
Heat Exposure and Multiple Sclerosis—A Regional and Temporal Analysis


Abstract
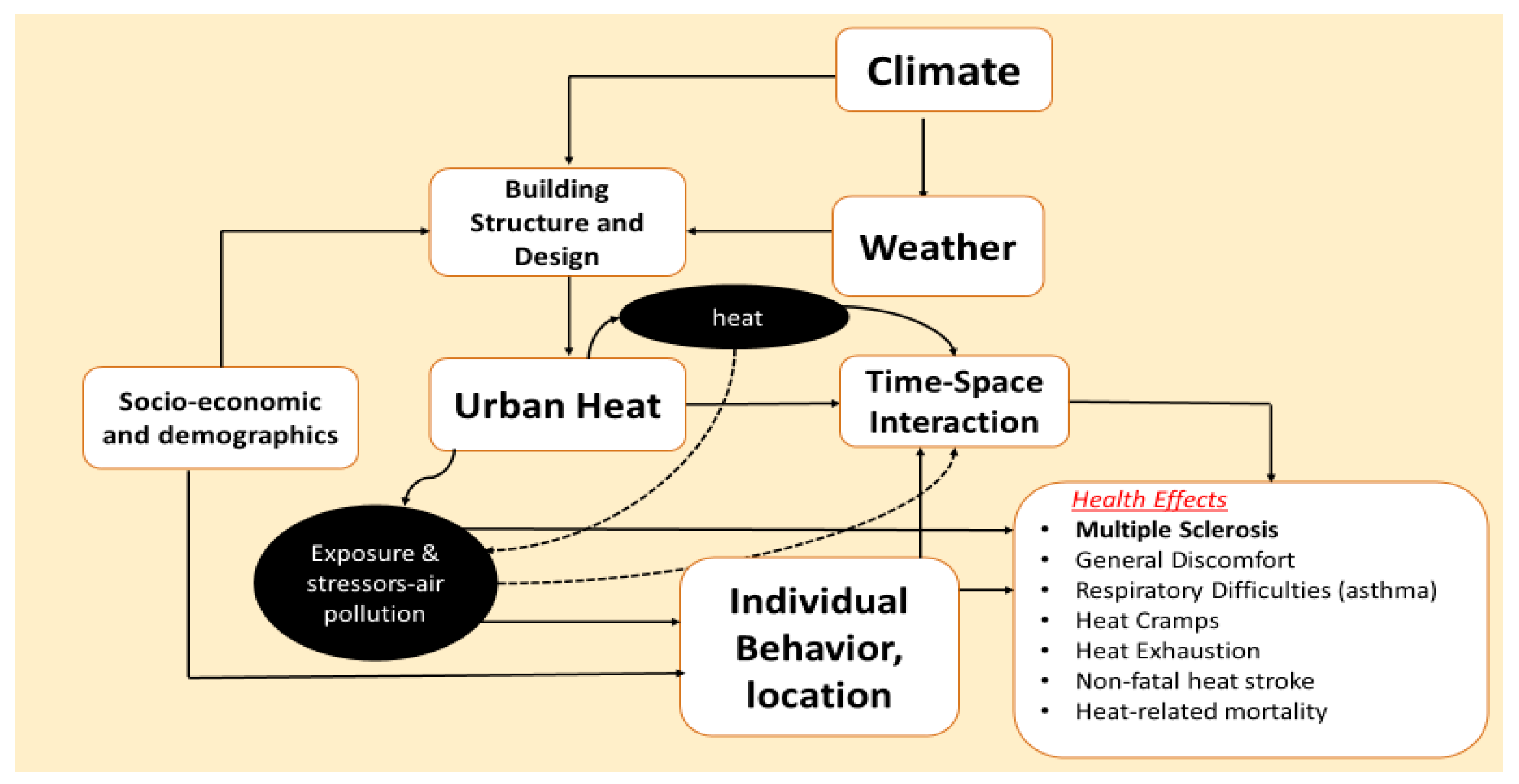
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Method
2.3. Meteorological Data
2.4. Statistical Analysis
3. Results
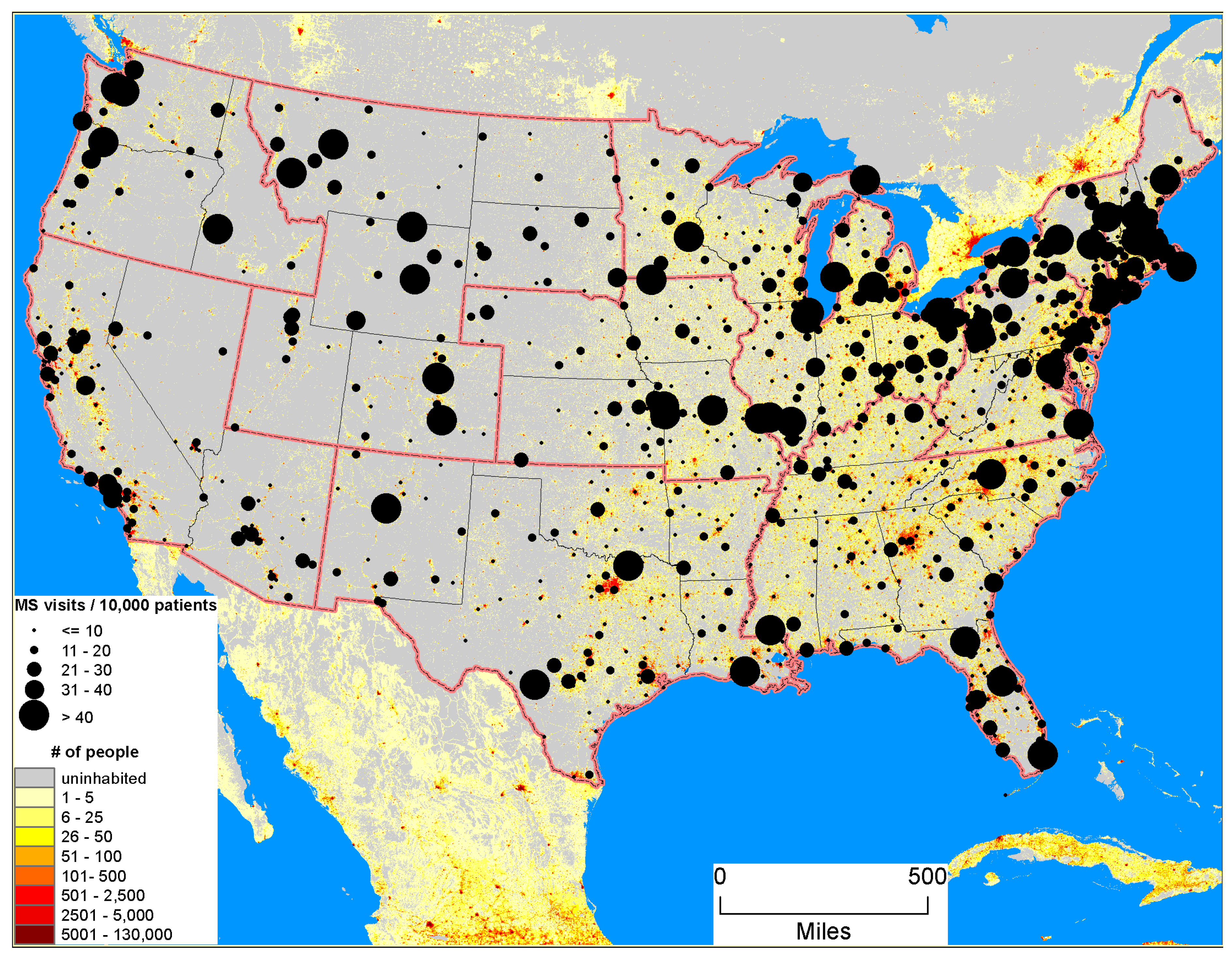
3.1. Study Population & Clinic Visits
3.2. Seasonal and Regional Trends in Meteorological Conditions
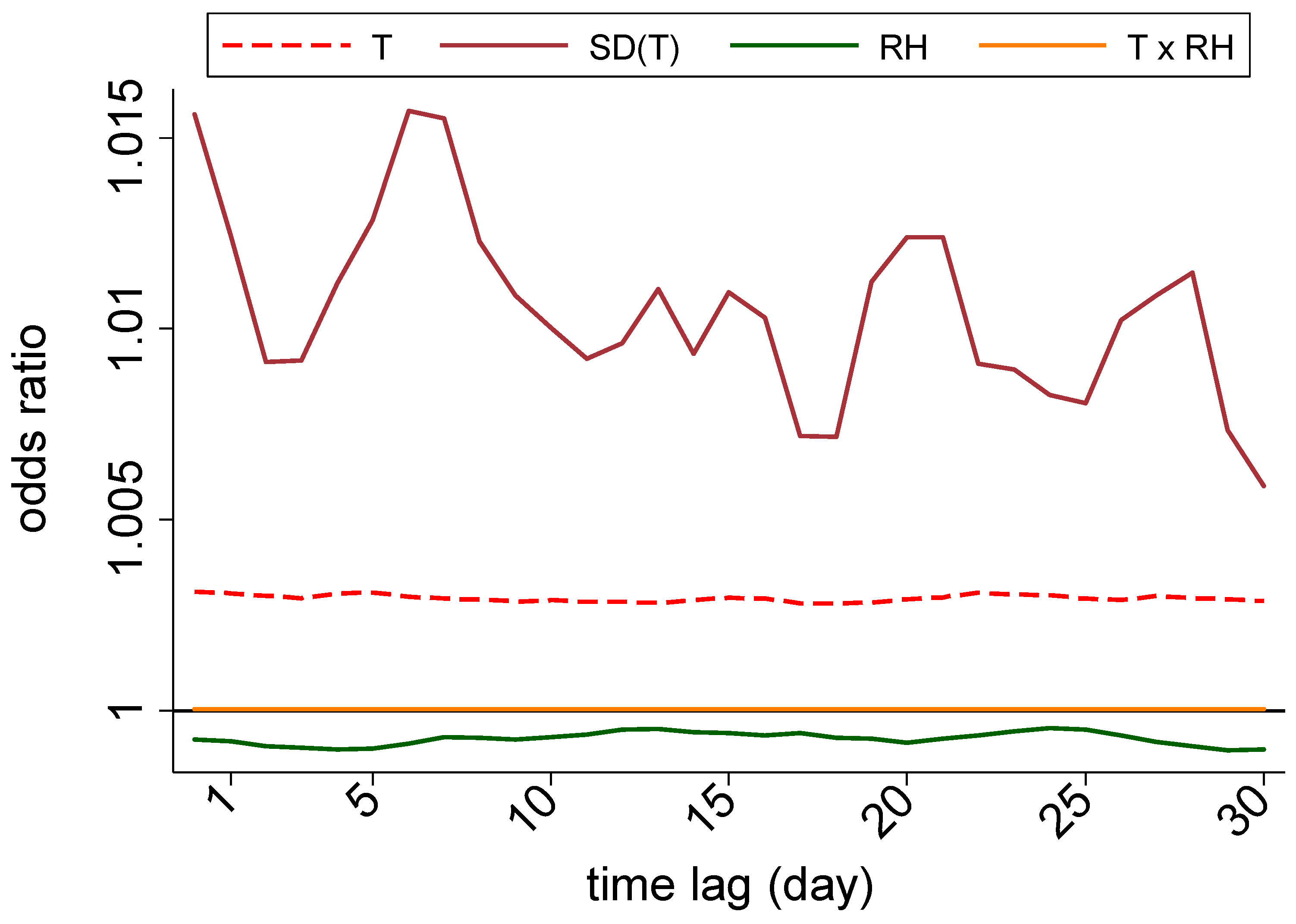
3.3. Nationwide Associations
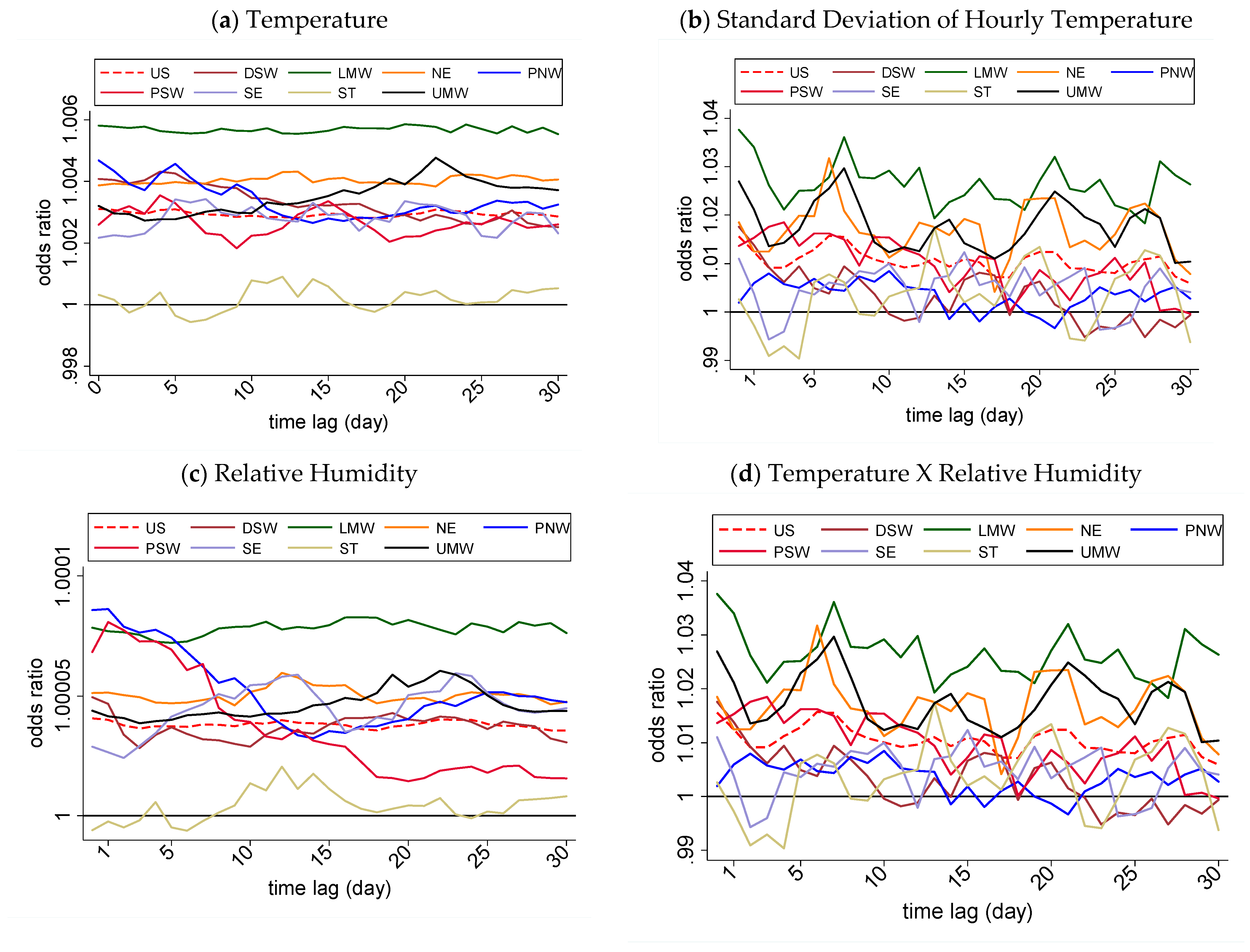
3.4. Region-Specific Associations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Davis, S.L.; Wilson, T.E.; White, A.T.; Frohman, E.M. Thermoregulation in multiple sclerosis. J. Appl. Physiol. 2010, 109, 1531–1537. [Google Scholar] [CrossRef]
- Dobson, R.; Giovannoni, G. Multiple sclerosis—A review. Eur. J. Neurol. 2019, 26, 27–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramagopalan, S.V.; Dobson, R.; Meier, U.C.; Giovannoni, G. Multiple sclerosis: Risk factors, prodromes, and potential causal pathways. Lancet Neurol. 2010, 9, 727–739. [Google Scholar] [CrossRef]
- Tarzjani, S.P.C.; Fazeli, S.A.S.; Sanati, M.H.; Nabavi, S.M. Heat Shock Protein 70 and The Risk of Multiple Sclerosis in The Iranian Population. Cell J. 2018, 20, 599–603. [Google Scholar]
- Moghaddam, V.K.; Sarmadi, M.; Tatari, M.; Najafi, F.; Esmaeili, A.; Hadei, M. Epidemiology of Multiple Sclerosis in Torbat-e Heydarieh (Northeast. of Iran.) during 1982–2016. Mult. Scler. Relat. Disord. 2018, 24, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Warren, S.; Warren, K.G.; WHO. Multiple Sclerosis. 2001. Available online: https://apps.who.int/iris/handle/10665/42394 (accessed on 17 August 2019).
