
The Impact of Caregiving Burden on Mental Well-Being in Coronary Artery Bypass Graft Surgery Caregivers: The Mediatory Role of Perceived Social Support

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
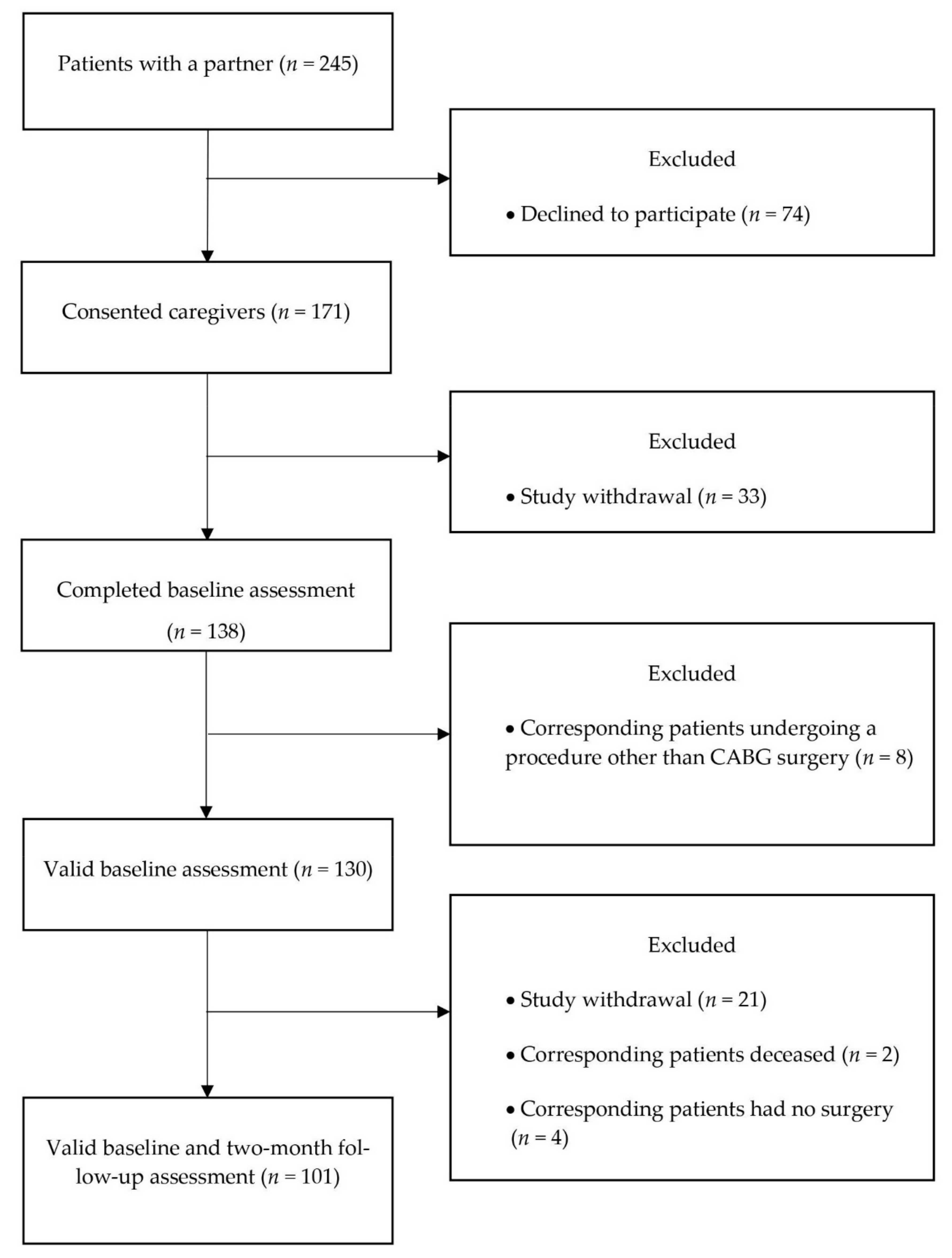
2.1. Participants
2.2. Measures
2.2.1. Predictor Variables: Caregiver Burden Change
2.2.2. Mediator Variables: Social Support Change
2.2.3. Outcome Variables: Depressive Symptoms and Well-Being
2.2.4. Covariates
2.2.5. Statistical Analysis
3. Results
3.1. Descriptive Analyses
3.2. Correlations between Change in Caregiver Burden, Change in Social Support, and Psychological Distress Measures
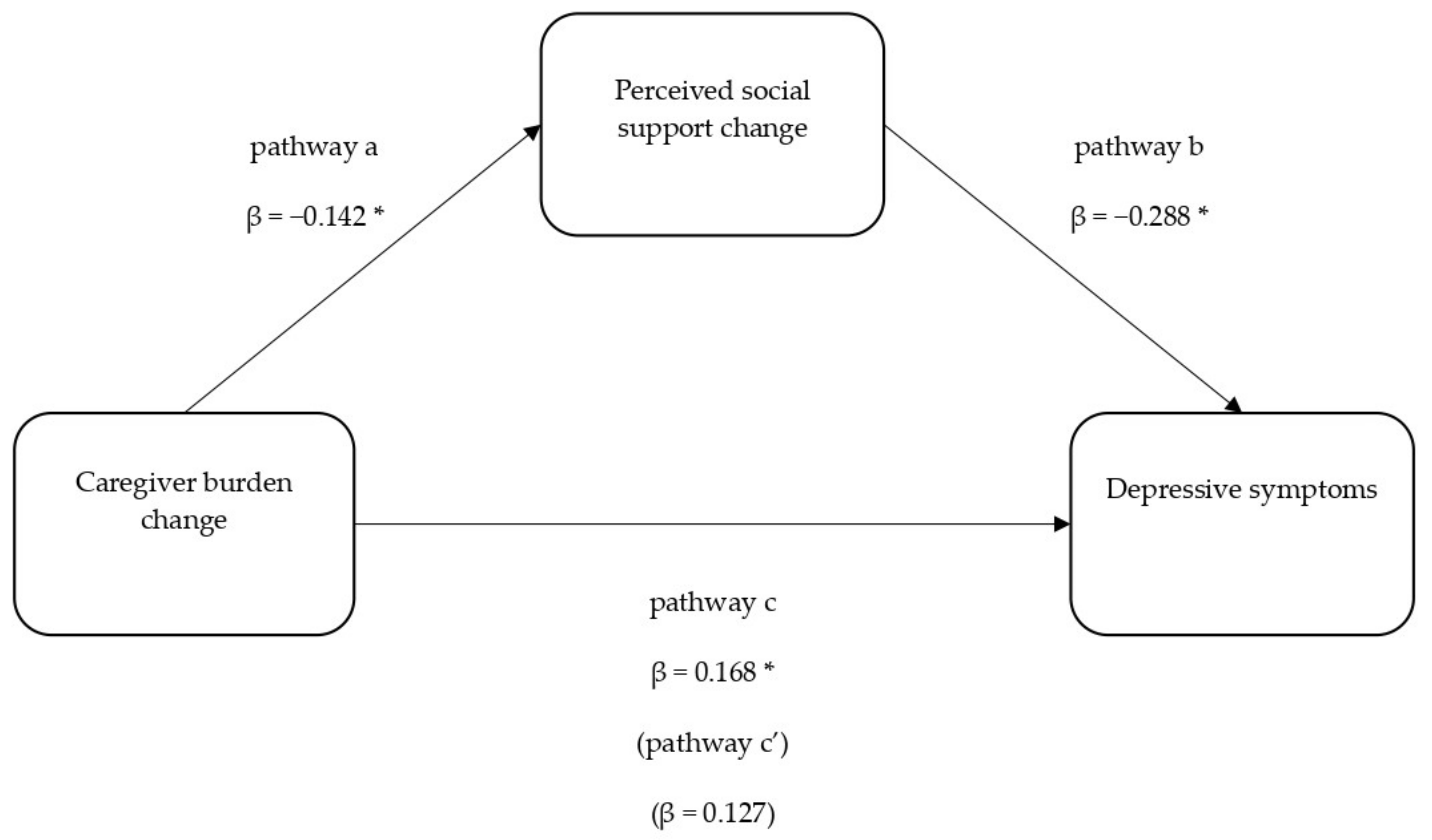
3.3. Caregiver Burden and Social Support in Predicting Depressive Symptoms at 2-Month Follow-Up
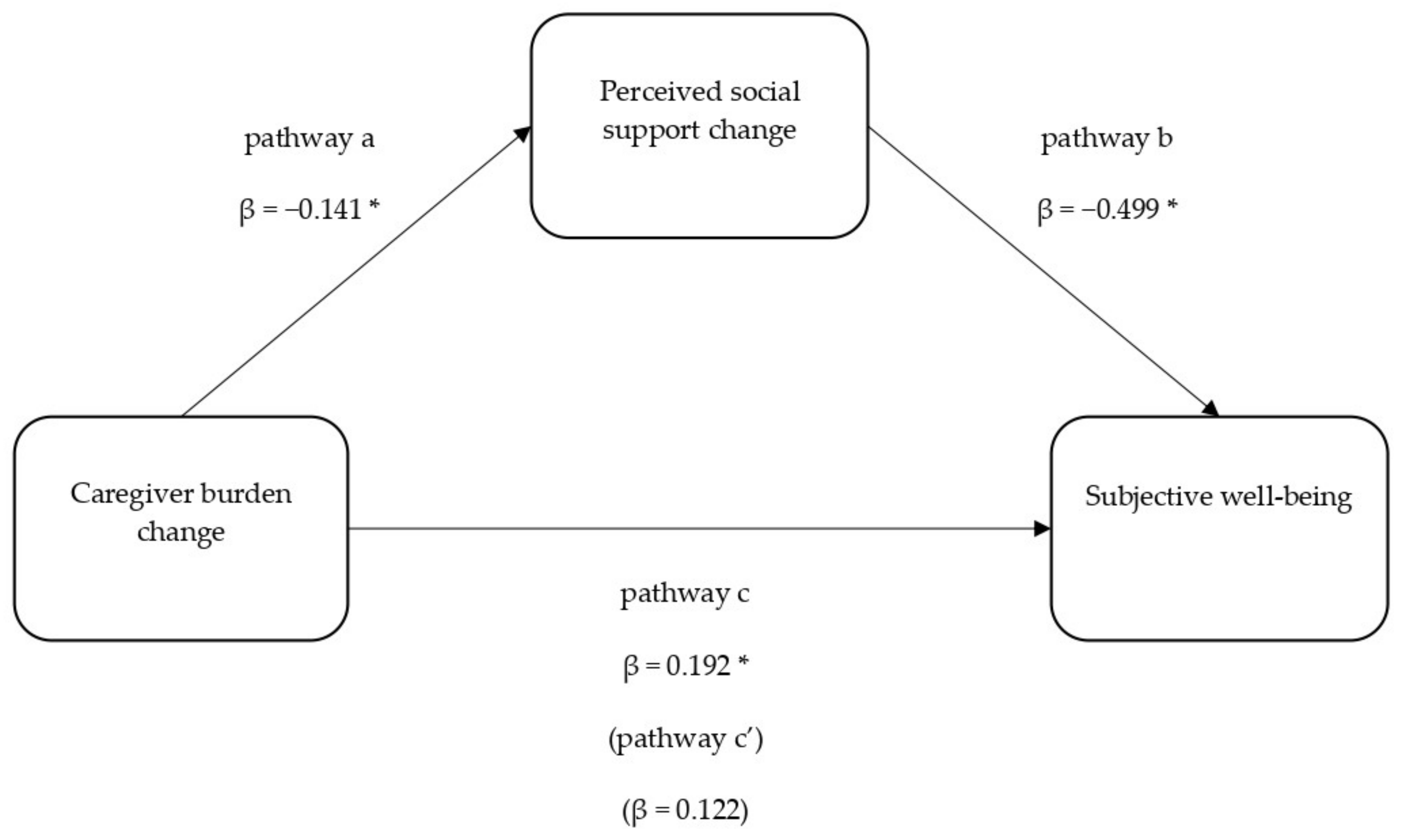
3.4. Caregiver Burden and Social Support in Predicting Subjective Well-Being at 2-Month Follow-Up
3.5. Secondary Analyses: Reverse Mediation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2016. Available online: https://www.who.int/healthinfo/global_burden_disease/estimates/en/ (accessed on 25 November 2019).
- Head, S.J.; Milojevic, M.; Taggart, D.P.; Puskas, J.D. Current Practice of State-of-the-Art Surgical Coronary Revascularization. Circulation 2017, 136, 1331–1345. [Google Scholar] [CrossRef] [PubMed]
- British Heart Foundation. Heart and Circulatory Disease Statistics 2019. 2019. Available online: https://www.bhf.org.uk/what-we-do/our-research/heart-statistics/heart-statistics-publications/cardiovascular-disease-statistics-2019 (accessed on 25 November 2019).
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart disease and stroke statistics—2019 update: A report from the American heart association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef] [PubMed]
- McNeely, C.; Markwell, S.; Vassileva, C. Trends in Patient Characteristics and Outcomes of Coronary Artery Bypass Grafting in the 2000 to 2012 Medicare Population. Ann. Thorac. Surg. 2016, 102, 132–138. [Google Scholar] [CrossRef] [Green Version]
- British Heart Foundation. Coronary Bypass Surgery-British Heart Foundation. Available online: https://www.bhf.org.uk/informationsupport/treatments/coronary-bypass-surgery (accessed on 3 May 2019).
- Halm, M.A. Specific needs, concerns, strategies and advice of caregivers after coronary artery bypass surgery. Hear. Lung 2016, 45, 416–422. [Google Scholar] [CrossRef]
- Halm, M.A.; Treat-Jacobson, D.; Lindquist, R.; Savik, K. Caregiver burden and outcomes of caregiving of spouses of patients who undergo coronary artery bypass graft surgery. Hear. Lung 2007, 36, 170–187. [Google Scholar] [CrossRef]
- Penning, M.J.; Wu, Z. Caregiver Stress and Mental Health: Impact of Caregiving Relationship and Gender. Gerontologist 2015, 56, 1102–1113. [Google Scholar] [CrossRef]
- Chappell, N.L.; Dujela, C.; Smith, A. Spouse and Adult Child Differences in Caregiving Burden. Can. J. Aging/La Rev. Can. du Vieil. 2014, 33, 462–472. [Google Scholar] [CrossRef] [PubMed]
