
Evaluation of a Post-Operative Rehabilitation Program in Patients Undergoing Laparoscopic Colorectal Cancer Surgery: A Pilot Study

 ,
, 
 ,
,
Abstract
:1. Introduction
1.1. The Primary Objective of the Study
1.2. Secondary Objectives of the Study
2. Materials & Methods
2.1. Study Design
2.2. Eligibility Criteria and Enrollment
- age 40–80;
- histologically confirmed diagnosis of primary colon or rectal neoplasm;
- physically inactive patients (duration of physical activity <150 min per week);
- Karnofsky Perfomance Status (KPS) > 60 and able to walk ≥ 60 m. The Karnosky Performance Status is one of the most used validated scales to define the functional status of the cancer patient. A KPS ≤ 60 indicates the inability to work and severe difficulty in carrying out activities of daily living and personal care of the cancer patient [17].
- laparotomic surgery;
- pregnancy;
- relapsing cancer or metastasic cancer;
- simultaneous diagnosis of other neoplasms;
- cancer treatment in the 5 years before recruitment;
- severe cardiovascular, pulmonary, orthopedic, neurological pathologies;
- cognitive impairment;
- regular use of immunosuppressive drugs.
2.3. Intervention
2.3.1. Physical Exercise
2.3.2. Aerobic Exercise
2.3.3. Muscle-Strengthening Exercise
2.3.4. Control Group
2.4. Outcome Measures
2.4.1. Primary Outcome
2.4.2. Secondary Outcomes
- position with feet together for 10;
- semi-tandem position for 10 s (big toe on the side of the heel);
- tandem position for 10 s (big toe behind the heel).
- Handgrip Strength test: Muscle strength was assessed by the Handgrip Strength test. The measure of handgrip strength is evaluated using a handheld dynamometer, equipped with a spring set of 20 kg capacity. The participants were seated in a chair without armrests with the elbow flexed in a 90° angle position and were asked to squeeze the handgrip instrument three times shortly maximally with one-minute rest between measurements. Once the grip width was adjusted, the subject held the dynamometer while the operator encouraged him or her to tighten with the maximum possible force. The value was then recorded. The final value of grip strength is the arithmetical mean of the three values. The measure of handgrip strength is used in numerous studies, conducted in different populations. Upper limb strength is strictly correlated with lower extremities muscle strength and calf sectional area [32,33,34,35,36]. Moreover, baseline handgrip strength has a linear relationship with disability in ADL [37].
- Skeletal Muscle Mass Index (SMI): muscle mass was estimated by calculating the Skeletal Muscle Mass Index (SMI) using a bioimpedance meter. According to the European Society for Clinical Nutrition and Metabolism (ESPEN), bioelectrical impedance analysis (BIA) is considered a quick, easy to perform, and non-invasive method to estimate body composition [38]. BIA is currently considered a widespread and validated body composition assessment technique in various clinical contexts [39,40]. The muscle mass index (SMI) is calculated as the ratio of skeletal muscle mass (SM) and the square of height (h2) (SM/h2). The European Working Group on Sarcopenia in Older People (EWGSOP) [41] defines BIA as a “good portable alternative” method; due to its affordability, portability, and ease of execution, it is recommended in the systematic and repeated assessment of muscle mass in clinical practice.
- The Phase Angle (PhA): nutritional status is assessed by calculating the Phase Angle (PhA). It is a value obtained from the reactance (Xc) and the resistance (R) parameters, assessed during BIA. PhA is calculated using the formula: arc tan (Xc/R) × (180/π). PhA is considered a valuable indicator of cellular health and integrity [42]. Thus, PhA is considered a prognostic marker in several clinical conditions, including cancer, as it represents either cell death or malnutrition, which are characterized by changes in cellular membrane integrity [43,44].
- The Italian version of the Hospital Anxiety and Depression Scale (HADS): Anxiety and depression were assessed using the Italian version of the Hospital Anxiety and Depression Scale (HADS) [45]. The questionnaire consists of 14 items, with each score ranging from 0 to 21. A value higher than 8 suggests the presence of a mood disorder [46].
