
Physical Activity during COVID-19 Lockdown in Italy: A Systematic Review




Abstract
:1. Introduction
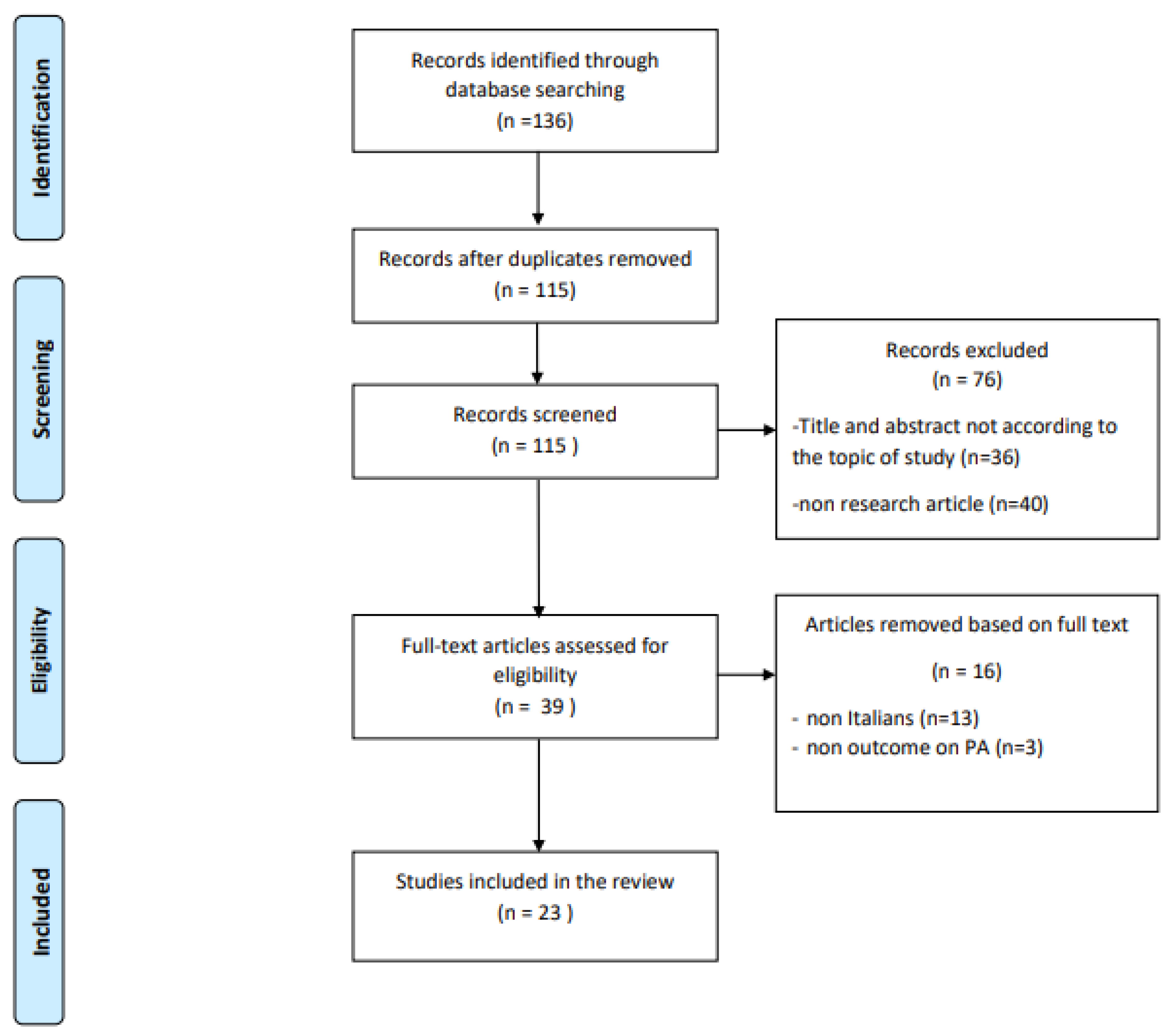
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bohn, B.; Herbst, A.; Pfeifer, M.; Krakow, D.; Zimny, S.; Kopp, F.; Melmer, A.; Steinacker, J.M.; Holl, R.W. DPV Initiative. Impact of Physical Activity on Glycemic Control and Prevalence of Cardiovascular Risk Factors in Adults With Type 1 Diabetes: A Cross-sectional Multicenter Study of 18,028 Patients. Diabetes Care. 2015, 38, 1536–1543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riddell, M.C.; Gallen, I.W.; Smart, C.E.; Taplin, C.E.; Adolfsson, P.; Lumb, A.N.; Kowalski, A.; Rabasa-Lhoret, R.; McCrimmon, R.J.; Hume, C.; et al. Exercise management in type 1 diabetes: A consensus statement. Lancet Diabetes Endocrinol. 2017, 5, 377–390. [Google Scholar] [CrossRef] [Green Version]
- Gielen, S.; Laughlin, M.H.; O’Conner, C.; Duncker, D.J. Exercise training in patients with heart disease: Review of beneficial effects and clinical recommendations. Prog. Cardiovasc. Dis. 2015, 57, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Ai, D.; Zhang, N. Exercise Benefits Coronary Heart Disease. Adv. Exp. Med. Biol. 2017, 1000, 3–7. [Google Scholar] [PubMed]
- Anziska, Y.; Inan, S. Exercise in neuromuscular disease. Semin. Neurol. 2014, 34, 542–556. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.L.; Lee, M.; Huang, T.T. Effectiveness of physical activity on patients with depression and Parkinson’s disease: A systematic review. PLoS ONE 2017, 27, e0181515. [Google Scholar] [CrossRef] [Green Version]
- Lauzé, M.; Daneault, J.F.; Duval, C. The Effects of Physical Activity in Parkinson’s Disease: A Review. J. Parkinsons Dis. 2016, 19, 685–698. [Google Scholar] [CrossRef] [Green Version]
- Duggal, N.A.; Niemiro, G.; Harridge, S.; Simpson, R.J.; Lord, J.M. Can physical activity ameliorate immunosenescence and thereby reduce age-related multi-morbidity? Nat. Rev. Immunol. 2019, 19, 563–572. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Non Randomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2009. [Google Scholar]
- Modesti, P.A.; Reboldi, G.; Cappuccio, F.P.; Agyemang, C.; Remuzzi, G.; Rapi, S.; Perruolo, E.; Parati, G.; ESH Working Group on CV Risk in Low Resource Settings. Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0147601. [Google Scholar] [CrossRef] [Green Version]
- Assaloni, R.; Pellino, V.C.; Puci, M.V.; Ferraro, O.E.; Lovecchio, N.; Girelli, A.; Vandoni, M. Coronavirus disease (Covid-19): How does the exercise practice in active people with type 1 diabetes change? A preliminary survey. Diabetes Res. Clin. Pract. 2020, 166, 108297. [Google Scholar] [CrossRef] [PubMed]
- Barchetta, I.; Cimini, F.A.; Bertoccini, L.; Ceccarelli, V.; Spaccarotella, M.; Baroni, M.G.; Cavallo, M.G. Effects of work status changes and perceived stress on glycaemic control in individuals with type 1 diabetes during COVID-19 lockdown in Italy. Diabetes Res. Clin. Pract. 2020, 170, 108513. [Google Scholar] [CrossRef] [PubMed]
