
Effects of Tele-Rehabilitation Compared with Home-Based in-Person Rehabilitation for Older Adult’s Function after Hip Fracture

 ,
,  , ,
, ,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
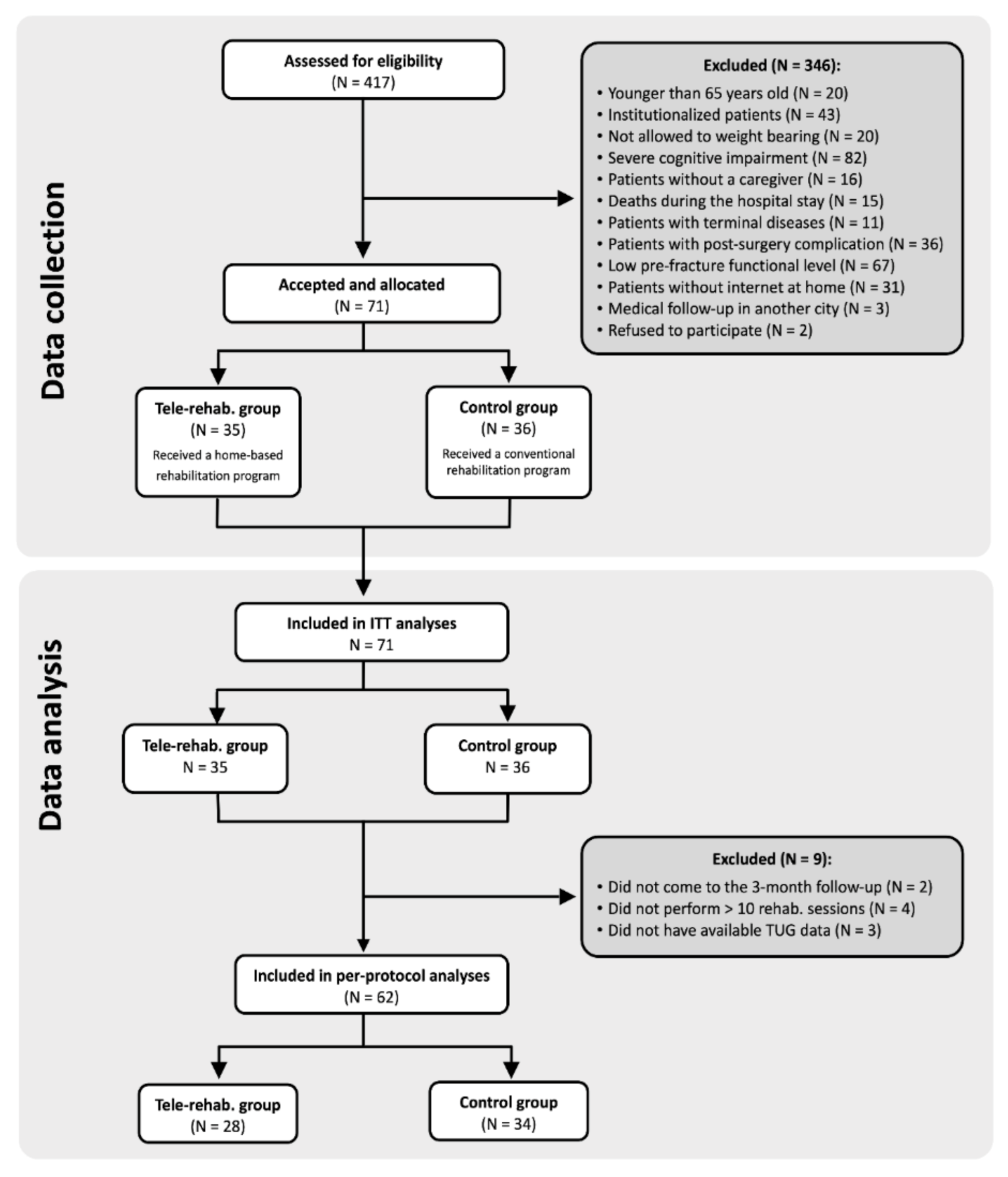
2.1. Study Design and Population
2.2. Recruitment, Allocation, and Blinding
2.3. Tele-Rehabilitation Characteristics
2.3.1. Both Groups: Usual Care during a Hospital Stay and Caregivers’ Workshop
2.3.2. Tele-Rehabilitation Group (@ctivehip)
2.3.3. Control Group
2.4. Primary Outcome: Functional Status
2.5. Secondary Outcome: Physical Performance
2.6. Descriptive Information
2.7. Sample Size
2.8. Data Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Variables | Tele-Rehab. (n = 35) | Control (n = 36) | p |
|---|---|---|---|
| Age (years) | 76.71 ± 6.04 | 80.72 ± 5.59 | 0.005 |
| Weight (kg) | 68.65 ± 9.45 | 69.05 ± 8.94 | 0.855 |
| Height (cm) | 160.6 ± 6.69 | 157.61 ± 7.68 | 0.085 |
| BMI (kg/m2) | 26.7 ± 3.95 | 27.82 ± 3.23 | 0.195 |
| Gender. n (%) | 1.000 | ||
| Men | 9 (25.7%) | 9 (25.0%) | |
| Women | 26 (74.3%) | 27 (75.0%) | |
| Outcomes Basal | |||
| FIM Basal | 77.46 ± 5.48 | 78.22 ± 6.48 | 0.593 |
| TUG Basal (seconds) | 81.02 ± 71.04 | 99.37 ± 63.71 | 0.256 |
| SPPB Basal | 3.03 ± 1.32 | 2.58 ± 1.36 | 0.166 |
| Outcomes Post-rehab. | |||
| FIM Post | 119.23 ± 8.15 | 108.5 ± 14.45 | |
| TUG Post (seconds) | 15.05 ± 9.01 | 23.96 ± 13.38 | |
| SPPB Post | 7.86 ± 2.99 | 6.00 ± 2.98 | |
| Confounder | |||
| Type of fracture | 0.232 | ||
| Intracapsular | 17 (48.6%) | 12 (33.3%) | |
| Extracapsular | 18 (51.4%) | 24 (66.7%) |
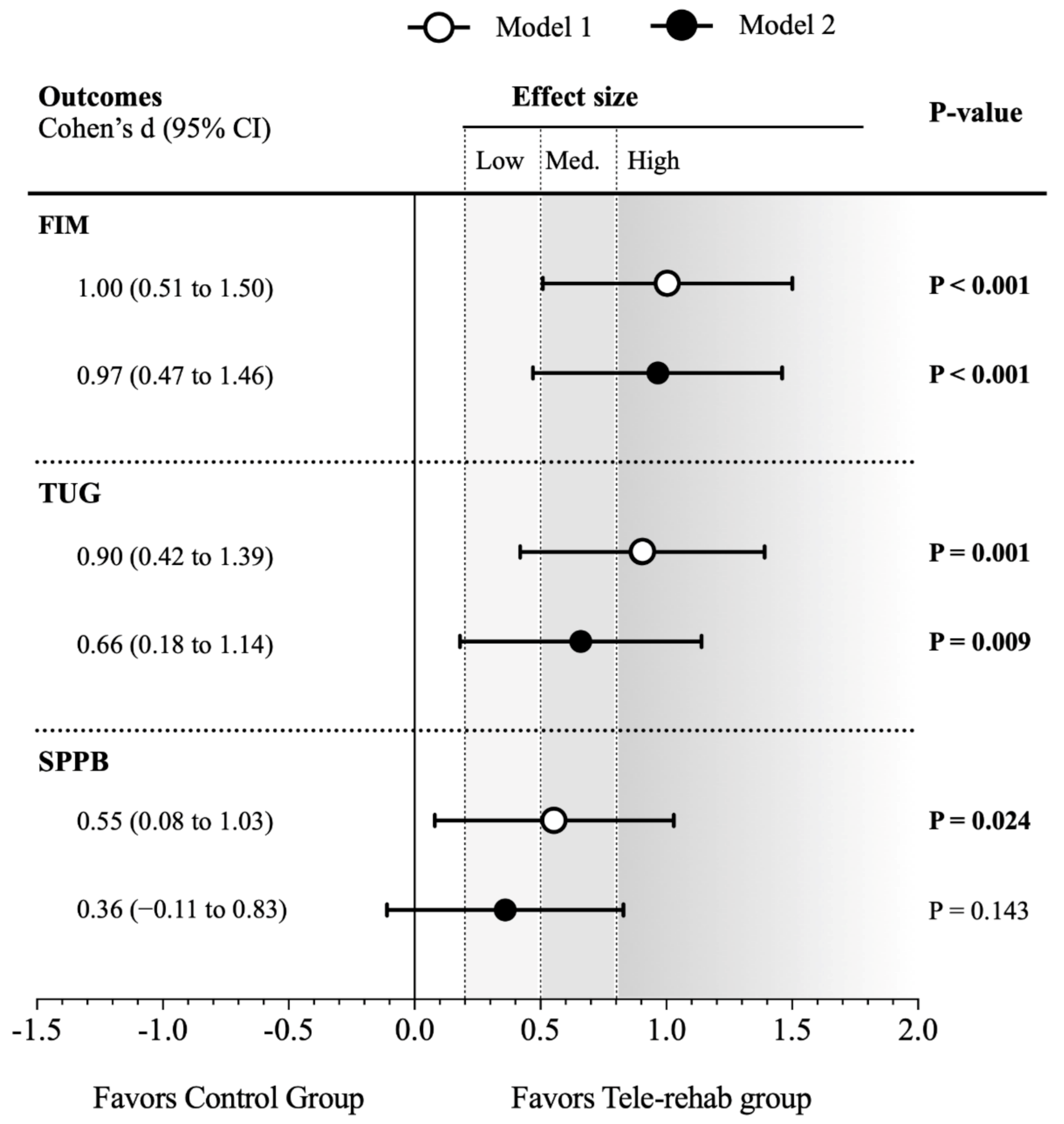
| Statistical Models Outcomes | Tele-Rehabilitation Group | Control Group | Z-Score Differences Rehab–Control (95% CI) | p | ||
|---|---|---|---|---|---|---|
| N | Z-Score (95% CI) | N | Z-Score (95% CI) | |||
| Model 1 | ||||||