- Post-operative complications: The surgical complications were recorded. They were classified according to their severity using the Dindo–Clavien Classification. Grade I indicates a complication that requires management in the patient’s bed; grade II a drug treatment; grade III a radiological, endoscopic, or surgical treatment; and grade IV intensive care [49].
3. Statistical Methods
Statistical Analysis
4. Results
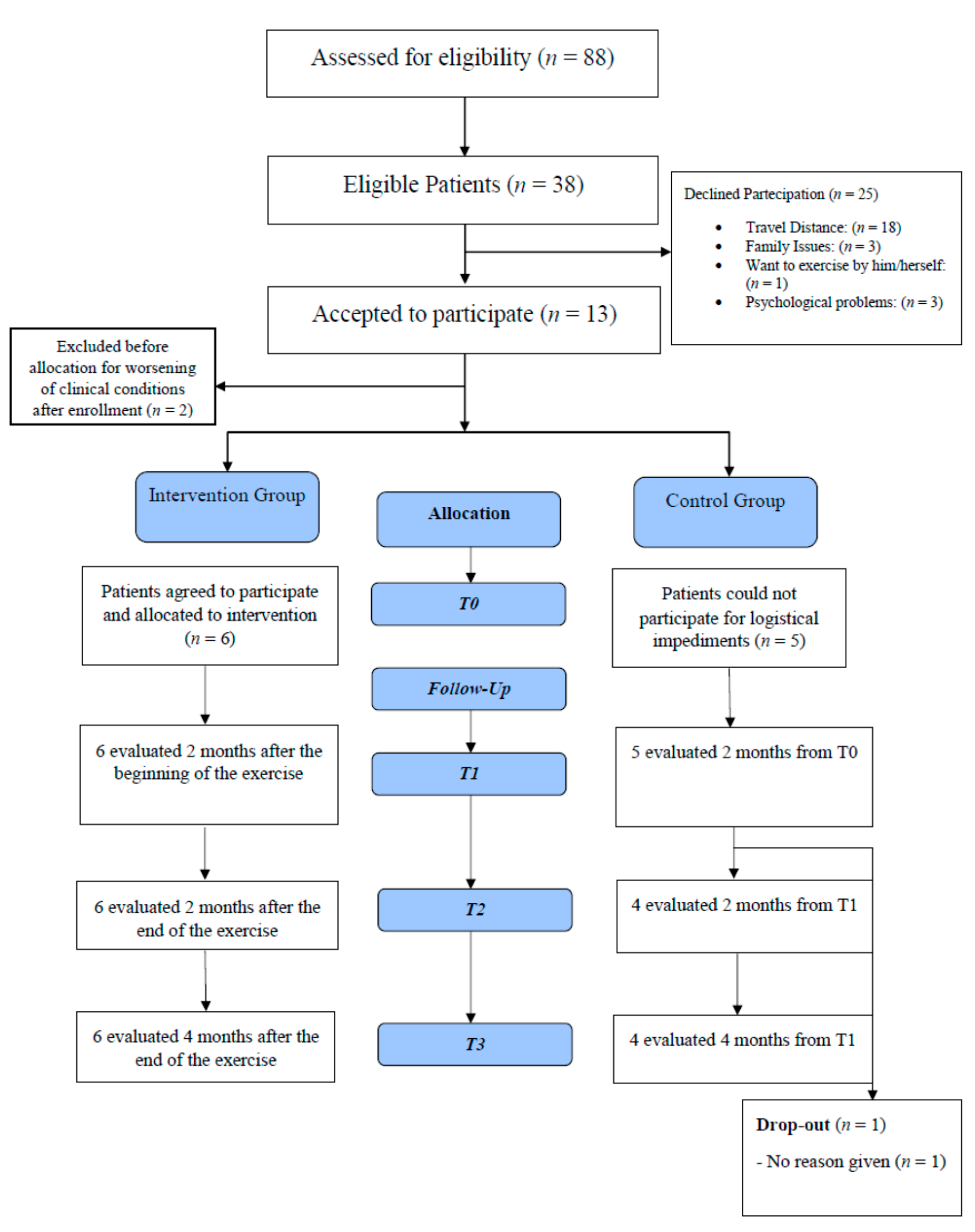
4.1. Reasons for the Refusal of Exercise Training
4.2. Demographic, Clinicopathologic, and Operative Variables
4.3. Clinical Results
4.3.1. Primary Objective
4.3.2. Secondary Objectives
4.4. Feasibility
4.5. Safety
4.6. Post-Surgical Complications
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Devin, J.; Sax, A.; Hughes, G.; Jenkins, D.; Aitken, J.; Chambers, S.; Dunn, J.C.; Bolam, K.A.; Skinner, T.L. The influence of high-intensity compared with moderate-intensity exercise training on cardiorespiratory fitness and body composition in colorectal cancer survivors: A randomized control trial. J. Cancer Surviv. 2016, 10, 467–479. [Google Scholar] [CrossRef]
- Cox, M.C.; Nusca, S.M.; Di Landro, F.; Marsilli, G.; Stella, G.; Sigona, M.; Ponzelli, F.; Passerini Desideri, J.; Di Gregorio, F.; Santoboni, F.; et al. Exercise training (ET) in adult and elderly patients receiving anti-lymphoma treatments is feasible and may improve the provision of care. Leuk. Lymphoma 2021, 62, 560–570. [Google Scholar] [CrossRef]
- Paolucci, T.; Bernetti, A.; Paoloni, M.; Capobianco, S.V.; Bai, A.V.; Rotundi, M.; Damiani, C.; Santilli, V. Therapeutic Alliance in a Single Versus Group Rehabilitative Setting After Breast Cancer Surgery: Psychological Profile and Performance Rehabilitation. Biores Open Access 2019, 8, 101–110. [Google Scholar] [CrossRef] [Green Version]
- Karkou, V.; Dudley-Swarbrick, I.; Starkey, J.; Parsons, A.; Aithal, S.; Omylinska-Thurston, J.; Verkooijen, H.M.; van den Boogaard, R.; Dochevska, Y.; Djobova, S.; et al. Dancing With Health: Quality of Life and Physical Improvements From an EU Collaborative Dance Programme With Women Following Breast Cancer Treatment. Front. Psychol. 2021, 12, 635578. [Google Scholar] [CrossRef]
- Cerulli, C.; Parisi, A.; Sacchetti, M.; Tranchita, E.; Murri, A.; Minganti, C.; Ciminelli, E.; Bellofiore, L.; Grazioli, E. Dancing with health: A new dance protocol to improve the quality of life of breast cancer survivors. Medicina Sport. 2019, 72, 295–304. [Google Scholar]
- Speck, R.M.; Courneya, K.S.; Mâsse, L.C.; Duval, S.; Schmitz Kathryn, H. An update of controlled physical activity trials in cancer survivors: A systematic review and meta-analysis. J. Cancer Surviv. 2010, 4, 87–100. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Ervik, M.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Globocan 2012 V1.0, Cancer Incidence and Mortality Worldwide: Iarc Cancerbase no. 11; International Agency for Research on Cancer: Lyon, France, 2013. [Google Scholar]
- AIOM (Associazione Italiana di Oncologia Medica); AIRTUM (Associazione Italiana dei Registri Tumori); Fondazione AIOM; PASSI d’Argento (sistema di sorveglianza dell’Istituto Superiore di Sanità sullo stato di salute della popolazione); SIAPEC-IAP (Società Italiana di Anatomia Patologica e Citodiagnostica). I Numeri del Cancro in Italia, 9th ed.; Intermedia Editore: Brescia, Italy, 2019. [Google Scholar]
- Lawrence, V.A.; Hazuda, H.P.; Cornell, J.E.; Pederson, T.; Bradshaw, P.T.; Mulrow, C.D.; Pederson, T.; Bradshaw, P.T.; Mulrow, C.D.; Page, C.P. Functional independence after major abdominal surgery in the elderly. J. Am. Coll. Surg. 2004, 199, 762–772. [Google Scholar] [CrossRef] [PubMed]
- Lassen, K.; Soop, M.; Nygren, J.; Cox, B.W.; Hendry, P.O.; Spies, C.; von Meyenfeldt, M.F.; Fearon, K.C.; Revhaug, A.; von Meyenfeldt, M.F.; et al. Consensus review of optimal perioperative care in colorectal surgery. Enhanced recovery after surgery (ERAS) group recommendations. Arch. Surg. 2009, 144, 961–969. [Google Scholar] [CrossRef]
- McGettigan, M.; Cardwell, C.R.; Cantwell, M.M.; Tully, M.A. Physical activity interventions for disease-related physical and mental health during and following treatment in people with non-advanced colorectal cancer. Cochrane Database Syst. Rev. 2020, 5, CD012864. [Google Scholar] [CrossRef] [Green Version]
