
Kramer Score, an Evidence of Its Use in Accordance with Indonesian Hyperbilirubinemia Published Guideline

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
Data Analysis
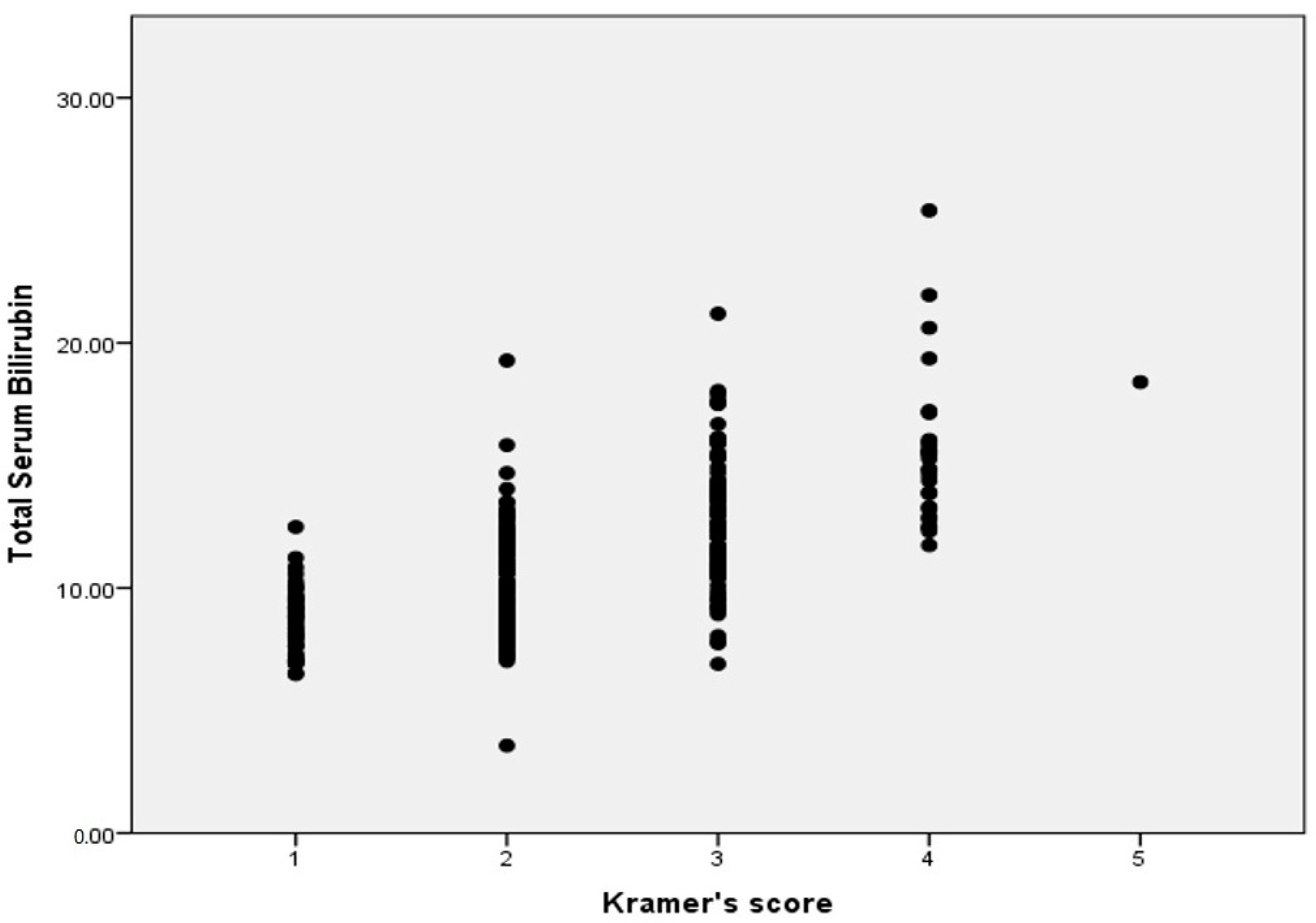
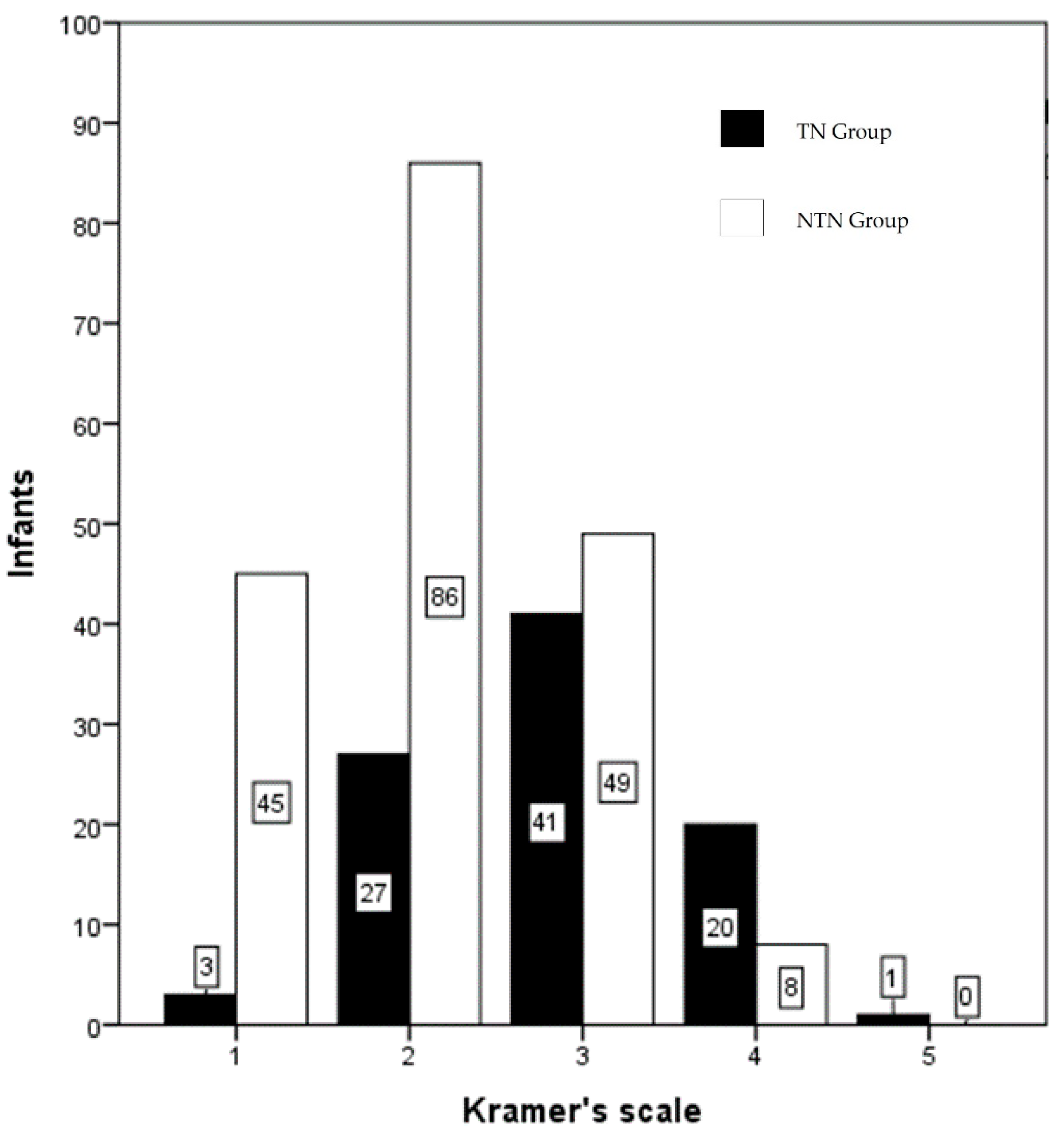
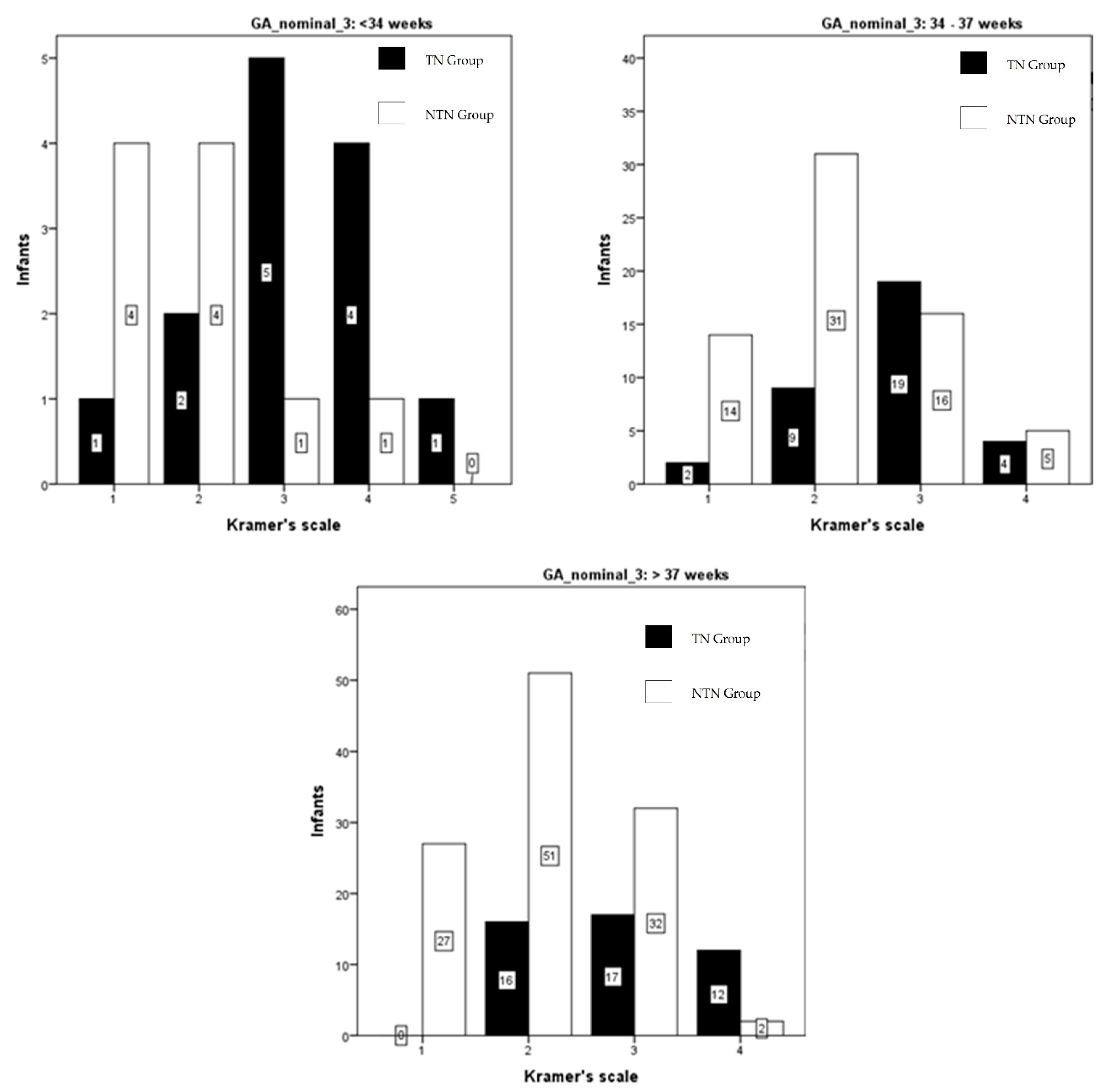
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Olusanya, B.O.; Osibanjo, F.B.; Slusher, T.M. Risk factors for severe neonatal hyperbilirubinemia in low and middle-income countries: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0117229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, T.W.R.; Wong, R.J.; Stevenson, D.K. Molecular physiology and pathophysiology of