
The Impact of COVID-19 on Admissions and Management of Patients with Atrial Fibrillation Episodes in the Emergency Department

 ,
,  , , ,
, , ,  , and
, and 
Abstract
:1. Background
2. Methods
2.1. COVID-19 Dynamics and Medical Care Structure during Pandemic
2.2. Statistical Analysis
- patient age (years) dichotomized as ≥65 years or <65 years;
- duration since AF episode onset trichotomized as up to 6 h, 7–43 h, or longer than 43 h (or unknown, as appropriate);
- sex.
3. Results
3.1. Studied Population
3.2. Demographic Data
3.2.1. The time since the AF onset to the ED admission
3.2.2. Restoration of sinus rhythm
3.3.3. Previous and current SARS-CoV-2 infection
3.3.4. The sinus rhythm restoration
3.3.5. Multivariate analysis of AF restoration
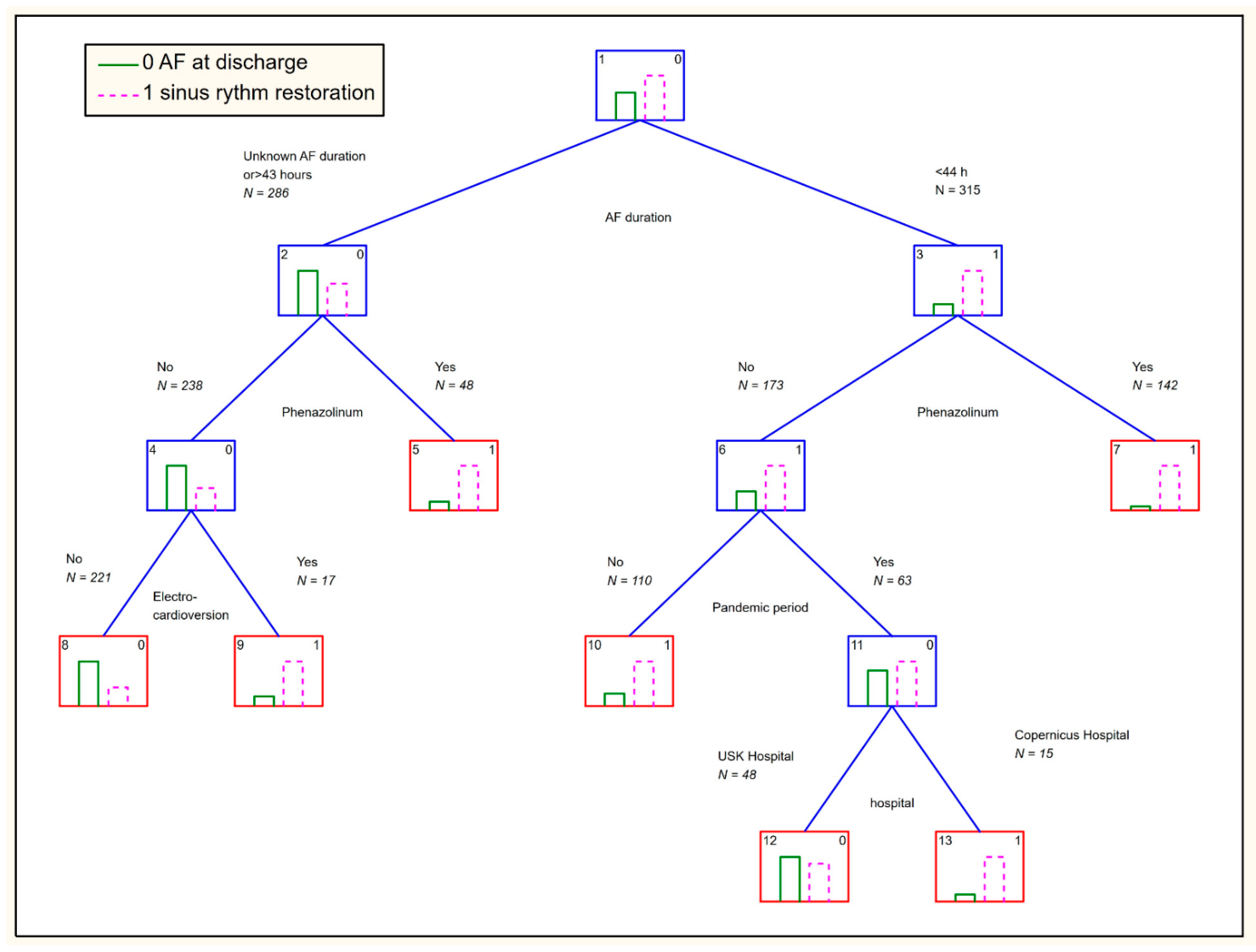
3.3.6. CART Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 19 May 2021).
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A Pneumonia Outbreak Associated with a New Coronavirus of Probable Bat Origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhee, C.; Baker, M.; Vaidya, V.; Tucker, R.; Resnick, A.; Morris, C.A.; Klompas, M. CDC Prevention Epicenters Program. JAMA Netw. Open 2020, 3, e2020498. [Google Scholar]
- Chourasia, G.; Sycz, W.K.; Wolniakowski, I.; Dudek, K.; Porębska, B.; Moczarska, J.; Budrewicz, K.; Wizowska, J.; Nadolny, K.; Soko-łowski, J.; et al. Changes in the Visits to Emergency Department of Non-Infectious Hospital during the Early COVID-19 State of Epidemic Emerg. Med. Serv. 2020, 7, 99–102. [Google Scholar] [CrossRef]
- Russo, V.; Navarin, S.; Zampini, G.; Magrini, L.; Mann, C.; Muiesan, M.L.; De Caterina, R.; Yılmaz, M.B.; Beton, O.; Monzani, V.; et al. Management of Atrial Fibrillation in the Emergency Department: Current Approach and Future Expectations. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 3132–3147. [Google Scholar] [PubMed]