- Mascherini, G.; Ringressi, M.N.; Castizo-Olier, J.; Badicu, G.; Irurtia, A.; Stefani, L.; Galanti, G.; Taddei, A. Preliminary Results of an Exercise Program After Laparoscopic Resective Colorectal Cancer Surgery in Non-Metastatic Adenocarcinoma: A Pilot Study of a Randomized Control Trial. Medicina 2020, 56, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Min, J.H.; Ahn, K.Y.; Park, H.; Cho, W.; Jung, H.J.; Kim, N.K.; Jeon, J.Y. The Effect of Post-operative Exercise in Colorectal Cancer Patients: A Pilot Randomized Controlled Trial (RCT) Study. Asian Oncol. Nurs. 2017, 17, 29. [Google Scholar] [CrossRef]
- Awasthi, R.; Minnella, E.M.; Ferreira, V.; Ramanakumar, A.V.; Scheede-Bergdahl, C.; Carli, F. Supervised exercise training with multimodal pre-habilitation leads to earlier functional recovery following colorectal cancer resection. Acta Anaesthesiol. Scand. 2019, 63, 461–467. [Google Scholar] [CrossRef]
- Gillis, C.; Li, C.; Lee, L.; Awasthi, R.; Augustin, B.; Gamsa, A.; Liberman, A.S.; Stein, B.; Charlebois, P.; Feldman, L.S.; et al. Prehabilitation versus rehabilitation: A randomized control trial in patients undergoing colorectal resection for cancer. Anesthesiology 2014, 121, 937–947. [Google Scholar] [CrossRef] [PubMed]
- Human, D. Declaration of Helsinki. Lancet 2001, 236, 357. [Google Scholar] [CrossRef]
- Conill, C.; Verger, E.; Salamero, M. Performance status assessment in cancer patients. Cancer 1990, 65, 1864–1866. [Google Scholar] [CrossRef]
- Schmitz, K.H.; Courneya, K.S.; Matthews, C.; emark-Wahnefried, W.; Galvão, D.A.; Pinto, B.M.; Irwin, M.L.; Wolin, K.Y.; Segal, R.J.; Lucia, A.; et al. American College of Sports Medicine roundtable on exercise guidelines for cancer survivors. Med. Sci. Sports Exerc. 2010, 42, 1409–1426. [Google Scholar] [CrossRef] [PubMed]
- Canadian Society for Exercise Physiology. Canadian Physical Activity Guidelines; Canadian Society for Exercise Physiology: Ottawa, Canada, 2011. [Google Scholar]
- van Waart, H.; Stuiver, M.M.; van Harten, W.H.; Geleijn, E.; Kieffer, J.M.; Buffart, L.M.; de Maaker-Berkhof, M.; Boven, E.; Schrama, J.; Geenen, M.M.; et al. Effect of Low-Intensity Physical Activity and Moderate- to High-Intensity Physical Exercise During Adjuvant Chemotherapy on Physical Fitness, Fatigue, and Chemotherapy Completion Rates: Results of the PACES Randomized Clinical Trial. J. Clin. Oncol. 2015, 33, 1918–1927. [Google Scholar] [CrossRef] [Green Version]
- van Vulpen, J.K.; Siersema, P.D.; van Hillegersberg, R.; Nieuwenhuijzen, G.A.P.; Kouwenhoven, E.A.; Groenendijk, R.P.R.; van der Peet, D.L.; Hazebroek, E.J.; Rosman, C.; Schippers, C.C.G.; et al. Physical ExeRcise Following Esophageal Cancer Treatment (PERFECT) study: Design of a randomized controlled trial. BMC Cancer 2017, 17, 552. [Google Scholar] [CrossRef] [Green Version]
- Courneya, K.S.; Friedenreich, C.M.; Quinney, H.A.; Fields, A.L.A.; Jones, L.W.; Fairey, A.S. A Randomized Trial of Exercise and Quality of Life in Colorectal Cancer Survivors. Eur. J. Cancer Care 2003, 12, 347–357. [Google Scholar] [CrossRef]
- Karvonen, M.J. The effects of training on heart rate: A longitudinal study. Ann. Med. Exp. Biol. Fenn. 1957, 35, 307–315. [Google Scholar]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Mayhew, J.L.; Prinster, J.L.; Ware, J.S.; Zimmer, D.L.; Arabas, J.R.; Bemben, M.G. Muscular endurance repetitions to predict bench press strength in men of different training levels. J. Sports Med. Phys. Fit. 1995, 35, 108–113. [Google Scholar]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European Organization for Research and Treatment of cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Unver, B.; Kahraman, T.; Kalkan, S.; Yuksel, E.; Karatosun, V. Reliability of the six-minute walk test after total hip arthroplasty. Hip. Int. 2013, 23, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Moriello, C.; Mayo, N.E.; Feldman, L.; Carli, F. Validating the six-minute walk test as a measure of recovery after elective colon resection surgery. Arch. Phys. Med. Rehabil. 2008, 89, 1083–1089. [Google Scholar] [CrossRef]
- Pecorelli, N.; Fiore, J.F., Jr.; Gillis, C.; Awasthi, R.; Mappin-Kasirer, B.; Niculiseanu, P.; Fried, G.M.; Carli, F.; Feldman, L.S. The six-minute walk test as a measure of postoperative recovery after colorectal resection: Further examination of its measurement properties. Surg. Endosc. 2016, 30, 2199–2206. [Google Scholar] [CrossRef]
- Laboratories ATSCoPSfCPF. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- Luna-Heredia, E.; Martın-Pena, G.; Ruiz-Galiana, J. Handgrip dynamometry in healthy adults. Clin. Nutr. 2005, 24, 250–258. [Google Scholar] [CrossRef]
