Knowledge, Attitude, and Practice (KAP) toward the Novel Coronavirus (COVID-19) Pandemic in a Saudi Population-Based Survey

 , , ,
, , ,
Abstract
:1. Introduction
2. Methodology
2.1. Study Design and Setting
2.2. Study Population and Sample
2.3. Data Collection Tool
2.4. Response Rate
2.5. Study Procedure
2.6. Data Management and Analysis
2.7. Ethical Considerations
3. Results
3.1. Demographic Findings
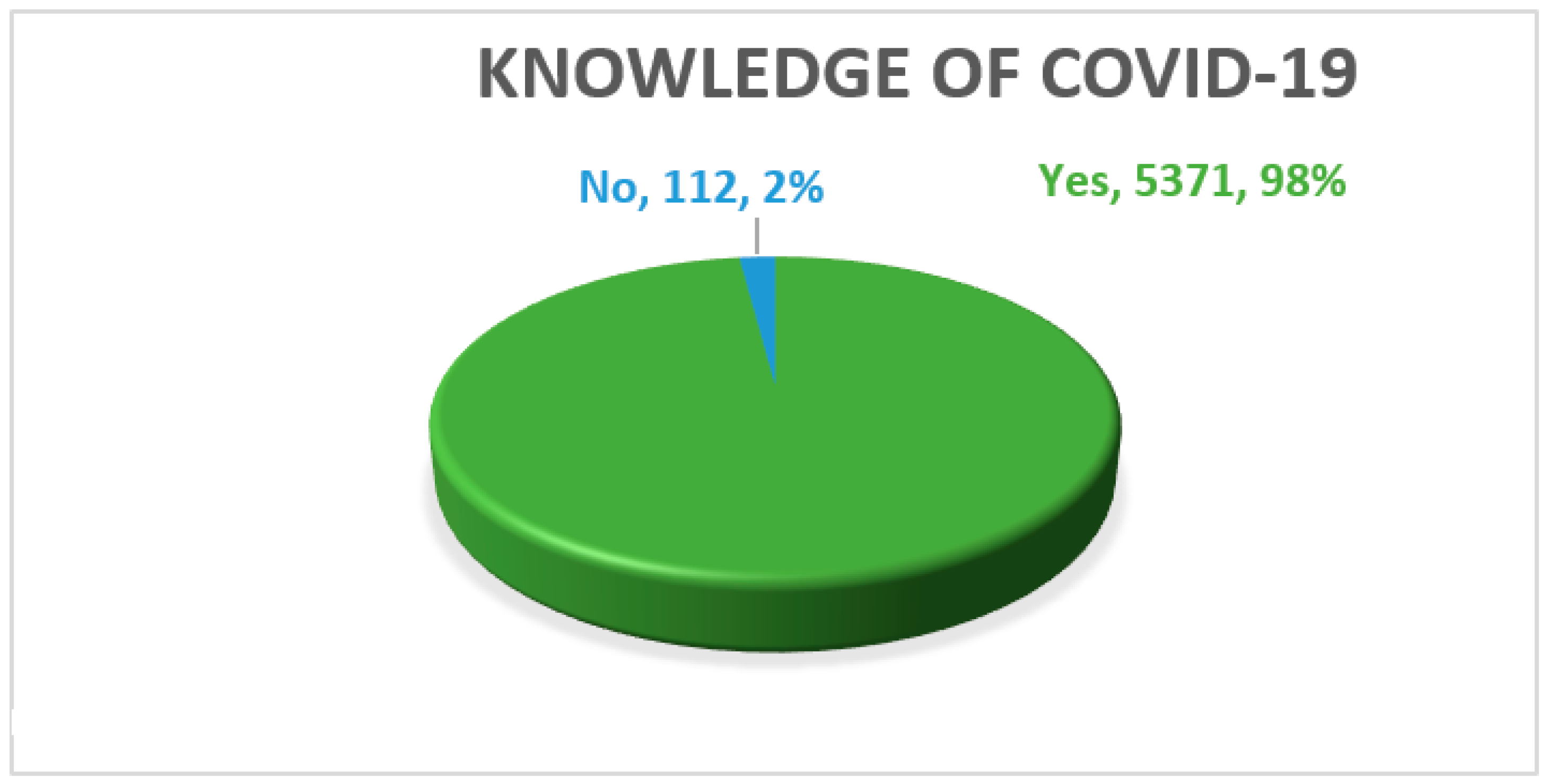
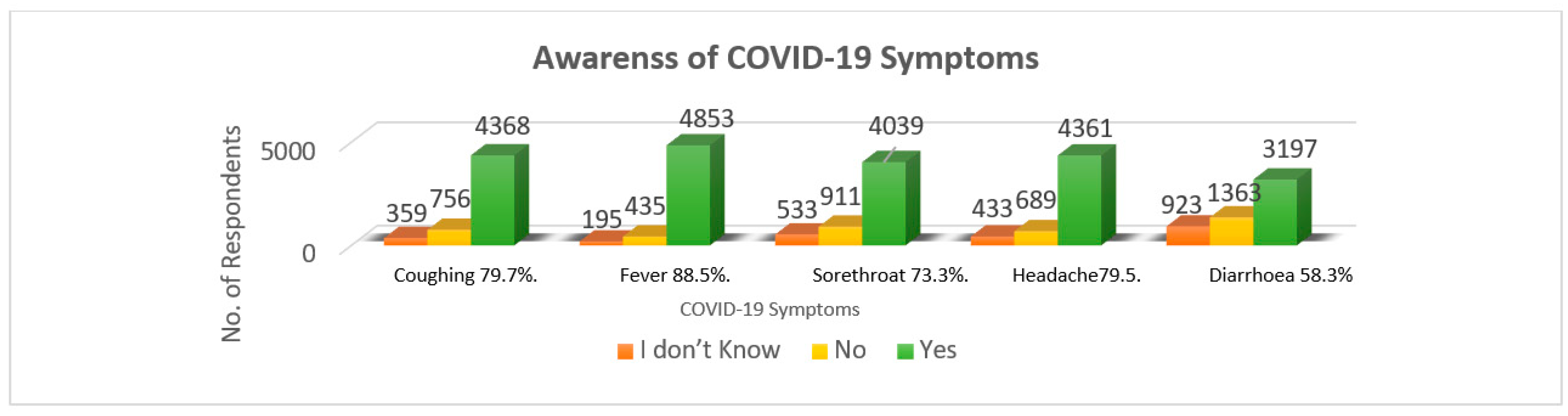
3.2. Level of Knowledge
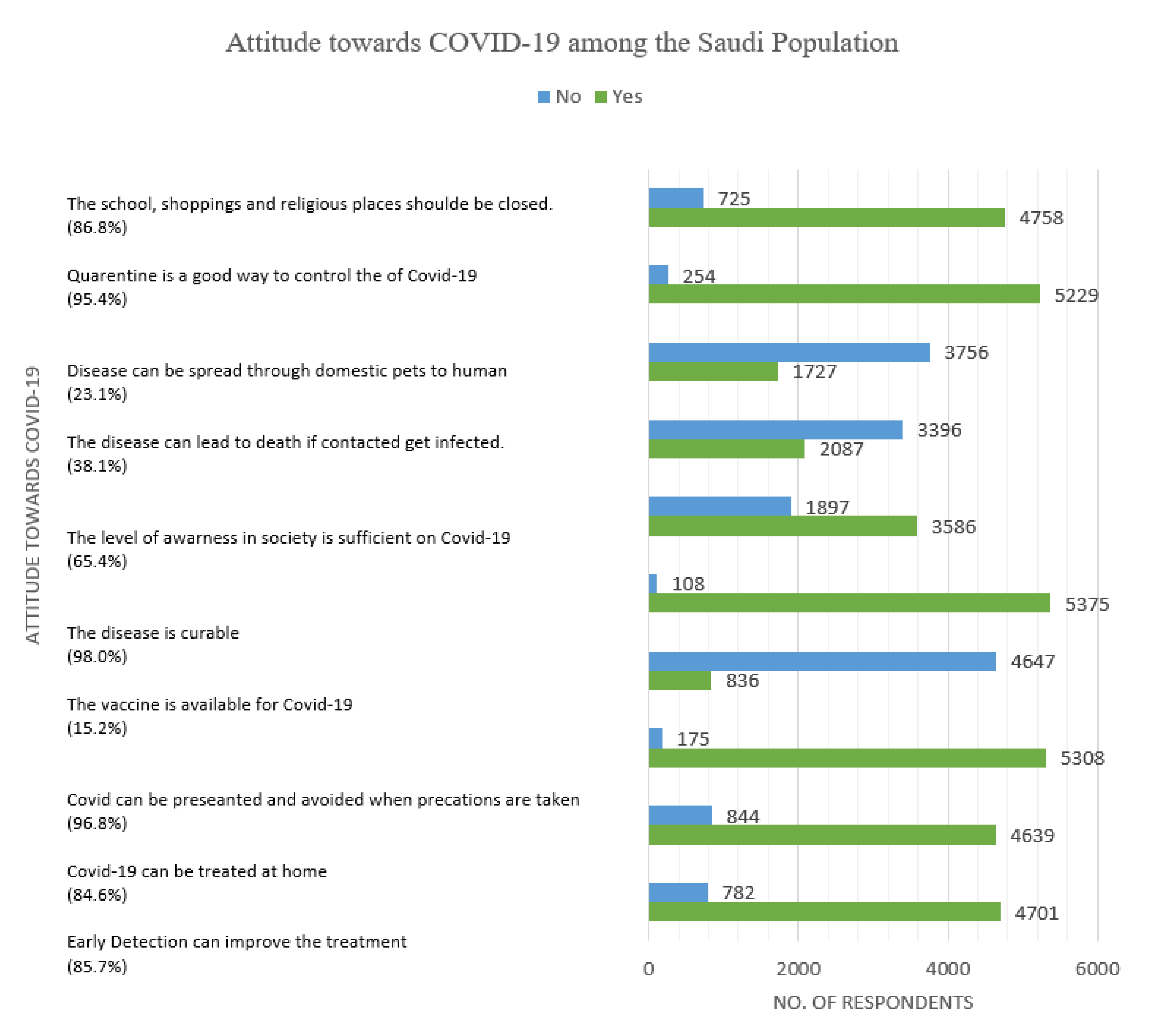
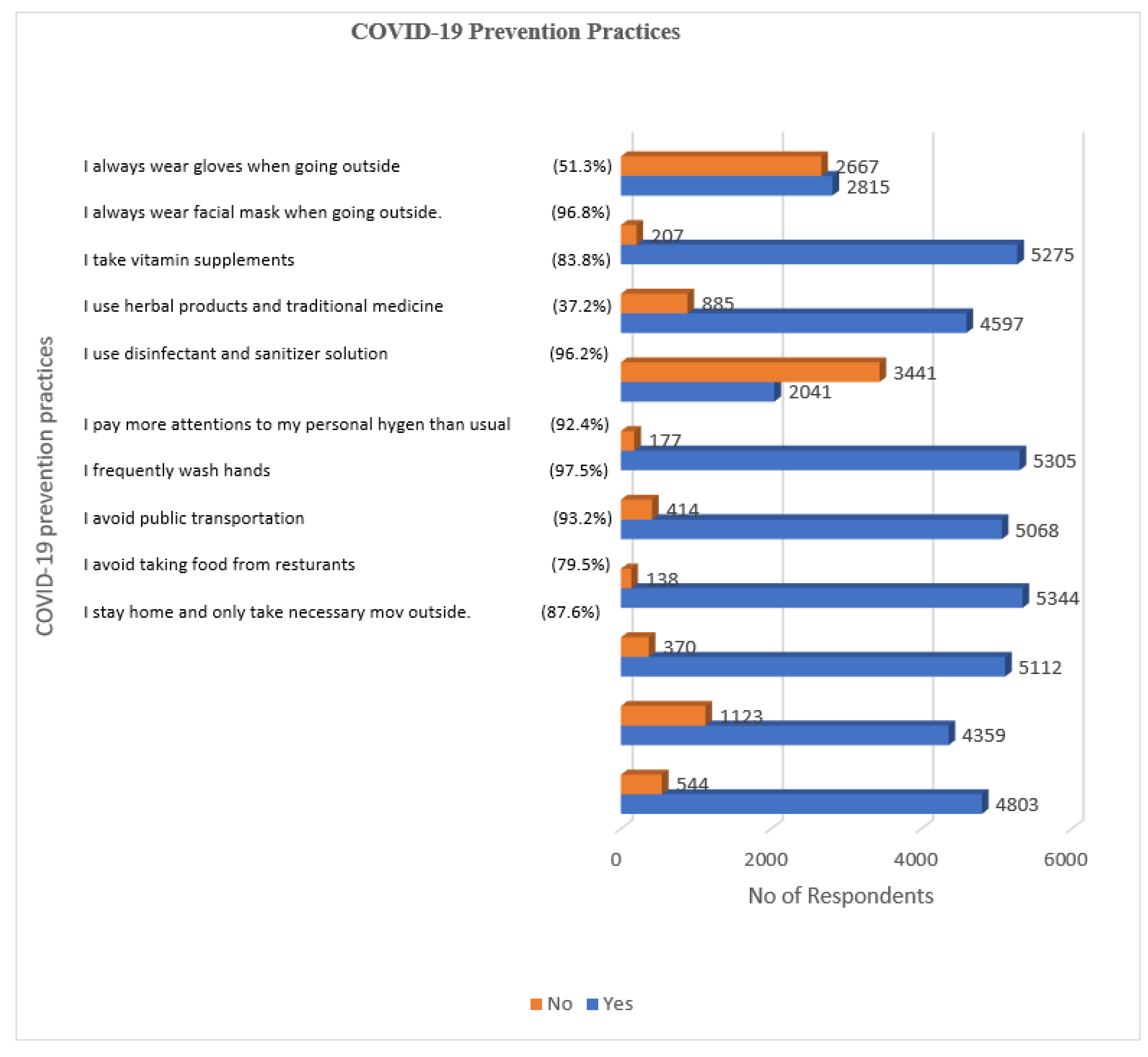
3.3. Practices to Control the COVID-19 Pandemic
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kobrin, S.J. How globalization became a thing that goes bump in the night. J. Int. Bus. Policy 2020, 3, 280–286. [Google Scholar] [CrossRef]
