1. Introduction
The Severe Acute Respiratory Syndrome (SARS-CoV-2) is an emerging infectious disease that causes serious threats to the physical and mental health of the population.
The behavior of the general population, or of specific at-risk groups, such as aging subjects, can play an important role in both the spread and control of infectious diseases. The older population with a frailty status, which is characterized by a clinical history of polypathology, had higher mortality due to SARS-CoV-2 [
1,
2]. This increased susceptibility to infection is probably driven not only by comorbidity but also by reduced immunity due to the physiology of ageing [
3].
Lockdown measures play a key role in containing SARS-CoV-2 infection. However, in the older population, aspects associated with isolation and social distancing are related to increased cognitive decline [
4]. As a result of COVID-19 containment measures, older adults may experience physical and other mental health problems [
5], such as depressive mood and anxiety-related fear of contagion [
6]. In line with these aspects, a recent study [
7] highlighted how both cognitive and physical issues related to the COVID-19 pandemic may play a key role in the novel “lockdown fatigue”. In particular, the authors found that pandemic fatigue was associated with decreased processing and walking speed and with mood changes in terms of depression.
While all these conditions represent the likely consequences of a pandemic, the variables driving modifications of behavior patterns—particularly concerning contagion prevention—also need to be considered and analyzed. One of the factors that can influence the willingness and motivation to adopt precautionary behavior is the perception of risk [
8,
9], i.e., the perceived personal vulnerability or likelihood of contracting a disease. Feeling vulnerable, together with realizing disease severity, can be jointly considered as “perceived threat”. People are expected to experience the highest perceived SARS-CoV-2 threat if they think that a likely infection will have serious health consequences. Indeed, people who are more vulnerable—such as older adults—present a higher level of fear [
10] and anxiety [
11] related to COVID-19.
On the other hand, some studies concerning outbreaks, such as the H5N1 and the current COVID-19 pandemic, found a lower risk perception in older adults than in younger people [
12,
13]. A recent study reported a lower perceived risk of being infected by COVID-19 in the oldest-old (75 years and older) than in the youngest-old (60–69 years) and middle-old (70–75 years) groups [
14]. According to the authors, this result might reflect an age-related cognitive decline, particularly concerning executive control functioning, as risk-taking and risk perception are associated with monitoring abilities [
15]. In light of this evidence, a reduction in perceived risk may lead older adults—who are more prone to unfavorable outcomes—to underestimate the importance of proper precautions to avoid COVID-19 infection.
To date, however, no longitudinal studies have analyzed the association among risk threat perception of SARS-CoV-2 contagion, physical-health status, cognitive functions, and mood deflections in cognitively preserved older adults during home confinement. These aspects should be further emphasized as personalized psychological interventions are found to play an important role in primary prevention and psychological well-being by reducing the negative impact on physical status, cognitive function, and mood disorders.
To fill this gap, we investigated the relationships among perceived risk of SARS-CoV-2 contagion, physical-cognitive functioning, and mood changes in cognitively preserved older adults, engaged as volunteers, and characterized by the presence of two or more age-related diseases (polypathology) and subsequent pharmacotherapy [
16]. The availability of pre-pandemic data (at T0) of 50 subjects allowed us to investigate the extent to which perceived threat of SARS-CoV-2 was predicted by cognitive functioning, psychological state, and frailty determinants assessed with the phenotypic model [
17], and by their interaction.
To the best of our knowledge, this is the first longitudinal study investigating: (a) the neuropsychological profile and frailty determinants of healthy older adults before the pandemic; (b) the perceived threat of SARS-CoV-2 contagion during the lockdown; and (c) whether the latter reflects the interacting effects of baseline variables concerning cognitive, psychological, and/or physical status.
Since perceived threat has been previously related to psychological issues, such as anxiety [
18], and the latter may influence the occurrence of attentional and interpretation threat biases [
19,
20], also related to information about contagion, we expect that both psychological and cognitive factors might be useful in predicting perceived risk of contagion in our sample.
4. Discussion
To the best of our knowledge, this is the first published study that has monitored subjects in healthy cognitive aging for more than one year, before and after extremely restrictive measures due to the COVID-19 pandemic (i.e., from April 2019 to July 2020). This longitudinal design has provided a unique opportunity to investigate whether, and to what extent, the perceived threat of contracting SARS-CoV-2 is explained by pre-existing individual differences concerning physical pre-frailty, cognitive performance and mood deflections. Indeed, unlike related studies on the effect of the pandemic, T0 data allowed us to unveil novel associations between pre-COVID-19 neuropsychological variables and perceived risk of contagion in the last stage of the lockdown.
Although most of the participants were robust at T0, some of them were pre-frail. Only a few minor neuropsychological deficits were observed in cognitive functioning and in line with the margin of error in tests administered to the normative population. Moreover, some participants showed mood changes in terms of depression and anxiety but these deflections were not significant from a mental health perspective.