- Capaldo, B.; Annuzzi, G.; Creanza, A.; Giglio, C.; De Angelis, R.; Lupoli, R.; Masulli, M.; Riccardi, G.; Rivellese, A.A.; Bozzetto, L. Blood Glucose Control During Lockdown for COVID-19: CGM Metrics in Italian Adults With Type 1 Diabetes. Diabetes Care 2020, 43, e88–e89. [Google Scholar] [CrossRef]
- Caruso, I.; Di Molfetta, S.; Guarini, F.; Giordano, F.; Cignarelli, A.; Natalicchio, A.; Perrini, S.; Leonardini, A.; Giorgino, F.; Laviola, L. Reduction of hypoglycaemia, lifestyle modifications and psychological distress during lockdown following SARS-CoV-2 outbreak in type 1 diabetes. Diabetes Metab. Res. Rev. 2020, e3404. [Google Scholar] [CrossRef] [PubMed]
- Predieri, B.; Leo, F.; Candia, F.; Lucaccioni, L.; Madeo, S.F.; Pugliese, M.; Vivaccia, V.; Bruzzi, P.; Iughetti, L. Glycemic Control Improvement in Italian Children and Adolescents With Type 1 Diabetes Followed Through Telemedicine During Lockdown Due to the COVID-19 Pandemic. Front. Endocrinol. 2020, 11, 595735. [Google Scholar] [CrossRef] [PubMed]
- Tornese, G.; Ceconi, V.; Monasta, L.; Carletti, C.; Faleschini, E.; Barbi, E. Glycemic Control in Type 1 Diabetes Mellitus During COVID-19 Quarantine and the Role of In-Home Physical Activity. Diabetes Technol Ther. 2020, 22, 462–467. [Google Scholar] [CrossRef]
- Di Stefano, V.; Battaglia, G.; Giustino, V.; Gagliardo, A.; D’Aleo, M.; Giannini, O.; Palma, A.; Brighina, F. Significant reduction of physical activity in patients with neuromuscular disease during COVID-19 pandemic: The long-term consequences of quarantine. J. Neurol. 2021, 268, 20–26. [Google Scholar] [CrossRef]
- Pellegrini, M.; Ponzo, V.; Rosato, R.; Scumaci, E.; Goitre, I.; Benso, A.; Belcastro, S.; Crespi, C.; De Michieli, F.; Ghigo, E.; et al. Changes in weight and nutritional habits in adults with obesity during the “lockdown” period caused by the COVID-19 virus emergency. Nutrients 2020, 12, 2016. [Google Scholar] [CrossRef]
- Sassone, B.; Mandini, S.; Grazzi, G.; Mazzoni, G.; Myers, J.; Pasanisi, G. Impact of COVID-19 Pandemic on Physical Activity in Patients With Implantable Cardioverter-Defibrillators. J. Cardiopulm. Rehabil. Prev. 2020, 40, 285–286. [Google Scholar] [CrossRef]
- Schirinzi, T.; Di Lazzaro, G.; Salimei, C.; Cerroni, R.; Liguori, C.; Scalise, S.; Alwardat, M.; Mercuri, N.B.; Pierantozzi, M.; Stefani, A.; et al. Physical activity changes and correlate effects in patients with Parkinson’s disease during COVID-19 lockdown. Mov. Disord. Clin. Pract. 2020, 7, 797–802. [Google Scholar] [CrossRef]
- Barrea, L.; Pugliese, G.; Framondi, L.; Di Matteo, R.; Laudisio, D.; Savastano, S.; Colao, A.; Muscogiuri, G. Does Sars-Cov-2 threaten our dreams? Effect of quarantine on sleep quality and body mass index. J. Transl. Med. 2020, 18, 318. [Google Scholar] [CrossRef]
- Buoite Stella, A.; AjČeviĆ, M.; Furlanis, G.; Cillotto, T.; Menichelli, A.; Accardo, A.; Manganotti, P. Smart technology for physical activity and health assessment during COVID-19 lockdown. J. Sports Med. Phys. Fitness. 2021, 61, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Cancello, R.; Soranna, D.; Zambra, G.; Zambon, A.; Invitti, C. Determinants of the Lifestyle Changes during COVID-19 Pandemic in the Residents of Northern Italy. Int J. Environ. Res. Public Health 2020, 17, 6287. [Google Scholar] [CrossRef] [PubMed]
