
Executive Function among Chilean Shellfish Divers: A Cross-Sectional Study Considering Working and Health Conditions in Artisanal Fishing


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Field Work and Study Instruments
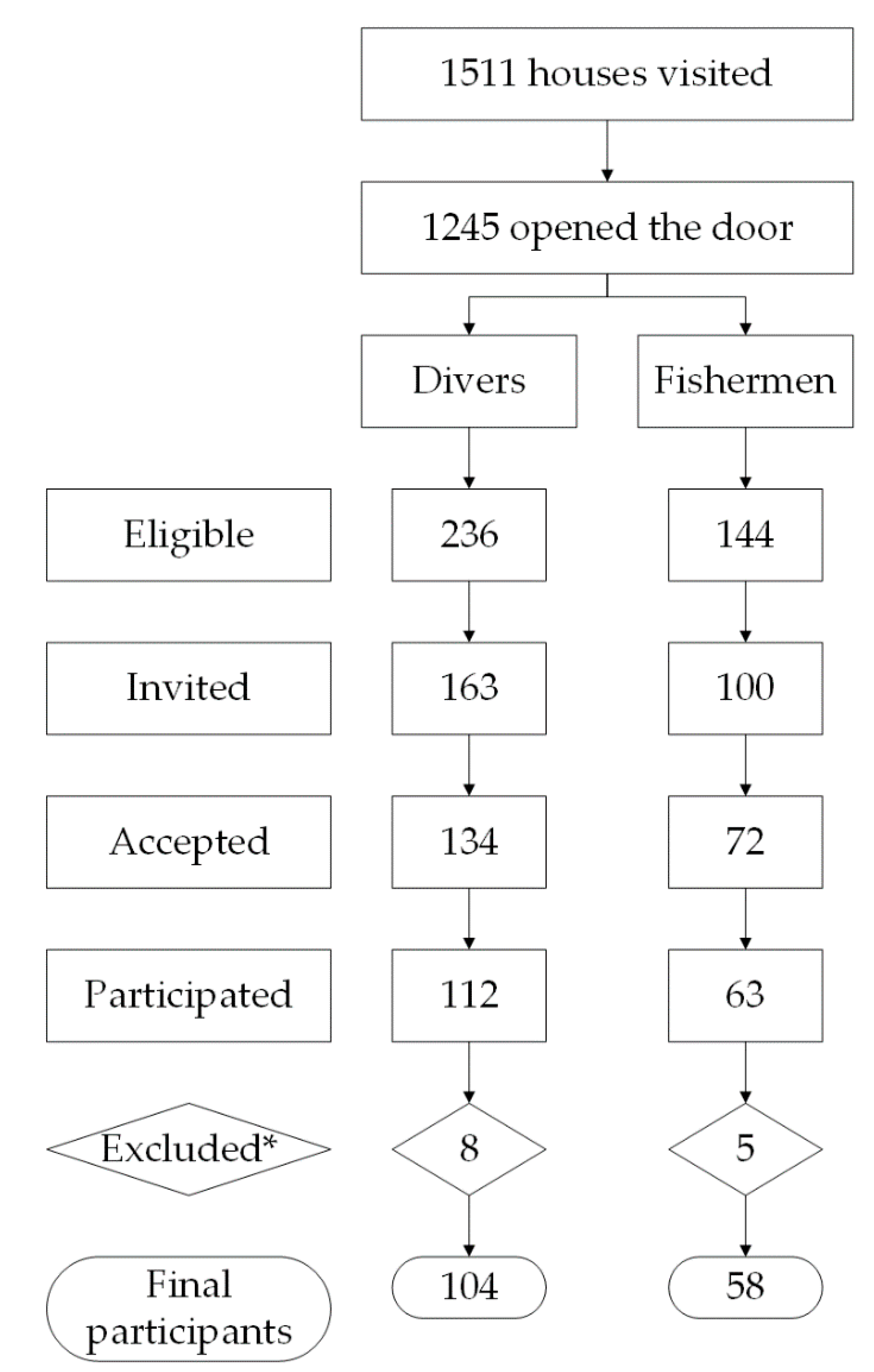
2.2.1. Recruitment
2.2.2. Data Collection and Data Collection Instruments
- (1)
- The Wisconsin Card Sorting Test (WCST) to evaluate executive function, mainly cognitive flexibility and task-shifting [18,33]. In the WCST, the examiner presents a set of 4 stimulus cards on a table. The cards contain figures that differ in shape, color, and quantity. The task of the examinee is to sort response cards with the appropriate stimulus card, according to classification criteria that he must find out. The only instruction he gets is a positive or negative feedback for his classification. The test ends when the examinee manages to solve the task by completing six correct classification categories or when all 128 response cards are finished.
