincus, H.A.; Bauer, M.S.; Stall, R. Implementing evidence-based interventions in health care: application of the replicating effective programs framework. Implement. Sci. 2007, 2, 42. [Google Scholar] [CrossRef] [Green Version]
- Bopp, M.; Saunders, R.P.; Lattimore, D. The tug-of-war: fidelity versus adaptation throughout the health promotion program life cycle. J. Prim. Prev. 2013, 34, 193–207. [Google Scholar] [CrossRef] [PubMed]
- Yamey, G. Scaling up global health interventions: a proposed framework for success. PLoS Med. 2011, 8, e1001049. [Google Scholar] [CrossRef] [Green Version]
- CATCH Global Foundation. How does CATCH work? 2021. Available online: https://catchinfo.org/about/ (accessed on 22 February 2021).
- Kibbe, D.L.; Hackett, J.; Hurley, M.; McFarland, A.; Schubert, K.G.; Schultz, A.; Harris, S. Ten Years of TAKE 10!((R)): Integrating physical activity with academic concepts in elementary school classrooms. Prev. Med. 2011, 52 Suppl 1, S43–S50. [Google Scholar] [CrossRef]
- Wears, R.L. Advanced Statistics: Statistical Methods for Analyzing Cluster and Cluster-randomized Data. Acad. Emerg. Med. 2002, 9, 330–341. [Google Scholar] [CrossRef]
- Williams, R.L. A note on robust variance estimation for cluster correlated data. Biometrics 2000, 56, 645–646. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Component | Description |
|---|---|
| Action Zones | Six areas in which opportunities for physical activity could be provided to students. The six Zones were: (1) School Environment, (2) School Spirit, (3) Physical Education, (4) Extra-curricular, (5) Family and Community and (6) Classroom Action. |
| AS! BC Support Team | A central technical support unit that developed and provided AS! BC resources (training workshops, written materials, Classroom Action Bins, school newsletter inserts for families) and ongoing consultation (on-site and telephone) to administrators, teachers and the School Action Team. |
| AS! BC School Facilitators | Two elementary school teachers seconded by the AS! BC Support Team to provide training, support and advice to the schools and liaise between the Support Team and the School Action Team. |
| School Action Team | A committee of school stakeholders (e.g., interested intermediate grade teachers, administrators, parents, health, sport/recreation practitioners) that created and supported implementation of the Action Plan. |
| Planning Guide for Schools and Teachers | A set of inventories and worksheets that guided teachers and the School Action Team to identify school priorities and create their Action Plan. |
| Action Pages! | A resource directory using curriculum organizers to link teachers, coaches or community instructors with recommended and available resources. |
| Classroom Action Bin | A storage bin for the classroom filled with playground balls, videos, skipping ropes, exercise bands, strength grippers and teaching resources that supported the Action Plan. |
| Strategy | Description | Specification | Alignment with Taxonomy [39] |
|---|---|---|---|
| Implementation Process Strategies: The Support Team worked with schools to support implementation of AS! BC | |||
| 4 Steps to Becoming an Action School | The Support Team worked with schools on the “4 Steps to Becoming an Action School”:
| Actor: AS! BC Support Team Action: Once a school indicated interest the Support Team sent materials (detailed below) to assist the school. Each school completed a needs assessment (see ‘Taking Stock’, in adjacent column) and created an Action Plan that supported the school’s goals and aligned with available resources. The flexibility of the AS! BC model made it adaptable to schools needs and available resources. Schools completed year-end reporting related to progress on the Action Plan. Action plans and annual reports were received and reviewed by the Support Team. Target: Participating schools Temporality: Needs assessment and action planning were done after registration. Reporting occurred annually at the end of the school year. | Provide ongoing consultation Provide local technical assistance Conduct local needs assessment Assess for readiness and identify barriers and facilitators Promote adaptability |