| FIM | 35 | 0.45 (0.15 to 0.75) | 36 | −0.45 (−0.74 to −0.15) | 0.89 (0.47 to 1.32) | <0.001 |
| TUG | 35 | −0.37 (−0.65 to −0.10) | 36 | 0.36 (0.09 to 0.64) | −0.74 (−1.13 to −0.35) | <0.001 |
| SPPB | 35 | 0.30 (−0.04 to 0.64) | 36 | −0.26 (−0.59 to 0.08) | 0.55 (0.08 to 1.03) | 0.024 |
| Model 2 | ||||||
| FIM | 35 | 0.41 (0.12 to 0.70) | 36 | −0.41 (−0.70 to −0.13) | 0.82 (0.42 to 1.23) | <0.001 |
| TUG | 35 | −0.24 (−0.48 to 0.00) | 36 | 0.24 (−0.01 to 0.47) | −0.48 (−0.83 to −0.12) | 0.009 |
| SPPB | 35 | 0.19 (−0.13 to 0.52) | 36 | −0.16 (−0.48 to 0.17) | 0.35 (−0.12 to 0.82) | 0.143 |

References
- Tei, R.M.H.; Ramlau-Hansen, C.H.; Plana-Ripoll, O.; Brink, O.; Langdahl, B.L. OFELIA: Prevalence of Osteoporosis in Fragility Fracture Patients. Calcif. Tissue Int. 2019, 104, 102–114. [Google Scholar] [CrossRef] [PubMed]
- Alexiou, K.I.; Roushias, A.; Evaritimidis, S.; Malizos, K.N. Quality of life and psychological consequences in elderly patients after a hip fracture: A review. Clin. Interv. Aging 2018, 13, 143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amarilla-Donoso, F.J.; Roncero-Martin, R.; Lavado-Garcia, J.M.; Toribio-Felipe, R.; Moran-Garcia, J.M.; Lopez-Espuela, F. Quality of life after hip fracture: A 12-month prospective study. PeerJ 2020. [Google Scholar] [CrossRef] [PubMed]
- Perracini, M.R.; Kristensen, M.T.; Cunningham, C.; Sherrington, C. Physiotherapy following fragility fractures. Injury 2018, 49, 1413–1417. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.; Zhu, X.; Zhang, S. Effect of home-based rehabilitation for hip fracture: A meta-analysis of randomized controlled trials. J. Rehabil. Med. 2018, 50, 481–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galea, M.D.F. Telemedicine in Rehabilitation. Phys. Med. Rehabil. Clin. N. Am. 2019, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Shukla, H.; Nair, S.; Thakker, D. Role of telerehabilitation in patients following total knee arthroplasty: Evidence from a systematic literature review and meta-analysis. J. Telemed. Telecare 2017, 23, 339–346. [Google Scholar] [CrossRef]