- Di Corrado, D.; Magnano, P.; Muzii, B.; Coco, M.; Guarnera, M.; De Lucia, S.; Maldonato, N.M. Effects of social distancing on psychological state and physical activity routines during the COVID-19 pandemic. Sport Sci. Health 2020, 1–6. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl Med. 2020, 18, 229. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, G.; Camussi, E.; Piccinelli, C.; Senore, C.; Armaroli, P.; Ortale, A.; Garena, F.; Giordano, L. Did social isolation during the SARS-CoV-2 epidemic have an impact on the lifestyles of citizens?. L’isolamento sociale durante l’epidemia da SARS-CoV-2 ha avuto un impatto sugli stili di vita dei cittadini? Epidemiol. Prev. 2020, 44 (Suppl. S2), 353–362. [Google Scholar] [PubMed]
- Gallè, F.; Sabella, E.A.; Da Molin, G.; De Giglio, O.; Caggiano, G.; Di Onofrio, V.; Ferracuti, S.; Montagna, M.T.; Liguori, G.; Orsi, G.B.; et al. Understanding Knowledge and Behaviors Related to CoViD-19 Epidemic in Italian Undergraduate Students: The EPICO Study. Int J. Environ. Res. Public Health 2020, 17, 3481. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.A.; Ferracuti, S.; De Giglio, O.; Caggiano, G.; Protano, C.; Valeriani, F.; Parisi, E.A.; Valerio, G.; Liguori, G.; et al. Sedentary Behaviors and Physical Activity of Italian Undergraduate Students during Lockdown at the Time of CoViD-19 Pandemic. Int J. Environ. Res. Public Health 2020, 17, 6171. [Google Scholar] [CrossRef]
- Giustino, V.; Parroco, A.M.; Gennaro, A.; Musumeci, G.; Palma, A.; Battaglia, G. Physical activity levels and related energy expenditure during COVID-19 quarantine among the sicilian active population: A cross-sectional online survey study. Sustainability 2020, 12, 4356. [Google Scholar] [CrossRef]
- Luciano, F.; Cenacchi, V.; Vegro, V.; Pavei, G. COVID-19 lockdown: Physical activity, sedentary behaviour and sleep in Italian medicine students. Eur. J. Sport Sci. 2020, 1–10. [Google Scholar] [CrossRef]
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during Covid-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef]
- Raiola, G.; Aliberti, S.; Esposito, G.; Altavilla, G.; D’Isanto, T.; D’Elia, F. How has the practice of physical activity changed during the covid-19 quarantine? a preliminary survey. Teor. Metod. Fiz. Vihov. 2020, 20, 242–247. [Google Scholar] [CrossRef]
- Tornaghi, M.; Lovecchio, N.; Vandoni, M.; Chirico, A.; Codella, R. Physical activity levels across COVID-19 outbreak in youngsters of Northwestern Lombardy. J. Sports Med. Phys. Fitness 2020. [Google Scholar] [CrossRef]
- Chirico, A.; Lucidi, F.; Galli, F.; Giancamilli, F.; Vitale, J.; Borghi, S.; La Torre, A.; Codella, R. COVID-19 Outbreak and Physical Activity in the Italian Population: A Cross-Sectional Analysis of the Underlying Psychosocial Mechanisms. Front. Psychol. 2020, 11, 2100. [Google Scholar] [CrossRef]
- Hart, P.H.; Gorman, S.; Finlay-Jones, J.J. Modulation of the immune system by UV radiation: More than just the effects of vitamin D? Nat. Rev. Immunol. 2011, 19, 584–596. [Google Scholar] [CrossRef] [PubMed]