| Teacher on Call Provincial release time | The BC Government provided funding for a Teacher On Call to allow at least one teacher per intervention school to attend an AS! BC workshop, or participate in another activity to support implementation of AS! BC at their school. | Actor: AS! BC Support Team Action: Release time Target: Participating schools/teachers Temporality: Once after registration and again as new training opportunities were offered (e.g., as AS! BC expanded to include Healthy Eating, release time was available to schools again) | Access funding |
| AS! BC Classroom Action Bin | Participating schools received a Classroom Action Bin (1/grade). Bins included equipment and best-practice resources teachers could use to support their Action Plan (e.g., playground balls, DVDs/videos, skipping ropes, posters promoting movement). | Actor: AS! BC Support Team Action: The Support Team provided Classroom Action Bins to support schools implementing AS! BC. Target: Classroom teachers Temporality: Resources were available on the website. The Support Team regularly updated materials based on feedback from participating schools, administrators and teachers. Action bins were provided (1/grade) once schools created an action plan. | Provide equipment |
| AS! BC support and communication materials | The Support Team developed materials to help schools promote healthy living (including PA and healthy eating) within the school community. Key resources included: AS! BC planning guide (‘how to’ manual that guided schools and teachers through the steps to become an ‘Action School’); Classroom Action resource (support delivery of Classroom Action—additional 15 min PA/day); Introduction to Classroom Action Zone DVD (1/school); Action Pages! (Nationwide inventory of PA, PE and healthy eating resources); AS! BC playground circuits (customized for schools and made available on the website); Weekly activity logs to track PA delivered to students; E-news delivered to administrators and teachers; Success stories shared on website and through outreach channels. | Actor: AS! BC Support Team Action: The Support Team developed, updated (e.g., revisions, new materials) and distributed support and communication materials to support schools implementing AS! BC. Target: Schools and teachers Temporality: Resources were available on the website. The Support Team regularly updated materials based on feedback from participating schools, administrators and teachers. E-news was delivered monthly. | Provide equipment Develop and distribute educational materials Obtain and use feedback Capture and share local knowledge |
| Branded incentives | Additional resources and equipment to support PA and healthy eating in the school. | Actor: AS! BC Support Team Action: The Support Team offered incentives to schools to encourage them to complete annual reports. Target: Participating schools Temporality: Annually to support reporting and also periodically throughout the year | Provide incentives |
| Advisory committees | The provincial advisory committee had community, school and government representatives. The school advisory committee had teacher and principal representatives | Actor: Principal investigators and AS! BC Support Team Action: After receipt of funding, the committees were formed to provide input on design and implementation of AS! BC Target: Key stakeholders Temporality: Advisory groups met regularly throughout delivery | Use advisory boards and workgroups Create an implementation blueprint |
| Teacher Mentorship | Additional support for schools and teachers | Actor: AS! BC Support Team Action: Trainers were available to provide additional support including classroom visits, action planning, planning for healthy eating, organizing equipment and resources, etc. Target: Participating schools and teachers Temporality: As requested throughout delivery | Provide ongoing consultation |