- Yaya, S.; Otu, A.; Labonté, R. Globalisation in the time of COVID-19: Repositioning Africa to meet the immediate and remote challenges. Glob. Health 2020, 16, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, K.F.; Karabulut, G.; Bilgin, M.H.; Doker, A.C. Inter-country distancing, globalisation and the coronavirus pandemic. World Econ. 2020, 43, 1484–1498. [Google Scholar] [CrossRef]
- World Health Organization [WHO]. Coronavirus Disease (COVID-19): How Is it Transmitted? 2020. Available online: https://www.who.int/news-room/q-a-detail/coronavirus-disease-covid-19-how-is-it-transmitted (accessed on 16 December 2020).
- Karamouzian, M.; Madani, N. COVID-19 response in the Middle East and North Africa: Challenges and paths forward. Lancet Glob. Health 2020, 8, 1–2. [Google Scholar] [CrossRef]
- Azuma, K.; Yanagi, U.; Kagi, N.; Kim, H.; Ogata, M.; Hayashi, M. Environmental factors involved in SARS-CoV-2 transmission: Effect and role of indoor environmental quality in the strategy for COVID-19 infection control. Environ. Health Prev. Med. 2020, 25, 1–16. [Google Scholar] [CrossRef]
- Alsofayan, Y.M.; Althunayyan, S.M.; Khan, A.A.; Hakawi, A.M.; Assiri, A.M. Clinical characteristics of COVID-19 in Saudi Arabia: A national retrospective study. J. Infect. Public Health 2020, 13, 920–925. [Google Scholar] [CrossRef]
- Alhazmi, A.; Ali, M.H.M.; Mohieldin, A.; Aziz, F.; Osman, O.B.; Ahmed, W.A. Knowledge, attitudes and practices among people in Saudi Arabia regarding COVID-19: A cross-sectional study. J. Public Health Res. 2020, 9, 18671875. [Google Scholar] [CrossRef] [PubMed]
- Azlan, A.A.; Hamzah, M.R.; Sern, T.J.; Ayub, S.H.; Mohamad, E. Public knowledge, attitudes and practices towards COVID-19: A cross-sectional study in Malaysia. PLoS ONE 2020, 15, e0233668. [Google Scholar] [CrossRef]
- Migone, A.R. The influence of national policy characteristics on COVID-19 containment policies: A comparative analysis. Policy Des. Pract. 2020, 3, 259–276. [Google Scholar] [CrossRef]
