
Examining Protection Motivation and Network Externality Perspective Regarding the Continued Intention to Use M-Health Apps




Abstract
:1. Introduction
2. Literature Review
2.1. M-Health Apps
2.2. Protection Motivation Theory
2.3. Network Externalities
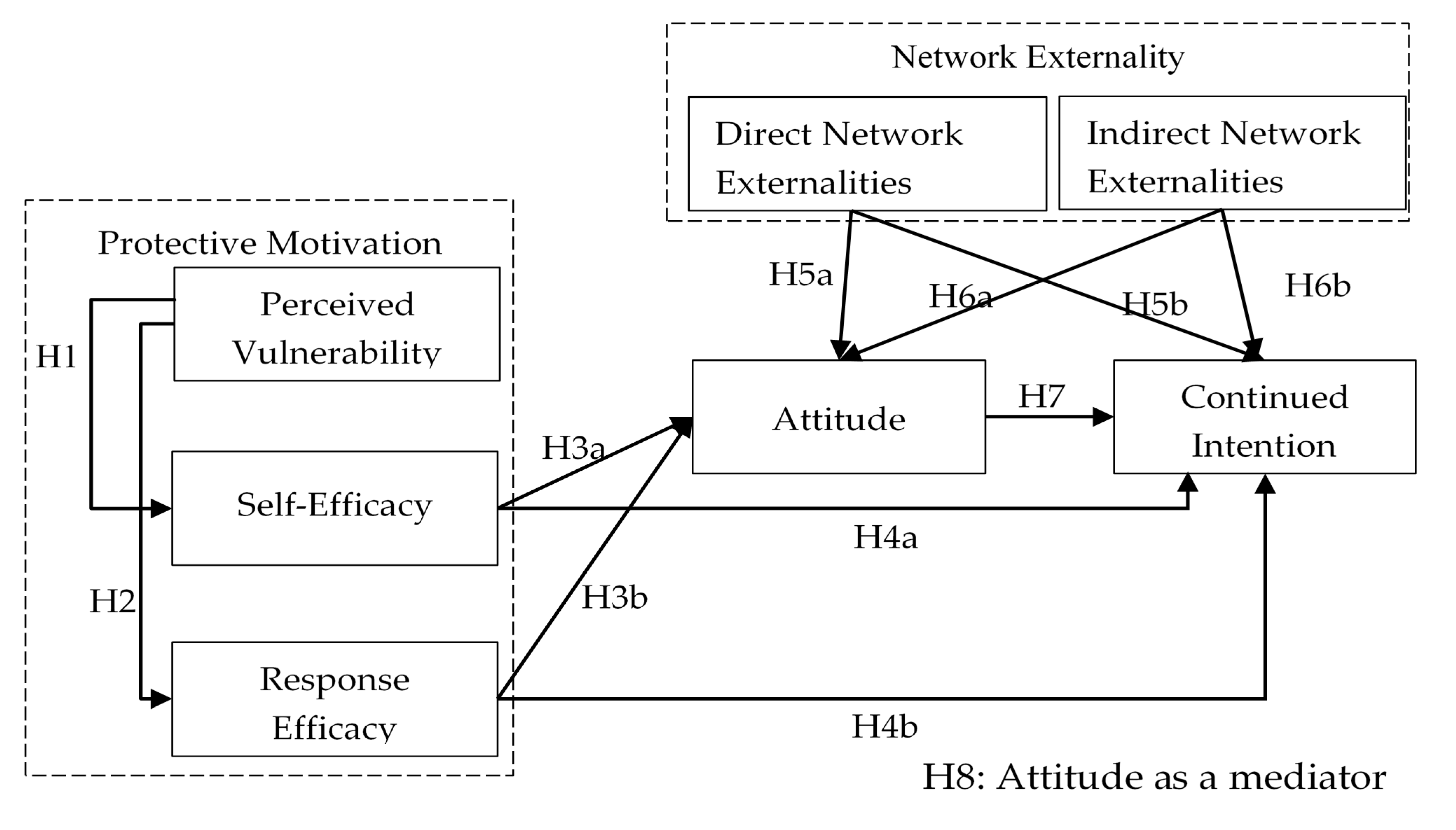
3. Research Model and Hypotheses
3.1. Hypotheses Based on PMT
3.2. Hypotheses Based on Network Externalities
3.2.1. Direct Network Externalities
3.2.2. Indirect Network Externalities
3.3. Attitudes
4. Methodology
4.1. Data Collection
4.2. Measures
4.3. Results
4.3.1. Measurement Model
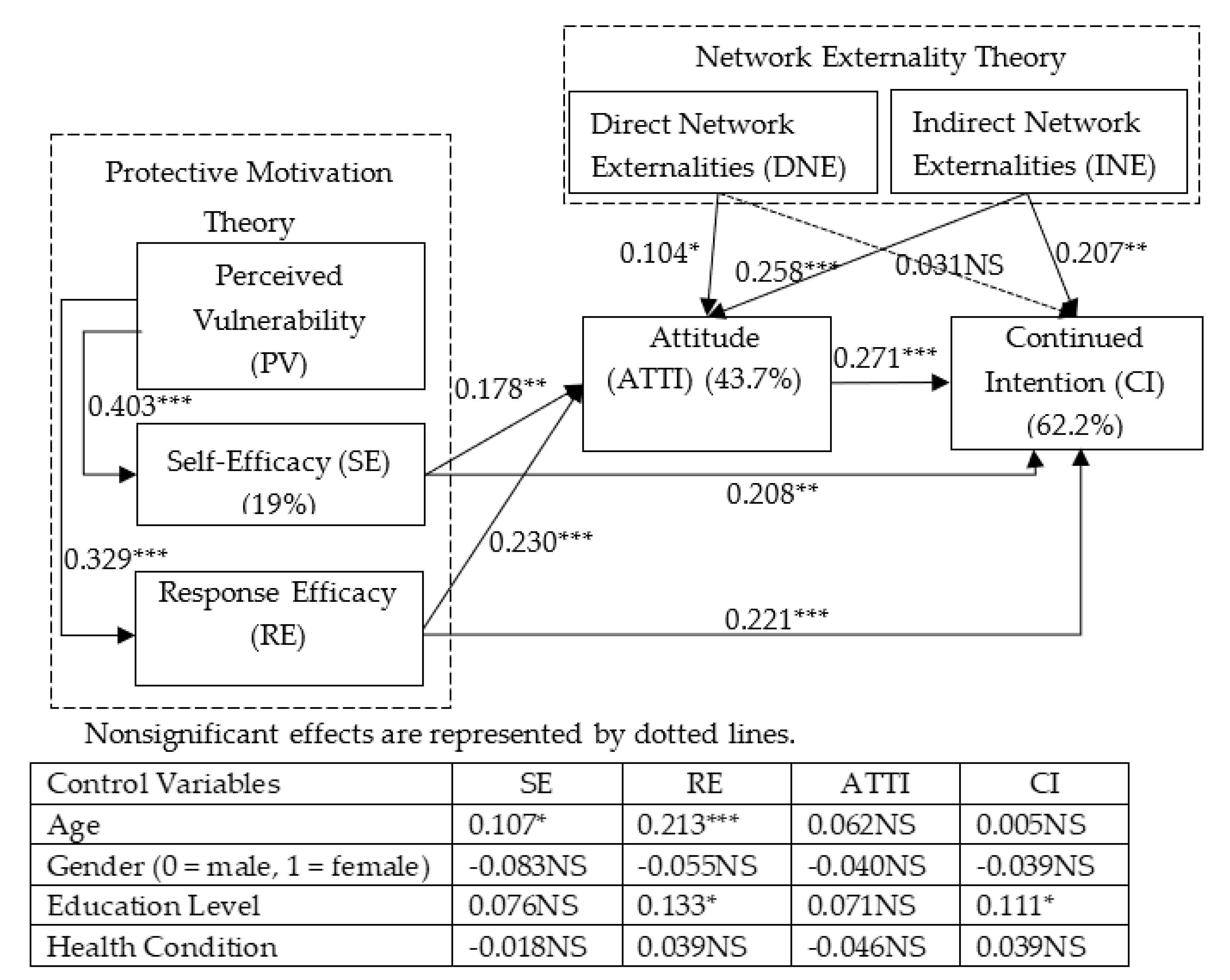
4.3.2. Structural Model
5. Discussion
5.1. Theoretical Implications
5.2. Practical Implications
5.3. Limitations and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ali, E.E.; Chew, L.; Yap, Y.L. Evolution and current status of mhealth research: A systematic review. BMJ Innov. 2016, 2, 33–40. [Google Scholar] [CrossRef]
- Birkhoff, S.D.; Moriarty, H. Challenges in mobile health app research: Strategies for interprofessional researchers. J. Interprof. Educ. Pract. 2020, 19, 100325. [Google Scholar] [CrossRef]
- Benjumea, J.; Ropero, J.; Rivera-Romero, O.; Dorronzoro-Zubiete, E.; Carrasco, A. Assessment of the Fairness of Privacy Policies of Mobile Health Apps: Scale Development and Evaluation in Cancer Apps. JMIR mHealth uHealth 2020, 8, e17134. [Google Scholar] [CrossRef]
- Larson, R.S. A Path to Better-Quality Mobile Health Apps. JMIR mHealth uHealth 2018, 6, e10414. [Google Scholar] [CrossRef]
- Zhang, X.; Yan, X.; Cao, X.; Sun, Y.; Chen, H.; She, J. The role of perceived e-health literacy in users’ continuance intention to use mobile healthcare applications: An exploratory empirical study in China. Inf. Technol. Dev. 2016, 24, 198–223. [Google Scholar] [CrossRef]
