
Multiple Gestations and Assisted Reproductive Technologies: Qualitative Study of the Discourse of Health Professionals in Spain

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Data Collection
- Current trend of multiple gestations (embryo transfer policies).
- Impact and consequences on the family, society, and the health system.
- Monitoring of multiple gestations.
- Demands on health administration (emerging category).
2.4. Data Analysis
- Opinion on multiple gestations.
- Attribution of multiple gestations.
- Approach to embryo transfer policies.
- Circumstances, motivations, or needs to undergo an ART. Impact of ART on the couple, at the work and social level.
- Motivations for the delay of maternity
- Impact of multiple gestation.
- Follow-up of pregnant women from primary care.
- Emotional monitoring for women and couples undergoing ART.
- Negative situation in emotional follow-up.
- Follow-up in the postpartum.
- Maternal mental health during follow-up.
- Treatment of health administration of multiple gestations.
- Role of the professionals of the administration in the treatment.
- Suggestions.
2.5. Ethical Considerations
3. Results
3.1. Current Trend of Multiple Gestations (Embryo Transfer Policies)
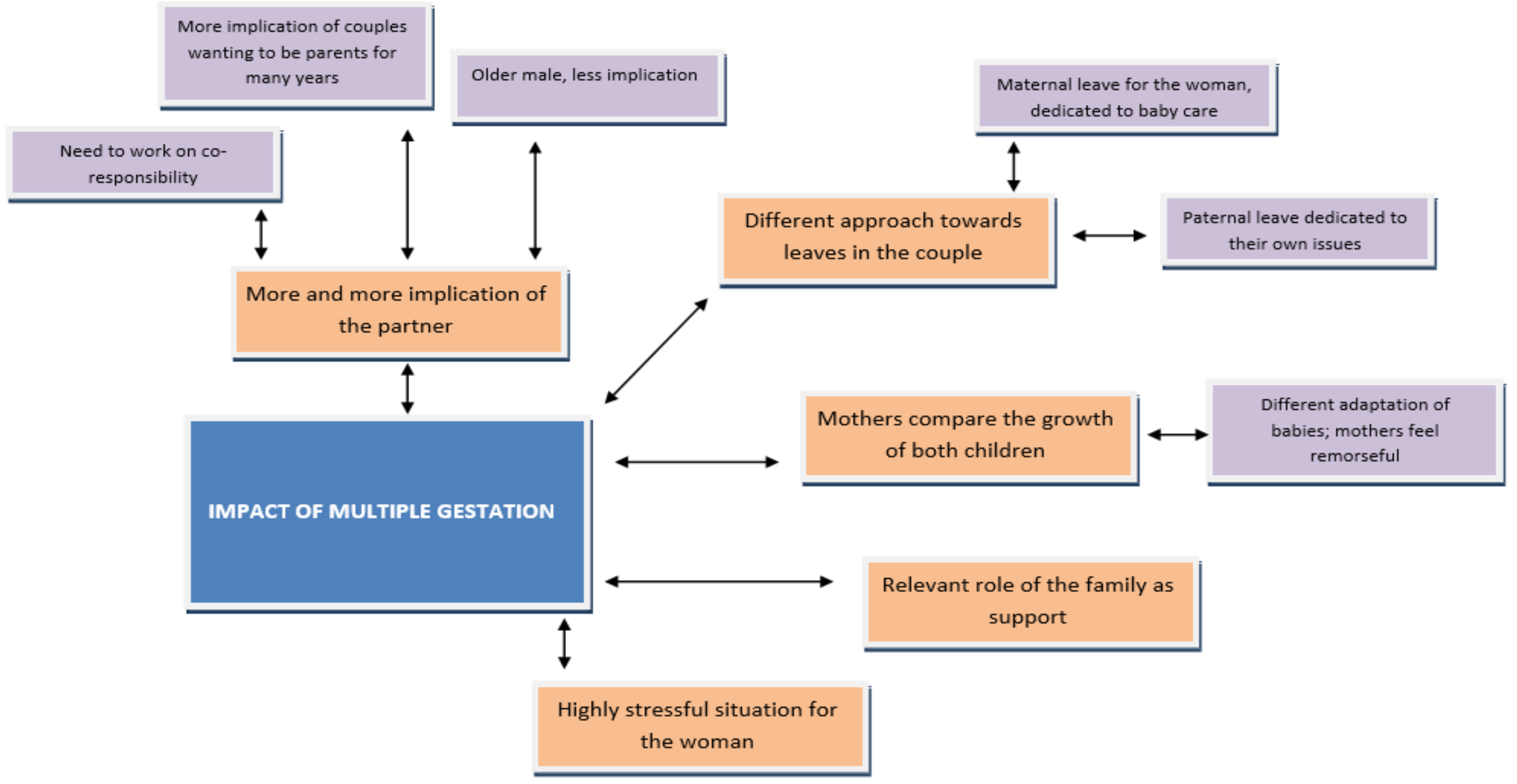
3.2. Impact of Multiple Gestation on Women, Partners, Society, and the Health System
3.3. Follow-Up
3.4. Demands to the Health Administration
3.5. Suggestions
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- González-Mesa, E.; Cazorla, O.; González-Valenzuela, M.J. The epidemic of twins: The challenge in obstetrics and gynecology. EMJ Reprod. Health 2015, 1, 101–105. [Google Scholar]
- Heino, A.; Gissler, M.; Hindori-Mohangoo, A.D.; Blondel, B.; Klungsøyr, K.; Verdenik, I.; Mierzejewska, E.; Velebil, P.; Sól Ólafsdóttir, H.; Macfarlane, A.; et al. Variations in Multiple Birth Rates and Impact on Perinatal Outcomes in Europe. PLoS ONE 2016, 11, e0149252. [Google Scholar] [CrossRef]
- Di Paola, R.; Garzon, S.; Giuliani, S.; Laganà, A.S.; Noventa, M.; Parissone, F.; Zorzi, C.; Raffaelli, R.; Ghezzi, F.; Franchi, M.; et al. Are we choosing the correct FSH starting dose during controlled ovarian stimulation for intrauterine insemination cycles? Potential application of a nomogram based on woman’s age and markers of ovarian reserve. Arch. Gynecol. Obstet. 2018, 298, 1024–1035. [Google Scholar] [CrossRef] [PubMed]