| Capacity-building Strategies: involve the management and implementation of a process to deliver AS! BC workshops, build capacity across the province, and maintain interest and momentum within registered schools. | |||
| AS! BC workshops and ongoing support | Training workshops were coordinated by the Support Team and delivered by the Support Team, Master or Regional Trainers. Ongoing support (via email, phone) was available as needed. | Actor: AS! BC Support Team Action: The Support Team worked with schools to secure a date for workshops. Classroom Action Training workshops were 3 h long. Refresher training workshops were 1 h long. Training was delivered face-to-face to groups of teachers in schools (gymnasia, multi-purpose rooms, empty classrooms) and followed principles of experiential learning and self-efficacy theory. Training workshops included positive modelling, verbal persuasion and opportunities for teachers to be successful and recognized. The Support Team and Trainers provided ongoing support during the school year via email and telephone, and over time teachers/schools could register for a selection of additional in-person workshops throughout the year (e.g., student playground leadership). Workshop participants completed evaluation forms, which were returned to the Support Team and used to improve future workshops. Target: Participating teachers and schools Temporality: Ongoing throughout the year | Conduct ongoing training Make training dynamic Obtain and use feedback |
| AS! BC Master and Regional Trainers | The Support Team used a network of Master Trainers and Regional Trainers to deliver workshops across the province. Regional trainers self-identified as interested and submitted a resume. If accepted, they participated in training during a Summer Institute, offered annually. | Actor: AS! BC Support Team Action: The network of Master and Regional Trainers supported the delivery of workshops province-wide. Target: Participating teachers and schools Temporality: Ongoing throughout the year | Identify and prepare champions Train the trainer |
| Summer Institute | The Summer Institute served as a training opportunity for Master and Regional trainers. | Actor: AS! BC Support Team Action: Individuals selected as Master or Regional Trainers attended the Summer Institute led by the Support Team. The Summer Institute used a train the trainer approach to build training capacity across the province. Target: Future Master and Regional trainers Temporality: The Summer Institute was 2 days in duration held in August prior to the start of the school academic year. | Identify and prepare champions Make training dynamic Train the trainer |
| Regional Trainer Support Materials | A number of resources supported the Master and Regional trainers. Key resources included: Regional Trainer Guides (workshop templates, presentation tips, checklists, evaluation forms and handouts for schools); Regional Trainer bags (teaching resources and equipment for leading workshops); AS! BC branded materials (e.g., clothing, clipboard, water bottle, pens); E-news | Actor: AS! BC Support Team Action: The Support Team provided Master and Regional Trainers with materials to support workshop delivery around the province Target: AS! BC Master and Regional Trainers Temporality: Master and Regional Trainers received support materials prior to delivering workshops. E-news was delivered monthly. | Provide equipment |
| AS! BC website | The AS! BC website was updated regularly with registration numbers and contained resources for teachers and schools including: playground circuits, and the latest versions of all support materials and teaching resources. | Actor: AS! BC Support Team Action: The Support Team kept the website up to date with the latest registration data (by school district and school) and resources. Target: Teachers, schools, communities Temporality: Updates and additions to website were ongoing | Develop and distribute educational materials |