- Conde-Sala, J.L.; Garre-Olmo, J.; Turró-Garriga, O.; Vilalta-Franch, J.; López-Pousa, S. Differential features of burden between spouse and adult-child caregivers of patients with Alzheimer’s disease: An exploratory comparative design. Int. J. Nurs. Stud. 2010, 47, 1262–1273. [Google Scholar] [CrossRef] [Green Version]
- Lin, I.-F.; Fee, H.R.; Wu, H.-S. Negative and Positive Caregiving Experiences: A Closer Look at the Intersection of Gender and Relationship. Fam. Relat. 2012, 61, 343–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinquart, M.; Sörensen, S. Spouses, adult children, and children-in-law as caregivers of older adults: A meta-analytic comparison. Psychol. Aging 2011, 26, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Ott, C.H.; Sanders, S.; Kelber, S.T. Grief and personal growth experience of spouses and adult-child caregivers of individuals with Alzheimer’s disease and related dementias. Gerontologist 2007, 47, 798–809. [Google Scholar] [CrossRef] [Green Version]
- Stolarik, A.; Lindsay, P.; Sherrard, H.; Woodend, A.K. Determination of the burden of care in families of cardiac surgery patients. Prog. Cardiovasc. Nurs. 2000, 15, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Moser, D.K.; Dracup, K. Role of Spousal Anxiety and Depression in Patients’ Psychosocial Recovery After a Cardiac Event. Psychosom. Med. 2004, 66, 527–532. [Google Scholar] [CrossRef]
- Ruiz, J.M.; Matthews, K.A.; Scheier, M.F.; Schulz, R. Does who you marry matter for your health? Influence of patients’ and spouses’ personality on their partners’ psychological well-being following coronary artery bypass surgery. J. Pers. Soc. Psychol. 2006, 91, 255–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halm, M.A.; Treat-Jacobson, D.; Lindquist, R.; Savik, K. Correlates of Caregiver Burden After Coronary Artery Bypass Surgery. Nurs. Res. 2006, 55, 426–436. [Google Scholar] [CrossRef] [Green Version]
- Thomson, P.; Niven, C.A.; Peck, D.F.; Eaves, J. Patients’ and partners’ health-related quality of life before and 4 months after coronary artery bypass grafting surgery. BMC Nurs. 2013, 12, 16. [Google Scholar] [CrossRef] [Green Version]
- Huppert, F.A.; Whittington, J.E. Evidence for the independence of positive and negative well-being: Implications for quality of life assessment. Br. J. Health Psychol. 2003, 8, 107–122. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. On Happiness and Human Potentials: A Review of Research on Hedonic and Eudaimonic Well-Being. Annu. Rev. Psychol. 2001, 52, 141–166. [Google Scholar] [CrossRef] [PubMed]
- Okely, J.A.; Gale, C.R. Well-Being and Chronic Disease Incidence. Psychosom. Med. 2016, 78, 335–344. [Google Scholar] [CrossRef] [Green Version]
- Pearlin, L.I.; Mullan, J.T.; Semple, M.S.J.; Skaff, M.M.M. Caregiving and the Stress Process: An Overview of Concepts and Their Measures. Gerontologist 1990, 30, 583–594. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Shaffer, K.M.; Carver, C.S.; Cannady, R.S. Prevalence and predictors of depressive symptoms among cancer caregivers 5 years after the relative’s cancer diagnosis. J. Consult. Clin. Psychol. 2014, 82, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Roth, D.L.; Mittelman, M.S.; Clay, O.J.; Madan, A.; Haley, W.E. Changes in social support as mediators of the impact of a psychosocial intervention for spouse caregivers of persons with Alzheimer’s disease. Psychol. Aging 2005, 20, 634–644. [Google Scholar] [CrossRef] [PubMed]