- Gulizia, M.M.; Cemin, R.; Colivicchi, F.; De Luca, L.; Di Lenarda, A.; Boriani, G.; Di Pasquale, G.; Nardi, F.; Scherillo, M.; Lucci, D.; et al. BLITZ-AF Investigators. Europace 2021, 21, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Pardo Sanz, A.; Salido Tahoces, L.; Ortega Pérez, R.; González Ferrer, E.; Sánchez Recalde, Á.; Zamorano Gómez, J.L. New-Onset Atrial Fibrillation during COVID-19 Infection Predicts Poor Prognosis. Cardiol. J. 2021, 28, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Schnaubelt, S.; Domanovits, H.; Niederdoeckl, J.; Schuetz, N.; Cacioppo, F.; Oppenauer, J.; Spiel, A.O.; Laggner, A.N. The Impact of the COVID-19 Pandemic on Incidences of Atrial Fibrillation and Electrical Cardioversion at a Tertiary Care Emergency Depart-Ment: An Inter- and Intra-Year Analysis. Front. Med. 2020, 12, 595881. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.-F.; Cheng, W.-H.; Hung, Y.; Lin, W.-Y.; Chao, T.-F.; Liao, J.-N.; Lin, Y.-J.; Lin, W.-S.; Chen, Y.-J.; Chen, S.-A. Management of Atrial Fibrillation in COVID-19 Pandemic. Circ. J. 2020, 84, 1679–1685. [Google Scholar] [CrossRef]
- Budrewicz, K.; Dudek, K.; Porębska, B.; Wolniakowski, I.; Nadolny, K.; Zyśko, D. Short-Term Prognosis in Patients Visiting Emer-Gency Departments. Na Ratunek 2019, 4, 66–69. [Google Scholar]
- Pinkas, J.; Jankowski, M.; Szumowski, Ł.; Lusawa, A.; Zgliczyński, W.S.; Raciborski, F.; Wierzba, W.; Gujski, M. Public Health Interventions to Mitigate Early Spread of SARS-CoV-2 in Poland. Med. Sci. Monit. 2020, 26, e924730. [Google Scholar] [CrossRef] [PubMed]
- Koronawirus We Wrocławiu, Na Dolnym Śląsku, w Polsce [RAPORT 31.12]. Available online: https://wroclife.pl/nasze-miasto/koronawirus-wroclaw-2020/koronawirus-dolny-slask-31-grudnia/ (accessed on 19 May 2021).
- Koronawirus w Polsce: Ile zakażeń Dzisiaj (31.12)? Jaki Jest Stan Zachorowań w Woj. łódzkim? OGROM ZGONÓW! [RAPORT KORONAWIRUS]. Available online: https://lodz.se.pl/koronawirus-w-polsce-ile-zakazen-dzisiaj-31-12-jaki-jest-stan-zachorowan-w-woj-lodzkim-raport-koronawirus-aa-biAS-QgE2-yMyL.html (accessed on 19 May 2021).
- Urząd Statystyczny We Wrocławiu. Available online: https://wroclaw.stat.gov.pl (accessed on 19 May 2021).