Concerning the T1 results, almost all subjects complied with the precautions recommended by the Italian Ministry of Health [
43] to prevent infection with SARS-CoV-2 and showed correct behaviors regarding the prevention of infection. It is noteworthy that almost the whole sample (90%) belonged to an upper-middle social class, according to HI. Combined with the high level of education, such aspects make clear the peculiarity of this population, characterized by social resources, which have enabled them to take the necessary precautions to avoid the risk of contagion. In fact, risk perception can be influenced by several aspects, including knowledge of the virus [
44] and the socio-economic status. Previous studies [
45,
46] have shown that older, socio-economically disadvantaged, and poorly-educated individuals are less informed about COVID-19 spreading and, therefore, do not take adequate precautions.
The T2 data collected immediately after the isolation period showed neither a significant worsening of cognitive functions nor mood deflections in terms of depression. However, the level of anxiety increased during the COVID-19 pandemic, from 4% to 10%.
Multiple linear regression analyses showed that perceived risk of SARS-CoV-2 at T2 was predicted by worse performance on the information processing speed component and on language comprehension, as well as higher levels of pre-frailty and anxiety, at T0. These cognitive difficulties may hamper the correct interpretation of the information provided on the risk of infection, leading to attentional threat bias, further increasing anxiety [
19]. Moreover, conflicting and confusing sources of information about the ongoing pandemic, in terms of ‘infodemia’, could exacerbate psychological distress in terms of anxiety and fear of contagion [
47,
48]. This would be even more pronounced in language processing in normal aging. Older subjects’ comprehension, even in the normative group, may also be less accurate due to an age-related slowdown in processing time, which increases in syntactically complex sentences. This pattern suggests an age-related decrease in parsing and interpretation efficiency suggesting how task-related operations are related to overall processing speed and working memory [
49].
In addition, the presence of a frailty state may reasonably lead to a greater perceived threat, as mortality rates from Covid-19 are higher in older adults suffering from this condition [
50].
In line with these considerations, the perceived threat caused by a new emerging virus, assessed at T2, was explained by reduced baseline performance in tasks of information processing speed and in linguistic comprehension (TMT-A and TT, respectively), and an increased level of anxiety (HARS), but not by frailty status. An unknown risk is usually perceived as more frightening [
44]; thus, a high level of anxiety at baseline may intensify the sense of danger. Furthermore, anxiety may influence attentional abilities [
20] but also the comprehension and the interpretation of stimuli [
19].
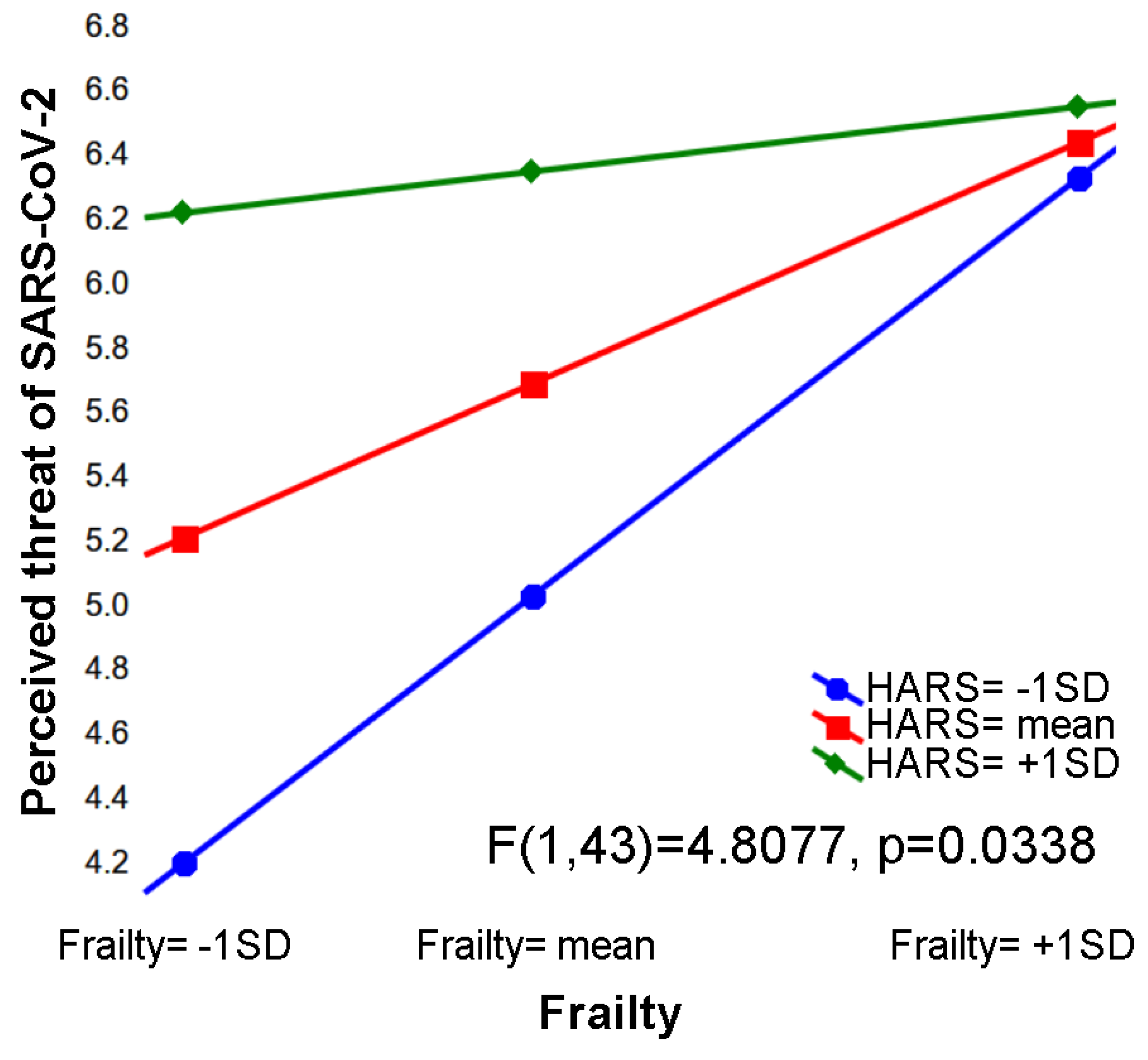
Since multiple regression models showed that frailty was related only to the perceived threat of SARS-CoV-2, we hypothesized that this factor, along with the anxiety status assessed at baseline, might play an important role in explaining perceived risk. Indeed, a moderation model showed an interaction between these two independent variables in predicting SARS-CoV-2 perceived threat. Particularly, at their highest level, both frailty and anxiety are sufficient to support the maximum degree of risk perception, on the other hand, when their values decrease, both are required to promote SARS-CoV-2 threat perception.