- Noonan, M.C.; Wingham, J.; Taylor, R.S. ’Who Cares?’ The experiences of caregivers of adults living with heart failure, chronic obstructive pulmonary disease and coronary artery disease: A mixed methods systematic review. BMJ Open 2018, 8, e020927. [Google Scholar] [CrossRef] [Green Version]
- King, K.B.; Reis, H.T.; Porter, L.A.; Norsen, L.H. Social support and long-term recovery from coronary artery surgery: Effects on patients and spouses. Health Psychol. 1993, 12, 56–63. [Google Scholar] [CrossRef]
- Thomson, P.; Molloy, G.J.; Chung, M.L. The effects of perceived social support on quality of life in patients awaiting coronary artery bypass grafting and their partners: Testing dyadic dynamics using the Actor–Partner Interdependence Model. Psychol. Health Med. 2012, 17, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Rantanen, A.; Kaunonen, M.; Åstedt-Kurki, P.; Tarkka, M.-T. Coronary artery bypass grafting: Social support for patients and their significant others. J. Clin. Nurs. 2004, 13, 158–166. [Google Scholar] [CrossRef]
- Rantanen, A.; Kaunonen, M.; Sintonen, H.; Koivisto, A.-M.; Åstedt-Kurki, P.; Tarkka, M.-T. Factors associated with health-related quality of life in patients and significant others one month after coronary artery bypass grafting. J. Clin. Nurs. 2008, 17, 1742–1753. [Google Scholar] [CrossRef]
- Poole, L.; Kidd, T.; Leigh, E.; Ronaldson, A.; Jahangiri, M.; Steptoe, A. Preoperative Sleep Complaints Are Associated with Poor Physical Recovery in the Months Following Cardiac Surgery. Ann. Behav. Med. 2014, 47, 347–357. [Google Scholar] [CrossRef]
- Ronaldson, A.; Kidd, T.; Poole, L.; Leigh, E.; Jahangiri, M.; Steptoe, A. Diurnal Cortisol Rhythm Is Associated With Adverse Cardiac Events and Mortality in Coronary Artery Bypass Patients. J. Clin. Endocrinol. Metab. 2015, 100, 3676–3682. [Google Scholar] [CrossRef] [Green Version]
- Oberst, M.T.; Thomas, S.E.; Gass, K.A.; Ward, S.E. Caregiving demands and appraisal of stress among family caregivers. Cancer Nurs. 1989, 12, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, P.H.; Powell, L.; Blumenthal, J.; Norten, J.; Ironson, G.; Pitula, C.R.; Froelicher, E.S.; Czajkowski, S.; Youngblood, M.; Huber, M.; et al. A Short Social Support Measure for Patients Recovering From Myocardial Infarction. J. Cardiopulm. Rehabil. 2003, 23, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Choi-Kwon, S.; Mitchell, P.H.; Veith, R.; Teri, L.; Buzaitis, A.; Cain, K.C.; Becker, K.J.; Tirschwell, D.; Fruin, M.; Choi, J.; et al. Comparing Perceived Burden for Korean and American Informal Caregivers of Stroke Survivors. Rehabil. Nurs. 2009, 34, 141–150. [Google Scholar] [CrossRef] [Green Version]