- Zhou, L.; Bao, J.; Watzlaf, V.; Parmanto, B. Barriers to and Facilitators of the Use of Mobile Health Apps from a Security Perspective: Mixed-Methods Study. JMIR mHealth uHealth 2019, 7, e11223. [Google Scholar] [CrossRef]
- Cheng, X.; Liu, Y. Current situation and future trend of mobile medical APP with the example of Ping’an good doctor. China Med. Her. 2017, 14, 157–160. [Google Scholar]
- Fan, Y.; Ji, X. Research on user satisfaction based onmedical and health APP. Comput. Eng. Softw. 2020, 14, 38–41. [Google Scholar]
- Abd-Alrazaq, A.A.; Bewick, B.M.; Farragher, T.; Gardner, P. Factors that affect the use of electronic personal health records among patients: A systematic review. Int. J. Med. Inform. 2019, 126, 164–175. [Google Scholar] [CrossRef]
- Dehzad, F.; Hilhorst, C.; Bie, C.D.; Claassen, E. Adopting Health Apps, What’s Hindering Doctors and Patients? Health 2014, 6, 2204–2217. [Google Scholar] [CrossRef] [Green Version]
- Guo, X.; Sun, Y.; Nan, W.; Peng, Z.; Yan, Z. The dark side of elderly acceptance of preventive mobile health services in China. Electron. Mark. 2012, 23, 49–61. [Google Scholar] [CrossRef]
- Stoyanov, S.R.; Hides, L.; Kavanagh, D.J.; Zelenko, O.; Mani, M. Mobile App Rating Scale: A New Tool for Assessing the Quality of Health Mobile Apps. JMIR mHealth uHealth 2015, 3, e27. [Google Scholar] [CrossRef] [Green Version]
- Cho, J. The impact of post-adoption beliefs on the continued use of health apps. Int. J. Med. Inform. 2016, 87, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Leung, L.; Chen, C. E-health/m-health adoption and lifestyle improvements: Exploring the roles of technology readiness, the expectation-confirmation model, and health-related information activities. Telecommun. Policy 2019, 43, 563–575. [Google Scholar] [CrossRef] [Green Version]