- (2)
- An adapted standardized questionnaire to assess socio-demographics, potential confounders [34,35], and work-related exposures using the following sources:
- -
- -
- The AUDIT-C questionnaire, corresponding to the first three questions on hazardous alcohol consumption from the World Health Organization’s (WHO) Alcohol Use Disorders Identification Test (AUDIT) [36].
- -
- The WHO STEPwise approach to noncommunicable disease risk factor surveillance (STEPS) Instrument [37] to assess smoking behavior.
- -
- The PHQ-9 (Patient Health Questionnaire-9), the Chilean validation for the diagnosis of depression in primary health care [38].
2.2.3. Variable Definition
2.2.4. Statistical Analysis
2.3. Ethics
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- FAO Food and Agriculture Organization of the United Nations. Voluntary Guidelines for Securing Sustainable Small-Scale Fisheries in the Context of Food Security and Poverty Eradication 2015. Available online: http://www.fao.org/3/i4356en/I4356EN.pdf (accessed on 16 March 2020).
- FAO Food and Agriculture Organization of the United Nations. Perfiles de Pesca y Acuicultura Por Países. La República de Chile 2010. Available online: http://www.fao.org/fishery/facp/CHL/es#CountrySector-SectorSocioEcoContribution (accessed on 16 March 2020).
- FAO Food and Agriculture Organization of the United Nations. El Buceo en la Pesca y la Acuicultura en América Latina y el Caribe 2017. Available online: http://www.fao.org/3/a-i7331s.pdf (accessed on 16 March 2020).
- Hermoso, M.I.; Martin, V.Y.; Stotz, W.; Gelcich, S.; Thiel, M. How Does the Diversity of Divers Affect the Design of Citizen Science Projects? Front. Mar. Sci. 2019, 6. [Google Scholar] [CrossRef]
- Garrido, M.A.; Parra, M.; Diaz, J.; Medel, J.; Nowak, D.; Radon, K. Occupational safety and health in a community of shellfish divers: A community-based participatory approach. J. Community Health 2020, 45, 569–578. [Google Scholar] [CrossRef]
- Gold, D.; Geater, A.; Aiyarak, S.; Wongcharoenyong, S.; Juengprasert, W.; Johnson, M.; Skinner, P. The indigenous fisherman divers of Thailand: Diving-related mortality and morbidity. Int. J. Occup. Saf. Ergon. 2000, 6, 147–167. [Google Scholar] [CrossRef] [Green Version]
- Huchim-Lara, O.; Salas, S.; Fraga, J.; Mendez, N.; Chin, W. Fishermen’s perceptions and attitudes toward risk diving and management issues in small-scale fisheries. AJHE 2016, 5, 1–10. [Google Scholar] [CrossRef]
- Westin, A.A.; Asvall, J.; Idrovo, G.; Denoble, P.; Brubakk, A.O. Diving behaviour and decompression sickness among Galapagos underwater harvesters. Undersea Hyperb. Med. 2005, 32, 175–184. [Google Scholar]
- Garrido Campos, M.A.; Hindelang, B.A.; De Carvalho, D.S.; Urzúa Finke, I.; Herrera, R.; Radon, K. Prevalence and risk factors for hearing loss in Chilean shellfish divers. Ann. Glob. Health 2018, 84, 442–449. [Google Scholar] [CrossRef]
- Levett, D.Z.; Millar, I.L. Bubble trouble: A review of diving physiology and disease. Postgrad. Med. J. 2008, 84, 571–578. [Google Scholar] [CrossRef]
- Vann, R.D.; Butler, F.K.; Mitchell, S.J.; Moon, R.E. Decompression illness. Lancet 2011, 377, 153–164. [Google Scholar] [CrossRef]
- Rosinska, J.; Lukasik, M.; Kozubski, W. Neurological complications of underwater diving. Neurol. Neurochir. Pol. 2015, 49, 45–51. [Google Scholar] [CrossRef]