- Papler, T.B.; Bokal, E.V.; Zmrzljak, U.P.; Stimpfel, M.; Laganà, A.S.; Ghezzi, F.; Jančar, N. PGR and PTX3 gene expression in cumulus cells from obese and normal weighting women after administration of long-acting recombinant follicle-stimulating hormone for controlled ovarian stimulation. Arch. Gynecol. Obstet. 2019, 299, 863–871. [Google Scholar] [CrossRef] [PubMed]
- Alemany-Lasheras, F.; Amezcua-Martínez, M.; Aparcero-Bernet, L.; Arroyo-Rodríguez, A.; Calvo-Cabrera, I.; Lancharro-Tavero, I. Memoria de la asignatura Trabajo Fin de Grado. Centro Universitario de Enfermería “San Juan de Dios”. Universidad de Sevilla. Bibl. Las Casas 2015, 11, 1–29. [Google Scholar]
- Goncé, A.; Boguña, J.; Marimon, E.; Muñoz, M.; Palacio, M.; Martínez, J. Protocolo Asistencia al Embarazo y Parto de Gestaciones Múltiples; Hospital Clinic, Hospital St Joan Déu: Barcelona, Spain, 2015. [Google Scholar]
- Committee on Practice Bulletins—Obstetrics; Society for Maternal–Fetal Medicine. Practice Bulletin No. 169: Multifetal Gestations: Twin, Triplet, and Higher-Order Multifetal Pregnancies. Obs. Gynecol. 2016, 128, 131–146. [Google Scholar] [CrossRef] [PubMed]
- Qazi, G. Obstetric and perinatal outcome of multiple pregnancy. J. Coll Physicians Surg. Pak. 2011, 21, 142–145. [Google Scholar] [PubMed]
- Qin, J.; Wang, H.; Sheng, X.; Xie, Q.; Gao, S. Assisted reproductive technology and risk of adverse obstetric outcomes in dichorionic twin pregnancies: A systematic review and meta-analysis. Fertil. Steril. 2016, 105, 1180–1192. [Google Scholar] [CrossRef] [Green Version]
- Bladilo, A.; Torre, N.; Herrera, M. Las técnicas de reproducción humana asistida desde los derechos humanos como perspectiva obligada de análisis. IUS 2017, 11. [Google Scholar] [CrossRef]
- Benute, G.; Nozzela, D.; Prohaska, C.; Liao, A.; De-Lucia, M.; Zugaib, M. Twin pregnancies: Evaluation of major depression, stress and social support. Twin Res. Hum. Genet. 2013, 16, 629–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chambers, G.M.; Lee, E.; Hansen, M.; Sullivan, E.A.; Bower, C.; Chapman, M. Hospital costs of multiple-birth and singleton-birth children during the first 5 years of life and the role of assisted reproductive technology. JAMA Pediatr. 2014, 168, 1045–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palacios-Ceña, D.; Corral-Liria, I. The basics and development of a phenomenological research protocol in nursing. EnfermeríaIntensiva 2010, 21, 68–73. [Google Scholar]