- Gimpel, H.; Manner-Romberg, T.; Schmied, F.; Winkler, T.J. Understanding the evaluation of mHealth app features based on a cross-country Kano analysis. Electron. Mark. 2021. [Google Scholar] [CrossRef]
- Guo, X.; Han, X.; Zhang, X.; Dang, Y.; Chen, C. Investigating m-Health Acceptance from a Protection Motivation Theory Perspective: Gender and Age Differences. Telemed. J. e-Health 2015, 21, 661–669. [Google Scholar] [CrossRef]
- Akter, S.; D’Ambra, J.; Ray, P. Service quality of mHealth platforms: Development and validation of a hierarchical model using PLS. Electron. Mark. 2010, 20, 209–227. [Google Scholar] [CrossRef]
- Johnston, A.C.; Warkentin, R. Fear Appeals and Information Security Behaviors: An Empirical Study. MIS Q. 2010, 34, 549–566. [Google Scholar] [CrossRef]
- Anderson, C.L.; Agarwal, R. Empirical examination of home computer user security behavioral intentions. MIS Q. 2010, 34, 613–643. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.P.; Bhattacherjee, A. Elucidating Individual Intention to Use Interactive Information Technologies: The Role of Network Externalities. Int. J. Electron. Commer. 2008, 13, 85–108. [Google Scholar] [CrossRef]
- Zhou, T. The effect of network externality on mobile social network site continuance. Program Electron. Libr. Inf. Syst. 2015, 49, 289–304. [Google Scholar] [CrossRef]
- Zhang, K.Z.K.; Cheung, C.M.K.; Lee, M.K.O. Examining the moderating effect of inconsistent reviews and its gender differences on consumers’ online shopping decision. Int. J. Inf. Manag. 2014, 34, 89–98. [Google Scholar] [CrossRef]
- Zhang, J.; Cheng, X. Study on the Status, Problem and Trend in the Development of Mobile Medical APP. J. Med. Inform. 2018, 39, 2–6. [Google Scholar]
- Bigdata. China Mobile Medical APP Product Detection Report in 2018. 2018. Available online: http://www.bigdata-research.cn/content/201804/663.html (accessed on 23 April 2018).