- Bast-Pettersen, R.; Skare, O.; Nordby, K.C.; Skogstad, M. A twelve-year longitudinal study of neuropsychological function in non-saturation professional divers. Int. Arch. Occup. Environ. Health 2015, 88, 669–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reuter, M.; Tetzlaff, K.; Hutzelmann, A.; Fritsch, G.; Steffens, J.C.; Bettinghausen, E.; Heller, M. MR imaging of the central nervous system in diving-related decompression illness. Acta Radiol. 1997, 38, 940–944. [Google Scholar] [CrossRef]
- Gao, G.K.; Wu, D.; Yang, Y.; Yu, T.; Xue, J.; Wang, X.; Jiang, Y.P. Cerebral magnetic resonance imaging of compressed air divers in diving accidents. Undersea Hyperb. Med. 2009, 36, 33–41. [Google Scholar]
- Mitchell, S.; Gorman, D. The pathophysiology of cerebral arterial gas embolism. J. Extra Corpor. Technol. 2002, 34, 18–23. [Google Scholar]
- Niendam, T.A.; Laird, A.R.; Ray, K.L.; Dean, Y.M.; Glahn, D.C.; Carter, C.S. Meta-analytic evidence for a superordinate cognitive control network subserving diverse executive functions. Cogn. Affect. Behav. Neurosci. 2012, 12, 241–268. [Google Scholar] [CrossRef]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The unity and diversity of executive functions and their contributions to complex “Frontal Lobe” tasks: A latent variable analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ardila, A.; Fatima, S.; Rosselli, M. Introduction. In Dysexecutive Syndromes Clinical and Experimental Perspectives; Ardila, A., Fatima, S., Rosselli, M., Eds.; Springer Nature Switzerland AG: Cham, Switzerland, 2019; pp. v–ix. [Google Scholar]
- Dajani, D.R.; Uddin, L.Q. Demystifying cognitive flexibility: Implications for clinical and developmental neuroscience. Trends Neurosci. 2015, 38, 571–578. [Google Scholar] [CrossRef] [Green Version]
- Fatima, S. Executive Dysfunctions in Autism Spectrum Disorders. In Dysexecutive Syndromes Clinical and Experimental Perspectives; Ardila, A., Fatima, S., Rosselli, M., Eds.; Springer Nature Switzerland AG: Cham, Switzerland, 2019; pp. 61–79. [Google Scholar]
- Taylor, C.L.; Macdiarmid, J.I.; Ross, J.A.; Osman, L.M.; Watt, S.J.; Adie, W.; Crawford, J.R.; Lawson, A. Objective neuropsychological test performance of professional divers reporting a subjective complaint of “forgetfulness or loss of concentration”. Scand. J. Work Environ. Health 2006, 32, 310–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ergen, M.; Uslu, A.; Caglar, O.; Akca-Kalem, S.; Cimsit, M.; Gurvit, H. Evaluation of cognitive performance in professional divers by means of event-related potentials and neuropsychology. Clin. Neurophysiol. 2017, 128, 579–588. [Google Scholar] [CrossRef]
- Coco, M.; Buscemi, A.; Perciavalle, V.; Maci, T.; Galvano, G.; Scavone, A.M.F.; Perciavalle, V.; Di Corrado, D. Cognitive deficits and white matter alterations in highly trained scuba divers. Front. Psychol. 2019, 10, 2376. [Google Scholar] [CrossRef]
- Tetzlaff, K.; Friege, L.; Hutzelmann, A.; Reuter, M.; Holl, D.; Leplow, B. Magnetic resonance signal abnormalities and neuropsychological deficits in elderly compressed-air divers. Eur. Neurol. 1999, 42, 194–199. [Google Scholar] [CrossRef]
- Shah, N.; Goyal, S. A study of neurocognitive and executive function of divers. J. Mar. Med. Soc. 2018, 20, 44–49. [Google Scholar] [CrossRef]
- Connolly, D.M.; Lee, V.M. Odds ratio meta-analysis and increased prevalence of white matter injury in healthy divers. Aerosp. Med. Hum. Perform. 2015, 86, 928–935. [Google Scholar] [CrossRef] [PubMed]