- Dewan, S.K.; Zheng, S.B.; Xia, S.J.; Bill, K. Senescent remodeling of the immune system and its contribution to the predisposition of the elderly to infections. Chin. Med. J. 2012, 125, 3325–3331. [Google Scholar] [PubMed]
- Simpson, R.J.; Lowder, T.W.; Spielmann, G.; Bigley, A.B.; LaVoy, E.C.; Kunz, H. Exercise and the aging immune system. Ageing Res. Rev. 2012, 11, 404–420. [Google Scholar] [CrossRef]
- Sharif, K.; Watad, A.; Bragazzi, N.L.; Lichtbroun, M.; Amital, H.; Shoenfeld, Y. Physical activity and autoimmune diseases: Get moving and manage the disease. Autoimmun. Rev. 2018, 17, 53–72. [Google Scholar] [CrossRef]


{kind=link}
| Samples with Pathologies | Focus | Study Design | Sample, Pathology, Size, Age, % Males | PA Assessment Tool Survey Type | Amount of PA (Mean ± SD) | Main Findings |
|---|---|---|---|---|---|---|
| Assaloni et al. [12] | PA level in diabetes | Observational, cross-sectional | N = 154 T1D 44.8 ± 12.5 y, 54.5% males | Godin Leisure Time Exercise Q. online survey | Before L: 66 ± 42 min During L: 38 ± 31 min | PA decreased with worst glycaemia |
| Barchetta et al. [13] | Glycemic control in diabetes | Observational, cross-sectional | N = 50 T1D, 40.7 ± 13.5 y, 62% males | Q not validated Online survey | NR | Reduction of blood glucose control and weekly PA |
| Capaldo et al. [14] | Glucose control in diabetes | Observational, cross-sectional | N = 207 T1D 38.4 ± 12.7 y, 53.6% males | Q not validated Online survey | NR | Increased glycemic control, more regular meals, reduced PA |
| Caruso et al. [15] | Glucose control in diabetes | Observational, cross-sectional | N = 48 T1D 42.4 ± 15.9 y, 52.1% males | Q not validated Phone interview | NR | Increased glycemic control, reduced PA |
| Predieri et al. [16] | Glycemic control in diabetes | Observational, longitudinal | N = 62 T1D 11.1 ± 4.4 y, 50% males | Q not validated telemedicine | Before L: 3.27 ± 2.82 h/w During L: 0.24 ± 0.59 h/w | Decreased PA, improved glycemic control |
| Tornese et al. [17] | Glycemic control in diabetes | Observational, cross-sectional | N = 13 T1D median age = 14.2 y, 61.5% males | Q not validated telemedicine | During L: 3.3 h/w | Regular PA at home improved glycemic control |
| Di Stefano et al. [18] | Levels of PA in neuromuscular diseases (NMD) | Observational, cross-sectional | N = 268, 149 NMD patients (57.3 ± 13.7 y, 62.4% males), 119 controls (56 ± 6.8 y, 62.2% males) | IPAQ-SF Phone interview | NMD Before L: 901.3 ± 1299.6 During L: 400.6 ± 1088.5 Controls Before L: 4506.5 ± 7600.1 During L: 2362.3 ± 4498.9 | Significantly decrease of PA in both groups |
| Pellegrini et al. [19] | Changes in weight and diet in obesity | Observational, cross-sectional | N = 150 obese, aged 47.9 ± 16.0, 22% males | Q not validated | Significant weight increase, reduction in PA | |
| Sassone et al. [20] | Changes in PA in patients with implantable Cardioverter-defibrillators | Observational, cross-sectional | N = 24 cardiac patients, 72 ± 10 y, 70.8% males | Accelerometric sensors- collected data | Before L: 1.6 ± 0.5 h/day During L: 1.2 ± 0.3 h/day | Significant reduction in PA |
