
Manual Therapy in Cervical and Lumbar Radiculopathy: A Systematic Review of the Literature


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Protocol
2.2. Search Strategy and Selection Criteria
2.3. Data Extraction and Quality Assessment
3. Results
3.1. Quality Assessment
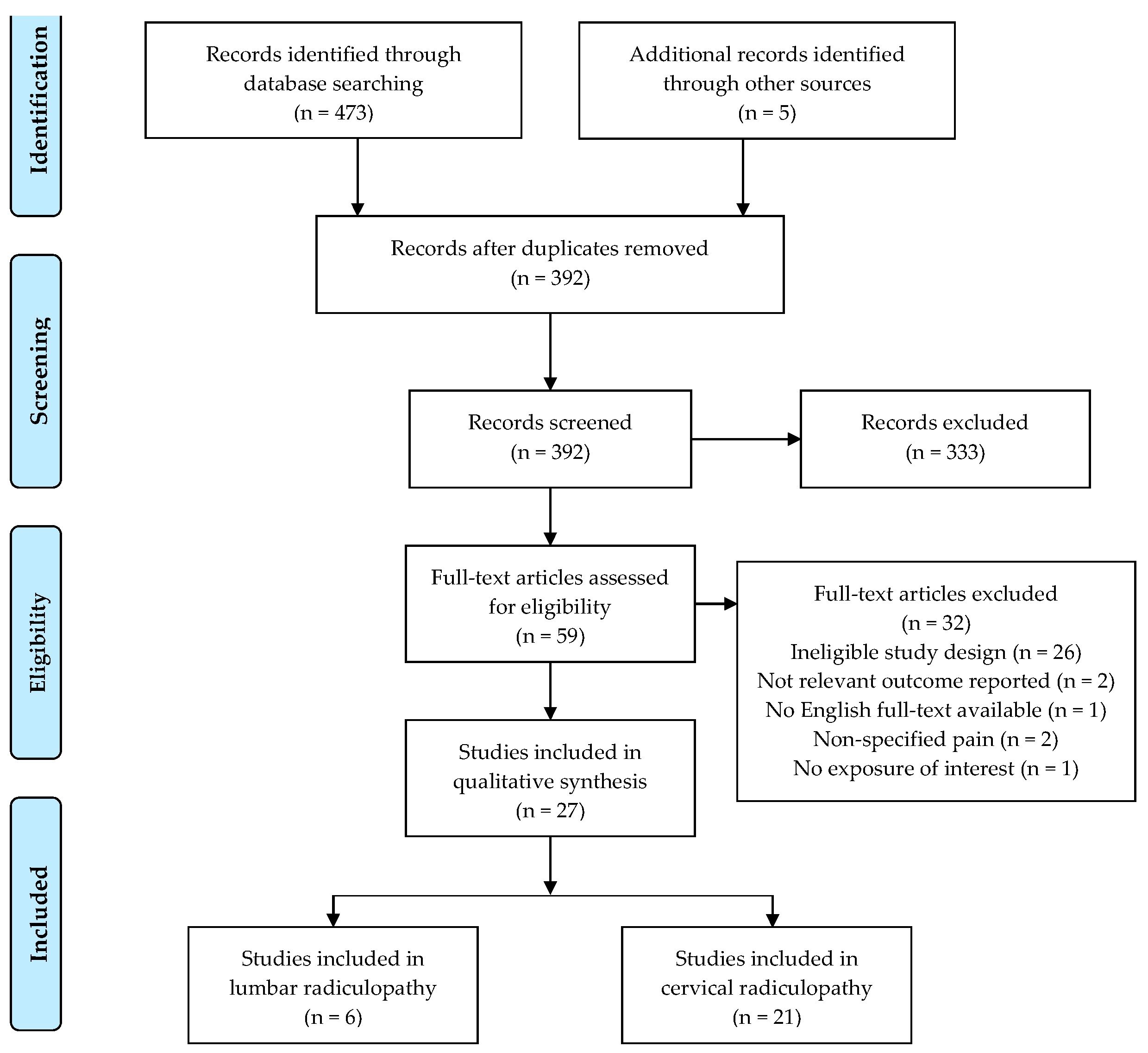
3.2. Literature Search
3.3. Study Characteristics
3.4. Types of Manual Therapy
4. Discussion
4.1. Cervical Radiculopathy
4.2. Lumbar Radiculopathy
4.3. Methodological Concerns
4.4. Future Directions
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Childress, M.A.; Becker, B.A. Nonoperative Management of Cervical Radiculopathy. Am. Fam. Physician 2016, 93, 746–754. [Google Scholar]
- Beckworth, W.J.; Abramoff, B.A.; Bailey, I.M.; Yoon, S.; Umpierrez, M.; Kakarala, A.; Lee, J.Y.; Ward, L.A.; Dows-Martinez, M.N.; Yoon, S.T. Acute Cervical Radiculopathy Outcomes: Soft Disc Herniations vs Osteophytes. Pain Med. 2021, 22, 561–566. [Google Scholar] [CrossRef]
- Corey, D.L.; Comeau, D. Cervical Radiculopathy. Med. Clin. N. Am. 2014, 98, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Tarulli, A.W.; Raynor, E.M. Lumbosacral Radiculopathy. Neurol. Clin. 2007, 25, 387–405. [Google Scholar] [CrossRef]
- Thoomes, E.J. Effectiveness of Manual Therapy for Cervical Radiculopathy, a Review. Chiropr. Man. Ther. 2016, 24, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Selkirk, S.M.; Ruff, R. Low Back Pain, Radiculopathy. Handb. Clin. Neurol. 2016, 136, 1027–1033. [Google Scholar] [CrossRef]
- Berry, J.A.; Elia, C.; Saini, H.S.; Miulli, D.E. A Review of Lumbar Radiculopathy, Diagnosis, and Treatment. Cureus 2019, 11, e5934. [Google Scholar] [CrossRef] [Green Version]
- Benoist, M. The Natural History of Lumbar Disc Herniation and Radiculopathy. Jt. Bone 2002, 69, 155–160. [Google Scholar] [CrossRef]
- Huysmans, E.; Goudman, L.; Van Belleghem, G.; De Jaeger, M.; Moens, M.; Nijs, J.; Ickmans, K.; Buyl, R.; Vanroelen, C.; Putman, K. Return to Work Following Surgery for Lumbar Radiculopathy: A Systematic Review. Spine J. 2018, 18, 1694–1714. [Google Scholar] [CrossRef]
- Cohen, S.P. Epidemiology, Diagnosis, and Treatment of Neck Pain. Mayo Clin. Proc. 2015, 90, 284–299. [Google Scholar] [CrossRef] [Green Version]
- Benditz, A.; Loher, M.; Boluki, D.; Grifka, J.; Völlner, F.; Renkawitz, T.; Maderbacher, G.; Götz, J. Positive Medium-Term Influence of Multimodal Pain Management on Socioeconomic Factors and Health Care Utilization in Patients with Lumbar Radiculopathy: A Prospective Study. J. Pain Res. 2017, 10, 389–395. [Google Scholar] [CrossRef] [Green Version]
- Casey, E. Natural History of Radiculopathy. Phys. Med. Rehabil. Clin. N. Am. 2011, 22, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Woods, B.I.; Hilibrand, A.S. Cervical Radiculopathy: Epidemiology, Etiology, Diagnosis, and Treatment. J. Spinal Disord. Tech. 2015, 28, 251–259. [Google Scholar] [CrossRef]
- Yamazaki, S.; Kokubun, S.; Ishii, Y.; Tanaka, Y. Courses of Cervical Disc Herniation Causing Myelopathy or Radiculopathy: An Analysis Based on Computed Tomographic Discograms. Spine 2003, 28, 1171–1175. [Google Scholar] [CrossRef]
- Rhee, J.M.; Yoon, T.; Riew, K.D. Cervical Radiculopathy. J. Am. Acad. Orthop. Surg. 2007, 15, 486–494. [Google Scholar] [CrossRef]
- Ostelo, R.W. Physiotherapy Management of Sciatica. J. Physiother. 2020, 66, 83–88. [Google Scholar] [CrossRef]
- Wang, R.; Weng, L.-M.; Peng, M.-S.; Wang, X.-Q. Exercise for Low Back Pain: A Bibliometric Analysis of Global Research from 1980 to 2018. J. Rehabil. Med. 2020, 52, jrm00052. [Google Scholar] [CrossRef]
- Sheng, Y.; Duan, Z.; Qu, Q.; Chen, W.; Yu, B. Kinesio Taping in Treatment of Chronic Non-Specific Low Back Pain: A Systematic Review and Meta-Analysis. J. Rehabil. Med. 2019, 51, 734–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pennetti, A. A Multimodal Physical Therapy Approach Utilizing the Maitland Concept in the Management of a Patient with Cervical and Lumbar Radiculitis and Ehlers-Danlos Syndrome-Hypermobility Type: A Case Report. Physiother. Theory Pract. 2018, 34, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Bilgilisoy Filiz, M.; Kiliç, Z.; Uçkun, A.; Çakir, T.; Koldaş Doğan, Ş.; Toraman, N.F. Mechanical Traction for Lumbar Radicular Pain: Supine or Prone? A Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2018, 97, 433–439. [Google Scholar] [CrossRef]