| Scale-up Strategies: The AS! BC Support Team used a comprehensive marketing and promotion strategy to achieve full school district representation and strategically inform community stakeholders to increase support and build sustainable, far-reaching networks for the initiative. | |||
| Build partnerships | To build partnerships with schools and stakeholders the Support Team participated in a number of events. This was an opportunity to promote AS! BC, network with relevant stakeholders. Stakeholders spanned the following sectors: government (e.g., ministries of health, education), education (e.g., teachers’ associations, parent advisory council, universities), health (e.g., health authorities, regional health units), sport (e.g., sport associations, parks and recreation) and community (e.g., neighbourhood houses, youth organizations). | Actor: AS! BC Support Team Action: Coordinated and/or delivered presentations, displays or promotional materials at events to support networking, relationship building, and ongoing collaboration with key stakeholders Target: Community and provincial organizations within BC, across Canada, and internationally Temporality: Ongoing during scale-up | Promote network weaving Work with educational institutions |
| Recruitment strategies | A range of marketing and promotion strategies were used to recruit teachers, school administrators and other members of the school community to be involved with AS! BC. | Actor: AS! BC Support Team Action: Prepared and shared one-pagers, rack cards, brochures, promotional posters, AS! BC displays, media profiles, mailouts to schools and managed the AS! BC website. The Support Team responded to requests for information (from website) and used targeted approaches (e.g., contacting schools directly) to engage schools. Target: Teachers, school administrators and other members of the school community Temporality: Mail-outs occurred twice a year (Sept, Jan). Other activities as needed and ongoing during scale-up. | Develop and distribute educational materials Increase demand |
| Promotional Strategies | The Support Team used a variety of promotional strategies to inform schools and community stakeholders about AS! BC. | Actor: AS! BC Support Team Action: The Support team made presentations to principals and administrators at school district meetings, and to teachers at school staff meetings. At these meetings, the Support Team provided an overview of AS! BC including requirements and benefits of enrolling. Other promotional strategies included maintaining an AS! BC website and semi-annual mailouts to all BC elementary and middle schools. Target: Principals, administrators, teachers, schools Temporality: Ongoing during scale-up | Conduct educational meetings Increase demand |
| Girls | Boys | |||||||
|---|---|---|---|---|---|---|---|---|
| Total (n = 694) | UP (n = 340) | INT (n = 354) | Difference (95% CI) | Total (n = 660) | UP (n = 336) | INT (n = 324) | Difference (95% CI) | |
| Age (years) | 9.9 (0.6) | 9.9 (0.6) | 9.9 (0.6) | 0.05 (−0.03, 0.1) | 9.9 (0.6) | 10.0 (0.6) | 9.9 (0.6) | 0.1 (0.03, 0.2) |
| BMI (kg/m2) | 18.2 (3.3) | 18.3 (3.2) | 18.1 (3.5) | 0.2 (−0.3, 0.7) | 18.8 (3.7) † | 18.8 (3.8) | 18.9 (3.6) | −0.2 (−0.7, 0.4) |
| Maturity offset (years from APHV) | −1.8 (0.6) | −1.8 (0.6) | −1.9 (0.5) | 0.05 (−0.03, 0.1) | −2.9 (0.5) † | −2.9 (0.5) | −3.0 (0.5) | −0.8 (0.004, 0.1) |
| Ethnicity, # Asian/white/other (% Asian/white/other) | 165/394/135 (24/57/19) | 110/163/67 (32/48/20) | 55/231/68 (16/65/19) | - | 173/386/101 (26/58/15) | 119/165/52 (35/49/15) | 54/221/49 (17/68/15) | - |
| PA score (range 1–5) | 3.0 (0.6) n = 631 | 3.0 (0.6) n = 328 | 3.1 (0.6) n = 303 | −0.1 (−0.2, 0.02) | 3.3 (0.7) † n = 605 | 3.2 (0.6) n = 326 | 3.3 (0.7) n = 279 | −0.1 (−0.2, 0.03) |
| MVPAPAQ (min/day) | 101.1 (92.7) n = 631 | 91.4 (81.3) n = 328 | 111.5 (102.8) n = 303 | −20.1 (−34.7, −5.5) | 131.8 (112.1) † n = 605 | 120.8 (101.9) n = 326 | 144.6 (121.8) n = 279 | −23.8 (−41.9, −5.6) |
| Cardiorespiratory fitness (laps) | 22.6 (11.3) n = 571 | 23.4 (12.0) n = 275 | 21.9 (10.5) n = 296 | 1.4 (−0.4, 3.3) | 26.6 (14.6) † n = 548 | 28.9 (15.2) n = 286 | 24.1 (13.5) n = 262 | 4.8 (2.4, 7.2) |