- Hoogland, J.; Wijnen, A.; Munsterman, T.; Gerritsma, C.L.E.; Dijkstra, B.; Zijlstra, W.P.; Annegarn, J.; Ibarra, F.; Zijlstra, W.; Stevens, M. Feasibility and Patient Experience of a Home-Based Rehabilitation Program Driven by a Tablet App and Mobility Monitoring for Patients After a Total Hip Arthroplasty. JMIR mHealth uHealth 2019, 7, e10342. [Google Scholar] [CrossRef] [Green Version]
- Ariza-Garcia, A.; Arroyo-Morales, M.; Lozano-Lozano, M.; Galiano-Castillo, N.; Postigo-Martin, P.; Cantarero-Villanueva, I. A web-based exercise system (e-cuidatechemo) to counter the side effects of chemotherapy in patients with breast cancer: Randomized controlled trial. J. Med. Internet Res. 2019. [Google Scholar] [CrossRef] [Green Version]
- Cramer, S.C.; Dodakian, L.; Le, V.; See, J.; Augsburger, R.; McKenzie, A.; Zhou, R.J.; Chiu, N.L.; Heckhausen, J.; Cassidy, J.M.; et al. Efficacy of Home-Based Telerehabilitation vs In-Clinic Therapy for Adults after Stroke: A Randomized Clinical Trial. JAMA Neurol. 2019. [Google Scholar] [CrossRef]
- Maddison, R.; Rawstorn, J.C.; Stewart, R.A.H.; Benatar, J.; Whittaker, R.; Rolleston, A.; Jiang, Y.; Gao, L.; Moodie, M.; Warren, I.; et al. Effects and costs of real-time cardiac telerehabilitation: Randomised controlled non-inferiority trial. Heart 2019. [Google Scholar] [CrossRef]
- Ashe, M.C.; Ekegren, C.L.; Chudyk, A.M.; Fleig, L.; Gill, T.K.; Langford, D.; Martin-Martin, L.; Ariza-Vega, P. Telerehabilitation for community-dwelling middle-aged and older adults after musculoskeletal trauma: A systematic review. AIMS Med. Sci. 2018, 5, 316–336. [Google Scholar] [CrossRef]
- Bedra, M.; Finkelstein, J. Feasibility of post-acute hip fracture telerehabilitation in older adults. Stud. Health Technol. Inform. 2015, 210, 469–473. [Google Scholar]