- Romberg, A.; Ikonen, A.; Ruutiainen, J.; Virtanen, A.; Hämäläinen, P. The effects of heat stress on physical functioning in persons with multiple sclerosis. J. Neurol. Sci. 2012, 319, 42–46. [Google Scholar] [CrossRef]
- Guthrie, T.C.; Nelson, D.A. Influence of temperature changes on multiple sclerosis: Critical review of mechanisms and research potential. J. Neurol. Sci. 1995, 129, 1–8. [Google Scholar] [CrossRef]
- Qeshmi, S.A.; Dabbagh, F.; Haghighi, A.B.; Ghasemi, Y. Bioinformatics evaluation of the possibility of heat shock proteins as autoantigens in multiple sclerosis based on molecular mimicry hypothesis. J. Neuroimmunol. 2016, 295, 100–121. [Google Scholar] [CrossRef]
- Mansilla, M.J.; Montalban, X.; Espejo, C. Heat Shock Protein 70: Roles in Multiple Sclerosis. Mol. Med. 2012, 18, 1018–1028. [Google Scholar] [CrossRef]
- Boiocchi, C.; Osera, C.; Monti, M.C.; Ferraro, O.E.; Govoni, S.; Cuccia, M.; Montomoli, C.; Pascale, A.; Bergamaschi, R. Are Hsp70 protein expression and genetic polymorphism implicated in multiple sclerosis inflammation? J. Neuroimmunol. 2014, 268, 84–88. [Google Scholar] [CrossRef]
- Petit, B.; Giraudet, F.; Béchon, C.; Bardin, L.; Avan, P.; Boespflug-Tanguy, O.; Bégou, M. Mice with a deletion of the major central myelin protein exhibit hypersensitivity to noxious thermal stimuli: Involvement of central sensitization. Neurobiol. Dis. 2014, 65, 55–68. [Google Scholar] [CrossRef] [PubMed]