| Cardiorespiratory fitness (z-score) | −0.1 (0.8) n = 571 | −0.1 (0.8) n = 275 | −0.1 (0.7) n = 296 | 0.1 (−0.04, 0.2) | −0.3 (0.8) † n = 548 | −0.2 (0.8) n = 286 | −0.4 (0.7) n = 262 | 0.2 (0.1, 0.3) |
| Accelerometry | n = 203 | n = 114 | n = 89 | n = 191 | n = 117 | n = 74 | ||
| Total PA (counts/min) | 439.4 (126.1) | 414.6 (111.7) | 471.2 (136.7) | −56.6 (−91.9, −21.4) | 502.4 (134.6)† | 513.5 (133.9) | 484.9 (134.7) | 28.5 (−10.9, 68.0) |
| MVPAAccel (min/day) | 42.3 (17.0) | 38.6 (14.8) | 47.2 (18.5) | −8.6 (−13.4, −3.9) | 54.3 (20.1) † | 55.6 (20.3) | 52.2 (19.8) | 3.3 (−2..5, 9.2) |
| 60 min MVPA/day, # (%) meeting/not meeting | 30/173 (15/85) | 9/105 (8/92) | 21/68 (24/76) | 16% (−6, −26) | 66/125 † (35/65) | 44/73 (38/62) | 22/52 (30/70) | −8% (−22, 6) |
| UP | INT | Difference (INT−UP) | p-Value | |
|---|---|---|---|---|
| Year 1 (n = 86) | 104.9 (89.2, 120.5) | 138.7 (124.5, 152.9) | 33.8 (12.7, 54.9) | <0.01 |
| Year 2 (n = 79) | 110.5 (95.9, 125.1) | 124.4 (111.7, 137.1) | 13.9 (−5.5, 33.3) | 0.2 |
| Difference (Year 2−Year 1) | 5.6 (−10.1, 21.3) p = 0.5 | −14.2 (−29.5, 1.1) p = 0.07 |
| Girls | Boys | |||||||
|---|---|---|---|---|---|---|---|---|
| UP | INT | Adjusted Difference (INT-UP) * | ES | UP | INT | Adjusted Difference (INT-UP) * | ES | |
| PA Score | ||||||||
| T2 | 3.1 (0.6) n = 214 | 3.2 (0.6) n = 126 | 0.05 (−0.1, 0.2) | 0.08 | 3.5 (0.6) n = 207 | 3.3 (0.6) n = 99 | −0.1 (−0.2, −0.03) | −0.16 |
| T4 | 3.0 (0.6) n = 256 | 3.1 (0.6) n = 236 | 0.02 (−0.1, 0.2) | 0.03 | 3.4 (0.6) n = 263 | 3.3 (0.6) n = 193 | −0.1 (−0.3, 0.02) | −0.23 |
| MVPAPAQ (min/day) | ||||||||
| T2 | 103.1 (87.7) n = 214 | 124.6 (101.3) n = 126 | 4.8 (−21.5, 31.2) | 0.05 | 150.5 (100.4) n = 207 | 141.8 (101.3) n = 99 | −10.8 (−35.4, 13.7) | −0.1 |
| T4 | 77.7 (51.8) n = 256 | 96.9 (72.4) n = 236 | 10.9 (−3.8, 25.6) | 0.17 | 108.1 (67.1) n = 263 | 115.2 (77.9) n = 193 | 2.2 (−16.6, 21.1) | 0.04 |
| Total PA (counts/min) | ||||||||
| T2 | 498.2 (181.0) n = 84 | 566.7 (248.3) n = 67 | 1.2 (−73.0, 75.4) | 0.01 | 615.1 (191.9) n = 77 | 588.5 (275.8) n = 55 | 11.1 (−152.4, 174.5) | 0.05 |
| T4 | 471.5 (174.3) n = 77 | 500.7 (185.3) n = 56 | −38.1 (−108.6, 32.3) | −0.2 | 567.4 (190.3) n = 76 | 535.6 (169.8) n = 44 | −6.9 (−109.1, 95.3) | −0.04 |
| MVPAAccel (min/day) | ||||||||
| T2 | 47.3 (19.4) n = 84 | 56.2 (23.1) n = 67 | −0.05 (−6.1, 6.0) | 0.0 | 70.2 (26.0) n = 77 | 60.2 (26.1) n = 55 | −4.2 (−18.7, 10.3) | −0.16 |
| T4 | 46.0 (18.5) n = 77 | 51.9 (22.0) n = 56 | −1.9 (−8.5, 4.7) | −0.1 | 64.9 (25.6) n = 76 | 59.8 (23.6) n = 44 | −1.5 (−17.3, 14.4) | −0.06 |
| CRF (# laps) | ||||||||
| T2 | 27.4 (13.6) n = 183 | 33.8 (18.8) n = 98 | 7.5 (−0.5, 15.5) | 0.48 | 33.8 (16.8) n = 172 | 35.4 (17.6) n = 92 | 4.7 (−1.2, 10.6) | 0.28 |
| T4 | 30.4 (14.2) n = 215 | 28.8 (14.1) n = 221 | −0.8 (−5.8, 4.1) | −0.06 | 38.3 (18.0) n = 226 | 34.2 (16.2) n = 180 | 0.5 (−3.9, 5.0) | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nettlefold, L.; Naylor, P.-J.; Macdonald, H.M.; McKay, H.A. Scaling up Action Schools! BC: How Does Voltage Drop at Scale Affect Student Level Outcomes? A Cluster Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 5182. https://doi.org/10.3390/ijerph18105182
Nettlefold L, Naylor P-J, Macdonald HM, McKay HA. Scaling up Action Schools! BC: How Does Voltage Drop at Scale Affect Student Level Outcomes? A Cluster Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(10):5182. https://doi.org/10.3390/ijerph18105182
Chicago/Turabian StyleNettlefold, Lindsay, Patti-Jean Naylor, Heather M. Macdonald, and Heather A. McKay. 2021. "Scaling up Action Schools! BC: How Does Voltage Drop at Scale Affect Student Level Outcomes? A Cluster Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 10: 5182. https://doi.org/10.3390/ijerph18105182
APA StyleNettlefold, L., Naylor, P. -J., Macdonald, H. M., & McKay, H. A. (2021). Scaling up Action Schools! BC: How Does Voltage Drop at Scale Affect Student Level Outcomes? A Cluster Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 18(10), 5182. https://doi.org/10.3390/ijerph18105182