- Kalron, A.; Tawil, H.; Peleg-Shani, S.; Vatine, J.-J. Effect of telerehabilitation on mobility in people after hip surgery: A pilot feasibility study. Int. J. Rehabil. Res. 2018, 41, 244–250. [Google Scholar] [CrossRef]
- Tappen, R.M.; Whitehead, D.; Folden, S.L.; Hall, R. Effect of a Video Intervention on Functional Recovery Following Hip Replacement and Hip Fracture Repair. Rehabil. Nurs. 2003, 28, 148–153. [Google Scholar] [CrossRef]
- Jensen, C.M.; Overgaard, S.; Wiil, U.K.; Clemensen, J. Can Tele-Health Support Self-Care and Empowerment? A Qualitative Study of Hip Fracture Patients’ Experiences With Testing an “App.”. SAGE Open Nurs. 2019. [Google Scholar] [CrossRef] [Green Version]
- Li, C.T.L.; Hung, G.K.N.; Fong, K.N.K.; Gonzalez, P.C.; Wah, S.H.; Tsang, H.W.H. Effects of a home-based occupational therapy telerehabilitation via smartphone for outpatients after hip fracture surgery: A feasibility randomised controlled study. J. Telemed. Telecare 2020. [Google Scholar] [CrossRef]
- Crotty, M.; Killington, M.; van den Berg, M.; Morris, C.; Taylor, A.; Carati, C. Telerehabilitation for older people using off-the-shelf applications: Acceptability and feasibility. J. Telemed. Telecare 2014, 20, 370–376. [Google Scholar] [CrossRef]
- Cottrell, M.A.; Galea, O.A.; O’Leary, S.P.; Hill, A.J.; Russell, T.G. Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 625–638. [Google Scholar] [CrossRef]
- Ariza-Vega, P.; Jiménez-Moleón, J.J.; Kristensen, M.T. Change of residence and functional status within three months and one year following hip fracture surgery. Disabil. Rehabil. 2014, 36, 685–690. [Google Scholar] [CrossRef]