- Slosman, D.O.; De Ribaupierre, S.; Chicherio, C.; Ludwig, C.; Montandon, M.L.; Allaoua, M.; Genton, L.; Pichard, C.; Grousset, A.; Mayer, E.; et al. Negative neurofunctional effects of frequency, depth and environment in recreational scuba diving: The Geneva “memory dive” study. Br. J. Sports Med. 2004, 38, 108–114. [Google Scholar] [CrossRef] [Green Version]
- Hindelang, B.; Garrido, M.A.; Urzúa, I.; Radon, K. Prevalence and Risk Factors for Attention Deficits in Chilean Artisanal Shellfish Divers. Medical Doctorate Thesis, Technische Universität München, München, Germany, 2014. [Google Scholar]
- Murman, D.L. The impact of age on cognition. Semin. Hear. 2015, 36, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Ridderinkhof, K.R.; Span, M.M.; van der Molen, M.W. Perseverative behavior and adaptive control in older adults: Performance monitoring, rule induction, and set shifting. Brain Cogn. 2002, 49, 382–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Princiotta, D.; DeVries, M.; Goldstein, S. Executive functioning as a mediator of age-related cognitive decline in adults. In Handbook of Executive Functioning, 1st ed.; Goldstein, S., Naglieri, J.A., Eds.; Springer: New York, NY, USA, 2014; pp. 143–155. [Google Scholar]
- Rosselli, M.; Torres, V.L. Executive Dysfunction during Normal and Abnormal Aging. In Dysexecutive Syndromes Clinical and Experimental Pespectives; Ardila, A., Fatima, S., Rosselli, M., Eds.; Springer Nature Switzerland AG: Cham, Switzerland, 2019; pp. 158–176. [Google Scholar]
- Snyder, H.R. Major depressive disorder is associated with broad impairments on neuropsychological measures of executive function: A meta-analysis and review. Psychol. Bull. 2013, 139, 81–132. [Google Scholar] [CrossRef] [Green Version]
- Mukherjee, S. Alcoholism and its effects on the central nervous system. Curr. Neurovasc. Res. 2013, 10, 256–262. [Google Scholar] [CrossRef]
- Babor, T.F.; Higgins-Biddle, J.C.; Saunders, J.B.; Monteiro, M.G. AUDIT: The Alcohol Use Disorders Identification Test: Guidelines for Use in Primary Health Care 2001. Available online: https://www.who.int/publications-detail/audit-the-alcohol-use-disorders-identification-test-guidelines-for-use-in-primary-health-care (accessed on 7 December 2019).
- World Health Organization. WHO STEPS Instrument (Core and Expanded). Available online: https://www.who.int/ncds/surveillance/steps/STEPS_Instrument_v2.1.pdf (accessed on 16 March 2020).
- Baader, M.T.; Molina, F.J.L.; Venezian, B.S.; Rojas, C.C.; Farías, S.R.; Fierro-Freixenet, C.; Backenstrass, M.; Mundt, C. Validación y utilidad de la encuesta PHQ-9 (Patient Health Questionnaire) en el diagnóstico de depresión en pacientes usuarios de atención primaria en Chile. Rev. Chil. Neuro-Psiquiat. 2012, 50, 10–22. [Google Scholar] [CrossRef]
- Townsend, C.L.; Maynard, R.L. Effects on health of prolonged exposure to low concentrations of carbon monoxide. Occup. Environ. Med. 2002, 59, 708–711. [Google Scholar] [CrossRef] [Green Version]
- Peters, R.; Ee, N.; Peters, J.; Booth, A.; Mudway, I.; Anstey, K.J. Air pollution and dementia: A systematic review. J. Alzheimers Dis. 2019, 70, S145–S163. [Google Scholar] [CrossRef] [Green Version]
- Health and Safety Laboratory. Biological Monitoring Guidance Values. Gudance Sheet for: Carbon Monoxide (CO) in Breath. Available online: https://www.hsl.gov.uk/media/1188337/carbon%20monoxide%20(co)%20in%20breath.pdf (accessed on 15 February 2020).