- Ahmed, S.; Ajisola, M.; Azeem, K.; Bakibinga, P.; Chen, Y.-F.; Choudhury, N.N.; Fayehun, O.; Griffiths, F.; Harris, B.; Kibe, P.; et al. Impact of the societal response to COVID-19 on access to healthcare for non-COVID-19 health issues in slum communities of Bangladesh, Kenya, Nigeria and Pakistan: Results of pre-COVID and COVID-19 lockdown stakeholder engagements. BMJ Glob. Health 2020, 5, e003042. [Google Scholar] [CrossRef]
- Pereno, A.; Eriksson, D. A multi-stakeholder perspective on sustainable healthcare: From 2030 onwards. Futures 2020, 122, 102605. [Google Scholar] [CrossRef] [PubMed]
- Allen, S.; Julian, Z.; Coyne-Beasley, T.; Erwin, P.C.; Fletcher, F.E. COVID-19’s impact on women: A stakeholder-engagement approach to increase public awareness through virtual town halls. J. Public Health Manag. Pract. 2020, 26, 534–538. [Google Scholar] [CrossRef] [PubMed]
- WHO. Emro.Who.Int. 2020. Available online: http://www.emro.who.int/images/stories/saudi_arabia/saudi-arabia-covid-sit-rep-167-2020-11-01.pdf?ua=1 (accessed on 1 May 2021).