- Kowalski, C.J.; Mrdjenovich, A.J. Patient Preference Clinical Trials: Why and When They Will Sometimes Be Preferred. Perspect. Biol. Med. 2013, 56, 18–35. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Ortiz-Piña, M.; Salas-Fariña, Z.; Mora-Traverso, M.; Martín-Martín, L.; Galiano-Castillo, N.; García-Montes, I.; Cantarero-Villanueva, I.; Fernández-Lao, C.; Arroyo-Morales, M.; Mesa-Ruíz, A.; et al. A home-based tele-rehabilitation protocol for patients with hip fracture called @ctivehip. Res. Nurs. Health 2019, 42, 29–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu-Yahiro, J.A.; Resnick, B.; Orwig, D.; Hicks, G.; Magaziner, J. Design and Implementation of a Home-Based Exercise Program Post-Hip Fracture: The Baltimore Hip Studies Experience. PM R 2009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Asanuma, D.; Momosaki, R. Characteristics of rehabilitation services in high-fim efficienchospitals after hip fracture. J. Med. Investig. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hobart, J.C.; Lamping, D.L.; Freeman, J.A.; Langdon, D.W.; McLellan, D.L.; Greenwood, R.J.; Thompson, A.J. Evidence-based measurement: Which disability scale for neurologic rehabilitation? Neurology 2001, 57, 639–644. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The Timed “ Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Steffen, T.M.; Hacker, T.A.; Mollinger, L. Age- and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and gait speeds. Phys. Ther. 2002, 82, 128–137. [Google Scholar] [CrossRef] [Green Version]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Gómez, J.F.; Curcio, C.-L.; Alvarado, B.; Zunzunegui, M.V.; Guralnik, J. Validity and reliability of the Short Physical Performance Battery (SPPB): A pilot study on mobility in the Colombian Andes. Colomb. Med. 2013, 44, 165–171. [Google Scholar] [CrossRef]
- Daabiss, M. American Society of Anaesthesiologists physical status classification. Indian J. Anaesth. 2011, 55, 111. [Google Scholar] [CrossRef]