bilirubin handling by the blood, liver, intestine, and brain in the newborn. Physiol. Rev. 2020, 100, 1291–1346. [Google Scholar] [CrossRef] [PubMed]
- Maisels, J.; McDonagh, A. Phototherapy for neonatal jaundice. N. Engl. J. Med. 2008, 358, 920–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mabogunje, C.A.; Olaifa, S.M.; Olusanya, B.O. Facility-based constraints to exchange transfusions for neonatal hyperbilirubinemia in resource-limited settings. World J. Clin. Paediatr. 2016, 5, 182. [Google Scholar] [CrossRef] [PubMed]
- Olusanya, B.O.; Ogunlesi, T.A.; Kumar, P.; Boo, N.Y.; Iskander, I.F.; Almeida, M.F.; Vaucher, Y.E.; Slusher, T.M. Management of late-preterm and term infants with hyperbilirubinaemia in resource-constrained settings. BMC Paediatr. 2015, 15, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, L.I. Advancement of Dermal Icterus in the Jaundiced Newborn. Am. J. Dis. Child. 1969, 118, 454–458. [Google Scholar] [CrossRef] [PubMed]
- Menteri Kesehatan Republik Indonesia. Pedoman Nasional Pelayanan Kedokteran Tata Laksana Hiperbilirubinemia; 2019; pp. 1–97. Available online: http://yankes.kemkes.go.id/unduh/fileunduhan_1610349726_94555.pdf/16 (accessed on 15 February 2021).
- BiliNorm: Web-Based Hyperbilirubinemia Management. Available online: https://www.bilinorm.babyhealthsby.org/#/intro (accessed on 1 June 2021).