| Schirinzi et al. [21] | Changes in PA in Parkinson disease | Observational, cross-sectional | N = 74 Parkinson disease 61.3 ± 9.3 y, 50% males | IPAQ-SF Online survey | During L: 1994.7 ± 1971 MET-min/w | 60% of patients worsened, performing less PA |
| Sample without pathologies | Focus | Study design | Sample size, age, % males | PA assessment tool Survey type | Amount of PA (mean ± SD) | Main findings |
| Barrea et al. [22] | Sleep quality, Body mass index | Observational, cross-sectional | N = 121 44.9 ± 13.3 y, 35.5% males | Q not validated phone interview | NR | Significant increase in mean body weight and BMI, significant decrease in PA |
| Buoite Stella et al. [23] | Smart technologies for PA | Observational, cross-sectional | N = 400 35 ± 15 y, 31% males | Online survey IPAQ-SF; daily step count measured by smart devices | Before L: 3101 ± 3815 METs During L: 1839 ± 2254 METs | Significant reduction of performed steps and PA |
| Cancello et al. [24] | Lifestyle changes during lockdown | Observational, cross-sectional | N = 490 adults 16% males | Q not validated online survey | NR | Reduction of PA in active individuals, inception of PA in sedentary individuals |
| Di Corrado et al. [25] | Psychological status, PA | Observational, cross-sectional | N = 679 33.4 ± 12.8 y, 51% males | Q not validated Online survey | NR | Maintained or increased PA significantly |
| Di Renzo et al. [26] | Eating habits and lifestyle changes | Observational, cross-sectional | N = 3533 aged 12–86 23.9% males | Q not validated Online survey | NR | No significant difference in PA among inactive subjects, increase in PA in subjects who used to train more than 5 times a week |
| Ferrante et al. [27] | Impact of social isolation on lifestyle | Observational, cross-sectional | N = 7847 48.6 ± 13.9 y, 28.7% males | Q not validated Online survey | NR | Significant decrease in PA |
| Gallè et al. [28] | Sedentary behaviors and PA | Observational, cross-sectional | N = 1430 undergraduate students, 22.9 ± 4.5 y, 34.5% males | IPAQ-SF Online survey | Before L: 520 ± 820 min/w During L: 270 ± 340 min/w | Significantly increased sedentary lifestyle, decreased PA |
| Gallè et al. [29] | Health-related behaviors PA | Observational, cross-sectional | N = 2125 undergraduate students, 22.5 ± 0.08 y, 37.2% males | Questionnaire online survey | NR | Significant reduction in PA |
| Giustino et al. [30] | Level of PA | Observational, cross-sectional | N = 802, 32.27 ± 12.81 y, 49% males | IPAQ-SF online survey | Before L: 3006 MET-min/w During L: 1483.8 MET-min/w | Significant reduction of PA, especially in males and in overweight |
| Luciano et al. [31] | Behaviors during lockdown (PA, sedentariness, sleep) | Observational, cross-sectional | N = 1471 medicine students 23 ± 2 y, 30% males | IPAQ-SF online survey | Before L: 1588 MET-min/w During L: 960 MET-min/w | Decreased PA, and increased sitting and sleep time |
| Maugeri et al. [32] | PA on psychological | Observational, cross-sectional | N = 2524 43.6% males | IPAQ Online survey | Before L: 2429 MET-min/w During L: 1577 MET-min/w | PA level decreased with negative impact on psychological health |