- Bohannon, R.W. Hand-grip dynamometry predicts future outcomes in aging adults. J. Geriatr. Phys. 2007, 30, 28–30. [Google Scholar] [CrossRef] [Green Version]
- Budziareck, M.B.; Roig Pureza Duarte, R.; Barbosa-Silva, M.C.G. Reference values and determinants for handgrip strength in healthy subject. Clin. Nutr. 2008, 27, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Schlussel, M.M.; dos Anjos, L.A.; Teixeira Leite de Vasconcellos, M.; Kac, G. Reference values of handgrip dynamometry of healthy adults: A population-based study. Clin. Nutr. 2008, 27, 601607. [Google Scholar] [CrossRef] [PubMed]
- Cespedes Feliciano, E.; Chen, W.Y. Clinical implications of low skeletal muscle mass in early-stage breast and colorectal cancer. Proc. Nutr. Soc. 2018, 77, 382–387. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Kuchnia, A.; Earthman, C.; Teigen, L.; Cole, A.; Mourtzakis, M.; Paris, M.; Looijaard, W.; Weijs, P.; Oudemans-van Straaten, H.; Beilman, G. Evaluation of bioelectrical impedance analysis in critically ill patients: Results of a multicenter prospective study. JPEN J. Parenter. Enteral Nutr. 2017, 41, 1131–1138. [Google Scholar] [CrossRef]
- Dehghan, M.; Merchant, A.T. Is bioelectrical impedance accurate for use in large epidemiological studies? Nutr. J. 2008, 7, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Castizo-Olier, J.; Irurtia, A.; Jemni, M.; Carrasco-Marginet, M.; Fernandez-Garcia, R.; Rodriguez, F.A. Bioelectrical impedance vector analysis (BIVA) in sport and exercise: Systematic review and future perspectives. PLoS ONE 2018, 13, e0197957. [Google Scholar] [CrossRef]
- Rinninella, E.; Ruggiero, A.; Maurizi, P.; Triarico, S.; Cintoni, M.; Mele, M.C. Clinical tools to assess nutritional risk and malnutrition in hospitalized children and adolescents. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2690–2701. [Google Scholar]
- Gupta, D.; Lammersfeld, C.A.; Burrows, J.L.; Dahlk, S.L.; Vashi, P.G.; Grutsch, J.F.; Hoffman, S.; Lis, C.G. Bioelectrical impedance phase angle in clinical practice: Implications for prognosis in advanced colorectal cancer. Am. J. Clin. Nutr. 2004, 80, 1634–1638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costantini, M.; Musso, M.; Viterbori, P.; Bonci, F.; Del Mastro, L.; Garrone, O.; Venturini, M.; Morasso, G. Detecting psychological distress in cancer patients: Validity of the Italian version of the Hospital Anxiety and Depression Scale. Supportive Care Cancer 1999, 7, 121–127. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Grandner, M.A.; Kripke, D.F.; Yoon, I.Y.; Youngstedt, S.D. Criterion validity of the Pittsburgh Sleep Quality Index: Investigation in a non-clinical sample. Sleep Biol. Rhythms 2006, 4, 129–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Labianca, R.; Nordlinger, B.; Beretta, G.D.; Mosconi, S.; Mandalà, M.; Cervantes, A.; Arnold, D.; ESMO Guidelines Working Group. ESMO Guidelines Working Group Early colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24, vi64–vi72. [Google Scholar] [CrossRef]
- Shim, Y.J.; Kim, H.J.; Oh, S.C.; Lee, S.I.; Choi, S.W. Exercise during adjuvant treatment for colorectal cancer: Treatment completion, treatment-related toxicities, body composition, and serum level of adipokines. Cancer Manag. Res. 2019, 11, 5403–5412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marventano, S.; Forjaz, M.J.; Grosso, G.; Mistretta, A.; Giorgianni, G.; Platania, A.; Mistretta, A.; Giorgianni, G.; Platania, A.; Gangi, S.; et al. Health related quality of life in colorectal cancer patients: State of the art. BMC Surg. 2013, 13 (Suppl. 2), 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popovic, M.; Nguyen, J.; Chen, E.; Di Giovanni, J.; Zeng, L.; Chow, E. Comparison of the EORTC QLQ-BM22 and the FACT-BP for assessment of quality of life in cancer patients with bone metastases. Expert Rev. Pharmacoecon. Outcomes Res. 2012, 12, 213–219. [Google Scholar] [CrossRef]
- Gotay, C.C. Assessing cancer-related quality of life across a spectrum of applications. J. Natl. Cancer Inst. Monogr. 2004, 33, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Fong, D.Y.; Ho, J.W.; Hui, B.P.; Lee, A.M.; Macfarlane, D.J.; Leung, S.S.; Cerin, E.; Chan, W.Y.; Leung, I.P.; Lam, S.H. Physical activity for cancer survivors: Meta-analysis of randomised controlled trials. BMJ 2012, 344, e70. [Google Scholar] [CrossRef] [Green Version]