- Chien, P. Multiple pregnancy and assisted conception treatment. BJOG An Int. J. Obstet. Gynaecol. 2020, 127, 525–526. [Google Scholar] [CrossRef]
- Rivas, A.; Álvarez, C.; Jociles, M. La intervención de ‘terceros’ en la producción de parentesco: Perspectiva de los/as donantes, las familias y la descendencia. Un estado de la cuestión. Rev. Antropol. Soc. 2018, 27, 221–245. [Google Scholar] [CrossRef]
- Jacklin, P.; Marceniuk, G. A Report by the National Guideline Alliance about Twin Pregnancy Costing Commissioned by: The Human Fertilisation and Embryology Authority, the British Fertility Society, the Multiple Births Foundation and Fertility Network UK. 2018. Available online: https://www.hfea.gov.uk/media/2650/nga-twin-pregnancy-costing-final.pdf (accessed on 18 April 2021).
- McLernon, D.J.; Harrild, K.; Bergh, C.; Davies, M.J.; De Neubourg, D.; Dumoulin, J.C.M.; Gerris, J.; Kremer, J.A.; Martikainen, H.; Mol, B.W.; et al. Clinical effectiveness of elective single versus double embryo transfer: Meta-analysis of individual patient data from randomised trials. BMJ 2011, 342, 34. [Google Scholar] [CrossRef] [Green Version]
- Tobias, T.; Sharara, F.; Franasiak, J.; Heiser, P.; Pinckney-Clark, E. Promoting the use of elective single embryo transfer in clinical practice. Fertil. Res. Pract. 2016, 2, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ley 14/2006 de 26 de mayo sobre técnicas de reproducción asistida. Boletín Oficial del Estado (BOE) 2006, 126, 1–21. Available online: https://www.boe.es/eli/es/l/2006/05/26/14/con (accessed on 6 May 2021).
- Comisión Nacional de Reproducción Humana Asistida. Informe Estadístico de Técnicas de ReproduccionAsisitda; Ministerio de Sanidad: Madrid, Spain, 2017.
- Ezugwu, E.; der-Burg, S. Debating elective single embryo transfer after in vitro fertilization: A plea for a context sensitive approach. Ann. Med. Health Sci. Res. 2015, 5, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adashi, E.; Gleicher, N. Is a blanket elective single embryo transfer policy defensible? Rambam Maimonides Med. J. 2017, 8, e0022. [Google Scholar] [CrossRef] [Green Version]
- Junta de Andalucía. Reproducción Humana Asistida en el Sistema Sanitario Público de Andalucía; Servicio Andaluz de Salud, Consejería de Salud y Familias: Sevilla, Spain, 2020. [Google Scholar]
- Instituto Nacional de Estadística. INE. Indicadores de Fecundidad. Registrosnacionales. 2019. Available online: https://www.ine.es/jaxiT3/Tabla.htm?t=1579 (accessed on 18 April 2021).