- Urząd Statystyczny w Łodzi. Available online: https://lodz.stat.gov.pl (accessed on 19 May 2021).
- Raciborski, F.; Pinkas, J.; Jankowski, M.; Sierpiński, R.; Zgliczyński, W.S.; Szumowski, Ł.; Rakocy, K.; Wierzba, W.; Gujski, M. Dynamics of the Coronavirus Disease 2019 Outbreak in Poland: An Epidemiological Analysis of the First 2 Months of the Epidemic. Pol. Arch. Intern. Med. 2020, 130, 615–621. [Google Scholar] [PubMed]
- Nowak, B.; Szymański, P.; Pańkowski, I.; Szarowska, A.; Życińska, K.; Rogowski, W.; Gil, R.; Furmanek, M.; Tatur, J.; Zaczyński, A.; et al. Clinical Characteristics and Short-Term Outcomes of Patients with Coronavirus Disease 2019: A Retrospective Sin-Gle-Center Experience of a Designated Hospital in Poland. Pol. Arch. Intern. Med. 2020, 29, 407–411. [Google Scholar]
- Strategia Walki z Pandemią COVID-19. Available online: https://www.termedia.pl/mz/-Strategia-walki-z-pandemia-COVID-19-,39390.html (accessed on 19 May 2021).
- Dudink, E.; Essers, B.; Holvoet, W.; Weijs, B.; Luermans, J.; Ramanna, H.; Liem, A.; Opstal, J.; Dekker, L.; Dijk, V.; et al. Acute Car-Dioversion vs a Wait-and-See Approach for Recent-Onset Symptomatic Atrial Fibrillation in the Emergency Department: Ra-Tionale and Design of the Randomized ACWAS Trial. Am. Heart J. 2017, 183, 49–53. [Google Scholar] [CrossRef]
- D’Ascenzi, F.; Cameli, M.; Forni, S.; Gemmi, F.; Szasz, C.; Fabrizio, V.D.; Mechi, M.T.; Nocci, M.; Mondillo, S.; Valente, S. Reduction of Emergency Calls and Hospitalizations for Cardiac Causes: Effects of Covid-19 Pandemic and Lockdown in Tuscany Region. Front. Cardiovasc. Med. 2021, 8, 625569. [Google Scholar] [CrossRef] [PubMed]
- Pluymaekers, N.A.H.A.; Dudink, E.A.M.P.; Luermans, J.G.L.M.; Meeder, J.G.; Lenderink, T.; Widdershoven, J.; Bucx, J.J.J.; Rienstra, M.; Kamp, O.; Van Opstal, J.M.; et al. RACE 7 ACWAS Investigators. Early or Delayed Cardioversion in Recent-Onset Atrial Fibrillation. N. Engl. J. Med. 2019, 380, 1499–1508. [Google Scholar] [CrossRef]
- Capucci, A.; Compagnucci, P. Is Delayed Cardioversion the Better Approach in Recent-Onset Atrial Fibrillation? No. Intern. Emerg. Med. 2020, 15, 5–7. [Google Scholar] [CrossRef]
- Wakai, A.; O’Neill, J.O. Emergency Management of Atrial Fibrillation. Postgrad. Med. J. 2003, 79, 313–319. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| University Hospital | Copernicus Memorial Hospital | |||||
|---|---|---|---|---|---|---|
| Non-Pandemic Period | Pandemic Period | SARS-CoV-2 Positive /Convalescent in the Pandemic Period | Non-Pandemic Period | Pandemic Period | SARS-CoV-2 Positive /Convalescents in the Pandemic Period | |
| Number of Patients | 193 | 128 | 3 (1 SARS-CoV-2 positive, 2 convalescents) | 102 | 85 | 4 SARS-COV-2 positive |
| Number of AF visits July–December | 232 | 157 | 3 | 117 | 95 | 4 |
| Number of visits per a patient | 1.2 | 1.2 | 1 | 1.1 | 1.2 | 1 |
| Age years+/−SD | 70.0+/−13.9 | 70.0+/−15.0 | 60.7+/−11.1 | 73.8+/−12.3 * | 73.3+/−11.1 * | 77.0+/−9.8 |
| Male gender n (%) | 107 (55.4) | 86 (44.6) | 2 (66.7) | 63 (49.2) | 39 (45.8) | 3 (75) |
| University Hospital | Copernicus Memorial Hospital | |||||
|---|---|---|---|---|---|---|