- Myers, J.S.; Erickson, K.I.; Sereika, S.M.; Bender, C.M. Exercise as an Intervention to Mitigate Decreased Cognitive Function From Cancer and Cancer Treatment: An Integrative Review. Cancer Nurs. 2018, 41, 327–343. [Google Scholar] [CrossRef]
- Galvão, D.A.; Taaffe, D.R.; Spry, N.; Joseph, D.; Newton, R.U. Combined resistance and aerobic exercise program reverses muscle loss in men undergoing androgen suppression therapy for prostate cancer without bone metastases: A randomized controlled trial. J. Clin. Oncol. 2010, 28, 340–3477. [Google Scholar] [CrossRef] [Green Version]
- Oechsle, K.; Wais, M.C.; Vehling, S.; Bokemeyer, C.; Mehnert, A. Relationship between symptom burden, distress, and sense of dignity in terminally ill cancer patients. J. Pain Symptom Manag. 2014, 48, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Vardy, J.; Dhillon, H.M.; Pond, G.R.; Rourke, S.B.; Xu, W.; Dodd, A.; Renton, C.; Park, A.; Bekele, T.; Ringash, J.; et al. Cognitive function and fatigue after diagnosis of colorectal cancer. Ann. Oncol. 2014, 25, 2404–2412. [Google Scholar] [CrossRef]
- Stone, P.C.; Minto, O. Cancer-related fatigue. Eur. J. Cancer 2008, 44, 1097–1104. [Google Scholar] [CrossRef]
- Curt, G.A.; Breibart, W.; Cella, D.; Groopman, J.E.; Horning, S.J.; Itri, L.M.; Johnson, D.H.; Miaskowski, C.; Scherr, S.L.; Portenoy, R.K.; et al. Impact of cancer-related fatigue on the lives of patients: New findings from the fatigue coalition. Oncologist 2000, 5, 353–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meneses-Echávez, J.F.; González-Jiménez, E.; Ramírez-Vélez, R. Effects of Supervised Multimodal Exercise Interventions on Cancer-Related Fatigue: Systematic Review and Meta-Analysis of Randomized Controlled Trials. BioMed Res. Int. 2015, 2015, 328636. [Google Scholar] [CrossRef]
- Ross, R.; Blair, S.N.; Arena, R.; Church, T.S.; Després, J.P.; Franklin, B.A.; Church, T.S.; Després, J.P.; Franklin, B.A.; Haskell, W.L.; et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e653–e699. [Google Scholar] [CrossRef] [PubMed]
- Ammitzbøll, G.; Kjær, K.T.; Johansen, C.; Lanng, C.; Wreford Andersen, E.; Kroman, N.; Zerahn, B.; Hyldegaard, O.; Envold Bidstrup, P.; Oksbjerg Dalton, S. Effect of progressive resistance training on health-related quality of life in the first year after breast cancer surgery—results from a randomized controlled trial. Acta Oncol. 2019, 58, 665–672. [Google Scholar] [CrossRef] [Green Version]
- van Waart, H.; Stuiver, M.M.; van Harten, W.H.; Geleijn, E.; de Maaker-Berkhof, M.; Schrama, J.; Geleijn, E.; de Maaker-Berkhof, M.; Schrama, J.; Geenen, M.M.; et al. Recruitment to and pilot results of the PACES randomized trial of physical exercise during adjuvant chemotherapy for colon cancer. Int. J. Colorectal. Dis. 2018, 33, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Segal, R.J.; Reid, R.D.; Courneya, K.S.; Sigal, R.J.; Kenny, G.P.; Prud’Homme, D.G.; Sigal, R.J.; Kenny, G.P.; Prud’Homme, D.G.; Malone, S.C.; et al. Randomized controlled trial of resistance or aerobic exercise in men receiving radiation therapy for prostate cancer. J. Clin. Oncol. 2009, 27, 344–351. [Google Scholar] [CrossRef] [Green Version]
- Daley, A.J.; Crank, H.; Mutrie, N.; Saxton, J.M.; Coleman, R. Randomised trial of exercise therapy in women treated for breast cancer. J. Clin. Oncol. 2007, 25, 1713–1721. [Google Scholar] [CrossRef]
- Courneya, K.S.; Sellar, C.M.; Stevinson, C.; McNeely, M.L.; Peddle, C.J.; Friedenreich, C.M.; Tankel, K.; Basi, S.; Chua, N.; Mazurek, A.; et al. Randomized controlled trial of the effects of aerobic exercise on physical functioning and quality of life in lymphoma patients. J. Clin. Oncol. 2009, 27, 4605–4612. [Google Scholar] [CrossRef] [Green Version]
- Balducci, S.; D’Errico, V.; Haxhi, J.; Sacchetti, M.; Orlando, G.; Cardelli, P.; Vitale, M.; Bollanti, L.; Conti, F.; Zanuso, S.; et al. Effect of a behavioral intervention strategy on sustained change in physical activity and sedentary behavior in patients with type 2 diabetes: The IDES_2 randomized clinical trial. JAMA 2019, 321, 880–890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiskemann, J.; Dreger, P.; Schwerdtfeger, R.; Bondong, A.; Huber, G.; Kleindienst, N.; Ulrich, C.M.; Bohus, M. Effects of a partly self-administered exercise program before, during, and after allogeneic stem cell transplantation. Blood 2011, 117, 2604–2613. [Google Scholar] [CrossRef]