| Raiola et al. [33] | Changes in PA | Observational, cross-sectional | N = 268 Mean age = 26 y | Q not validated Online survey | NR | No change in PA |
| Tornaghi et al. [34] | PA levels | Observational, cross-sectional | N = 1568 students Aged 15–18 | IPAQ Online survey | Before L: 1676.37 ± 20.6 MET-min/w After L: 1774.50 ± 33.93 MET-min/w | Inactive or moderately active students unchanged their PA level; highly active ones increased PA level |
| REFERENCE | Representativeness of Sample | Sample Size | Non-Respondents | Ascertainment of the Exposure | Comparability | Assessment of the Outcome | Statistics | NOS Score |
|---|---|---|---|---|---|---|---|---|
| Assaloni et al. [12] | 1 | 0 | 0 | 2 | 0 | 1 | 1 | 6 |
| Barchetta et al. [13] | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 4 |
| Barrea et al. [22] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 5 |
| Buoite Stella et al. [23] | 1 | 0 | 0 | 2 | 0 | 1 | 1 | 5 |
| Cancello et al. [24] | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 4 |
| Capaldo et al. [14] | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 2 |
| Caruso et al. [15] | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 3 |
| Di Corrado et al. [25] | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 3 |
| Di Renzo et al. [26] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Di Stefano et al. [18] | 1 | 0 | 0 | 2 | 1 | 1 | 1 | 6 |
| Ferrante et al. [27] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 8 |
| Gallè et al. [28] | 1 | 1 | 0 | 2 | 0 | 1 | 1 | 6 |
| Gallè et al. [29] | 1 | 1 | 0 | 2 | 0 | 1 | 1 | 6 |
| Giustino et al. [30] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 5 |
| Luciano et al. [31] | 1 | 1 | 0 | 2 | 0 | 1 | 1 | 6 |
| Maugeri et al. [32] | 1 | 0 | 0 | 2 | 0 | 1 | 1 | 5 |
| Pellegrini et al. [19] | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 4 |
| Predieri et al. [16] | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 4 |
| Raiola et al. [33] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 5 |
| Sassone et al. [20] | 1 | 0 | 0 | 2 | 0 | 2 | 1 | 6 |
| Schirinzi et al. [21] | 1 | 0 | 0 | 2 | 0 | 1 | 1 | 5 |
| Tornaghi et al. [34] | 1 | 0 | 0 | 2 | 1 | 1 | 1 | 6 |
| Tornese et al. [17] | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaccagni, L.; Toselli, S.; Barbieri, D. Physical Activity during COVID-19 Lockdown in Italy: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6416. https://doi.org/10.3390/ijerph18126416
Zaccagni L, Toselli S, Barbieri D. Physical Activity during COVID-19 Lockdown in Italy: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(12):6416. https://doi.org/10.3390/ijerph18126416
Chicago/Turabian StyleZaccagni, Luciana, Stefania Toselli, and Davide Barbieri. 2021. "Physical Activity during COVID-19 Lockdown in Italy: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 12: 6416. https://doi.org/10.3390/ijerph18126416
APA StyleZaccagni, L., Toselli, S., & Barbieri, D. (2021). Physical Activity during COVID-19 Lockdown in Italy: A Systematic Review. International Journal of Environmental Research and Public Health, 18(12), 6416. https://doi.org/10.3390/ijerph18126416