- Eubanks, J.D. Cervical Radiculopathy: Nonoperative Management of Neck Pain and Radicular Symptoms. Am. Fam. Physician 2010, 81, 33–40. [Google Scholar] [PubMed]
- Romeo, A.; Vanti, C.; Boldrini, V.; Ruggeri, M.; Guccione, A.A.; Pillastrini, P.; Bertozzi, L. Cervical Radiculopathy: Effectiveness of Adding Traction to Physical Therapy-A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Phys. Ther. 2018, 98, 231–242. [Google Scholar] [CrossRef] [PubMed]
- Fritz, J.M.; Thackeray, A.; Childs, J.D.; Brennan, G.P. A Randomized Clinical Trial of the Effectiveness of Mechanical Traction for Sub-Groups of Patients with Low Back Pain: Study Methods and Rationale. BMC Musculoskelet. Disord. 2010, 11, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benditz, A.; Brunner, M.; Zeman, F.; Greimel, F.; Florian, V.; Boluki, D.; Grifka, J.; Weber, M.; Renkawitz, T. Effectiveness of a Multimodal Pain Management Concept for Patients with Cervical Radiculopathy with Focus on Cervical Epidural Injections. Sci. Rep. 2017, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, L.; Wei, X.; Wang, S. Does Cervical Spine Manipulation Reduce Pain in People with Degenerative Cervical Radiculopathy? A Systematic Review of the Evidence, and a Meta-Analysis. Clin. Rehabil. 2016, 30, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Rodine, R.J.; Vernon, H. Cervical Radiculopathy: A Systematic Review on Treatment by Spinal Manipulation and Measurement with the Neck Disability Index. J. Can. Chiropr. Assoc. 2012, 56, 18–28. [Google Scholar]
- Leininger, B.; Bronfort, G.; Evans, R.; Reiter, T. Spinal Manipulation or Mobilization for Radiculopathy: A Systematic Review. Phys. Med. Rehabil. Clin. N. Am. 2011, 22, 105–125. [Google Scholar] [CrossRef]
- Efstathiou, M.A.; Stefanakis, M.; Savva, C.; Giakas, G. Effectiveness of Neural Mobilization in Patients with Spinal Radiculopathy: A Critical Review. J. Bodyw. Mov. Ther. 2015, 19, 205–212. [Google Scholar] [CrossRef]
- Boyles, R.; Toy, P.; Mellon, J.; Hayes, M.; Hammer, B. Effectiveness of Manual Physical Therapy in the Treatment of Cervical Radiculopathy: A Systematic Review. J. Man. Manip. Ther. 2011, 19, 135–142. [Google Scholar] [CrossRef] [Green Version]
- Andersen, M.Ø.; Andresen, A.K.; Lorenzen, M.D.; Isenberg-Jørgensen, A.; Støttrup, C. Non-surgical treatment of lumbar radiculopathy. Ugeskr. Laeger. 2017, 179, V05170397. [Google Scholar]
- Verhagen, A.P.; de Vet, H.C.; de Bie, R.A.; Kessels, A.G.; Boers, M.; Bouter, L.M.; Knipschild, P.G. The Delphi List: A Criteria List for Quality Assessment of Randomized Clinical Trials for Conducting Systematic Reviews Developed by Delphi Consensus. J. Clin. Epidemiol. 1998, 51, 1235–1241. [Google Scholar] [CrossRef] [Green Version]
- van Tulder, M.; Furlan, A.; Bombardier, C.; Bouter, L.; Editorial Board of the Cochrane Collaboration Back Review Group. Updated Method Guidelines for Systematic Reviews in the Cochrane Collaboration Back Review Group. Spine 2003, 28, 1290–1299. [Google Scholar] [CrossRef] [Green Version]
- Herrador Colmenero, L.; Perez Marmol, J.M.; Martí-García, C.; de Los Ángeles Querol Zaldivar, M.; Tapia Haro, R.M.; Castro Sánchez, A.M.; Aguilar-Ferrándiz, M.E. Effectiveness of Mirror Therapy, Motor Imagery, and Virtual Feedback on Phantom Limb Pain Following Amputation: A Systematic Review. Prosthet. Orthot. Int. 2018, 42, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Hassan, F.; Osama, M.; Ghafoor, A.; Yaqoob, M.F. Effects of Oscillatory Mobilization as Compared to Sustained Stretch Mobilization in the Management of Cervical Radiculopathy: A Randomized Controlled Trial. J. Back Musculoskelet. Rehabil. 2020, 33, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Young, I.A.; Pozzi, F.; Dunning, J.; Linkonis, R.; Michener, L.A. Immediate and Short-Term Effects of Thoracic Spine Manipulation in Patients With Cervical Radiculopathy: A Randomized Controlled Trial. J. Orthop. Sports Phys. Ther. 2019, 49, 299–309. [Google Scholar] [CrossRef]
- Eldesoky, M.T.; Al Amer, H.S.; Abutaleb, E.E.; Nassif, A.A. Effect of Cervical Mobilization on Nerve Root Function in Cervical Radiculopathy: A Randomized Trial. Biosci. Res. 2019, 16, 3962–3972. [Google Scholar]
- Afzal, R.; Ghous, M.; Shakil Ur Rehman, S.; Masood, T. Comparison between Manual Traction, Manual Opening Technique and Combination in Patients with Cervical Radiculopathy: Randomized Control Trial. J. Pak. Med. Assoc. 2019, 69, 1237–1241. [Google Scholar] [PubMed]