- Steven, P.D.; Rogers, R.W. Protection Motivation Theory and preventive health: Beyond the Health Belief Model. Health Educ. Res. 1986, 1, 153–161. [Google Scholar]
- Wang, Y.; Xiao, X.; Zheng, P.; Fu, H. Application and development of protection motivation theory in individual behavior change. Chin. J. Health Educ. 2009, 25, 853–856. [Google Scholar]
- Rogers, R.W. A Protection Motivation Theory of Fear Appeals and Attitude Change1. J. Psychol. Interdiscip. Appl. 1975, 91, 94–114. [Google Scholar] [CrossRef]
- Stainback, R.D.; Rogers, R.W. Identifying Effective Components of Alcohol Abuse Prevention Programs: Effects of Fear Appeals, Message Style, and Source Expertise. Int. J. Addict. 1983, 18, 393–405. [Google Scholar] [CrossRef]
- Liu, C. Study on Application of Protection Motivation Theory in the Interpretation, Intervention and Prediction of Health Behavior. Med. Soc. 2015, 28, 77–79. [Google Scholar]
- Yin, M.; Li, Q. An Empirical study on the intention of healthcare application usage based on the PMT. J. Mod. Inf. 2016, 36, 63–70. [Google Scholar]
- Huan, Y.; Li, X.; Aydeniz, M.; Wyatt, T. Mobile Learning Adoption: An Empirical Investigation for Engineering Education. Int. J. Eng. Educ. 2015, 31, 1081–1091. [Google Scholar]
- Yoon, C.; Kim, H. Understanding computer security behavioral intention in the workplace: An empirical study of Korean firms. Inf. Technol. People 2013, 26, 425–456. [Google Scholar] [CrossRef]
- Zhou, T.; Li, H.; Liu, Y. Understanding mobile IM continuance usage from the perspectives of network externality and switching costs. Int. J. Mob. Commun. 2015, 13, 188–203. [Google Scholar] [CrossRef] [Green Version]
- Katz, M.L.; Shapiro, C. Network Externalities, Competition, and Compatibility. Am. Econ. Rev. 1985, 75, 424–440. [Google Scholar]
- Economides, N. The Economics of Networks. Int. J. Ind. Organ. 1996, 14, 673–699. [Google Scholar] [CrossRef]
- Zhou, T. The Effects of Network Externality and Flow Experience on Mobile SNS Continuance. Int. J. Technol. Hum. Interact. 2017, 13, 57–69. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Y.M. What Drives Nurses’ Blended E-Learning Continuance Intention? Educ. Technol. Soc. 2014, 17, 203–215. [Google Scholar]
- Rogers, R.W. Cognitive and physiological process in fear appeals and attitudes changer: A revised theory of protection motivation. Soc. Psychophysiol. 1983, 19, 469–479. [Google Scholar]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. User acceptance of computer technology: A comparison of two theoretical models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef] [Green Version]
- Bulgurcu, B.; Cavusoglu, R.; Benbasat, R. Information Security Policy Compliance: An Empirical Study of Rationality-Based Beliefs and Information Security Awareness. MIS Q. 2010, 34, 523–548. [Google Scholar] [CrossRef] [Green Version]
- Lewis, W.; Agarwal, R.; Sambamurthy, V. Sources of influence on beliefs about information technology use: An empirical study of knowledge workers. MIS Q. 2003, 27, 657–678. [Google Scholar] [CrossRef] [Green Version]
- Pavlou, P.A.; Fygenson, M. Understanding and predicting electronic commerce adoption: An extension of the theory of planned behavior. MIS Q. 2006, 30, 115–143. [Google Scholar] [CrossRef]
- Woon, I.M.Y.; Tan, G.W.; Low, R.T. A Protection Motivation Theory Approach to Home Wireless Security. In Proceedings of the the 26th International Conference on Information Systems, Las Vegas, NV, USA, 11–14 December 2005; pp. 367–380. [Google Scholar]