- Warshawsky, I.; Rudick, R.A.; Staugaitis, S.M.; Natowicz, M.R. Primary progressive multiple sclerosis as a phenotype of a PLP1 gene mutation. Ann. Neurol. 2005, 58, 470–473. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, M.A.; O’Reilly, P.M. Temporal Influences on Relapses of Multiple Sclerosis. Eur. Neurol. 1991, 31, 391–395. [Google Scholar] [CrossRef]
- Leavitt, V.M.; Sumowski, J.F.; Chiaravalloti, N.; DeLuca, J. Warmer outdoor temperature is associated with worse cognitive status in multiple sclerosis. Neurology 2012, 78, 964–968. [Google Scholar] [CrossRef] [PubMed]
- Tataru, N.; Vidal, C.; Decavel, P.; Berger, E.; Rumbach, L. Limited Impact of the Summer Heat Wave in France (2003) on Hospital Admissions and Relapses for Multiple Sclerosis. Neuroepidemiology 2006, 27, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Karimi, A.; Delpisheh, A.; Ashtari, F.; Sayehmiri, K.; Meamar, R. The relationship between the amount of radiation, relative humidity, and temperature with the risk of multiple sclerosis in isfahan province, iran, during the years 2001–2014. J. Isfahan Med. Sch. 2017, 35, 434–439. [Google Scholar]
- Karl, T.R.; Kukla, G.; Razuvayev, V.N.; Changery, M.J.; Quayle, R.G.; Heim, R.R.; Easterling, D.R.; Bin Fu, C. Global warming: Evidence for asymmetric diurnal temperature change. Geophys. Res. Lett. 1991, 18, 2253–2256. [Google Scholar] [CrossRef]
- ESRI; ArcGIS. Redlands, CA: Environmental Systems Research Institute; Version 10.8; Environmental Systems Research Institute: Redlands, CA, USA, 2019. [Google Scholar]
- NCDC. NOAA National Operational Model. Archive & Distribution System. 2015. Available online: http://nomads.ncdc.noaa.gov/ (accessed on 2 December 2015).