- Ayub, A.; Osama, M.; Ahmad, S. Effects of Active versus Passive Upper Extremity Neural Mobilization Combined with Mechanical Traction and Joint Mobilization in Females with Cervical Radiculopathy: A Randomized Controlled Trial. J. Back Musculoskelet. Rehabil. 2019, 32, 725–730. [Google Scholar] [CrossRef]
- Ojoawo, A.O.; Olabode, A.D. Comparative Effectiveness of Transverse Oscillatory Pressure and Cervical Traction in the Management of Cervical Radiculopathy: A Randomized Controlled Study. Hong Kong Physiother. J. 2018, 38, 149–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, T.; Pan, X. Observation on Clinical Efficacy of Warm Needling Moxibustion plus Mulligan Dynamic Joint Mobilization for Cervical Radiculopathy. J. Acupunct. Tuina Sci. 2017, 15, 440–445. [Google Scholar] [CrossRef]
- Rodríguez-Sanz, D.; Calvo-Lobo, C.; Unda-Solano, F.; Sanz-Corbalán, I.; Romero-Morales, C.; López-López, D. Cervical Lateral Glide Neural Mobilization Is Effective in Treating Cervicobrachial Pain: A Randomized Waiting List Controlled Clinical Trial. Pain Med. 2017, 18, 2492–2503. [Google Scholar] [CrossRef]
- Cui, X.-J.; Yao, M.; Ye, X.-L.; Wang, P.; Zhong, W.-H.; Zhang, R.-C.; Li, H.-Y.; Hu, Z.-J.; Tang, Z.-Y.; Wang, W.-M.; et al. Shi-Style Cervical Manipulations for Cervical Radiculopathy: A Multicenter Randomized-Controlled Clinical Trial. Medicine 2017, 96, e7276. [Google Scholar] [CrossRef]
- Kim, D.-G.; Chung, S.H.; Jung, H.B. The Effects of Neural Mobilization on Cervical Radiculopathy Patients’ Pain, Disability, ROM, and Deep Flexor Endurance. J. Back Musculoskelet. Rehabil. 2017, 30, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.R.; Awan, W.A.; Rashid, S.; Masood, T. A Randomized Controlled Trial of Intermittent Cervical Traction in Sitting Vs. Supine Position for the Management of Cervical Radiculopathy. Pak. J. Med. Sci. 2017, 33, 1333–1338. [Google Scholar] [CrossRef] [PubMed]
- Savva, C.; Giakas, G.; Efstathiou, M.; Karagiannis, C.; Mamais, I. Effectiveness of Neural Mobilization with Intermittent Cervical Traction in the Management of Cervical Radiculopathy: A Randomized Controlled Trial. Int. J. Osteopath. Med. 2016, 21, 19–28. [Google Scholar] [CrossRef]
- Khan, K.; Yasmeen, S.; Ishaque, F.; Imdad, F.; Lal, W.; Sheikh, S.A.; Kumar, N.; Khanzada, S. Effectiveness of manual traction and other physiotherapy treatment in the management of painful cervical radiculopathy. Int. J. Physiother. 2016, 3, 286–290. [Google Scholar] [CrossRef]
- Waqas, S.; Ahmad, A.; Ahmad, S.; Shafi, T.; Shahid, H.A. Comparison of Maitland Thoracic Spine Manipulation Versus Maitland Cervical Spine Mobilization in Chronic Unilateral C6-C7 Cervical Radiculopathy. Ann. King Edw. Med. Univ. 2016, 22, 102–108. [Google Scholar] [CrossRef]
- Bukhari, S.R.I.; Shakil-ur-Rehman, S.; Ahmad, S.; Naeem, A. Comparison between Effectiveness of Mechanical and Manual Traction Combined with Mobilization and Exercise Therapy in Patients with Cervical Radiculopathy. Pak. J. Med. Sci. 2016, 32, 31–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costello, M.; Puentedura, E.; Louie, J.; Cleland, J.; Ciccone, C.D. The Immediate Effects of Soft Tissue Mobilization versus Therapeutic Ultrasound for Patients with Neck and Arm Pain with Evidence of Neural Mechanosensitivity: A Randomized Clinical Trial. J. Man. Manip. Ther. 2016, 24, 128–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langevin, P.; Desmeules, F.; Lamothe, M.; Robitaille, S.; Roy, J.-S. Comparison of 2 Manual Therapy and Exercise Protocols for Cervical Radiculopathy: A Randomized Clinical Trial Evaluating Short-Term Effects. J. Orthop. Sports Phys. Ther. 2015, 45, 4–17. [Google Scholar] [CrossRef] [Green Version]
- Fritz, J.M.; Thackeray, A.; Brennan, G.P.; Childs, J.D. Exercise Only, Exercise with Mechanical Traction, or Exercise with over-Door Traction for Patients with Cervical Radiculopathy, with or without Consideration of Status on a Previously Described Subgrouping Rule: A Randomized Clinical Trial. J. Orthop. Sports Phys. Ther. 2014, 44, 45–57. [Google Scholar] [CrossRef] [Green Version]
- Jellad, A.; Ben Salah, Z.; Boudokhane, S.; Migaou, H.; Bahri, I.; Rejeb, N. The Value of Intermittent Cervical Traction in Recent Cervical Radiculopathy. Ann. Phys. Rehabil. Med. 2009, 52, 638–652. [Google Scholar] [CrossRef] [Green Version]