- Griffin, J.M.; Lee, M.K.; Bangerter, L.R.; Van Houtven, C.H.; Friedemann-Sánchez, G.; Phelan, S.M.; Carlson, K.F.; Meis, L.A. Burden and mental health among caregivers of veterans with traumatic brain injury/polytrauma. Am. J. Orthopsychiatry 2017, 87, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Stalder, T.; Tietze, A.; Steudte, S.; Alexander, N.; Dettenborn, L.; Kirschbaum, C. Elevated hair cortisol levels in chronically stressed dementia caregivers. Psychoneuroendocrinology 2014, 47, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Steer, R.A.; Carbin, M.G. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clin. Psychol. Rev. 1988, 8, 77–100. [Google Scholar] [CrossRef]
- Steer, R.A.; Beck, A.T.; Garrison, B. Applications of the Beck Depression Inventory. In Assessment of Depression; Springer Science +Business Media LLC: Berlin/Heidelberg, Germany, 1986; pp. 123–142. [Google Scholar]
- Aggarwal, B.; Liao, M.; Christian, A.; Mosca, L. Influence of Caregiving on Lifestyle and Psychosocial Risk Factors Among Family Members of Patients Hospitalized with Cardiovascular Disease. J. Gen. Intern. Med. 2008, 24, 93–98. [Google Scholar] [CrossRef]
- Hyde, M.; Wiggins, R.D.; Higgs, P.; Blane, D.B. A measure of quality of life in early old age: The theory, development and properties of a needs satisfaction model (CASP-19). Aging Ment. Health 2003, 7, 186–194. [Google Scholar] [CrossRef]
- Office for National Statistics. Standard Occupational Clasification 2010: Volume 1 Structure and Descriptions of Unit Groups; Office for National Statistics: Newport, UK, 2010; Volume 1, ISBN 9780230248199. Available online: https://www.ons.gov.uk/methodology/classificationsandstandards/standardoccupationalclassificationsoc/soc2010/soc2010volume1structureanddescriptionsofunitgroups#the-soc2010-manual) (accessed on 25 November 2019).
- Booth, M. Assessment of Physical Activity: An International Perspective. Res. Q. Exerc. Sport 2000, 71, 114–120. [Google Scholar] [CrossRef]
- Roques, F.; Michel, P.; Goldstone, A.; Nashef, S. The logistic EuroSCORE. Eur. Hear. J. 2003, 24, 882–883. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple me-diator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Davies, N. Carers’ opinions and emotional responses following cardiac surgery: Cardiac rehabilitation implications for critical care nurses. Intensiv. Crit. Care Nurs. 2000, 16, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Park, E.O.; Yates, B.C.; Meza, J.L.; Kosloski, K.; Pullen, C.H. Spousal Caregivers of Coronary Artery Bypass Surgery Patients: Differences between Caregivers with Low vs. High Caregiving Demands. Rehabil. Nurs. 2016, 41, 260–269. [Google Scholar] [CrossRef]
- Halm, M.A.; Bakas, T. Factors Associated with Caregiver Depressive Symptoms, Outcomes, and Perceived Physical Health After Coronary Artery Bypass Surgery. J. Cardiovasc. Nurs. 2007, 22, 508–515. [Google Scholar] [CrossRef]
- Nieboer, A.; Schulz, R.; Matthews, K.; Scheier, M.; Ormel, J.; Lindenberg, S. Spousal caregivers’ activity restriction and de-pression: A model for changes over time. Soc. Sci. Med. 1998, 47, 1361–1371. [Google Scholar] [CrossRef]
- Thielemann, P.A.; Conner, N.E. Social Support as a Mediator of Depression in Caregivers of Patients with End-Stage Disease. J. Hosp. Palliat. Nurs. 2009, 11, 82–90. [Google Scholar] [CrossRef]