- Román, E.; Coca, A.; García, E. Maternidad y conciliación laboral: ¿mito o realidad? Enfermería Docente 2017, 58, 58–86. [Google Scholar]
- Kawwass, J.; Badell, M. Maternal and fetal risk associated with assisted reproductive technology. Obstet. Gynecol. 2018, 132, 763–772. [Google Scholar] [CrossRef]
- Toneut, C.M.; García, M.E.G.; Vega, A.M.; Fernández, R.B.; Arechavaleta, N.M.; Arechavaleta, A.M. Maternal and perinatal outcomes in pregnant women with advanced maternal age. Rev. Cuba. Obstet. y Ginecol. 2017, 43, 1–14. [Google Scholar]
- Santana, D.S.; Silveira, C.; Costa, M.L.; Souza, R.T.; Surita, F.G.; Souza, J.P.; Mazhar, S.B.; Jayaratne, K.; Qureshi, Z.; Sousa, M.H.; et al. Perinatal outcomes in twin pregnancies complicated by maternal morbidity: Evidence from the WHO Multicountry Survey on Maternal and Newborn Health. BMC Pregnancy Childbirth. 2018, 18, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Reitter, A.; Daviss, B.A.; Krimphove, M.J.; Johnson, K.C.; Schlößer, R.; Louwen, F.; Bisits, A. Mode of birth in twins: Data and reflections. J. Obstet. Gynaecol. 2018, 38, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Ellwood, D. Caesarean secion births for twins: Rational choice, or a non-evidence-based intervention that may cause harm? Med. J. Aust. 2020, 212, 70–71. [Google Scholar] [CrossRef] [PubMed]
- Díez, M.; Morgado, B.; González, M. El apoyo social y la satisfacción vital, factores clave en el caso de las madres adptivas solas. Apuntes Psicol. 2017, 34, 139–149. [Google Scholar]
- Van den Akker, O.; Postavaru, G.; Purewal, S. Maternal psychosocial consequences of twins and multiple births following assisted and natural conception: A meta-analysis. Reprod. Biomed. Online 2016, 33, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wenze, S.; Battle, C.; Tezanos, K. Raising multiples: Mental health of mothers and fathers in early parenthood. Arch. Women’s Ment Health 2015, 18, 163–176. [Google Scholar] [CrossRef] [Green Version]
- Lemos, E.; Zhang, D.; Van Voorhis, B.; Hu, X. Healthcare expenses associated with multiple vs singleton pregnancies in the United States. Am. J. Obstet. Gynecol. 2013, 209, 586.e1–586.e11. [Google Scholar] [CrossRef] [PubMed]
- National Collaborating Centre for Women’s and Children’s Health. Commissioned by the National Institute for Health and Clinical Excellence. Multiple Pregnancy: The Management of Twin and Triplet Pregnancies in the Antenatal Period. 2011. Available online: https://www.nice.org.uk/guidance/ng137/evidence/september-2011-full-guideline-pdf-6901736510 (accessed on 18 April 2021).
- National Institute for Health and Care Excellence. NICE Guideline. Twin and Triplet Pregnancy. 2019. Available online: www.nice.org.uk/guidance/ng137 (accessed on 29 May 2021).
- SEGO (Sociedad Española de Ginecología y Obstetricia). Guía de asistencia práctica. Dichorionic twin pregnancy. Prog. Obstet. Ginecol. 2016, 59, 43–57.