- Young, I.A.; Michener, L.A.; Cleland, J.A.; Aguilera, A.J.; Snyder, A.R. Manual Therapy, Exercise, and Traction for Patients with Cervical Radiculopathy: A Randomized Clinical Trial. Phys. Ther. 2009, 89, 632–642. [Google Scholar] [CrossRef] [Green Version]
- Joghataei, M.T.; Arab, A.M.; Khaksar, H. The Effect of Cervical Traction Combined with Conventional Therapy on Grip Strength on Patients with Cervical Radiculopathy. Clin. Rehabil. 2004, 18, 879–887. [Google Scholar] [CrossRef]
- Plaza-Manzano, G.; Cancela-Cilleruelo, I.; Fernández-de-Las-Peñas, C.; Cleland, J.A.; Arias-Buría, J.L.; Thoomes-de-Graaf, M.; Ortega-Santiago, R. Effects of Adding a Neurodynamic Mobilization to Motor Control Training in Patients With Lumbar Radiculopathy Due to Disc Herniation: A Randomized Clinical Trial. Am. J. Phys. Med. Rehabil. 2020, 99, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Satpute, K.; Hall, T.; Bisen, R.; Lokhande, P. The Effect of Spinal Mobilization With Leg Movement in Patients With Lumbar Radiculopathy-A Double-Blind Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2019, 100, 828–836. [Google Scholar] [CrossRef] [PubMed]
- Tambekar, N.; Sabnis, S.; Phadke, A.; Bedekar, N. Effect of Butler’s Neural Tissue Mobilization and Mulligan’s Bent Leg Raise on Pain and Straight Leg Raise in Patients of Low Back Ache. J. Bodyw. Mov. Ther. 2016, 20, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, I.M.; Diab, A.A. Extension Traction Treatment for Patients with Discogenic Lumbosacral Radiculopathy: A Randomized Controlled Trial. Clin. Rehabil. 2013, 27, 51–62. [Google Scholar] [CrossRef] [PubMed]
- McMorland, G.; Suter, E.; Casha, S.; du Plessis, S.J.; Hurlbert, R.J. Manipulation or Microdiskectomy for Sciatica? A Prospective Randomized Clinical Study. J. Manip. Physiol. Ther. 2010, 33, 576–584. [Google Scholar] [CrossRef]
- Gudavalli, M.R.; Cambron, J.A.; McGregor, M.; Jedlicka, J.; Keenum, M.; Ghanayem, A.J.; Patwardhan, A.G. A Randomized Clinical Trial and Subgroup Analysis to Compare Flexion-Distraction with Active Exercise for Chronic Low Back Pain. Eur. Spine J. 2006, 15, 1070–1082. [Google Scholar] [CrossRef] [Green Version]
- Bobos, P.; MacDermid, J.C.; Walton, D.M.; Gross, A.; Santaguida, P.L. Patient-Reported Outcome Measures Used for Neck Disorders: An Overview of Systematic Reviews. J. Orthop. Sports Phys. Ther. 2018, 48, 775–788. [Google Scholar] [CrossRef]
- Young, I.A.; Cleland, J.A.; Michener, L.A.; Brown, C. Reliability, Construct Validity, and Responsiveness of the Neck Disability Index, Patient-Specific Functional Scale, and Numeric Pain Rating Scale in Patients with Cervical Radiculopathy. Am. J. Phys. Med. Rehabil. 2010, 89, 831–839. [Google Scholar] [CrossRef]
- Brodke, D.S.; Goz, V.; Lawrence, B.D.; Spiker, W.R.; Neese, A.; Hung, M. Oswestry Disability Index: A Psychometric Analysis with 1,610 Patients. Spine J. 2017, 17, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Shafique, S.; Ahmad, S.; Shakil-Ur-Rehman, S. Effect of Mulligan Spinal Mobilization with Arm Movement along with Neurodynamics and Manual Traction in Cervical Radiculopathy Patients: A Randomized Controlled Trial. J. Pak. Med. Assoc. 2019, 69, 1601–1604. [Google Scholar] [CrossRef] [PubMed]
- Wainner, R.S.; Fritz, J.M.; Irrgang, J.J.; Boninger, M.L.; Delitto, A.; Allison, S. Reliability and Diagnostic Accuracy of the Clinical Examination and Patient Self-Report Measures for Cervical Radiculopathy. Spine 2003, 28, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Li, W.-X.; Liu, Z.; Liu, L. Balance Chiropractic Therapy for Cervical Spondylotic Radiculopathy: Study Protocol for a Randomized Controlled Trial. Trials 2016, 17, 513. [Google Scholar] [CrossRef] [Green Version]
- Akkan, H.; Gelecek, N. The Effect of Stabilization Exercise Training on Pain and Functional Status in Patients with Cervical Radiculopathy. J. Back Musculoskelet. Rehabil. 2018, 31, 247–252. [Google Scholar] [CrossRef]
- Wibault, J.; Öberg, B.; Dedering, Å.; Löfgren, H.; Zsigmond, P.; Peolsson, A. Structured Postoperative Physiotherapy in Patients with Cervical Radiculopathy: 6-Month Outcomes of a Randomized Clinical Trial. J. Neurosurg. Spine 2018, 28, 1–9. [Google Scholar] [CrossRef]