- Graven, L.J.; Azuero, A.; Abbott, L.; Grant, J.S. Psychosocial Factors Related to Adverse Outcomes in Heart Failure Caregivers. J. Cardiovasc. Nurs. 2020, 35, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Burnette, D.; Duci, V.; Dhembo, E. Psychological distress, social support, and quality of life among cancer caregivers in Albania. Psychooncology 2017, 26, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Tolea, M.I.; Arcay, V.; Lopes, Y.; Galvin, J.E. Self-efficacy and social support for psychological well-being of family caregivers of care recipients with dementia with Lewy bodies, Parkinson’s disease dementia, or Alzheimer’s disease. Soc. Work Ment. Health 2019, 17, 253–278. [Google Scholar] [CrossRef]
- Pinquart, M.; Sörensen, S. Differences between caregivers and noncaregivers in psychological health and physical health: A meta-analysis. Psychol. Aging 2003, 18, 250–267. [Google Scholar] [CrossRef]
- Wolff, J.L.; Spillman, B.C.; Freedman, V.A.; Kasper, J.D. A National Profile of Family and Unpaid Caregivers Who Assist Older Adults With Health Care Activities. JAMA Intern. Med. 2016, 176, 372–379. [Google Scholar] [CrossRef]
- Cheng, S.-T. Dementia Caregiver Burden: A Research Update and Critical Analysis. Curr. Psychiatry Rep. 2017, 19, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallim, A.B.; Sayampanathan, A.A.; Cuttilan, A.; Chun-Man Ho, R. Prevalence of Mental Health Disorders Among Care-givers of Patients with Alzheimer Disease. J. Am. Med. Dir. Assoc. 2015, 16, 1034–1041. [Google Scholar] [CrossRef]
- Bevans, M.F.; Sternberg, E.M. Caregiving Burden, Stress, and Health Effects Among Family Caregivers of Adult Cancer Pa-tients. JAMA 2012, 307, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Kelley, D.E.; Kent, E.E.; Litzelman, K.; Mollica, M.A.; Rowland, J.H. Dyadic associations between perceived social support and cancer patient and caregiver health: An actor-partner interdependence modeling approach. Psycho-Oncology 2019, 28, 1453–1460. [Google Scholar] [CrossRef]
- Clay, O.J.; Roth, D.L.; Wadley, V.G.; Haley, W.E. Changes in social support and their impact on psychosocial outcome over a 5-year period for African American and White dementia caregivers. Int. J. Geriatr. Psychiatry 2008, 23, 857–862. [Google Scholar] [CrossRef]
- Akosile, C.O.; Banjo, T.O.; Okoye, E.C.; Ibikunle, P.O.; Odole, A.C. Informal caregiving burden and perceived social support in an acute stroke care facility. Health Qual. Life Outcomes 2018, 16, 57. [Google Scholar] [CrossRef] [Green Version]
- Haber, M.G.; Cohen, J.L.; Lucas, T.; Baltes, B.B. The relationship between self-reported received and perceived social support: A meta-analytic review. Am. J. Community Psychol. 2007, 39, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Thoits, P.A. Mechanisms Linking Social Ties and Support to Physical and Mental Health. J. Health Soc. Behav. 2011, 52, 145–161. [Google Scholar] [CrossRef] [Green Version]