- Setia, M.S. Methodology series module 3: Cross-sectional studies. Indian J. Dermatol. 2016, 61, 261–264. [Google Scholar] [CrossRef]
- The World Bank. Individuals Using the Internet (% of Population)—Saudi Arabia. Available online: https://data.worldbank.org/indicator/IT.NET.USER.ZS?locations=SA (accessed on 7 May 2021).
- Pillay, M. Knowledge, Attitude and Practices (KAP) Survey. Ph.D. Thesis, Stellenbosch University, Stellenbosch, South Africa, 2005. [Google Scholar]
- Bakla, A.; Cekic, A.; Köksal, O. Web-based surveys in educational research. Int. J. Acad. Res. 2013, 5, 5–13. [Google Scholar] [CrossRef]
- AlAnezi, F.; Aljahdali, A.; Alyousef, S.; Alrashed, H.; AlShaikh, W.; Mushcab, H.; Alanzi, T. Implications of public understanding of COVID-19 in Saudi Arabia for fostering effective communication through awareness framework. Front. Public Health 2020, 8, 494–501. [Google Scholar] [CrossRef]
- Alhaddad, M.S. The use of social media among Saudi residents for medicines related information. Saudi Pharm. J. 2018, 26, 1106–1111. [Google Scholar] [CrossRef]
- Aluga, M.A. Coronavirus disease 2019 (COVID-19) in Kenya: Preparedness, response and transmissibility. J. Microbiol. Immunol. Infect. 2020, 53, 671–673. [Google Scholar] [CrossRef]
- Smith, C. The structural vulnerability of healthcare workers during COVID-19: Observations on the social context of risk and the equitable distribution of resources. Soc. Sci. Med. 2020, 258, 113119. [Google Scholar] [CrossRef] [PubMed]
- Csiszar, A.; Jakab, F.; Valencak, T.G.; Lanszki, Z.; Tóth, G.E.; Kemenesi, G.; Tarantini, S.; Fazekas-Pongor, V.; Ungvari, Z. Companion animals likely do not spread COVID-19 but may get infected themselves. GeroScience 2020, 42, 1229–1236. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease (COVID-19) Advice for the Public. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 16 December 2020).
- Liang, X.-H.; Tang, X.; Luo, Y.-T.; Zhang, M.; Feng, Z.-P. Effects of policies and containment measures on control of COVID-19 epidemic in Chongqing. World J. Clin. Cases 2020, 8, 2959–2976. [Google Scholar] [CrossRef]
- Güner, R.; Hasanoğlu, I.; Aktaş, F. COVID-19: Prevention and control measures in community. Turk. J. Med. Sci. 2020, 50, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Acedhars Unilag COVID-19 Response Team; Akindele, A.J.; Agunbiade, F.O.; Sofidiya, M.O.; Awodele, O.; Sowemimo, A.; Ade-Ademilua, O.; Akinleye, M.O.; Ishola, I.O.; Orabueze, I.; et al. COVID-19 pandemic: A case for phytomedicines. Nat. Prod. Commun. 2020, 15, 1934578X20945086. [Google Scholar] [CrossRef]
- WHO. Herbal Medicine Research and Global Health: An Ethical Analysis. Who.Int. 2021. Available online: https://www.who.int/bulletin/volumes/86/8/07-042820/en/ (accessed on 1 May 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Factors | Frequencies (f) | Percentage (%) | |
|---|---|---|---|
| Age | 18–35 years | 3722 | 67.9% |
| 36–50 years | 1177 | 21.5% | |
| 51–65 years | 544 | 9.9% | |
| Above 65 years | 39 | 0.7% | |
| Gender | Female | 2204 | 40.2% |
| Male | 3278 | 59.8% | |