- Halvorsen, M.; Falla, D.; Gizzi, L.; Harms-Ringdahl, K.; Peolsson, A.; Dedering, Å. Short- and Long-Term Effects of Exercise on Neck Muscle Function in Cervical Radiculopathy: A Randomized Clinical Trial. J. Rehabil. Med. 2016, 48, 696–704. [Google Scholar] [CrossRef] [Green Version]
- Dedering, Å.; Peolsson, A.; Cleland, J.A.; Halvorsen, M.; Svensson, M.A.; Kierkegaard, M. The Effects of Neck-Specific Training Versus Prescribed Physical Activity on Pain and Disability in Patients With Cervical Radiculopathy: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2018, 99, 2447–2456. [Google Scholar] [CrossRef]
- Kostadinović, S.; Milovanović, N.; Jovanović, J.; Tomašević-Todorović, S. Efficacy of the Lumbar Stabilization and Thoracic Mobilization Exercise Program on Pain Intensity and Functional Disability Reduction in Chronic Low Back Pain Patients with Lumbar Radiculopathy: A Randomized Controlled Trial. J. Back Musculoskelet. Rehabil. 2020, 33, 897–907. [Google Scholar] [CrossRef] [PubMed]
- Ghasabmahaleh, S.H.; Rezasoltani, Z.; Dadarkhah, A.; Hamidipanah, S.; Mofrad, R.K.; Najafi, S. Spinal Manipulation for Subacute and Chronic Lumbar Radiculopathy: A Randomized Controlled Trial. Am. J. Med. 2021, 134, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Yin, M.; Mo, W.; Wu, H.; Xu, J.; Ye, J.; Chen, N.; Marla, A.S.; Ma, J. Efficacy of Caudal Epidural Steroid Injection with Targeted Indwelling Catheter and Manipulation in Managing Patients with Lumbar Disk Herniation and Radiculopathy: A Prospective, Randomized, Single-Blind Controlled Trial. World Neurosurg. 2018, 114, e29–e34. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author (Year) | (1) * | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | PEDro Score | IVS | Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cervical radiculopathy | ||||||||||||||
| Hassan et al. (2020) [34] | X | X | X | X | X | 5/10 | 2/7 | Limited | ||||||
| Young et al. (2019) [35] | X | X | X | X | X | X | X | X | X | X | 9/10 | 6/7 | High | |
| Eldesoky et al. (2019) [36] | X | X | X | X | X | X | X | X | 7/10 | 4/7 | Moderate | |||
| Afzal et al. (2019) [37] | X | X | X | X | X | X | X | 6/10 | 4/7 | Moderate | ||||
| Ayub et al. (2019) [38] | X | X | X | X | X | X | X | X | X | 8/10 | 5/7 | Moderate | ||
| Ojoawo and Olabode (2018) [39] | X | X | X | X | X | X | X | 6/10 | 3/7 | Limited | ||||
| Song and Pan (2017) [40] | X | X | X | X | X | X | X | X | 7/10 | 5/7 | Moderate | |||
| Rodríguez-Sanz et al. (2017) [41] | X | X | X | X | X | X | X | 6/10 | 4/7 | Moderate | ||||
| Cui et al. (2017) [42] | X | X | X | X | X | X | 6/10 | 3/7 | Limited | |||||
| Kim et al. (2017) [43] | X | X | X | X | X | X | 5/10 | 2/7 | Limited | |||||
| Khan et al. (2017) [44] | X | X | X | X | X | X | X | X | 7/10 | 4/7 | Moderate | |||
| Savva et al. (2016) [45] | X | X | X | X | X | X | X | 7/10 | 5/7 | Moderate | ||||
| Khan et al. (2016) [46] | X | X | X | X | X | X | 5/10 | 3/7 | Limited | |||||
| Waqas et al. (2016) [47] | X | X | X | X | X | 5/10 | 3/7 | Limited | ||||||
| Bukhari et al. (2016) [48] | X | X | X | X | X | X | 5/10 | 2/7 | Limited | |||||
| Costello et al. (2016) [49] | X | X | X | X | X | X | X | X | X | 8/10 | 5/7 | Moderate | ||
| Langevin et al. (2015) [50] | X | X | X | X | X | X | X | X | X | X | 9/10 | 6/7 | High | |
| Fritz et al. (2014) [51] | X | X | X | X | X | X | X | X | X | 8/10 | 5/7 | Moderate | ||
| Jellad et al. (2009) [52] | X | X | X | X | X | X | X | 6/10 | 3/7 | Limited | ||||
| Young et al. (2009) [53] | X | X | X | X | X | X | X | X | X | 8/10 | 5/7 | Moderate | ||
| Joghataei et al. (2004) [54] | X | X | X | X | X | X | X | 6/10 | 3/7 | Limited | ||||
| Lumbar radiculopathy | ||||||||||||||
| Plaza-Manzano et al. (2019) [55] | X | X | X | X | X | X | X | X | X | X | 9/10 | 6/7 | High | |
| Satpute et al. (2018) [56] | X | X | X | X | X | X | X | X | X | 8/10 | 5/7 | Moderate | ||
| Tambekar et al. (2015) [57] | X | X | X | X | X | X | 5/10 | 2/7 | Limited | |||||
| Moustafa et al. (2013) [58] | X | X | X | X | X | X | X | X | 7/10 | 4/7 | Moderate | |||
| McMorland et al. (2010) [59] | X | X | X | X | X | X | X | 6/10 | 3/7 | Limited | ||||
| Gudavalli et al. (2006) [60] | X | X | X | X | X | X | 5/10 | 2/7 | Limited | |||||
| %, X | 85 | 100 | 56 | 85 | 7 | 4 | 59 | 89 | 70 | 100 | 93 | |||
| Author (Year) | Groups Characteristic (Mean Age, Sex) | n | Interventions | Outcome Measures | Conclusions |
|---|---|---|---|---|---|