- Jiang, L.; Drolet, A.; Kim, H.S. Age and Social Support Seeking: Understanding the Role of Perceived Social Costs to Others. Pers. Soc. Psychol. Bull. 2018, 44, 1104–1116. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.E. Social Support: A Review. In The Oxford Handbook of Health Psychology; Oxford University Press (OUP): New York, NY, USA, 2011; pp. 189–214. [Google Scholar]
- Wang, J.; Mann, F.; Lloyd-Evans, B.; Ma, R.; Johnson, S. Associations between loneliness and perceived social support and outcomes of mental health problems: A systematic review. BMC Psychiatry 2018, 18, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dam, A.E.; de Vugt, M.E.; Klinkenberg, I.P.; Verhey, F.R.; van Boxtel, M.P. A systematic review of social support interventions for caregivers of people with dementia: Are they doing what they promise? Maturitas 2016, 85, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Parker Oliver, D.; Patil, S.; Benson, J.J.; Gage, A.; Washington, K.; Kruse, R.L.; Demiris, G. The Effect of Internet Group Sup-port for Caregivers on Social Support, Self-Efficacy, and Caregiver Burden: A Meta-Analysis. Telemed. J. e-Health 2017, 23, 621–629. [Google Scholar]
- Nissen, N.K.; Madsen, M.; Kjøller, M.; Waldorff, S.B.; Zwisler, A.-D.O. Are hospitals also for relatives? A survey of hospitals’ activities regarding relatives of cardiac patients. Scand. J. Public Health 2008, 36, 827–831. [Google Scholar] [CrossRef] [PubMed]
- Hartford, K.; Wong, C.; Zakaria, D. Randomized controlled trial of a telephone intervention by nurses to provide information and support to patients and their partners after elective coronary artery bypass graft surgery: Effects of anxiety. Hear. Lung 2002, 31, 199–206. [Google Scholar] [CrossRef]
- Keeping-Burke, L.; Purden, M.; Frasure-Smith, N.; Cossette, S.; McCarthy, F.; Amsel, R. Bridging the Transition from Hospital to Home: Effects of the VITAL Telehealth Program on Recovery for CABG Surgery Patients and their Caregivers. Res. Nurs. Health 2013, 36, 540–553. [Google Scholar] [CrossRef]
- Hopwood, J.; Walker, N.; McDonagh, L.; Rait, G.; Walters, K.; Iliffe, S.; Ross, J.; Davies, N. Internet-Based Interventions Aimed at Supporting Family Caregivers of People With Dementia: Systematic Review. J. Med Internet Res. 2018, 20, e216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dam, A.E.; Christie, H.L.; Smeets, C.M.; van Boxtel, M.P.; Verhey, F.R.; de Vugt, M.E. Process evaluation of a social support platform ‘Inlife’ for caregivers of people with dementia. Internet Interv. 2019, 15, 18–27. [Google Scholar] [CrossRef]
- Riecher-Rössler, A. Sex and gender differences in mental disorders. Lancet Psychiatry 2017, 4, 8–9. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Mean ± SD or n (%) |
|---|---|
| Baseline demographic variables | |
| Age | 65.89 ± 8.48 |
| Sex—Female | 97 (96.0) |
| Occupation classification | |
| High | 41 (40.6) |
| Intermediate | 49 (48.5) |
| Low | 11 (10.9) |
| Household of two persons | 88 (87.1) |
| Baseline behavioural variables | |
| Smoker | 3 (3.0) |
| Physical activity—walking (hours per week) | 4.26 ± 5.58 |
| Patients’ clinical risk | |
| EuroSCORE (%) | 4.28 ± 3.58 |