- Carrick-Sen, D.; Steen, N.; Robson, S. Twin parenthood: The midwife’s role—A randomised controlled trial. BJOG 2014, 121, 1302–1310. [Google Scholar] [CrossRef] [Green Version]
- Ponce, J.; Bennasar, M.; Muñoz, M.; Palacio, M.; Crovetto, F.; Boguña, J. Protocolo Asistencia al Embarazo y Parto de Gestaciones Múltiples; Report No.: MMF2548; Hospital Clinic and Hospital Sant Joan de Déu: Barcelona, Spain, 2021. [Google Scholar]
- Griffith, R. Records: What to include. Br. J. Midwifery 2016, 24, 743–744. [Google Scholar] [CrossRef]
- Kerkin, B.; Lennox, S.; Patterson, J. Making midwifery work visible: The multiple purposes of documentation. Women Birth 2018, 31, 232–239. [Google Scholar] [CrossRef] [PubMed]
- De España, G. Ley Orgánica 3/2007 de 22 de marzo para la igualdad efectiva de hombres y mujeres. Boletín Oficial del Estado (BOE) 2007, 71, 12611–12645. [Google Scholar]
- Maroto-Navarro, G.; Castaño-López, E.; García-Calvente, M.; Hidalgo-Ruzzante, N.; Mateo-Rodríguez, I. Paternity and HealthServices. Qualitative Research on Men’s experiences during Pregnancy, Delivery and Postpartum of theirs Partners. Rev. Española de SaludPública 2009, 4, 263–274. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Professionals | Time of Service | Sex | Occupation | Age (years) | Place of Work |
|---|---|---|---|---|---|
| P 1 | 15 years | Female | Midwife | 58 | PC |
| P 2 | 30 years | Male | Midwife | 55 | PC |
| P 3 | 20 years | Female | Midwife | 62 | PC |
| P 4 | 30 years | Female | Midwife | 57 | PC |
| P 5 | 12 years | Male | Gynaecologist | 62 | Public ART Unit |
| P 6 | 7 years | Female | Gynaecologist | 47 | Public ART Unit |
| P 7 | 3 years | Female | Gynaecologist | 32 | Private ART Unit |
| P 8 | 24 years | Male | Gynaecologist | 53 | Private ART Unit |
| Current Trend for Multiple Gestations (Embryo Transfer Policies) |
|---|
| “Of course. The big increase has come since assisted reproductive…” (p2). “Transferring three embryos is a bad practice, by all standards, even twin pregnancies are in question. But of course, as by law, it’s not illegal… That is, there are people who do it and are protected by law, and even there are some… a unique embryo transfer policy is being made in many…” (p6). “It’s an individual ethical-personal issue, so I think the first thing is primary prevention, not transferring more than two embryos. In fact, the increasing trend is to transfer one” (p7). “The law in Spain… only three was authorised and this did a lot to correct multiple pregnancies and, currently, the goal is to reduce even the gestation of two” (p8). “Here is a very clear economic approach, everything achieved by that perverse incentive, which is that if I have two children at once, all the better, I have my family and once for in a year or two, I have already solved the problem and I return to my work and personal life” (p8). “But you understand that, for many women that age, they cannot stop working three times to have three children, with the maternal leaves this implies and everything it entails. Unfortunately, there is still a lot of machismo and micro-machismo, so many women in their jobs will not tolerate two pregnancies or three” (p6). “I also believe that if motherhood were better cared for with regard to maternity leave… But if there is no reconciliation, you reach 42 years old and you want to have everything arranged, for the nursery and all these things, you have no choice but to leave at 40–42 years. But if you have more facilities such as governments to help you, more reconciliation so that the father can access a good paternal leave… because perhaps you raise it younger because, well, the government helps me in this period, and my husband is also there” (p7). |
| Impact of Multiple Gestations on Women, Couples, Society, and the Health System |
|---|
| “To the woman, very emotionally, the whole issue of morbidity, postpartum depressions, any kind of psychiatric morbidity, everything is going to shoot up” (p1). “All kinds of couple crises can be seen in matters of reproduction and infertility, because it is a kind of vital crisis that can sometimes be very disturbing” (p8). “It’s not only physiological stress, it is also a psychic and economic stress. So, this strains the couple” (p8). “When they are premature… you have to spend 3 or 4 weeks at hospital… and that marks women a lot, huh, that… they end up shattered, because they are coming and going all the time…” (p2). “They get exhausted and see that all the emotional resources are allocated to the children, they are the only ones who have the focus on them and they somehow recover “a life of man” (p8). “Of course, prematurity has this problem of these children, their early neonatal but also long-term intellectual performance” (p8). “In fact, there is a psychologist at the clinic who recently emailed us that all women undergoing treatment should do therapy” (p7). “But, come on, males put up with it worse. And it is true that we live in a very sexist society, very sexist, it is still very sexist and… and women… I increasingly admire women for their ability to hold on” (p6). |
| Follow-Up of Multiple Gestations |
|---|