| Cervical radiculopathy | |||||
| Hassan et al. (2020) [34] | G1: 43.0 (14M, 6F) | G1: 20 | G1: Kaltenborn sustained stretch mobilization, TENS, hot packs | NPRS NDI ROM | Both oscillatory and sustained stretch mobilization techniques are found to be effective in the management of cervical radiculopathy in terms of pain, range and disability. However, oscillatory mobilization is found to be superior in terms of functional ability and range of motion. |
| G2: 43.0 (13M, 7F) | G2: 20 | G2: Maitland oscillatory mobilization, TENS, hot packs | |||
| Young et al. (2019) [35] | G1: 48.8 (5M, 17F) G2: 43.1 (9M, 12F) | G1: 22 G2: 21 | G1: Thoracic spine manipulation G2: Sham thoracic spine manipulation | NPRS NDI ROM | One session of thoracic manipulation resulted in improvements in pain, disability, cervical ROM, and deep neck flexor endurance in patients with cervical radiculopathy. |
| Eldesoky et al. (2019) [36] | G1: 43.1 (13M, F12) G2: 43.9 (14M, 11F) | G1: 25 G2: 25 | G1: Maitland postero-anterior and rotation oscillatory mobilization techniques G2: Therapeutic ultrasonic and exercise program | VAS NDI Somatosensory evoked potentials | Cervical mobilization could be utilized as an effective physical therapy program design for patients with cervical radiculopathy for improvement of pain level, functional disability and nerve root function. |
| Afzal et al. (2019) [37] | G1: 42.1 (M, F) G2: 40.9 (M, F) G3: 42.5 (M, F) | G1: 13 G2: 13 G3: 14 | G1: Opening of intervertebral foramen technique G2: Manual cervical traction G3: Combined both above techniques | NPRS NDI PSFS Active extension/extension Right/left side bending Right/left Rotation | Manual intervertebral foramen opening technique, manual traction, and combination of both techniques were equally effective in decreasing pain, level of disability and improved cervical mobility in patients with cervical radiculopathy. |
| Ayub et al. (2019) [38] | G1: 21.9 (0M, 22F) G2: 23.1 (0M, 22F) | G1: 22 G2: 22 | G1: Cervical traction, Unilateral Posterior Anterior glide and passive upper extremity neural mobilization G2: Cervical traction, Unilateral Posterior Anterior glide and active upper extremity neural mobilization | NPRS NDI ROM | Both active and passive neural mobilization is effective in the management of cervical radiculopathy. One of the interventions is not superior to the other. |
| Ojoawo and Olabode (2018) [39] | G1: 51.4 (14M, 11F) G2: 55.7 (15M, 10F) G3: 59.5 (11M, 14F) | G1: 25 G2: 25 G3: 25 | G1: Cervical traction plus Exercise, massage, ice therapy G2: Transverse oscillatory pressure plus Exercise, massage, ice therapy G3: Exercise, massage, ice therapy only | VAS NDI | Transverse oscillatory pressure reduces the PI and disability of patients with cervical radiculopathy more quickly, compared to conventional therapy. |
| Song and Pan (2017) [40] | G1: 42.4 (7M, 12F) G2: 42.5 (7M, 13F) G3: 42.2 (8M, 12F) | G1: 19 G2: 20 G3: 20 | G1: Warm needling moxibustion G2: Warm needling moxibustion and Mulligan dynamic joint mobilization G3: Warm needling moxibustion and cervical traction | ROM VAS | Warm needling moxibustion plus Mulligan dynamic joint mobilization can effectively improve neck ROM and relieve pain in patients with cervical radiculopathy. |
| Rodríguez-Sanz et al. (2017) [41] | G1: 33.3 (14M, 11F) G2: 32.5 (12M, 15F) | G1: 25 G2: 27 | G1: Cervical lateral glide G2: Waiting list (without intervention) | NPRS QuickDASH Ipsilateral cervical rotation | Cervical lateral glide is superior to the absence of treatment in reducing pain and increasing the affected upper limb function of participants who suffer from cervicobrachial pain. |
| Cui et al. (2017) [42] | G1: 44.1 (45M, 128F) G2: 44.4 (35M, 141F) | G1: 173 G2: 176 | G1: Shi-style cervical manipulations G2: Mechanical cervical traction | NDI VAS SF-36 | Shi-style cervical manipulations could be a better option than mechanical cervical traction for the treatment of cervical radiculopathy-related pain and disability. |
| Kim et al. (2017) [43] | G1: 29.3 (5M, 10F) G2: 29.3 (6M, 9F) | G1: 15 G2: 15 | G1: Manual cervical traction G2: Manual cervical traction and neural mobilization | NPRS NDI ROM Cranio-Cervical Flexion Test | These results suggest that the neural mobilization can contribute to pain relief, recovery from neck disability, ROM, and deep flexor endurance for patients with cervical radiculopathy. |