- Keren, R.; Tremont, K.; Luan, X.; Cnaan, A. Visual assessment of jaundice in term and late preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 2009, 94, F317–F322. [Google Scholar] [CrossRef] [PubMed]
- Tikmani, S.S.; Warraich, H.J.; Abbasi, F.; Rizvi, A.; Darmstadt, G.L.; Zaidi, A.K.M. Incidence of neonatal hyperbilirubinemia: A population-based prospective study in Pakistan. Trop. Med. Int. Health 2010, 15, 502–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okwundu, C.I.; Saini, S.S. Noninvasive Methods for Bilirubin Measurements in Newborns: A Report. Semin. Perinatol. 2021, 45, 151355. [Google Scholar] [CrossRef] [PubMed]
- Afanetti, M.; dit Eleni, T.S.; Yousef, N. Transkutane Bilirubinbestimmung als Screening für alle Neugeborenen geeignet. Neonatol. Scan 2015, 4, 34. [Google Scholar]
- Maya-Enero, S.; Candel-Pau, J.; Garcia-Garcia, J.; López-Vílchez Ángeles, M.; Duran-Jordà, X. Reliability of transcutaneous bilirubin determination based on skin color determined by a neonatal skin color scale of our own. Eur. J. Paediatr. 2021, 180, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Szabo, P.; Wolf, M.; Bucher, H.U.; Haensse, D.; Fauchère, J.C.; Arlettaz, R. Assessment of jaundice in preterm neonates: Comparison between clinical assessment, two transcutaneous bilirubinometers and serum bilirubin values. Acta Paediatr. 2004, 93, 1491–1495. [Google Scholar] [CrossRef] [PubMed]
- Mcdonagh, F.; Lightner, D. ‘Like a Shrivelled Blood Orange’—Bilirubin, Jaundice, and Phototherapy Antony. Pediatrics 1985, 75, 443–455. [Google Scholar] [PubMed]
- Wong, R.J. Neonatal jaundice and liver disease. In Fanaroff and Martin’s Neonatal-Perinatal Medicine: Disease of the Fetus and Infant; Elsevier Mosby: St. Louis, MO, USA, 2006; p. 1419. [Google Scholar]
- Ree, I.M.C.; Smits-Wintjens, V.E.H.J.; van der Bom, J.G.; van Klink, J.M.M.; Oepkes, D.; Lopriore, E. Neonatal management and outcome in alloimmune hemolytic disease. Expert Rev. Hematol. 2017, 10, 607–616. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics (N = 280) | Value |
|---|---|
| Gestational age (weeks) | 37.3 ± 2.3 (32–42) |
| <34 weeks | 23 (8.2) |
| 34–37 weeks | 100 (35.7) |
| >37 weeks | 157 (56.1) |
| Birth weight (gram) | 2744.6 ± 685.8 (1500–4700) |
| 1500–1999 g | 53 (18.9) |
| 2000–2499 g | 44 (15.7) |
| 2500–2999 g | 68 (24.3) |
| 3000–3499 g | 82 (29.3) |
| ≥3500 g | 33 (11.8) |
| Age (days) | 3.9 ± 2.6 (1–14.8) |
| Age (hours) | 93 ± 62.2 (24–355) |
| Total Serum Bilirubin (mg/dL) | 11.31 ± 3.1 (3.57–25.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sampurna, M.T.A.; Mapindra, M.P.; Mahindra, M.P.; Ratnasari, K.A.; Rani, S.A.D.; Handayani, K.D.; Angelika, D.; Harianto, A.; Utomo, M.T.; Etika, R.; et al. Kramer Score, an Evidence of Its Use in Accordance with Indonesian Hyperbilirubinemia Published Guideline. Int. J. Environ. Res. Public Health 2021, 18, 6173. https://doi.org/10.3390/ijerph18116173
Sampurna MTA, Mapindra MP, Mahindra MP, Ratnasari KA, Rani SAD, Handayani KD, Angelika D, Harianto A, Utomo MT, Etika R, et al. Kramer Score, an Evidence of Its Use in Accordance with Indonesian Hyperbilirubinemia Published Guideline. International Journal of Environmental Research and Public Health. 2021; 18(11):6173. https://doi.org/10.3390/ijerph18116173
Chicago/Turabian StyleSampurna, Mahendra Tri Arif, Muhammad Pradhika Mapindra, Muhammad Pradhiki Mahindra, Kinanti Ayu Ratnasari, Siti Annisa Dewi Rani, Kartika Darma Handayani, Dina Angelika, Agus Harianto, Martono Tri Utomo, Risa Etika, and et al. 2021. "Kramer Score, an Evidence of Its Use in Accordance with Indonesian Hyperbilirubinemia Published Guideline" International Journal of Environmental Research and Public Health 18, no. 11: 6173. https://doi.org/10.3390/ijerph18116173
APA StyleSampurna, M. T. A., Mapindra, M. P., Mahindra, M. P., Ratnasari, K. A., Rani, S. A. D., Handayani, K. D., Angelika, D., Harianto, A., Utomo, M. T., Etika, R., & Sauer, P. J. J. (2021). Kramer Score, an Evidence of Its Use in Accordance with Indonesian Hyperbilirubinemia Published Guideline. International Journal of Environmental Research and Public Health, 18(11), 6173. https://doi.org/10.3390/ijerph18116173