- Ochoa Angrino, S.; Cruz Panesso, I. Wisconsin Card Sorting Test en el estudio del déficit de atención con hiperactividad, trastornos psiquiátricos, autismo y vejez. Univ. Psychol. 2007, 6, 637–648. [Google Scholar]
- Lange, F.; Seer, C.; Kopp, B. Cognitive flexibility in neurological disorders: Cognitive components and event-related potentials. Neurosci. Biobehav. Rev. 2017, 83, 496–507. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, C.; Bennett, M.; Lippmann, J.; Mitchell, S.J. Decompression Sickness: Manifestations. In Diving and Subaquatic Medicine, 5th ed.; Edmonds, C., Ed.; CRC Press: Boca Raton, FL, USA, 2015; pp. 141–151. [Google Scholar]
- Norambuena, P. Intervenciones Breves Para Reducir el Consumo de Alcohol Riesgoso. Guía Técnica Para Atención Primaria de Salud 2011. Available online: https://intervencionesbrevesenalcohol.files.wordpress.com/2014/11/01_guia-tecnica.pdf (accessed on 16 March 2020).
- Marquine, M.J.; Yassai-Gonzalez, D.; Perez-Tejada, A.; Umlauf, A.; Kamalyan, L.; Morlett Paredes, A.; Suarez, P.; Rivera Mindt, M.; Franklin, D.; Artiola, I.F.L.; et al. Demographically adjusted normative data for the Wisconsin Card Sorting Test-64 item: Results from the Neuropsychological Norms for the U.S.-Mexico Border Region in Spanish (NP-NUMBRS) project [published online ahead of print 3 January 2020]. Clin. Neuropsychol. 2020, 1–17. [Google Scholar] [CrossRef]
- Seo, J.; Chang, Y.; Jang, K.E.; Park, J.W.; Kim, Y.T.; Park, S.J.; Jeong, K.S.; Kim, A.; Kim, S.H.; Kim, Y. Altered executive function in the welders: A functional magnetic resonance imaging study. Neurotoxicol. Teratol. 2016, 56, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.J.; Bennett, M.H.; Bryson, P.; Butler, F.K.; Doolette, D.J.; Holm, J.R.; Kot, J.; Lafere, P. Consensus guideline: Pre-hospital management of decompression illness: Expert review of key principles and controversies. Undersea Hyperb. Med. 2018, 45, 273–286. [Google Scholar] [PubMed]
- Ministerio de Salud Gobierno de Chile. Encuesta Nacional de Salud 2016–2017. Segunda Entrega de Resultados 2018. Available online: https://www.minsal.cl/wp-content/uploads/2018/01/2-Resultados-ENS_MINSAL_31_01_2018.pdf (accessed on 16 March 2020).
- Petarli, G.B.; Cattafesta, M.; Sant’Anna, M.M.; Bezerra, O.; Zandonade, E.; Salaroli, L.B. Multimorbidity and complex multimorbidity in Brazilian rural workers. PLoS ONE 2019, 14, e0225416. [Google Scholar] [CrossRef] [Green Version]
- Collins, J.; Ward, B.M.; Snow, P.; Kippen, S.; Judd, F. Compositional, contextual, and collective community factors in mental health and well-being in Australian rural communities. Qual. Health Res. 2017, 27, 677–687. [Google Scholar] [CrossRef]
- Marzuki, N.; Abdulrahman, S.; Khan, A. Prevalence and risk factors of depression among a population of economically-disadvantaged fishermen in Teluk Bahang, Penang. J. Adv. Med. Med. Res. 2017, 23, 1–20. [Google Scholar] [CrossRef]
- Jiang, H.; Li, S.; Yang, J. Work stress and depressive symptoms in fishermen with a smoking habit: A mediator role of nicotine dependence and possible moderator role of expressive suppression and cognitive reappraisal. Front. Psychol. 2018, 9, 386. [Google Scholar] [CrossRef]