- Zidén, L.; Frandin, K.; Kreuter, M. Home rehabilitation after hip fracture. A randomized controlled study on balance confidence, physical function and everyday activities. Clin. Rehabil. 2008, 22, 1019–1033. [Google Scholar] [CrossRef]
- Wallace, D.; Duncan, P.W.; Lai, S.M. Comparison of the responsiveness of the Barthel Index and the Motor Component of the Functional Independence Measure in stroke. J. Clin. Epidemiol. 2002, 55, 922–928. [Google Scholar] [CrossRef]
- Blom, G. Transformations of the binomial, negative binomial, poisson and χ2 distributions. Biometrika 1954, 41, 302–316. [Google Scholar] [CrossRef]
- Sink, K.M.; Espeland, M.A.; Castro, C.M.; Church, T.; Cohen, R.; Dodson, J.A.; Guralnik, J.; Hendrie, H.C.; Jennings, J.; Katula, J.; et al. Effect of a 24-Month Physical Activity Intervention vs Health Education on Cognitive Outcomes in Sedentary Older Adults. JAMA 2015, 314, 781. [Google Scholar] [CrossRef]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013. [Google Scholar] [CrossRef] [Green Version]
- Nakagawa, S.; Cuthill, I.C. Effect size, confidence interval and statistical significance: A practical guide for biologists. Biol. Rev. 2007, 82, 591–605. [Google Scholar] [CrossRef]
- Rocha, S.A.; de Avila, M.A.G.; Bocchi, S.C.M. Influência do cuidador informal na reabilitação do idoso em pós-operatório de fratura de fêmur proximal. Rev. Gaúcha Enferm. 2016, 37, 12. [Google Scholar] [CrossRef] [Green Version]
- Saletti-Cuesta, L.; Tutton, E.; Langstaff, D.; Willett, K. Understanding informal carers’ experiences of caring for older people with a hip fracture: A systematic review of qualitative studies. Disabil. Rehabil. 2018, 40, 740–750. [Google Scholar] [CrossRef] [Green Version]
- Ariza-Vega, P.; Castillo-Pérez, H.; Ortiz-Piña, M.; Ziden, L.; Palomino-Vidal, J.; Ashe, M.C. The Journey of Recovery: Caregivers’ Perspectives From a Hip Fracture Telerehabilitation Clinical Trial. Phys. Ther. 2021. [Google Scholar] [CrossRef]