| Career | Non-health professional | 4415 | 80.5% |
| Health professional | 1067 | 19.5% | |
| Level of education | Primary school | 52 | 0.9% |
| High school | 1502 | 27.4% | |
| Intermediate school | 200 | 3.6% | |
| University | 3729 | 68.0% | |
| COVID-19 Awareness | Frequency (f) | Percentage (%) | |
|---|---|---|---|
| Sources of information | Social media | 4189 | 76.4% |
| TV | 1049 | 19.1% | |
| Friends chat | 125 | 2.3% | |
| Newspapers | 120 | 2.2% | |
| Incubation period | I don’t know | 226 | 4.1% |
| Less than 2 days | 44 | 0.8% | |
| 2–5 days | 363 | 6.6% | |
| 6–14 days | 4850 | 88.5% | |
| Vulnerable age group | Less than 15 years | 115 | 2.1% |
| Between 16 and 30 | 65 | 1.2% | |
| Between 31 and 50 | 238 | 4.3% | |
| Above 50 | 5065 | 92.4% | |
| Treatment | I don’t know | 1569 | 28.6% |
| Antibiotics | 985 | 18.0% | |
| Symptomatic therapy | 1284 | 23.4% | |
| Vitamins | 1645 | 30.0% | |
| Hygiene | Wash hands with water and soap | 4793 | 87.4% |
| Use hand sanitizer | 667 | 12.2% | |
| Use water only | 23 | 0.4% | |
| Causes | Immune deficiency | 1434 | 26.2% |
| Viruses | 3282 | 59.9% | |
| Population crowds | 695 | 12.7% | |
| Fungi | 72 | 1.2% | |
| COVID-19 prevention | Social distancing | 3673 | 67.0% |
| Wearing mask | 1475 | 26.9% | |
| Wearing gloves | 37 | 0.7% | |
| Wearing gowns | 298 | 5.4% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alqahtani, A.H.; Alqahtani, S.A.; Alhodaib, A.S.; Al-Wathinani, A.M.; Daoulah, A.; Alhamid, S.; Al-Otaibi, S.N.; Abufayyah, M.; Wazzan, A.M.; Alshahrani, S.S.; et al. Knowledge, Attitude, and Practice (KAP) toward the Novel Coronavirus (COVID-19) Pandemic in a Saudi Population-Based Survey. Int. J. Environ. Res. Public Health 2021, 18, 5286. https://doi.org/10.3390/ijerph18105286
Alqahtani AH, Alqahtani SA, Alhodaib AS, Al-Wathinani AM, Daoulah A, Alhamid S, Al-Otaibi SN, Abufayyah M, Wazzan AM, Alshahrani SS, et al. Knowledge, Attitude, and Practice (KAP) toward the Novel Coronavirus (COVID-19) Pandemic in a Saudi Population-Based Survey. International Journal of Environmental Research and Public Health. 2021; 18(10):5286. https://doi.org/10.3390/ijerph18105286
Chicago/Turabian StyleAlqahtani, Abdulrahman H., Saleh A. Alqahtani, Abdullah S. Alhodaib, Ahmed M. Al-Wathinani, Amin Daoulah, Sameer Alhamid, Salah N. Al-Otaibi, Mohammed Abufayyah, Ahmad M. Wazzan, Saif S. Alshahrani, and et al. 2021. "Knowledge, Attitude, and Practice (KAP) toward the Novel Coronavirus (COVID-19) Pandemic in a Saudi Population-Based Survey" International Journal of Environmental Research and Public Health 18, no. 10: 5286. https://doi.org/10.3390/ijerph18105286
APA StyleAlqahtani, A. H., Alqahtani, S. A., Alhodaib, A. S., Al-Wathinani, A. M., Daoulah, A., Alhamid, S., Al-Otaibi, S. N., Abufayyah, M., Wazzan, A. M., Alshahrani, S. S., Almaleh, Y. S., & Mobrad, A. M. (2021). Knowledge, Attitude, and Practice (KAP) toward the Novel Coronavirus (COVID-19) Pandemic in a Saudi Population-Based Survey. International Journal of Environmental Research and Public Health, 18(10), 5286. https://doi.org/10.3390/ijerph18105286