- Yang, X.; Chen, T.; Liang, X. Research on Influence Factors of Mobile Products of NEEP Based on Technology Acceptance Model and Networt Externalities. Comput. Eng. Softw. 2018, 39, 185–190. [Google Scholar]
- Hong, H.; Xu, D. An Empirical Study on Continuance Using Intention of Mobile Social Apps. In Proceedings of the WHICEB 2015, Wuhan, China, 19 June 2015; pp. 95–104. [Google Scholar]
- Wang, C.; Hsu, Y.; Fang, W. Acceptance of Technology with Network Externalities: An Empirical Study of Internet Instant Messaging Services. JITTA J. Inf. Technol. Theory Appl. 2005, 6, 15–28. [Google Scholar]
- Li, M.; Gu, R.; Shang, X.; Wang, K. Critical Factors of post-adoption intention of mobile instanat messaging service. J. Manag. Sci. 2010, 23, 72–83. [Google Scholar]
- Hung, S.-Y.; Ku, C.-Y.; Chang, C.-M. Critical factors of WAP services adoption: An empirical study. Electron. Commer. Res. Appl. 2003, 2, 42–60. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of inforamtion technology: Toward a unifed view. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I.; Fishbein, M. Understanding Attitudes and Predicting Social Behavior; Prentice-Hall: Englewood Cliffs, NJ, USA, 1980. [Google Scholar]
- Zhang, S.; Han, Y.; Wan, T. A Research on Continuance Usage Intention of the Interactive Academic Web Portals. Future Dev. 2014, 37, 43–50. [Google Scholar]
- Li, C.-R.; Chu, C.-P.; Lin, C.-J. The contingent value of exploratory and exploitative learning for new product development performance. Ind. Mark. Manag. 2010, 39, 1186–1197. [Google Scholar] [CrossRef]
- Venkatesh, V.; Goyal, S. Expectation disconfirmation and technology adoption: Polynomal modeling and response surface analysis. MIS Q. 2010, 34, 281–303. [Google Scholar] [CrossRef] [Green Version]
- Brislin, R.W. Back-translation for cross-cultural research. J. Cross-Cult. Psychol. 1970, 1, 185–216. [Google Scholar] [CrossRef]
- Ringle, C.M.; Wende, S.; Will, A. Finite mixture partial least squares analysis: Methodology and numerical examples. In Handbook of Partial Least Squares; Springer: Berlin/Heidelberg, Germany, 2010; pp. 195–218. [Google Scholar]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Baron, S.; Harris, K. Toward an understanding of consumer perspectives on experiences. J. Serv. Mark. 2010, 24, 518–531. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Category | Frequency | Percentage (%) |
|---|---|---|---|
| Age | 18–25 | 75 | 20.4 |
| 26–35 | 186 | 50.5 | |
| 36–45 | 70 | 19.0 | |
| 46–65 | 37 | 10.1 | |
| Education | High school or below | 38 | 10.4 |
| Junior college | 62 | 16.8 | |
| Bachelor’s degree | 202 | 54.9 | |
| Master’s degree or above | 66 | 17.9 | |
| Gender | Female | 140 | 38.1 |
| Male | 228 | 61.9 | |
| Health condition | Healthy | 156 | 42.4 |
| Sub-health | 164 | 44.6 | |
| Underlying minor illness | 32 | 8.7 | |
| Underlying chronic disease | 16 | 4.3 |
| Constructs | Items | References |
|---|---|---|
| Self-Efficacy | SE1. I know what kind of health-related information is provided on this m-health app. SE2. I have the competence to assess the correctness of the health-related information provided on this m-health app. SE3. I can use this m-health app to make health-related decisions. | [18] |
| Perceived Vulnerability | PV1. I think I am facing the threat of serious disease. PV2. I think I am facing the probability of suffering from a serious disease in the future. PV3. I will probably suffer from a disease. | |
| Response Efficacy | RE1. This m-health app can notify users of the starting and ending time of healthcare services in time. RE2. This m-health app can send in-time feedback to me. RE3. This m-health app can provide instructions if I have some problems. | |