- Persoon, S.; ChinAPaw, M.J.M.; Buffart, L.M.; Liu, R.D.K.; Wijermans, P.; Koene, H.R.; Minnema, M.C.; Lugtenburg, P.J.; Marijt, E.W.A.; Brug, J. Randomized controlled trial on the effects of a supervised high intensity exercise program in patients with a hematologic malignancy treated with autologous stem cell transplantation: Results from the EXIST study. PLoS ONE 2017, 12, e0181313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiskemann, J.; Kuehl, R.; Dreger, P.; Schwerdtfeger, R.; Huber, G.; Ulrich, C.M.; Jaeger, D.; Bohus, M. Efficacy of exercise training in SCT patients--who benefits most? Bone Marrow Transpl. 2014, 49, 443–448. [Google Scholar] [CrossRef] [Green Version]
- Northgraves, M.J.; Arunachalam, L.; Madden, L.A.; Marshall, P.; Hartley, J.E.; MacFie, J.; Vince, R.V. Feasibility of a novel exercise prehabilitation programme in patients scheduled for elective colorectal surgery: A feasibility randomised controlled trial. Support Care Cancer 2020, 28, 3197–3206. [Google Scholar] [CrossRef] [Green Version]
- Agasi-Idenburg, C.S.; Zuilen, M.K.; Westerman, M.J.; Punt, C.J.A.; Aaronson, N.K.; Stuiver, M.M. “I am busy surviving”—Views about physical exercise in older adults scheduled for colorectal cancer surgery. J. Geriatr. Oncol. 2020, 11, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Carli, F.; Charlebois, P.; Stein, B.; Feldman, L.; Zavorsky, G.; Kim, D.J.; Scott, S. Randomized clinical trial of prehabilitation in colorectal surgery. BJS 2010, 97, 1187–1197. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Carli, F.; Lee, L.; Charlebois, P.; Stein, B.; Liberman, A.S.; Kaneva, P.; Augustin, B.; Wongyingsinn, M.; Gamsa, A. Impact of a trimodal prehabilitation program on functional recovery after colorectal cancer surgery: A pilot study. Surg. Endosc. 2013, 27, 1072–1082. [Google Scholar] [CrossRef] [PubMed]
- Carli, F.; Zavorsky, G.S. Optimizing functional exercise capacity in the elderly surgical population. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 23–32. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | IG (n = 6) | CG (n = 5) | p-Value |
|---|---|---|---|
| Age-(median, range) | 63.5 (43.0–80.0) | 73.0 (51.0–80.0) | 0.580 |
| Sex-n. (%) | |||
| Male | 5 (83.3) | 2(33.3) | |
| Female | 1 (16.7) | 3 (66.7) | |
| BMI-(median, range) | 21.4 (17.2–25.7) | 24.0 (22.0–41.4) | 0.200 |
| KPS (median, range) | 80.0 (70.0–80.0) | 80.0 (70.0–80.0) | 0.540 |
| Neoplasm type-n. (%) | |||
| Colon cancer | 5 (83.3) | 3 (66.7) | |
| Rectal cancer | 1 (16.7) | 2 (33.3) | |
| TNM Cancer stage-n. (%) | |||
| Stage IIA | 1 (16.7) | 1 (20.0) | |
| Stage IIB | 2 (33.3) | 1 (20.0) | |
| Stage IIIB | 3 (50.0) | 3 (60.0) | |
| Type of resection-n. (%) | |||
| Colon * | 5 (83.3) | 3 (66.7) | |
| Rectum ** | 1 (16.7) | 2 (33.3) | |
| New Stoma-n. (%) | 0 (0.0) | 0 (0.0) | |
| Chemotherapy-n. (%) | 6 (100.0) | 5 (100.0) | |
| EORTC QLQ-C30-(median, range) | |||
| QL2 | 50.0 (16.7–83.3) | 58.0 (50.0–83.3) | 0.910 |
| PF2 | 93 (60.0–100.0) | 90.0 (87.0–93.0) | 0.733 |
| RF2 | 66.5 (33.0–100.0) | 67.0 (50.0–100.0) | 0.692 |
| EF | 79.5 (42.0–93.0) | 75.0 (57.0–83.0) | 0.580 |
| CF | 100.0 (83.0–100.0) | 83.3 (83.0–84.0) | 0.442 |
| SF | 67.0 (33.0–83.0) | 84.0 (66.6–100.0) | 0.443 |
| FA | 38.8 (0.0–66.7) | 33.3 (22.0–53.3) | 0.854 |
| NV | 0.0 (0.0–50.0) | 0.0 (0.0–16.7) | 0.560 |
| PA | 16.7 (0.0–66.7) | 0.0 (0.0–33.3) | 0.561 |
| DY | 0.0 (0.0–33.3) | 0.0 (0.0–33.3) | 0.892 |
| SL | 33.3 (0.0–66.7) | 0.0 (0.0–33.3) | 0.609 |
| AP | 33.4 (0.0–100.0) | 33.3 (0.0–66.6) | 0.564 |
| CO | 16.7 (0.0–66.7) | 0.0 (0.0–33.3) | 0.242 |
| DI | 16.7 (0.0–33.3) | 0.0 (0.0–33.3) | 0.326 |
| FI | 0.0 (0.0–33.3) | 0.0 (0.0–33.3) | 0.892 |
| EORTC QLQ-C30 | T1 Group IG | T1 Group CG | p-Value |
|---|---|---|---|
| QL2 | 70.9 (25.0–100.0) | 62.5 (41.7–66.7) | 0.330 |
| PF2 | 96.5 (86.7–100.0) | 83.4 (60.0–87.0) | 0.030 * |
| RF2 | 92.0 (50.0–100.0) | 83.3 (83.0–84.0.) | 0.228 |
| EF | 87.5 (58.0–100.0) | 75.0 (58.3–75.0) | 0.249 |
| CF | 100.0 (100.0–100.0) | 74.8 (66.6–100.0) | 0.018 * |
| SF | 68.5 (50.0–100.0) | 83.3 (50.0–100.0) | 0.912 |
| FA | 22.8 (0.0–33.3) | 55.6 (33.3–66.7) | 0.017 * |
| NV | 0.0 (0.0–16.6) | 0.0 (0.0–0.0) | 0.414 |
| PA | 0.0 (0.0–33.3) | 8.4 (0.0–16.7) | 0.807 |
| DY | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 1000 |
| SL | 16.7 (0.0–66.7) | 50.0 (0.0–66.7) | 0.309 |
| AP | 0.0 (0.0–33.3) | 0.0 (0.0–33.3) | 0.759 |
| CO | 0.0 (0.0–66.7) | 16.7 (0.0–33.3) | 0.429 |
| DI | 0.0 (0.0–33.3) | 0.0 (0.0–33.3) | 0.789 |
| FI | 0.0 (0.0–0.0) | 0.0 (0.0–33.3) | 0.221 |