- Coulter, A.; Oldham, J. Person-centred care: What is it and how do we get there? Futur. Hosp. J. 2016, 3, 114–116. [Google Scholar] [CrossRef]


| Variables | Tele-Rehab. (n = 28) | Control (n = 34) | p |
|---|---|---|---|
| Age (years) | 75.86 ± 5.79 | 80.38 ± 5.54 | 0.003 |
| Weight (kg) | 68.1 ± 9.94 | 69.15 ± 10.21 | 0.708 |
| Height (cm) | 160.88 ± 7.32 | 158.04 ± 8.83 | 0.215 |
| BMI (kg/m2) | 26.38 ± 3.98 | 27.63 ± 3.58 | 0.248 |
| Gender, n (%) | 0.557 | ||
| Men | 8 (28.6%) | 9 (26.5%) | |
| Women | 20 (71.4%) | 27 (73.5%) | |
| Outcomes Basal | |||
| FIM (18–126 points) | 77.75 ± 4.22 | 78.12 ± 6.61 | 0.800 |
| TUG (seconds) | 66.53 ± 36.89 | 99.72 ± 68.82 | 0.027 |
| SPPB (0 to 12 points) | 3.21 ± 1.17 | 2.58 ± 1.46 | 0.072 |
| Outcomes Post-rehab. | |||
| FIM (18–126 points) | 120.54 ± 7.48 | 108.29 ± 14.67 | |
| TUG (seconds) | 12.95 ± 4.94 | 24.38 ± 13.56 | |
| SPPB (0 to 12 points) | 8.36 ± 2.39 | 5.94 ± 3.01 | |
| Confounder | |||
| Type of fracture | 0.123 | ||
| Intracapsular | 15 (53.6%) | 11 (32.3%) | |
| Extracapsular | 13 (46.4%) | 23 (67.7%) |
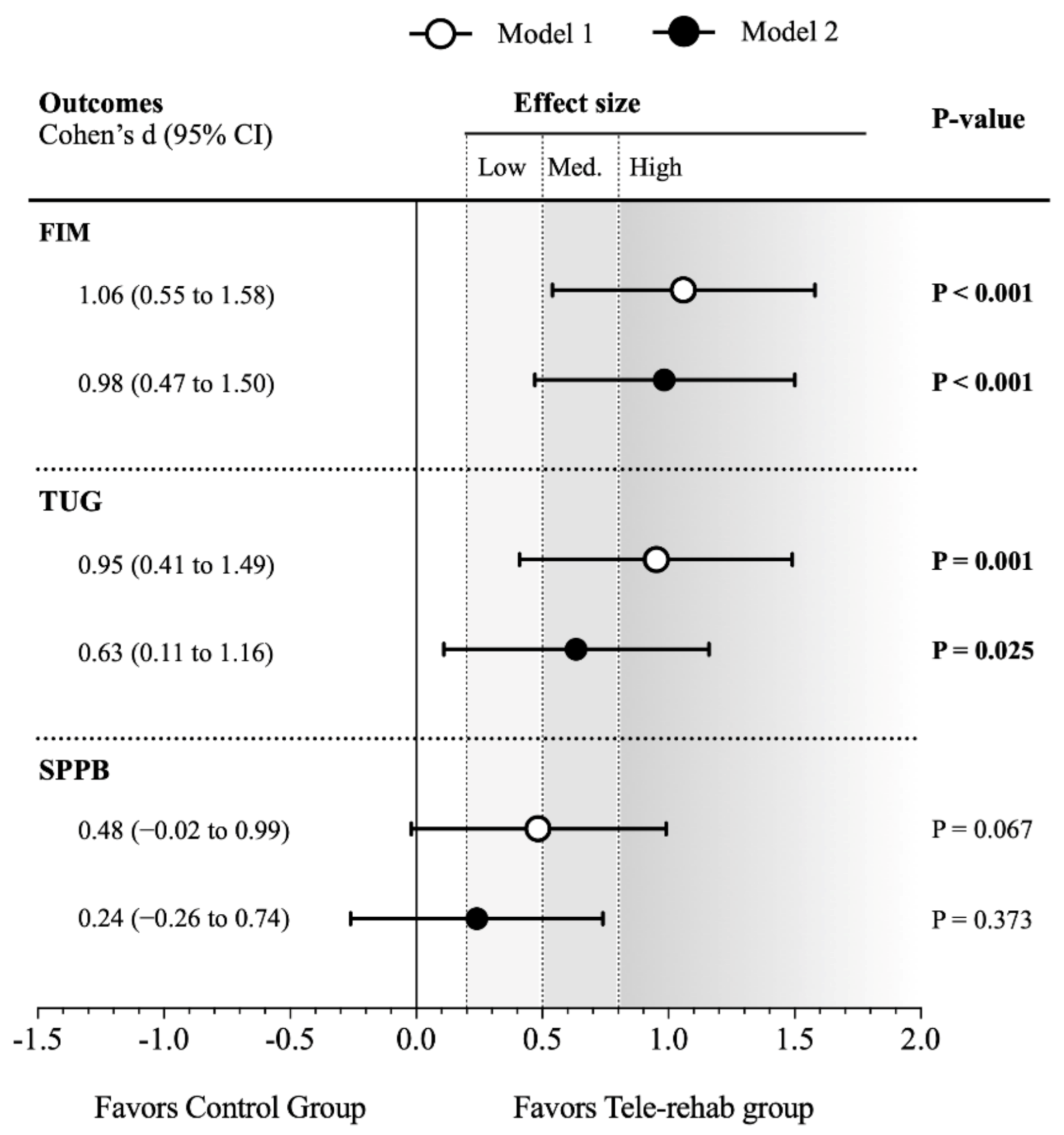
| Statistical Models Outcomes | Tele-Rehabilitation Group | Control Group | Z-Score Differences Tele-Rehab-Control (95% CI) | p | ||
|---|---|---|---|---|---|---|
| N | Z-Score (95% CI) | N | Z-Score (95% CI) | |||
| Model 1 | ||||||
| FIM | 30 | 0.50 (0.18 to 0.82) | 35 | −0.44 (−0.73 to −0.14) | 0.93 (0.49 to 1.37) | <0.001 |
| TUG | 28 | −0.45 (−0.76 to −0.14) | 34 | 0.32 (0.03 to 0.62) | −0.77 (−1.21 to −0.34) | 0.001 |
| SPPB | 30 | 0.33 (−0.03 to 0.69) | 35 | −0.15 (−0.5 to 0.2) | 0.48 (−0.03 to 0.98) | 0.067 |
| Model 2 | ||||||
| FIM | 30 | 0.44 (0.13 to 0.75) | 35 | −0.39 (−0.67 to −0.1) | 0.83 (0.40 to 1.25) | <0.001 |
| TUG | 28 | −0.28 (−0.55 to −0.01) | 34 | 0.17 (−0.09 to 0.43) | −0.45 (−0.84 to −0.06) | 0.025 |