- STATA. STATA/MP 14.2—Data Analysis and Statistical Software; Stata Corp LP, College Station: College Station, TX, USA, 2017. [Google Scholar]
- Lam, T.; VoPham, T.; Munger, K.L.; Laden, F.; Hart, J.E. Long-term effects of latitude, ambient temperature, and ultraviolet radiation on the incidence of multiple sclerosis in two cohorts of US women. Environ. Epidemiol. 2020, 4, e0105. [Google Scholar] [CrossRef]
- Diniz, F.R.; Frony-Macedo, A.L.; Piacenti-Silva, M. Influence of particulate matter and meteorological conditions on multiple sclerosis relapse: A preliminary study in São Paulo, Brazil. Arch. Health Investig. 2017, 6. [Google Scholar] [CrossRef] [Green Version]
- Salvi, F.; Bartolomei, I.; Smolensky, M.H.; Lorusso, A.; Barbarossa, E.; Malagoni, A.M.; Zamboni, P.; Manfredini, R. A seasonal periodicity in relapses of multiple sclerosis? A single-center, population-based, preliminary study conducted in Bologna, Italy. BMC Neurol. 2010, 10, 105. [Google Scholar] [CrossRef] [Green Version]
- Hopkins, C.E.; Swank, R.L. Multiple sclerosis and the local weather; a four-year study of correlation between multiple sclerosis exacerbation and local weather factors in Montreal. A.M.A. Arch. Neurol. Psychiatry 1955, 74, 203–207. [Google Scholar] [CrossRef]
- Byun, S.; Myung, W.; Kim, H.; Lee, H. Association between diurnal temperature range and emergency department visits for multiple sclerosis: A time-stratified case-crossover study. Sci. Total Environ. 2020, 720, 137565. [Google Scholar] [CrossRef] [PubMed]
- Dendrou, C.; Fugger, L.; Friese, M.A. Immunopathology of multiple sclerosis. Nat. Rev. Immunol. 2015, 15, 545–558. [Google Scholar] [CrossRef] [PubMed]
- Secor, V.H.; Secor, W.E.; Gutekunst, C.-A.; Brown, M.A. Mast Cells Are Essential for Early Onset and Severe Disease in a Murine Model of Multiple Sclerosis. J. Exp. Med. 2000, 191, 813–822. [Google Scholar] [CrossRef] [Green Version]
- Qiu, H.; Yu, I.T.-S.; Tse, L.A.; Chan, E.Y.Y.; Wong, T.W.; Tian, L. Greater temperature variation within a day associated with increased emergency hospital admissions for asthma. Sci. Total Environ. 2015, 505, 508–513. [Google Scholar] [CrossRef]
- Kim, J.; Lim, Y.; Kim, H. Outdoor temperature changes and emergency department visits for asthma in Seoul, Korea: A time-series study. Environ. Res. 2014, 135, 15–20. [Google Scholar] [CrossRef]
- Xu, Z.; Huang, C.; Su, H.; Turner, L.R.; Qiao, Z.; Tong, S. Diurnal temperature range and childhood asthma: A time-series study. Environ. Health 2013, 12, 12. [Google Scholar] [CrossRef] [Green Version]
- Li, K.; Ni, H.; Yang, Z.; Wang, Y.; Ding, S.; Wen, L.; Yang, H.; Cheng, J.; Su, H. Effects of temperature variation between neighbouring days on daily hospital visits for childhood asthma: A time-series analysis. Public Health 2016, 136, 133–140. [Google Scholar] [CrossRef]
- Kenny, G.P.; Yardley, J.; Brown, C.; Sigal, R.J.; Jay, O. Heat stress in older individuals and patients with common chronic diseases. Can. Med. Assoc. J. 2010, 182, 1053–1060. [Google Scholar] [CrossRef] [Green Version]
- Kovats, R.S.; Hajat, S. Heat Stress and Public Health: A Critical Review. Annu. Rev. Public Health 2008, 29, 41–55. [Google Scholar] [CrossRef]
- Hori, S.; Ohnaka, M.; Shiraki, K.; Tsujita, J.; Yoshimura, H.; Saito, N.; Panata, M. Comparison of physical characteristics, body temperature and basal metabolism between Thai and Japanese in a neutral temperature zone. Jpn. J. Physiol. 1977, 27, 525–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hori, S.; Tsujita, J.; Tanaka, N.; Mayuzumi, M. Studies on heat tolerance of subtropical natives after migration to a temperate zone. Int. J. Biometeorol. 1978, 22, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, G.; Mochizuki, H.; Kanzaki, M.; Kaida, K.; Motoyoshi, K.; Kamakura, K. Seasonal variation of multiplesclerosis exacerbations in Japan. Neurol. Sci. 2004, 24, 417–419. [Google Scholar] [CrossRef] [PubMed]