| Khan et al. (2017) [44] | G1: 43.1 (16M, 4F) G2: 48.8 (16M, 4F) | G1: 20 G2: 20 | G1: Intermittent cervical traction in sitting position, TENS, hot pack G2: Intermittent cervical traction in supine position, TENS, hot pack | NDI | Supine position is a better choice for applying cervical traction as compared to sitting position for the management of cervical radiculopathy when comparing post interventional NDI score |
| Savva et al. (2016) [45] | G1: 45.2 (8M, 13F) G2: 49.2 (8M, 13F) | G1: 21 G2: 21 | G1: Neural mobilization and intermittent cervical traction G2: Participants did not receive any type of treatment | NPRS PSFS NDI Grip strength ROM | Neural mobilization with simultaneous intermittent cervical traction can improve pain, function, disability, grip strength and cervical range of motion in people with cervical radiculopathy. |
| Khan et al. (2016) [46] | G1: 38.0 (25M, 25F) G2: 38.0 (25M, 25F) | G1: 50 G2: 50 | G1: Manual cervical traction and a combination of conventional exercises and modalities including TENS and superficial thermotherapy. G2: A combination of conventional exercises and modalities including TENS and superficial thermotherapy. | VAS | Manual cervical traction when used with conventional exercises and modalities was an effective method for decreasing pain in cervical radiculopathy. |
| Waqas et al. (2016) [47] | G1: 47.0 (29M, 21F) G2: 47.0 (34M, 16F) | G1: 50 G2: 50 | G1: Maitland Thoracic spine manipulation G2: Maitland cervical spine mobilization | NPRS NDI | The result shows that Maitland Thoracic spine manipulation and Maitland cervical spine mobilization were effective techniques for pain reduction and functional abilities restoration. |
| Bukhari et al. (2016) [48] | G1: Not specified G2: Not specified | G1: 21 G2: 15 | G1: Segmental mobilization and exercise therapy and manual traction G2: Segmental mobilization and exercise therapy and mechanical traction | NPRS NDI | If cervical radiculopathy patients are treated with mechanical traction, segmental mobilization, and exercise therapy, pain and disability will be managed more effectively than when treated with manual traction, segmental mobilization, and exercise therapy. |
| Costello et al. (2016) [49] | G1: 46.2 (sex not specified) G2: 42.0 (sex not specified) | G1: 12 G2: 11 | G1: Soft tissue mobilization G2: Therapeutic Ultrasound | NDI GROC PSFS NPRS ROM | Patients with neck and arm pain demonstrated greater improvements in ROM, GROC, and PSFS, and pain following soft tissue mobilization than after receiving therapeutic ultrasounds. |
| Langevin et al. (2015) [50] | G1: 42.8 (6M, 12F) G2: 47.8 (6M, 12F) | G1: 18 G2: 18 | G1: Manual therapy and exercise program aimed at increasing the size of the intervertebral foramen G2: Manual therapy and exercise program without the specific goal of increasing the size of the intervertebral foramen | NDI QuickDASH NPRS | Results suggest that manual therapy and exercises are effective in reducing pain and functional limitations related to CR. The addition of techniques thought to increase the size of the intervertebral foramen of the affected nerve root yielded no significant additional benefits. |
| Fritz et al. (2014) [51] | G1: 44.9 (10M, 18F) G2: 48.1 (18M,13F) G3: 47.6 (12M, 15F) | G1: 28 G2: 31 G3: 27 | G1: Exercise alone G2: Exercise and mechanical traction G3: Exercise and over-door traction | NDI VAS | Adding mechanical traction to exercise for patients with cervical radiculopathy resulted in lower disability and pain, particularly at long-term follow-ups. |
| Jellad et al. (2009) [52] | G1: 38.5 (4M, 9F) G2: 44.2 (3M,10F) G3: 41.3 (2M, 11F) | G1: 13 G2: 13 G3: 13 | G1: Conventional rehabilitation with intermittent manual traction G2: Conventional rehabilitation with intermittent mechanical traction G3: Conventional rehabilitation alone | VAS | Manual or mechanical cervical traction appears to be a major contribution in the rehabilitation of cervical radiculopathy particularly if it is included in a multimodal approach to rehabilitation. |
| Young et al. (2009) [53] | G1: 47.8 (14M, 31F) G2: 46.2 (12M, 24F) | G1: 45 G2: 36 | G1: Manual therapy, exercise, and intermittent cervical traction G2: Manual therapy, exercise, and sham intermittent cervical traction | NDI NPRS PSFS | The results suggest that the addition of mechanical cervical traction to a multimodal treatment program of manual therapy and exercise yields no significant additional benefit to pain, function, or disability in patients with cervical radiculopathy. |