| SPPB | 30 | 0.20 (−0.15 to 0.56) | 35 | −0.03 (−0.38 to 0.32) | 0.24 (−0.29 to 0.76) | 0.373 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortiz-Piña, M.; Molina-Garcia, P.; Femia, P.; Ashe, M.C.; Martín-Martín, L.; Salazar-Graván, S.; Salas-Fariña, Z.; Prieto-Moreno, R.; Castellote-Caballero, Y.; Estevez-Lopez, F.; et al. Effects of Tele-Rehabilitation Compared with Home-Based in-Person Rehabilitation for Older Adult’s Function after Hip Fracture. Int. J. Environ. Res. Public Health 2021, 18, 5493. https://doi.org/10.3390/ijerph18105493
Ortiz-Piña M, Molina-Garcia P, Femia P, Ashe MC, Martín-Martín L, Salazar-Graván S, Salas-Fariña Z, Prieto-Moreno R, Castellote-Caballero Y, Estevez-Lopez F, et al. Effects of Tele-Rehabilitation Compared with Home-Based in-Person Rehabilitation for Older Adult’s Function after Hip Fracture. International Journal of Environmental Research and Public Health. 2021; 18(10):5493. https://doi.org/10.3390/ijerph18105493
Chicago/Turabian StyleOrtiz-Piña, Mariana, Pablo Molina-Garcia, Pedro Femia, Maureen C. Ashe, Lydia Martín-Martín, Susana Salazar-Graván, Zeus Salas-Fariña, Rafael Prieto-Moreno, Yolanda Castellote-Caballero, Fernando Estevez-Lopez, and et al. 2021. "Effects of Tele-Rehabilitation Compared with Home-Based in-Person Rehabilitation for Older Adult’s Function after Hip Fracture" International Journal of Environmental Research and Public Health 18, no. 10: 5493. https://doi.org/10.3390/ijerph18105493
APA StyleOrtiz-Piña, M., Molina-Garcia, P., Femia, P., Ashe, M. C., Martín-Martín, L., Salazar-Graván, S., Salas-Fariña, Z., Prieto-Moreno, R., Castellote-Caballero, Y., Estevez-Lopez, F., & Ariza-Vega, P. (2021). Effects of Tele-Rehabilitation Compared with Home-Based in-Person Rehabilitation for Older Adult’s Function after Hip Fracture. International Journal of Environmental Research and Public Health, 18(10), 5493. https://doi.org/10.3390/ijerph18105493