- Wood, B.; Van Der Mei, I.A.F.; Ponsonby, A.-L.; Pittas, F.; Quinn, S.; Dwyer, T.; Lucas, R.M.; Taylor, B. Prevalence and concurrence of anxiety, depression and fatigue over time in multiple sclerosis. Mult. Scler. J. 2013, 19, 217–224. [Google Scholar] [CrossRef]
- Bakalidou, D.; Giannopoulos, S.; Stamboulis, E.; Voumvourakis, K. Effect of seasonal fluctuation of ambient temperature on fatigue in multiple sclerosis patients living in Attica, Greece. J. Clin. Neurosci. 2014, 21, 1188–1191. [Google Scholar] [CrossRef]
- Freti, L.; Condemi, V.; Mazza, M.; Di Nicola, M.; Janiri, L.; Antonietti, A.; Gestro, M.; Solimene, U. Meteorosensitivity in a Group of Patients Affected by Multiple Sclerosisand Hospitalized in a Rehabilitation Facility: An Observational Study. Altern. Integr. Med. 2017, 6, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Amezcua, L.; McCauley, J.L. Race and ethnicity on MS presentation and disease course. Mult. Scler. J. 2020, 26, 561–567. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Region | Mean | CI |
|---|---|---|
| DSW | 25.4 | 9.7–41.1 |
| LMW | 15.1 | 11.2–18.9 |
| NE | 64.0 | −16.7–144.8 |
| PNW | 67.6 | −24.0–159.2 |
| PSW | 25.2 | 3.1–47.2 |
| SE | 41.7 | −10.3–93.7 |
| ST | 46.8 | −19.0–112.5 |
| UMW | 24.6 | 13.4–35.8 |
| Total | 39.4 | 17.6–61.1 |
| Month | DSW | LMW | NE | PNW | PSW | SE | ST | UMW | Total |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 8.2 | 7.7 | 7.9 | 8.1 | 8.3 | 7.8 | 8.6 | 8.0 | 8.0 |
| 2 | 7.9 | 7.5 | 7.4 | 7.7 | 7.9 | 8.0 | 7.8 | 7.6 | 7.7 |
| 3 | 8.9 | 8.8 | 9.0 | 8.8 | 9.1 | 8.9 | 9.0 | 8.9 | 8.9 |
| 4 | 8.3 | 8.6 | 8.6 | 8.3 | 8.6 | 8.2 | 8.4 | 8.5 | 8.5 |
| 5 | 8.4 | 8.6 | 8.8 | 8.7 | 8.7 | 8.3 | 8.4 | 8.8 | 8.6 |
| 6 | 8.5 | 8.5 | 8.5 | 8.5 | 8.5 | 8.3 | 8.3 | 8.4 | 8.4 |
| 7 | 8.3 | 8.4 | 8.3 | 8.0 | 8.3 | 8.3 | 8.0 | 8.4 | 8.3 |
| 8 | 9.2 | 9.0 | 8.6 | 9.0 | 8.7 | 9.0 | 8.8 | 8.9 | 8.8 |
| 9 | 8.3 | 8.4 | 8.4 | 8.2 | 8.1 | 8.3 | 8.1 | 8.2 | 8.3 |
| 10 | 8.6 | 8.9 | 8.8 | 8.8 | 8.4 | 8.8 | 8.5 | 8.6 | 8.7 |
| 11 | 8.0 | 8.1 | 8.1 | 8.2 | 7.9 | 8.3 | 7.9 | 8.0 | 8.1 |
| 12 | 7.6 | 7.4 | 7.6 | 7.8 | 7.7 | 7.7 | 8.0 | 7.8 | 7.7 |
| Total | 100 (53,191) | 100 (54,100) | 100 (119,781) | 100 (44,443) | 100 (52,531) | 100 (56,871) | 100 (55,128) | 100 (94,030) | 100 (530,075) |
| Month | US | DSW | LMW | NE | PNW | PSW | SE | ST | UMW |
|---|---|---|---|---|---|---|---|---|---|
| Jan | 1.5 (9.0) | 4.9 (7.8) | −2.1 (6.9) | −2.1 (6.5) | 1.4 (6.6) | 9.4 (5.2) | 5.1 (6.8) | 14.7 (6.3) | −6.3 (7.2) |
| Feb | 3.2 (8.6) | 6.5 (8.6) | 0.1 (6.8) | −0.3 (5.5) | 2.2 (6.1) | 9.9 (4.6) | 7.2 (6.2) | 16.2 (5.8) | −4.6 (6.5) |
| Mar | 7.9 (7.8) | 11.6 (7.4) | 6.8 (7.0) | 4.3 (6.1) | 5.3 (4.8) | 12.6 (4.6) | 11.6 (5.9) | 18.2 (4.6) | 1.8 (7.2) |
| Apr | 12.9 (6.7) | 15.9 (7.3) | 12.9 (5.4) | 10.4 (5.2) | 8.1 (4.3) | 15.0 (5.4) | 16.9 (4.4) | 21.9 (3.3) | 7.9 (5.4) |
| May | 17.7 (5.9) | 20.0 (6.6) | 18.3 (5.0) | 16.0 (4.6) | 11.9 (4.2) | 18.5 (6.0) | 21.0 (4.0) | 24.6 (2.5) | 14.5 (5.3) |
| Jun | 22.0 (5.3) | 25.4 (5.1) | 23.4 (3.6) | 20.1 (4.0) | 15.5 (4.0) | 21.8 (6.9) | 25.2 (2.8) | 27.1 (1.7) | 19.2 (4.0) |
| Jul | 24.0 (4.5) | 26.3 (4.5) | 24.9 (3.7) | 22.9 (3.5) | 19.7 (4.5) | 23.9 (7.1) | 25.8 (2.7) | 27.5 (1.6) | 21.9 (3.5) |
| Aug | 23.3 (4.6) | 26.4 (5.0) | 23.9 (3.3) | 21.5 (3.1) | 19.2 (4.0) | 23.6 (6.6) | 25.5 (2.7) | 27.8 (1.6) | 20.9 (3.1) |
| Sep | 19.8 (5.3) | 22.4 (5.5) | 19.2 (4.2) | 17.8 (4.3) | 16.2 (3.8) | 22.2 (5.8) | 22.4 (3.5) | 26.5 (2.1) | 16.3 (4.3) |
| Oct | 14.0 (6.2) | 16.3 (6.9) | 12.7 (4.9) | 12.2 (4.7) | 10.0 (4.5) | 17.4 (4.9) | 16.3 (4.7) | 23.1 (4.1) | 9.7 (4.9) |
| Nov | 8.2 (7.0) | 10.2 (7.5) | 6.4 (5.7) | 6.2 (5.0) | 4.6 (6.0) | 12.6 (4.8) | 10.5 (5.2) | 18.7 (5.2) | 3.1 (5.9) |
| Dec | 3.6 (8.1) | 5.3 (8.2) | 0.6 (6.1) | 1.5 (5.6) | 0.9 (7.0) | 8.9 (5.0) | 7.1 (5.9) | 16.4 (6.1) | −3.0 (6.6) |
| Total | 13.2 (10.4) | 16.0 (10.4) | 12.3 (10.8) | 10.9 (9.8) | 9.6 (8.3) | 16.4 (7.8) | 16.3 (8.8) | 21.9 (6.2) | 8.5 (11.2) |
| N | 2,249,597 | 260,647 | 296,187 | 529,893 | 155,558 | 220,850 | 273,826 | 164,316 | 348,320 |
| Month | US | DSW | LMW | NE | PNW | PSW | SE | ST | UMW |
|---|---|---|---|---|---|---|---|---|---|