| Joghataei et al. (2004) [54] | G1: 47.5 (8M, 7F) G2: 46.3 (7M, 8F) | G1: 15 G2: 15 | G1: Cervical traction and electrotherapy/exercise G2: Electrotherapy/exercise treatment | Grip strength | The application of cervical traction combined with electrotherapy and exercise produced an immediate improvement in the hand grip function in patients with cervical radiculopathy. |
| Lumbar radiculopathy | |||||
| Plaza-Manzano et al. (2019) [55] | G1: 47.0 (8M,8F) G2: 45.5 (8M, 8F) | G1: 16 G2: 16 | G1: Neurodynamic mobilization plus motor control exercises G2: Motor control exercises | NPRS PLE PPT RMQ | The addition of neurodynamic mobilization to a motor control exercise program led to reductions in neuropathic symptoms and mechanical sensitivity, but did not result in greater changes of pain. |
| Satpute et al. (2018) [56] | G1: 49.9 (14M, 16F) G2: 42.3 (20M, 10F) | G1: 30 G2: 30 | G1: Spinal mobilization with leg movement, exercise and electrotherapy G2: Exercise and electrotherapy alone | VAS ODI GROC SLR ROM | In patients with lumbar radiculopathy, the addition of spinal mobilization with leg movement, exercise and electrotherapy provided significantly improved benefits in leg and back pain, disability, SLR ROM, and patient satisfaction in the short and long term. |
| Tambekar et al. (2015) [57] | G1: 34.1 (8M, 8F) G2: 32.3 (7M, 8F) | G1: 16 G2: 15 | G1: Mulligan bent leg raise G2: Butler’s neural tissue mobilization | VAS SLR ROM | The study showed that both techniques produce immediate improvement in pain and SLR range, but this effect was not maintained during the follow up period. |
| Moustafa et al. (2013) [58] | G1: 43.9 (19M, 13F) G2: 43.2 (17M, 15F) | G1: 32 G2: 32 | G1: Lumbar extension traction in addition to hot packs and interferential therapy G2: Hot packs and interferential therapy | Lumbar lordotic angle NPRS ODI Modified Schober test EMG | The traction group receiving lumbar extension traction in addition to hot packs and interferential therapy experienced better effects than the control group with regard to pain, disability, H-reflex parameters and segmental intervertebral movements. |
| McMorland et al. (2010) [59] | G1: 41.5 (6M, 7F) G2: 42.4 (2M, 9F) | G1: 13 G2: 11 | G1: Microdiscectomy G2: Spinal manipulation | MGP RMQ SF-36 | Sixty percent of patients with sciatica who had failed other medical management benefited from spinal manipulation to the same degree as if they underwent surgical intervention. Of 40% left unsatisfied, subsequent surgical intervention confers excellent outcome. Patients with symptomatic LDH failing medical management should consider spinal manipulation followed by surgery if warranted. |
| Gudavalli et al. (2006) [60] | G1: 42.2 (81M, 42F) G2: 40.9 (66M, 46F) | G1: 123 G2: 112 | G1: Flexion-distraction G2: Active trunk exercise program | VAS RMQ SF-36 | Subgroup analysis indicated that subjects categorized as chronic, with moderate to severe symptoms, and those with radiculopathy, improved most with flexion-distraction. Subjects categorized with recurrent pain and moderate to severe symptoms improved most with an active trunk exercise program. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuligowski, T.; Skrzek, A.; Cieślik, B. Manual Therapy in Cervical and Lumbar Radiculopathy: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2021, 18, 6176. https://doi.org/10.3390/ijerph18116176
Kuligowski T, Skrzek A, Cieślik B. Manual Therapy in Cervical and Lumbar Radiculopathy: A Systematic Review of the Literature. International Journal of Environmental Research and Public Health. 2021; 18(11):6176. https://doi.org/10.3390/ijerph18116176
Chicago/Turabian StyleKuligowski, Tomasz, Anna Skrzek, and Błażej Cieślik. 2021. "Manual Therapy in Cervical and Lumbar Radiculopathy: A Systematic Review of the Literature" International Journal of Environmental Research and Public Health 18, no. 11: 6176. https://doi.org/10.3390/ijerph18116176
APA StyleKuligowski, T., Skrzek, A., & Cieślik, B. (2021). Manual Therapy in Cervical and Lumbar Radiculopathy: A Systematic Review of the Literature. International Journal of Environmental Research and Public Health, 18(11), 6176. https://doi.org/10.3390/ijerph18116176