| Non-Pandemic Period | Pandemic Period | SARS-CoV-2 Positive /Convalescents in the Pandemic Period | Non-Pandemic Period | Pandemic Period | SARS-CoV-2 Positive /Convalescents in the Pandemic Period | |
| July n (%) | 37 (16.0) | 29 (18.5) | 0/0 | 23 (19.7) | 15 (15.8) | 0 |
| August n (%) | 36 (15.5) | 27 (17.2) | 0/0 | 18 (15.4) | 20 (21.1) | 0 |
| September n (%) | 33 (14.2) | 25 (15.9) | 0/0 | 14 (12.0) | 20 (21.1) | 0 |
| October n (%) | 47 (20.3) | 26 (16.6) | 1/0 | 21 (18.0) | 15 (15.8) | 3 |
| November n (%) | 34 (14.7) | 13 (8.3) | 0/0 | 19 (16.2) | 11 (11.6) | 1 |
| December n (%) | 45 (19.4) | 37 (23.6) | 0/2 | 22 (18.8) | 14 (14.8) | 0 |
| Total July–December n (%) | 232 (100) | 157 (100) | 1/2 | 117 (100) | 95 (100) | 4/0 |
| Time since AF onset (h; N*) | 5 (3–15.5) | 10 (4–48) @ | 5 | 6 (2–24) | 12 (6–72) @ | 1 |
| N* = 164 | N* = 111 | N* = 1 | N* = 70 | N* = 61 | N* = 1 | |
| ED stay duration (min) | 362 | 452 ^ | 227 | 322 | 312 | 1007 |
| (227–507) | (290–598) | (243–967) | (88–519) | (180–527) | (550–1162) | |
| Sinus rhythm restoration n (%) | 147 (63.4) | 78 (49.7) $ | 2 (66.7) | 69 (72.6) | 76 (65) # | 2 (50.0) |
| University Hospital | Copernicus Memorial Hospital | |||
|---|---|---|---|---|
| Non-Pandemic Period | Pandemic Period | Non-Pandemic Period | Pandemic Period | |
| Electro-cardioversion N (%) | 14 (6) | 16 (10.2) | 1 | |
| 23 (19.7) * | 8 (19.0) | |||
| Phenazolinum n (%) | 72 (31.6) | 118 (30.3) | 37 (31.6) | 35 (36.8) |
| Amiodarone n (%) | 14 (6.0) | 13 (8.3) | 9 (7.7) | 15 (15.8) |
| Beta blocker n (%) | 19 (8.2) | 23 (14.7) | 61 (52.1) * | 69 (72.6) * |
| Propafenone n (%) | 13 (3.3) | 6 (3.8) | 24 (11.3) * | 7 (7.4) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bilaszewski, Ł.; Timler, W.; Budrewicz, K.; Marczak, M.; Kozłowski, R.; Wizowska, J.; Timler, M.; Jagielski, D.; Dudek, M.; Rasmus, P.; et al. The Impact of COVID-19 on Admissions and Management of Patients with Atrial Fibrillation Episodes in the Emergency Department. Int. J. Environ. Res. Public Health 2021, 18, 6048. https://doi.org/10.3390/ijerph18116048
Bilaszewski Ł, Timler W, Budrewicz K, Marczak M, Kozłowski R, Wizowska J, Timler M, Jagielski D, Dudek M, Rasmus P, et al. The Impact of COVID-19 on Admissions and Management of Patients with Atrial Fibrillation Episodes in the Emergency Department. International Journal of Environmental Research and Public Health. 2021; 18(11):6048. https://doi.org/10.3390/ijerph18116048
Chicago/Turabian StyleBilaszewski, Łukasz, Wojciech Timler, Katarzyna Budrewicz, Michał Marczak, Remigiusz Kozłowski, Joanna Wizowska, Małgorzata Timler, Dariusz Jagielski, Michał Dudek, Paweł Rasmus, and et al. 2021. "The Impact of COVID-19 on Admissions and Management of Patients with Atrial Fibrillation Episodes in the Emergency Department" International Journal of Environmental Research and Public Health 18, no. 11: 6048. https://doi.org/10.3390/ijerph18116048
APA StyleBilaszewski, Ł., Timler, W., Budrewicz, K., Marczak, M., Kozłowski, R., Wizowska, J., Timler, M., Jagielski, D., Dudek, M., Rasmus, P., Zyśko, D., & Timler, D. (2021). The Impact of COVID-19 on Admissions and Management of Patients with Atrial Fibrillation Episodes in the Emergency Department. International Journal of Environmental Research and Public Health, 18(11), 6048. https://doi.org/10.3390/ijerph18116048