| Characteristic | Pre-Surgery | 2-Month Follow-Up | Change Score |
|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | |
| Caregiver Burden (OCBS) | 21.45 ± 5.17 | 26.48 ± 7.85 | 5.02 ± 6.47 * |
| Social Support (ESSI) | 28.51 ± 4.65 | 25.74 ± 5.03 | −2.76 ± 4.27 * |
| Depressive Symptoms (BDI) | 7.18 ± 5.96 | 6.80 ± 6.34 | |
| Subjective Well-Being (CASP-19) | 15.38 ± 7.77 | 15.89 ± 9.15 |
| Variable | 1. Change in Caregiver Burden | 2. Change in Social Support | 3. Depressive Symptoms | 4. Subjective Well-Being |
|---|---|---|---|---|
| 1. Change in caregiver burden | - | |||
| 2. Change in social support | −0.213 * | - | ||
| 3. Depressive symptoms | 0.258 ** | −0.226 * | - | |
| 4. Subjective well-being | 0.299 ** | −0.295 ** | 0.691 ** | - |
| Predictor Variable | B | S.E. | 95% CI | β | p |
|---|---|---|---|---|---|
| Step 1 | |||||
| Age | 0.032 | 0.071 | [−0.109; 0.173] | 0.043 | 0.652 |
| Gender | 2.538 | 2.300 | [−2.031; 7.106] | 0.078 | 0.273 |
| Occupation | 0.144 | 0.238 | [−0.328; 0.616] | 0.043 | 0.546 |
| Number in household | 1.455 | 0.752 | [−0.039; 2.949] | 0.149 | 0.056 |
| Smoking | 5.491 | 2.620 | [0.286; 10.695] | 0.148 | 0.039 |
| Physical activity | 0.146 | 0.083 | [−0.019; 0.311] | 0.128 | 0.083 |
| Patients’ EuroSCORE | 0.034 | 0.142 | [−0.247; 0.316] | 0.019 | 0.809 |
| Baseline depressive symptoms | 0.759 | 0.074 | [0.612; 0.906] | 0.714 | <0.001 |
| Step 2 | |||||
| Age | 0.019 | 0.069 | [−0.118; 0.156] | 0.025 | 0.785 |
| Gender | 1.664 | 2.267 | [−2.839; 6.168] | 0.051 | 0.465 |
| Occupation | 0.102 | 0.232 | [−0.359; 0.563] | 0.030 | 0.661 |
| Number in household | 1.068 | 0.749 | [−0.420; 2.556] | 0.109 | 0.157 |
| Smoking | 5.127 | 2.555 | [0.051; 10.203] | 0.138 | 0.048 |
| Physical activity | 0.132 | 0.081 | [−0.029; 0.293] | 0.116 | 0.108 |
| Patients’ EuroSCORE | 0.074 | 0.139 | [−0.202; 0.350] | 0.042 | 0.594 |
| Baseline depressive symptoms | 0.750 | 0.072 | [0.607; 0.893] | 0.705 | <0.001 |
| ΔCaregiver burden | 0.168 | 0.068 | [0.032; 0.303] | 0.171 | 0.016 |
| Step 3 | |||||
| Age | 0.007 | 0.067 | [−0.126; 0.139] | 0.009 | 0.918 |
| Gender | 2.320 | 2.195 | [−2.040; 6.681] | 0.072 | 0.293 |
| Occupation | 0.118 | 0.224 | [−0.326; 0.562] | 0.035 | 0.599 |
| Number in household | 0.808 | 0.726 | [−0.625; 2.261] | 0.084 | 0.263 |
| Smoking | 3.546 | 2.522 | [−1.464; 8.555] | 0.095 | 0.163 |
| Physical activity | 0.136 | 0.078 | [−0.019; 0.291] | 0.120 | 0.085 |
| Patients’ EuroSCORE | 0.083 | 0.134 | [−0.183; 0.348] | 0.047 | 0.539 |
| Baseline depressive symptoms | 0.758 | 0.069 | [0.620; 0.896] | 0.712 | <0.001 |
| ΔCaregiver burden | 0.127 | 0.067 | [−0.006; 0.260] | 0.129 | 0.062 |
| ΔSocial support | −0.288 | 0.101 | [−0.487; −0.088] | −0.193 | 0.005 |
| Predictor Variable | B | S.E. | 95% CI | β | p |
|---|---|---|---|---|---|
| Step 1 | |||||
| Age | 0.058 | 0.090 | [−0.122; 0.237] | 0.054 | 0.524 |
| Gender | 4.455 | 2.970 | [−1.443; 10.353] | 0.095 | 0.137 |
| Occupation | 0.395 | 0.305 | [−0.212; 1.002] | 0.081 | 0.199 |
| Number in household | 2.725 | 0.974 | [0.791; 4.659] | 0.193 | 0.006 |
| Smoking | 8.717 | 3.389 | [1.987; 15.447] | 0.163 | 0.012 |