- Wang, J.; Chen, C.Y.; Lai, L.J.; Chen, M.L.; Chen, M.Y. The effectiveness of a community-based health promotion program for rural elders: A quasi-experimental design. Appl. Nurs. Res. 2014, 27, 181–185. [Google Scholar] [CrossRef]
- Bustos, B.; Délano, J.; Prieto, M. Chilote tipo salmón. Relaciones entre comodificación de la naturaleza y procesos de producción identitaria. El caso de la región de Los Lagos y la industria salmonera. Estud. Atacam. 2019, 63, 383–402. [Google Scholar] [CrossRef]
- Garrido, A.; Parra, M.; Medel, J.; Díaz, J.; Radon, K. Temporal migration due to harmful algal bloom among artisanal fishermen in Southern Chile. In Proceedings of the 1st Exceed Conference Summary Forced Migration–Environmental and Socioeconomic Dimensions–Perspectives of Higher Education Institutions in Development Cooperation, Berlin, Germany, 19–20 October 2016; p. 48. [Google Scholar]
- Darwish, H.; Farran, N.; Assaad, S.; Chaaya, M. Cognitive reserve factors in a developing country: Education and occupational attainment lower the risk of dementia in a sample of Lebanese older adults. Front. Aging Neurosci. 2018, 10, 277. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.X.; MacDonald, S.W.; Dekhtyar, S.; Fratiglioni, L. Association of lifelong exposure to cognitive reserve-enhancing factors with dementia risk: A community-based cohort study. PLoS Med. 2017, 14, e1002251. [Google Scholar] [CrossRef]


{kind=link}
| Total N = 162 | Fishermen 1 N = 58 | Divers 2 N = 104 | pChi 2 (Divers vs. Fishermen) | |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| Age (years) | 0.05 | |||
| 18–39 | 51 (31.5) | 25 (43.1) | 26 (25.0) | |
| 40–49 | 57 (35.2) | 18 (31.0) | 39 (37.5) | |
| 50–59 | 54 (33.3) | 15 (25.9) | 39 (37.5) | |
| Education | 0.61 | |||
| Incomplete primary | 32 (19.8) | 10 (17.2) | 22 (21.2) | |
| Complete primary & incomplete secondary | 70 (43.2) | 28 (48.3) | 42 (40.4) | |
| Complete secondary & superior | 60 (37.0) | 20 (34.5) | 40 (38.5) | |
| Community | 0.49 | |||
| A | 133 (82.1) | 46 (79.3) | 87 (83.7) | |
| B | 29 (17.9) | 12 (20.7) | 17 (16.3) | |
| Depressive symptoms3 | 23 (14.2) | 14 (24.1) | 9 (8.7) | <0.01 |
| Hazardous alcohol consumption 4 | 61 (37.7) | 26 (44.8) | 35 (33.7) | 0.16 |
| N; Median (Min–Max) | N; Median (Min–Max) | p (Median test) | ||
| History of decompression illness score5 | n/a | n/a | 103; 2.00 (0.00–18.00) | n/a |
| % change in exhaled CO6 | 60; 0.00 (−80.00–400.00) | 20; 0.00 (−40.00–150.00) | 40; 33.33 (−80.00–400.00) | 0.02 |
| WCST categories completed7 | 162; 2.50 (0–6) | 58; 2.00 (0–6) | 104; 3.00 (0–6) | 0.41 |
| % Perseverative Responses | % Perseverative Errors | % Non-Perseverative Errors | ||||
|---|---|---|---|---|---|---|
| Median (Min–Max) | p | Median (Min–Max) | p | Median (Min–Max) | p | |
| Age (years) | <0.01 # | <0.01 # | 0.94 # | |||
| 18–39 | 17.0 (2.00–80.00) | 16.0 (2.00–63.00) | 20.0 (4.00–53.00) | |||
| 40–49 | 22.0 (3.00–98.00) | 20.0 (3.00–74.00) | 22.0 (2.00–54.00) | |||
| 50–59 | 28.0 (5.00–98.00) | 24.0 (5.00–73.00) | 22.0 (2.00–66.00) | |||
| Education | <0.01 # | <0.01 # | 0.13 # | |||
| Incomplete primary | 32.5 (8.00–98.00) | 28.0 (7.00–73.00) | 15.0 (2.00–59.00) | |||