| Direct Network Externalities | DNE1. Most of my friends use this m-health app. DNE2. The majority of my colleagues use this m-health app. DNE3. The majority of the people I know use this m-health app. | [20] |
| Indirect Network Externalities | INE1. This m-health app provides many complementary services (e.g., health management tools and discussion groups). INE2. This m-health app provides many other application services. INE3. This m-health app provides some value-added services (online shopping, outfits, skincare, weight reduction and body shaping, medical cosmetology, etc.) | |
| Attitude | ATTI1. Using this m-health app is a good idea. ATTI2. Using this m-health app makes seeing a doctor easier and more enjoyable. ATTI3. I like to use this m-health app. | [53] |
| Continued Intention | CI1. I intend to continue using this m-health app in the future. CI2. I will continue to use this m-health app. CI3. I will recommend this m-health app to others. |
| Constructs | PV | SE | RE | DNE | INE | ATTI | CI |
|---|---|---|---|---|---|---|---|
| Perceived Vulnerability (PV) | 0.875 | ||||||
| Self-Efficacy (SE) | 0.414 | 0.840 | |||||
| Response Efficacy (RE) | 0.362 | 0.670 | 0.848 | ||||
| Direct Network Externalities (DNE) | 0.276 | 0.514 | 0.529 | 0.923 | |||
| Indirect Network Externalities (INE) | 0.333 | 0.604 | 0.606 | 0.478 | 0.83 | ||
| Attitude (ATTI) | 0.266 | 0.550 | 0.574 | 0.447 | 0.563 | 0.833 | |
| Continued Intention (CI) | 0.293 | 0.645 | 0.664 | 0.470 | 0.642 | 0.651 | 0.894 |
| Mean (SD) | 3.894 (1.384) | 4.913 (1.038) | 5.158 (0.983) | 4.530 (1.263) | 4.997 (1.005) | 5.495 (1.012) | 5.418 (1.051) |
| Composite reliability | 0.908 | 0.878 | 0.884 | 0.945 | 0.869 | 0.872 | 0.922 |
| Cronbach’s alpha | 0.851 | 0.791 | 0.804 | 0.912 | 0.775 | 0.779 | 0.874 |
| CFA Item Loadings ^ | 0.814–0.917 | 0.812–0.879 | 0.837–0.855 | 0.915–0.936 | 0.773–0.853 | 0.808–0.871 | 0.877–0.910 |
| Independent Variables | Mediator Variable | Dependent Variable | Indirect Effect Coefficients | 95% Bias-Corrected Confidence Intervals | Hypotheses |
|---|---|---|---|---|---|
| SE | ATTI | CI | 0.048 (0.020) | (0.008, 0.089) | H8a (√) |
| RE | 0.062 (0.023) | (0.017, 0.108) | H8b (√) | ||
| DNE | 0.028 (0.013) | (0.002, 0.054) | H8c (√) | ||
| INE | 0.070 (0.021) | (0.028, 0.111) | H8d (√) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, Y.; Wang, G.; Li, Y.; Ye, Q. Examining Protection Motivation and Network Externality Perspective Regarding the Continued Intention to Use M-Health Apps. Int. J. Environ. Res. Public Health 2021, 18, 5684. https://doi.org/10.3390/ijerph18115684
Luo Y, Wang G, Li Y, Ye Q. Examining Protection Motivation and Network Externality Perspective Regarding the Continued Intention to Use M-Health Apps. International Journal of Environmental Research and Public Health. 2021; 18(11):5684. https://doi.org/10.3390/ijerph18115684
Chicago/Turabian StyleLuo, Yumei, Guiping Wang, Yuwei Li, and Qiongwei Ye. 2021. "Examining Protection Motivation and Network Externality Perspective Regarding the Continued Intention to Use M-Health Apps" International Journal of Environmental Research and Public Health 18, no. 11: 5684. https://doi.org/10.3390/ijerph18115684
APA StyleLuo, Y., Wang, G., Li, Y., & Ye, Q. (2021). Examining Protection Motivation and Network Externality Perspective Regarding the Continued Intention to Use M-Health Apps. International Journal of Environmental Research and Public Health, 18(11), 5684. https://doi.org/10.3390/ijerph18115684