| EORTC QLQ-C30 | T2 Group IG | T2 Group CG | p-Value |
|---|---|---|---|
| (Median, Range) | (Median, Range) | ||
| QL2 | 87.5 (75.0–91.7) | 75.0 (66.7–83.3) | 0.134 |
| PF2 | 100.0 (93.3–100.0) | 82.0 (73.3–87.0) | 0.018 * |
| RF2 | 100.0 (100.0–100.0) | 100.0 (100.0–100.0) | 1.000 |
| EF | 95.8 (66.7–100.0) | 91.7 (75.0–100.0) | 0.762 |
| CF | 100.0 (100.0–100.0) | 100.0 (100.0–100.0) | 1.000 |
| SF | 91.7 (83.3–100.0) | 92.5 (83.0–100.0) | 1.000 |
| FA | 5.5 (0.0–11.0) | 19.5 (11.0–22.2) | 0.045 * |
| NV | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 1.000 |
| PA | 0.0 (0.0–33.3) | 0.0 (0.0–16.7) | 0.850 |
| DY | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 1.000 |
| SL | 0.0 (0.0–33.3) | 0.0 (0.0–33.3) | 1.000 |
| AP | 0.0 (0.0–0.0) | 0.0 (0.0–33.3) | 0.317 |
| CO | 0.0 (0.0–33.3) | 0.0 (0.0–33.3) | 1.000 |
| DI | 0.0 (0.0–33.3) | 0.0 (0.0–33.3) | 1.000 |
| FI | 0.0 (0.0–0.0) | 0.0 (0.0–33.3) | 0.317 |
| EORTC QLQ-C30 | T3 Group IG | T3 Group CG | p-Value |
|---|---|---|---|
| (Median, Range) | (Median, Range) | ||
| QL2 | 79.2 (50.0–100.0) | 79.2 (75.0–100.0) | 0.664 |
| PF2 | 93.7 (60.0–100.0) | 91.7 (87.0–100.0) | 0.914 |
| RF2 | 100.0 (80.0–100.0) | 100.0 (100.0–100.0) | 0.414 |
| EF | 87.9 (50.0–100.0) | 89.4 (50.0–100.0) | 0.914 |
| CF | 100.0 (100.0–100.0) | 100.0 (100.0–100.0) | 1.000 |
| SF | 100.0 (100.0–100.0) | 100.0 (100.0–100.0) | 1.000 |
| FA | 11.1 (0.0–44.0) | 11.6 (0.0–33.0) | 0.577 |
| NV | 0.0 (0.0–20.0) | 0.0 (0.0–16.6) | 0.693 |
| PA | 0.0 (0.0–33.3) | 0.0 (0.0–23.3) | 0.793 |
| DY | 0.0 (0.0–33.3) | 0.0 (0.0–33.3) | 0.759 |
| SL | 16.7 (0.0–66.0) | 16.7 (0.0–66.7) | 0.818 |
| AP | 0.0 (0.0–33.3) | 0.0 (0.0–33.3) | 0.789 |
| CO | 0.0 (0.0–33.3) | 0.0 (0.0–33.3) | 0.895 |
| DI | 0.0 (0.0–66.6) | 0.0 (0.0–66.7) | 0.648 |
| FI | 0.0 (0.0–0.0) | 0.0 (0.0–0.0) | 1.000 |
| Group IG | Group CG | p-Value | |
|---|---|---|---|
| (Median, Range) | (Median, Range) | ||
| GLOBAL PSQI | |||
| T0 | 8.5 (2.0–13.0) | 7.0 (4.0–15.0) | 0.855 |
| T1 | 5.0 (3.0–10.0) | 10.0 (4.0–12.0) | 0.133 |
| T2 | 3.0 (1.0–7.0) | 4.0 (2.0–8.0) | 0.554 |
| T3 | 5.5 (3.0–10.0) | 5.0 (2.0–9.0) | 0.668 |
| HADS: ANXIETY | |||
| T0 | 7.0 (3.0–17.0) | 6.0 (4.0–9.0) | 0.783 |
| T1 | 5.5 (0.0–14.0) | 6.0 (2.0–8.0) | 0.745 |
| T2 | 4.0 (2.0–9.0) | 5.0 (4.0–6.0) | 0.554 |
| T3 | 3.0 (1.0–9.0) | 3.5 (0.0–8.0) | 0.086 |
| HADS: DEPRESSION | |||
| T0 | 8.5 (2.0–14.0) | 6.0 (4.0–8.0) | 0.410 |
| T1 | 4.5 (1.0–13.0) | 5.5 (2.0–7.0) | 0.830 |
| T2 | 2.5 (0.0–16.0) | 6.0 (3.0–7.0) | 0.384 |
| T3 | 2.0 (1.0–10.0) | 3.0 (0.0–8.0) | 0.104 |
| SMWT | |||
| T0 | 590.0 (360.0–685.0) | 375.0 (330.0–560.0) | 0.100 |
| T1 | 625.0 (400.0–815.0) | 359.0 (320.0–510.0) | 0.022 * |
| T2 | 573.0 (445.0–815.0) | 500.0 (400.0–535.0) | 0.067 |
| T3 | 580.0 (445.0–750.0) | 450.0 (400.0–600.0) | 0.100 |
| SPPB | |||
| T0 | 11.0 (7.0–12.0) | 11.0 (9.0–11.0) | 1.000 |
| T1 | 11.0 (10.0–12.0) | 11.0 (9.0–11.0) | 0.161 |
| T2 | 12.0 (10.0–12.0) | 11.0 (10.0–12.0) | 0.287 |
| T3 | 12.0 (10.0–12.0) | 10.0 (9.0–12.0) | 0.169 |
| HANDGRIP | |||
| T0 | 57.0 (28.0–62.0) | 41.0 (40.0–59.0) | 0.272 |
| T1 | 57.0 (28.0–62.0) | 50.0 (41.0–55.0) | 0.099 |
| T2 | 57.0 (37.0–62.0) | 52.0 (41.0–58.0) | 0.233 |
| T3 | 56.0 (39.0–65.0) | 50.0 (41.0–55.0) | 0.120 |
| BMI | |||
| T0 | 21.4 (17.2–25.7) | 24.0 (22.0–41.4) | 0.200 |
| T1 | 21.8 (18.6–26.8) | 24.0 (20.0–39.5) | 0.465 |
| T2 | 22.6 (19.5–27.6) | 22.5 (20.0–39.5) | 0.927 |
| T3 | 23.0 (21.0–28.3) | 22.5 (20.2–39.6) | 0.647 |
| SMI-BIA | |||
| T0 | 8.9 (7.6–9.6) | 7.8 (6.4–8.6) | 0.086 |
| T1 | 9.2 (7.6–10.5) | 8.0 (6.5–10.7) | 0.310 |
| T2 | 9.7 (7.1–10.5) | 8.0 (7.1–10.8) | 0.582 |
| T3 | 9.4 (7.0–9.7) | 8.0 (7.4–10.9) | 0.712 |
| PhA-BIA | |||
| T0 | 5.6 (4.1–5.7) | 4.6 (4.5–5.6) | 0.460 |
| T1 | 5.6 (4.4–6.5) | 5.0 (4.4–5.1) | 0.141 |
| T2 | 5.8 (5.0–6.5) | 5.0 (4.4–5.3) | 0.054 |
| T3 | 5.8 (5.0–6.1) | 5.0 (4.4–5.3) | 0.022 * |
| IG (n = 6) | Follow-up | |||||
|---|---|---|---|---|---|---|
| t0vst1 | t0vst2 | t0vst3 | t1vst2 | t1vst3 | t2vst3 | |
| EORTC QLQ-C30 | p-Value | |||||
| QL2 | 0.104 | 0.066 | 0.074 | 0.141 | 0.339 | 1.000 |
| PF2 | 0.197 | 0.068 | 0.715 | 0.180 | 0.593 | 0.109 |
| RF2 | 0.078 | 0.180 | 0.068 | 0.180 | 0.109 | 1.000 |
| EF | 0.116 | 0.068 | 0.075 | 0.655 | 0.893 | 1.000 |
| CF | 0.317 | 1.000 | 0.317 | 1.000 | 1.000 | 1.000 |
| SF | 0.078 | 0.068 | 0.027 * | 0.180 | 0.068 | 0.157 |
| FA | 0.141 | 0.109 | 0.046 * | 0.285 | 0.269 | 1.000 |