Limitation Section
Although the present study was carefully designed and achieved its purposes, some limitations should be addressed.
Firstly, an important aspect to be clarified concerns the scale used to assess threat perception. Even though the evaluation of “Perceived Threat” was performed indirectly, multiplying the measures of perceived “severity” and “vulnerability” of the Risk Perception of Infectious Diseases Questionnaire, it should be noted that this methodology has been validated and used in previous studies, i.e., [
9]. In particular, the “Perceived Threat” scale was considered a reliable tool for assessing risk perception of infection due to a very contagious and dangerous virus.
Secondly, our subjects were enrolled at the University of the Third Age, which promotes learning during aging. For this reason, they represent a very distinctive sample of older adults, characterized by a medium-high socioeconomic status and a medium-high level of education.
Finally, a sample size of 50 participants represents a limitation to this study; however, this population was studied in-depth through a neuropsychogeriatric assessment before the COVID-19 pandemic (T0) and during the first lockdown, both with strong restrictive measures (T1) and when they were eased (T2).
5. Conclusions
To the best of our knowledge, this is the first study examining the association between perceived threat of SARS-CoV-2 during the lockdown and a set of cognitive, psychological, and physical variables measured before and during restrictive lockdown measures, in cognitively normal aging subjects. Therefore, it is important to underline how UNITRE healthy participants represent a very distinctive reference sample to implement possible primary prevention pathways on older adults, with a particular focus on early determinants that may affect well-being in the current pandemic.
Our results showed, on the one hand, how physical frailty and mood deflection in terms of anxiety and, on the other hand, how cognition involved in information processing speed tasks and language comprehension, could influence the perceived threat of SARS-CoV-2 infection risk. The evidence that neuropsychogeriatric factors contribute to the perception of risk of an infectious disease shows the need to consider these variables.
Particular attention should be paid to frailty, as the pandemic lifestyle, characterized by reduced social interaction and a decrease in physical activities, may lead to the so-called “Corona-Frailty” [
51]. Moreover, the level of anxiety should be considered as it seems to modulate the perception of fear concerning COVID-19 infection.
The evidence that neuropsychological factors contribute to the perceived threat of an infectious disease (i.e., new virus) shows the need to consider these variables when planning information campaigns in older people, with the aim of achieving favorable changes in public behavior.
The present study emphasizes the contribution of neuropsychological factors to perceived threat of SARS-CoV-2 highlighting the importance of tailoring information campaigns addressed to older people.
The presence of pre-pandemic neurocognitive measures has provided a unique opportunity to investigate which facets of psychological, physical, and cognitive status predict a crucial variable such as perceived threat of SARS-CoV-2 in the aftermath of the lockdown. Furthermore, the COVID-19 containment measures, constrained to perform T2 neuropsychogeriatric assessment via selected neuropsychological, tests as suitable for remote administration.


 ,
, 

{kind=link}