| Complete primary & incomplete secondary | 22.0 (3.00–97.00) | 20.0 (3.00–73.00) | 22.5 (2.00–66.00) | |||
| Complete secondary & superior | 19.0 (2.00–98.00) | 16.5 (2.00–74.00) | 20.5 (2.00–53.00) | |||
| Occupation | 0.29~ | 0.24~ | 0.30~ | |||
| Fishermen | 25.0 (2.00–98.00) | 22.0 (2.00–74.00) | 20.0 (2.00–54.00) | |||
| Diver | 21.0 (3.00–98.00) | 19.0 (3.00–73.00) | 22.5 (2.00–66.00) | |||
| Community | 0.79~ | 0.85~ | 0.25~ | |||
| B | 21.0 (5.00–98.00) | 20.0 (5.00–73.00) | 19.0 (2.00–54.00) | |||
| A | 22.0 (2.00–98.00) | 20.0 (2.00–74.00) | 22.0 (2.00–66.00) | |||
| Depressive symptoms1 | 0.05~ | 0.05~ | 0.20~ | |||
| No | 21.0 (3.00–98.00) | 19.0 (3.00–74.00) | 22.0 (2.00–66.00) | |||
| Yes | 34.0 (2.00–97.00) | 29.0 (2.00–73.00) | 18.0 (2.00–54.00) | |||
| Hazardous alcohol consumption2 | 0.22~ | 0.31~ | 0.60~ | |||
| No | 20.0 (3.00–98.00) | 19.0 (3.00–74.00) | 22.0 (2.00–66.00) | |||
| Yes | 26.0 (2.00–98.00) | 22.0 (2.00–73.00) | 20.0 (2.00–52.00) | |||
| History of decompression illness score 3 (Spearman’s coefficient) | 0.34 | <0.01 | 0.34 | <0.01 | −0.17 | 0.09 |
| % Perseverative Responses | % Perseverative Errors | % Non-Perseverative Errors | ||||
|---|---|---|---|---|---|---|
| Adjusted R2 (pAnova) | 0.134 (p = 0.002) | 0.132 (p = 0.002) | 0.013 (p = 0.284) | |||
| B | 95% CI | B | 95% CI | B | 95% CI | |
| Age (years) | ||||||
| <40 | 0 | 0 | 0 | |||
| 40–49 | 12.95 | 0.00–25.90 | 10.06 | 0.64–19.47 | 0.01 | −6.73–6.75 |
| 50–59 | 14.75 | 1.34–28.16 | 10.97 | 1.22–20.73 | 3.62 | −3.36–10.60 |
| Depressive symptoms 1 yes vs. no | 11.18 | −6.17–28.54 | 7.74 | −4.89–20.36 | −6.67 | −15.71–2.36 |
| Hazardous alcohol consumption 2 yes vs. no | 3.45 | −6.81–13.71 | 2.43 | −5.03–9.89 | −0.08 | −5.42–5.26 |
| History of decompression illness score3 | 1.25 | 0.20–2.30 | 0.88 | 0.12–1.64 | −0.46 | −1.00–0.09 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garrido, M.A.; Mark, L.; Parra, M.; Nowak, D.; Radon, K. Executive Function among Chilean Shellfish Divers: A Cross-Sectional Study Considering Working and Health Conditions in Artisanal Fishing. Int. J. Environ. Res. Public Health 2021, 18, 5923. https://doi.org/10.3390/ijerph18115923
Garrido MA, Mark L, Parra M, Nowak D, Radon K. Executive Function among Chilean Shellfish Divers: A Cross-Sectional Study Considering Working and Health Conditions in Artisanal Fishing. International Journal of Environmental Research and Public Health. 2021; 18(11):5923. https://doi.org/10.3390/ijerph18115923
Chicago/Turabian StyleGarrido, Marie Astrid, Lorenz Mark, Manuel Parra, Dennis Nowak, and Katja Radon. 2021. "Executive Function among Chilean Shellfish Divers: A Cross-Sectional Study Considering Working and Health Conditions in Artisanal Fishing" International Journal of Environmental Research and Public Health 18, no. 11: 5923. https://doi.org/10.3390/ijerph18115923
APA StyleGarrido, M. A., Mark, L., Parra, M., Nowak, D., & Radon, K. (2021). Executive Function among Chilean Shellfish Divers: A Cross-Sectional Study Considering Working and Health Conditions in Artisanal Fishing. International Journal of Environmental Research and Public Health, 18(11), 5923. https://doi.org/10.3390/ijerph18115923