| NV | 0.285 | 1.000 | 1.000 | 0.317 | 0.414 | 0.317 |
| PA | 0.131 | 0.785 | 0.131 | 0.655 | 1.000 | 0.317 |
| DY | 0.317 | 1.000 | 1.000 | 1.000 | 0.317 | 1.000 |
| SL | 0.102 | 0.102 | 0.077 | 1.000 | 0.655 | 1.000 |
| AP | 0.141 | 0.317 | 0.221 | 0.317 | 0.564 | 0.157 |
| CO | 0.180 | 1.000 | 0.197 | 0.317 | 1.000 | 1.000 |
| DI | 0.564 | 0.317 | 0.705 | 0.317 | 1.000 | 0.317 |
| FI | 0.317 | 1.000 | 0.317 | 1.000 | 1.000 | 1.000 |
| PSQI | ||||||
| Global | 0.078 | 0.144 | 0.339 | 0.180 | 0.752 | 0.357 |
| HADS | ||||||
| Anxiety | 0.236 | 1.000 | 0.078 | 1.000 | 0.248 | 0.102 |
| Depression | 0.673 | 0.854 | 0.068 | 1.000 | 0.115 | 0.581 |
| FUNCTIONAL PARAMETERS | ||||||
| SMWT | 0.028 * | 0.173 | 0.075 | 0.465 | 0.172 | 0.892 |
| HANDGRIP | 0.715 | 0.917 | 0.600 | 0.285 | 0.500 | 0.686 |
| SPPB | 0.285 | 0.197 | 0.109 | 0.317 | 0.564 | 1.000 |
| NUTRITIONAL PARAMETERS | ||||||
| BMI | 0.068 | 0.080 | 0.060 | 0.144 | 0.055 | 0.080 |
| SMI-BIA | 0.225 | 0.172 | 0.416 | 0.285 | 0.916 | 0.167 |
| PhA-BIA | 0.109 | 0.028 * | 0.027 * | 0.109 | 0.206 | 1.000 |
| CG (n = 5) | Follow-up | |||||
|---|---|---|---|---|---|---|
| t0vst1 | t0vst2 | t0vst3 | t1vst2 | t1vst3 | t2vst3 | |
| EORTC QLQ C30 | p-Value | |||||
| QL2 | 0.715 | 1.000 | 0.066 | 0.141 | 0.066 | 0.109 |
| PF2 | 0.102 | 1.000 | 0.180 | 0.655 | 0.109 | 0.109 |
| RF2 | 0.357 | 1.000 | 0.109 | 0.066 | 0.066 | 1.000 |
| EF | 1.000 | 0.066 | 0.715 | 0.109 | 0.144 | 0.715 |
| CF | 0.276 | 0.066 | 0.066 | 0.102 | 0.102 | 1.000 |
| SF | 0.285 | 0.285 | 0.180 | 0.285 | 0.180 | 0.180 |
| FA | 0.180 | 0.144 | 0.144 | 0.068 | 0.068 | 0.715 |
| NV | 0.317 | 0.317 | 0.655 | 1.000 | 0.317 | 0.317 |
| PA | 0.593 | 0.276 | 0.180 | 0.276 | 1.000 | 0.655 |
| DY | 0.317 | 0.317 | 1.000 | 1.000 | 0.317 | 0.317 |
| SL | 0.655 | 0.141 | 0.180 | 0.276 | 0.317 | 0.655 |
| AP | 0.317 | 1.000 | 0.317 | 0.655 | 1.000 | 0.655 |
| CO | 0.317 | 0.655 | 1.000 | 0.655 | 0.564 | 0.655 |
| DI | 0.317 | 0.317 | 0.317 | 0.317 | 0.655 | 0.655 |
| FI | 1.000 | 0.317 | 0.317 | 0.317 | 0.317 | 0.317 |
| PSQI | ||||||
| Global | 1.000 | 0.066 | 0.066 | 0.066 | 0.066 | 0.785 |
| HADS | ||||||
| Anxiety | 0.581 | 0.141 | 0.197 | 1000 | 0.109 | 0.785 |
| Depression | 0.715 | 0.465 | 0.285 | 0.715 | 0.197 | 0.854 |
| FUNCTIONAL PARAMETERS | ||||||
| SMWT | 0.225 | 0.223 | 0.860 | 0.138 | 0.155 | 0.715 |
| HANDGRIP | 0.465 | 0.465 | 0.465 | 0.465 | 0.083 | 0.705 |
| SPPB | 1.000 | 0.414 | 1.000 | 0.414 | 1.000 | 0.414 |
| NUTRITIONAL PARAMETERS | ||||||
| BMI | 0.144 | 0.078 | 0.078 | 1.000 | 0.713 | 0.063 |
| SMI-BIA | 0.176 | 0.176 | 0.131 | 0.109 | 0.109 | 0.593 |
| PHA-BIA | 0.786 | 0.588 | 0.498 | 0.180 | 0.180 | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nusca, S.M.; Parisi, A.; Mercantini, P.; Gasparrini, M.; Pitasi, F.A.; Lacopo, A.; Colonna, V.; Stella, G.; Cerulli, C.; Grazioli, E.; et al. Evaluation of a Post-Operative Rehabilitation Program in Patients Undergoing Laparoscopic Colorectal Cancer Surgery: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 5632. https://doi.org/10.3390/ijerph18115632
Nusca SM, Parisi A, Mercantini P, Gasparrini M, Pitasi FA, Lacopo A, Colonna V, Stella G, Cerulli C, Grazioli E, et al. Evaluation of a Post-Operative Rehabilitation Program in Patients Undergoing Laparoscopic Colorectal Cancer Surgery: A Pilot Study. International Journal of Environmental Research and Public Health. 2021; 18(11):5632. https://doi.org/10.3390/ijerph18115632
Chicago/Turabian StyleNusca, Sveva Maria, Attilio Parisi, Paolo Mercantini, Marcello Gasparrini, Francesco Antonio Pitasi, Alessandra Lacopo, Vincenzo Colonna, Giulia Stella, Claudia Cerulli, Elisa Grazioli, and et al. 2021. "Evaluation of a Post-Operative Rehabilitation Program in Patients Undergoing Laparoscopic Colorectal Cancer Surgery: A Pilot Study" International Journal of Environmental Research and Public Health 18, no. 11: 5632. https://doi.org/10.3390/ijerph18115632
APA StyleNusca, S. M., Parisi, A., Mercantini, P., Gasparrini, M., Pitasi, F. A., Lacopo, A., Colonna, V., Stella, G., Cerulli, C., Grazioli, E., Tranchita, E., Santoboni, F., Latini, E., Trischitta, D., Vetrano, M., Visco, V., Pavan, A., & Vulpiani, M. C. (2021). Evaluation of a Post-Operative Rehabilitation Program in Patients Undergoing Laparoscopic Colorectal Cancer Surgery: A Pilot Study. International Journal of Environmental Research and Public Health, 18(11), 5632. https://doi.org/10.3390/ijerph18115632