| Jan | 69.7 (16.0) | 61.8 (17.4) | 71.0 (13.4) | 69.5 (14.0) | 79.8 (13.1) | 57.9 (22.5) | 70.8 (15.2) | 73.5 (12.8) | 75.2 (10.0) |
| Feb | 69.4 (15.3) | 63.6 (18.5) | 71.2 (12.8) | 67.6 (14.0) | 76.6 (12.5) | 61.0 (20.8) | 70.2 (14.1) | 73.9 (12.2) | 74.6 (10.1) |
| Mar | 65.6 (16.8) | 57.7 (19.9) | 67.9 (13.5) | 64.9 (15.9) | 71.8 (14.7) | 55.8 (23.1) | 68.6 (14.3) | 70.1 (11.2) | 69.5 (13.3) |
| Apr | 63.1 (17.3) | 56.8 (20.6) | 64.5 (14.5) | 63.5 (15.9) | 66.3 (16.2) | 51.0 (23.7) | 67.2 (12.9) | 71.4 (9.5) | 64.8 (14.8) |
| May | 66.2 (17.6) | 57.8 (20.6) | 69.0 (13.3) | 71.9 (13.9) | 62.8 (17.2) | 47.2 (24.8) | 72.9 (10.7) | 72.8 (8.7) | 66.3 (13.8) |
| Jun | 67.3 (17.2) | 55.0 (19.7) | 70.5 (10.8) | 74.1 (10.8) | 62.4 (18.0) | 46.9 (25.9) | 73.1 (9.4) | 75.0 (7.0) | 70.4 (11.8) |
| Jul | 68.1 (15.6) | 58.5 (16.1) | 70.6 (10.8) | 73.8 (10.2) | 56.1 (19.7) | 51.8 (21.9) | 75.4 (8.8) | 76.9 (6.7) | 70.3 (10.5) |
| Aug | 69.2 (15.8) | 55.5 (14.2) | 72.1 (10.5) | 76.9 (8.6) | 57.2 (19.7) | 51.9 (21.9) | 76.1 (8.8) | 77.3 (6.4) | 72.4 (11.2) |
| Sep | 70.1 (16.1) | 60.6 (17.8) | 72.1 (11.5) | 77.2 (9.6) | 60.2 (20.0) | 51.7 (21.6) | 75.8 (10.0) | 77.9 (6.9) | 72.3 (12.3) |
| Oct | 69.6 (15.8) | 61.0 (16.9) | 69.2 (13.1) | 75.3 (11.3) | 70.5 (17.1) | 53.3 (22.3) | 73.6 (11.7) | 73.8 (9.5) | 72.4 (12.4) |
| Nov | 68.7 (15.4) | 61.1 (16.8) | 68.8 (12.7) | 69.9 (13.2) | 76.2 (14.8) | 56.3 (22.2) | 71.8 (12.3) | 74.4 (10.1) | 71.7 (11.8) |
| Dec | 74.3 (14.1) | 68.3 (16.1) | 76.6 (11.7) | 73.8 (12.7) | 80.1 (12.7) | 64.6 (20.3) | 76.3 (12.3) | 76.6 (11.1) | 78.1 (9.9) |
| Total | 68.4 (16.3) | 59.8 (18.3) | 70.3 (12.8) | 71.6 (13.4) | 68.3 (18.5) | 54.1 (23.2) | 72.7 (12.2) | 74.5 (9.8) | 71.5 (12.4) |
| N | 2,249,597 | 260,647 | 296,187 | 529,893 | 155,558 | 220,850 | 273,826 | 164,316 | 348,320 |
| Variable Name | Time Lag (Day) | |||||
|---|---|---|---|---|---|---|
| 0 | 1 | 7 | 14 | 21 | 28 | |
| United States (US) | ||||||
| Ambient temperature (°C) | 0.994 *** | 0.993 *** | 0.995 *** | 0.996 *** | 0.996 ** | 0.996 ** |
| (0.991–0.998) | (0.990–0.997) | (0.991–0.998) | (0.992–0.999) | (0.993–0.999) | (0.993–1.000) | |
| Standard deviation of temperature (°C) | 1.012 *** | 1.008 *** | 1.011 *** | 1.005 *** | 1.009 *** | 1.008 *** |
| (1.008–1.017) | (1.004–1.012) | (1.007–1.015) | (1.001–1.009) | (1.005–1.012) | (1.004–1.012) | |
| Relative humidity (%) | 0.999 *** | 0.998 *** | 0.998 *** | 0.999 *** | 0.999 *** | 0.999 *** |
| (0.998–1.000) | (0.997–0.999) | (0.997–0.999) | (0.998–0.999) | (0.998–0.999) | (0.998–0.999) | |
| Temperature X relative humidity | 1.000 *** | 1.000 *** | 1.000 *** | 1.000 *** | 1.000 *** | 1.000 ** |
| (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | |
| Season (0 = Nov to Feb.; 1 otherwise) | 1.079 *** | 1.083 *** | 1.084 *** | 1.086 *** | 1.087 *** | 1.087 *** |
| (1.056–1.102) | (1.061–1.107) | (1.061–1.107) | (1.063–1.109) | (1.064–1.110) | (1.064–1.110) | |
| Observations | 1,059,723 | 1,059,391 | 1,058,304 | 1,057,287 | 1,055,302 | 1,059,006 |
| Desert Southwest (DSW) | ||||||
| Ambient temperature (°C) | 1.003 | 0.999 | 0.999 | 0.989 | 0.981 *** | 0.979 ** |
| (0.993–1.012) | (0.989–1.008) | (0.983–1.014) | (0.972–1.007) | (0.967–0.994) | (0.963–0.995) | |
| Standard deviation of temperature (°C) | 1.026 *** | 1.012 | 1.006 | 0.998 | 1.001 | 0.998 |
| (1.009–1.044) | (0.997–1.026) | (0.993–1.018) | (0.986–1.011) | (0.988–1.013) | (0.985–1.011) | |
| Relative humidity (%) | 1 | 0.998 | 0.995 ** | 0.995 ** | 0.995 *** | 0.995 ** |
| (0.997–1.003) | (0.995–1.001) | (0.991–0.999) | (0.991–0.999) | (0.991–0.998) | (0.991–0.999) | |
| Temperature X relative humidity | 1 | 1 | 1 | 1 | 1.000 *** | 1.000 ** |
| (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.001) | |
| Season (0 = Nov to Feb.; 1 otherwise) | 1.01 | 1.021 | 1.019 | 1.051 | 1.072 * | 1.081 ** |
| (0.940–1.085) | (0.951–1.097) | (0.946–1.097) | (0.975–1.133) | (0.997–1.152) | (1.007–1.161) | |
| Observations | 106,376 | 106,377 | 106,383 | 106,267 | 106,216 | 106,383 |
| Lower Midwest (LMW) | ||||||