| Physical Activity | 0.152 | 0.107 | [−0.060; 0.364] | 0.093 | 0.157 |
| Patients’ EuroSCORE | −0.022 | 0.186 | [−0.390; 0.347] | −0.008 | 0.907 |
| Baseline well-being | 0.910 | 0.074 | [0.763; 1.057] | 0.774 | <0.001 |
| Step 2 | |||||
| Age | 0.044 | 0.089 | [−0.133; 0.221] | 0.041 | 0.622 |
| Gender | 3.405 | 2.953 | [−2.460; 9.270] | 0.073 | 0.252 |
| Occupation | 0.343 | 0.301 | [−0.255; 0.940] | 0.070 | 0.257 |
| Number in household | 2.308 | 0.974 | [0.372; 4.243] | 0.164 | 0.020 |
| Smoking | 8.226 | 3.331 | [1.609; 14.842] | 0.153 | 0.015 |
| Physical activity | 0.134 | 0.105 | [−0.074; 0.343] | 0.082 | 0.204 |
| Patients’ EuroSCORE | 0.016 | 0.183 | [−0.347; 0.379] | 0.006 | 0.929 |
| Baseline well-being | 0.891 | 0.073 | [0.745; 1.036] | 0.757 | <0.001 |
| ΔCaregiver burden | 0.192 | 0.089 | [0.015; 0.369] | 0.136 | 0.034 |
| Step 3 | |||||
| Age | 0.025 | 0.083 | [−0.139; 0.189] | 0.023 | 0.762 |
| Gender | 4.536 | 2.754 | [−0.934; 10.006] | 0.097 | 0.103 |
| Occupation | 0.374 | 0.279 | [−0.181; 0.928] | 0.077 | 0.184 |
| Number in household | 1.885 | 0.910 | [0.077; 3.693] | 0.134 | 0.041 |
| Smoking | 5.477 | 3.166 | [−0.813; 11.767] | 0.102 | 0.087 |
| Physical activity | 0.143 | 0.097 | [−0.050; 0.336] | 0.087 | 0.145 |
| Patients’ EuroSCORE | 0.029 | 0.170 | [−0.308; 0.366] | 0.011 | 0.864 |
| Baseline well-being | 0.892 | 0.068 | [0.757; 1.027] | 0.759 | <0.001 |
| ΔCaregiver burden | 0.121 | 0.084 | [−0.046; 0.289] | 0.086 | 0.153 |
| ΔSocial support | −0.499 | 0.126 | [−0.748; −0.249] | −0.233 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singh Solorzano, C.; Leigh, E.; Steptoe, A.; Ronaldson, A.; Kidd, T.; Jahangiri, M.; Poole, L. The Impact of Caregiving Burden on Mental Well-Being in Coronary Artery Bypass Graft Surgery Caregivers: The Mediatory Role of Perceived Social Support. Int. J. Environ. Res. Public Health 2021, 18, 5447. https://doi.org/10.3390/ijerph18105447
Singh Solorzano C, Leigh E, Steptoe A, Ronaldson A, Kidd T, Jahangiri M, Poole L. The Impact of Caregiving Burden on Mental Well-Being in Coronary Artery Bypass Graft Surgery Caregivers: The Mediatory Role of Perceived Social Support. International Journal of Environmental Research and Public Health. 2021; 18(10):5447. https://doi.org/10.3390/ijerph18105447
Chicago/Turabian StyleSingh Solorzano, Claudio, Elizabeth Leigh, Andrew Steptoe, Amy Ronaldson, Tara Kidd, Marjan Jahangiri, and Lydia Poole. 2021. "The Impact of Caregiving Burden on Mental Well-Being in Coronary Artery Bypass Graft Surgery Caregivers: The Mediatory Role of Perceived Social Support" International Journal of Environmental Research and Public Health 18, no. 10: 5447. https://doi.org/10.3390/ijerph18105447
APA StyleSingh Solorzano, C., Leigh, E., Steptoe, A., Ronaldson, A., Kidd, T., Jahangiri, M., & Poole, L. (2021). The Impact of Caregiving Burden on Mental Well-Being in Coronary Artery Bypass Graft Surgery Caregivers: The Mediatory Role of Perceived Social Support. International Journal of Environmental Research and Public Health, 18(10), 5447. https://doi.org/10.3390/ijerph18105447