| “You have to further control: these women… you have to follow up much more. So, it’s pregnancies that you have to control them more…” (p1). “When I see that it’s a twin pregnancy, I like to do the home visit, see the conditions these kids are going to be in” (p2). “Protocols tell the same old thing, but then you have to have your internal protocol that we all have that is given by experience” (p3). “I do. Normally, you’re required a post-night visit by the administration. If I, to a normal woman with one child, I don’t have enough because I give her an appointment her and then I do it again to remove the stitches, then I give these women five appointments because with the tits they need more care” (p4). “And me, for instance, in twin pregnancies, streptococcus [¿?] I perform it a bit earlier, on my own account. This is not protocolised, but I know this woman needs it (p2)”. “Then I start preparing these women separately, a little earlier; in the remaining pregnant women, I start at week 27; in those, I start at week 24 or 23, so… just in case” (p2). “They need the midwife more than the… that norm… patients with a single pregnancy” (p6). |
| Demands to the Health Administration |
|---|
| “More midwives must be demanded considering the women” (p3). “I think with the twins there should be more visits because, besides, many are C-sections, and coming with the two children is more complicated. What’s more, the visits I make are for twins or if there has been some complication in the postpartum” (p4). “To contemplate that, if it is a twin pregnancy, the ten days should not count because since the children are admitted, that woman does not come until twenty days later, and now you see her at 20 days and the visit does not count. So, this is very hard, but in public health it’s a disaster” (p4). “Yes, yes, they consider it to be… a slightly absurd specialty,… should be more recognised and that goes through the economic issue, above all” (p6). “And in the end, they choose to go to a private clinic to speed things up, because in the public system, waiting times are often unsustainable, then more investment to speed up times” (p7). “Like public medicine, I believe that… that does not live up to the circumstances, most of the… couples have to resort to the private ones that take less time, and couples are taken care of more psychologically” (p5). |
| Suggestions |
|---|
| “To raise patients’ awareness of the risks of a multiple pregnancy for both her and the foetuses. And I think that’s everybody’s job.” (p7). “Also, as primary prevention is to raise awareness of the age of the first pregnancy. To know that from the age of 35 fertility is reduced exponentially and that from the age of 38, it is much more reduced” (p7). “Then, we should find a positive incentive for these women to take on gestations one at a time” (p8). “No. Not at all. No. Someone who, at any given time, the moment comes… and have free time and say “Well, I’m going to get ready…”, and do a programme and mess with the psychologists, and mess with the midwives, and with the gynaecologists, and does a programme, and make a booklet and a brochure and a downloadable PDF and… whatever you want…” (p1). “The thing would be to have a specific unit of… of… psychology of… to support these couples, that would be clear, that would be great” (p5). “The social and economic aspect is where we should find an economic support network for couples, for the financing of procedures and cycles, which would reduce the stress of having multiple pregnancies, and this would be the most efficient way to reduce the number of embryos and multiple gestations” (p8). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurado-García, E.; Botello-Hermosa, A.; Fernández-Carrasco, F.J.; Gómez-Salgado, J.; Navas-Rojano, N.; Casado-Mejía, R. Multiple Gestations and Assisted Reproductive Technologies: Qualitative Study of the Discourse of Health Professionals in Spain. Int. J. Environ. Res. Public Health 2021, 18, 6031. https://doi.org/10.3390/ijerph18116031
Jurado-García E, Botello-Hermosa A, Fernández-Carrasco FJ, Gómez-Salgado J, Navas-Rojano N, Casado-Mejía R. Multiple Gestations and Assisted Reproductive Technologies: Qualitative Study of the Discourse of Health Professionals in Spain. International Journal of Environmental Research and Public Health. 2021; 18(11):6031. https://doi.org/10.3390/ijerph18116031
Chicago/Turabian StyleJurado-García, Estefanía, Alicia Botello-Hermosa, Francisco Javier Fernández-Carrasco, Juan Gómez-Salgado, Nazaret Navas-Rojano, and Rosa Casado-Mejía. 2021. "Multiple Gestations and Assisted Reproductive Technologies: Qualitative Study of the Discourse of Health Professionals in Spain" International Journal of Environmental Research and Public Health 18, no. 11: 6031. https://doi.org/10.3390/ijerph18116031
APA StyleJurado-García, E., Botello-Hermosa, A., Fernández-Carrasco, F. J., Gómez-Salgado, J., Navas-Rojano, N., & Casado-Mejía, R. (2021). Multiple Gestations and Assisted Reproductive Technologies: Qualitative Study of the Discourse of Health Professionals in Spain. International Journal of Environmental Research and Public Health, 18(11), 6031. https://doi.org/10.3390/ijerph18116031