| Ambient temperature (°C) | 0.987 ** | 0.983 *** | 0.983 *** | 0.979 *** | 0.981 *** | 0.982 *** |
| (0.976–0.997) | (0.972–0.994) | (0.971–0.994) | (0.967–0.992) | (0.970–0.992) | (0.973–0.991) | |
| Standard deviation of temperature (°C) | 1.025 *** | 1.020 *** | 1.026 *** | 1.014 ** | 1.025 *** | 1.026 *** |
| (1.012–1.038) | (1.007–1.034) | (1.015–1.038) | (1.002–1.026) | (1.013–1.036) | (1.015–1.038) | |
| Relative humidity (%) | 0.997 *** | 0.996 *** | 0.995 *** | 0.996 *** | 0.996 *** | 0.996 *** |
| (0.994–0.999) | (0.993–0.998) | (0.993–0.998) | (0.994–0.999) | (0.993–0.998) | (0.994–0.998) | |
| Temperature X relative humidity | 1.000 *** | 1.000 *** | 1.000 *** | 1.000 *** | 1.000 *** | 1.000 *** |
| (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | |
| Season (0 = Nov to Feb.; 1 otherwise) | 1.101 *** | 1.114 *** | 1.115 *** | 1.131 *** | 1.121 *** | 1.137 *** |
| (1.038–1.168) | (1.050–1.181) | (1.051–1.182) | (1.067–1.199) | (1.060–1.185) | (1.073–1.204) | |
| Observations | 108,199 | 108,199 | 108,173 | 108,196 | 108,191 | 108,172 |
| Northeast (NE) | ||||||
| Ambient temperature (°C) | 0.986 *** | 0.989 ** | 0.996 | 0.994 ** | 0.997 | 0.997 |
| (0.977–0.994) | (0.980–0.998) | (0.991–1.001) | (0.988–1.000) | (0.991–1.003) | (0.991–1.004) | |
| Standard deviation of temperature (°C) | 1.014 *** | 1.008 * | 1.014 *** | 1.009 ** | 1.017 *** | 1.014 *** |
| (1.005–1.024) | (0.999–1.017) | (1.006–1.023) | (1.000–1.018) | (1.009–1.026) | (1.005–1.023) | |
| Relative humidity (%) | 0.998 *** | 0.998 ** | 0.999 * | 0.998 ** | 0.999 * | 0.998 *** |
| (0.996–0.999) | (0.997–1.000) | (0.997–1.000) | (0.997–1.000) | (0.997–1.000) | (0.996–0.999) | |
| Temperature X relative humidity | 1.000 *** | 1.000 ** | 1 | 1.000 ** | 1 | 1 |
| (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | |
| Season (0 = Nov to Feb.; 1 otherwise) | 1.125 *** | 1.131 *** | 1.122 *** | 1.119 *** | 1.114 *** | 1.107 *** |
| (1.079–1.174) | (1.085–1.180) | (1.075–1.171) | (1.072–1.169) | (1.068–1.163) | (1.061–1.155) | |
| Observations | 239,452 | 239,111 | 239,376 | 239,482 | 239,495 | 239,494 |
| Pacific Northwest (PNW) | ||||||
| Ambient temperature (°C) | 1 | 0.999 | 1.004 | 0.999 | 1 | 0.991 |
| (0.986–1.014) | (0.987–1.011) | (0.992–1.016) | (0.983–1.014) | (0.984–1.016) | (0.976–1.007) | |
| Standard deviation of temperature (°C) | 0.999 | 1.004 | 0.992 | 0.99 | 0.989* | 0.997 |
| (0.981–1.018) | (0.988–1.020) | (0.980–1.005) | (0.977–1.003) | (0.976–1.002) | (0.984–1.010) | |
| Relative humidity (%) | 1 | 1 | 1.001 | 0.998 | 1 | 0.999 |
| (0.997–1.003) | (0.998–1.003) | (0.999–1.004) | (0.995–1.001) | (0.997–1.003) | (0.996–1.002) | |
| Temperature X relative humidity | 1 | 1 | 1 | 1 | 1 | 1 |
| (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | |
| Season (0 = Nov to Feb.; 1 otherwise) | 1.048 | 1.043 | 1.03 | 1.051 | 1.066 | 1.055 |
| (0.960–1.143) | (0.956–1.137) | (0.944–1.123) | (0.967–1.142) | (0.975–1.165) | (0.966–1.152) | |
| Observations | 88,886 | 88,886 | 88,874 | 88,886 | 88,885 | 88,451 |
| Pacific Southwest (PSW) | ||||||
| Ambient temperature (°C) | 0.995 | 0.992 ** | 0.994 * | 0.999 | 0.990 ** | 0.999 |
| (0.986–1.004) | (0.984–1.000) | (0.988–1.000) | (0.991–1.007) | (0.981–1.000) | (0.987–1.011) | |
| Standard deviation of temperature (°C) | 1.015 * | 1.015 * | 1.013 * | 1.002 | 1.006 | 0.999 |
| (0.999–1.031) | (0.999–1.031) | (0.999–1.027) | (0.988–1.016) | (0.992–1.020) | (0.985–1.013) | |
| Relative humidity (%) | 0.999 | 0.997 * | 0.998 | 0.999 | 0.996 ** | 0.998 |
| (0.996–1.002) | (0.995–1.000) | (0.996–1.001) | (0.997–1.002) | (0.993–0.999) | (0.995–1.002) | |
| Temperature X relative humidity | 1 | 1.000 *** | 1.000 * | 1 | 1 | 1 |
| (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | |
| Season (0 = Nov to Feb.; 1 otherwise) | 1.096 *** | 1.088 ** | 1.102 *** | 1.096 *** | 1.122 *** | 1.113 *** |
| (1.024–1.173) | (1.018–1.163) | (1.031–1.179) | (1.023–1.175) | (1.047–1.203) | (1.038–1.194) | |
| Observations | 105,012 | 105,029 | 103,864 | 105,061 | 105,061 | 104,490 |
| Southeast (SE) | ||||||
| Ambient temperature (°C) | 0.973 *** | 0.982 *** | 0.994 | 1.001 | 0.998 | 1 |
| (0.959–0.987) | (0.969–0.995) | (0.984–1.004) | (0.993–1.008) | (0.990–1.005) | (0.992–1.007) | |
| Standard deviation of temperature (°C) | 1.012 * | 1.002 | 1.004 | 1.007 | 1.005 | 1.009 |
| (0.998–1.026) | (0.989–1.015) | (0.992–1.017) | (0.994–1.019) | (0.993–1.017) | (0.997–1.021) | |
| Relative humidity (%) | 0.994 *** | 0.995 *** | 0.997 ** | 1 | 0.999 | 1 |
| (0.990–0.997) | (0.991–0.998) | (0.994–1.000) | (0.997–1.002) | (0.997–1.001) | (0.997–1.002) | |
| Temperature X relative humidity | 1.000 *** | 1.000 *** | 1.000 ** | 1 | 1 | 1 |
| (1.000–1.001) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | |
| Season (0 = Nov to Feb.; 1 otherwise) | 1.034 | 1.036 | 1.015 | 1.017 | 1.025 | 1.031 |
| (0.970–1.103) | (0.972–1.104) | (0.953–1.081) | (0.953–1.086) | (0.963–1.090) | (0.969–1.096) | |
| Observations | 113,682 | 113,709 | 113,705 | 111,316 | 113,704 | 113,736 |
| Subtropical (ST) | ||||||
| Ambient temperature (°C) | 1.017 | 1.008 | 1.001 | 0.99 | 1.012 | 1.002 |
| (0.988–1.047) | (0.983–1.034) | (0.980–1.022) | (0.970–1.010) | (0.996–1.028) | (0.986–1.019) | |
| Standard deviation of temperature (°C) | 1 | 0.996 | 1.008 | 1.008 | 1.008 | 1.015 |
| (0.981–1.019) | (0.979–1.013) | (0.992–1.025) | (0.991–1.026) | (0.989–1.027) | (0.996–1.034) | |
| Relative humidity (%) | 1.005 | 1.003 | 1.002 | 0.999 | 1.004 * | 1.002 |
| (0.996–1.013) | (0.996–1.010) | (0.996–1.007) | (0.994–1.004) | (0.999–1.009) | (0.998–1.005) | |
| Temperature X relative humidity | 1 | 1 | 1 | 1 | 1 | 1 |
| (0.999–1.000) | (0.999–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | |
| Season (0 = Nov to Feb.; 1 otherwise) | 1.044 | 1.044 | 1.049 | 1.036 | 1.037 | 1.041 |
| (0.958–1.137) | (0.961–1.135) | (0.970–1.134) | (0.959–1.120) | (0.964–1.116) | (0.965–1.122) | |
| Observations | 110,254 | 110,233 | 110,075 | 110,244 | 110,248 | 110,232 |
| Upper Midwest (UMW) | ||||||
| Ambient temperature (°C) | 0.988 ** | 0.985 ** | 0.985 ** | 0.993 | 1 | 1.006 |
| (0.976–1.000) | (0.973–0.997) | (0.972–0.998) | (0.981–1.005) | (0.989–1.012) | (0.995–1.017) | |
| Standard deviation of temperature (°C) | 1.017 *** | 1.013 ** | 1.023 *** | 1.011 * | 1.018 *** | 1.012 ** |
| (1.004–1.029) | (1.000–1.025) | (1.011–1.035) | (1.000–1.023) | (1.006–1.030) | (1.001–1.024) | |
| Relative humidity (%) | 0.997 ** | 0.997 ** | 0.997 ** | 0.998 | 0.999 | 0.999 |
| (0.995–1.000) | (0.994–0.999) | (0.995–1.000) | (0.996–1.001) | (0.997–1.001) | (0.997–1.001) | |
| Temperature X relative humidity | 1.000 ** | 1.000 ** | 1.000 ** | 1 | 1 | 1 |
| (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | (1.000–1.000) | |
| Season (0 = Nov to Feb.; 1 otherwise) | 1.083 ** | 1.098 *** | 1.095 *** | 1.094 *** | 1.076 ** | 1.089 *** |
| (1.019–1.152) | (1.033–1.167) | (1.030–1.163) | (1.031–1.162) | (1.012–1.144) | (1.025–1.156) | |
| Observations | 187,862 | 187,847 | 187,854 | 187,835 | 183,502 | 188,048 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chacko, G.; Patel, S.; Galor, A.; Kumar, N. Heat Exposure and Multiple Sclerosis—A Regional and Temporal Analysis. Int. J. Environ. Res. Public Health 2021, 18, 5962. https://doi.org/10.3390/ijerph18115962
Chacko G, Patel S, Galor A, Kumar N. Heat Exposure and Multiple Sclerosis—A Regional and Temporal Analysis. International Journal of Environmental Research and Public Health. 2021; 18(11):5962. https://doi.org/10.3390/ijerph18115962
Chicago/Turabian StyleChacko, Gill, Sneh Patel, Anat Galor, and Naresh Kumar. 2021. "Heat Exposure and Multiple Sclerosis—A Regional and Temporal Analysis" International Journal of Environmental Research and Public Health 18, no. 11: 5962. https://doi.org/10.3390/ijerph18115962
APA StyleChacko, G., Patel, S., Galor, A., & Kumar, N. (2021). Heat Exposure and Multiple Sclerosis—A Regional and Temporal Analysis. International Journal of Environmental Research and Public Health, 18(11), 5962. https://doi.org/10.3390/ijerph18115962