
Comprehensive Analysis of Risk Factors for Periodontitis Focusing on the Saliva Microbiome and Polymorphism

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethical Procedures and Informed Consent
2.3. Oral Examinations
2.4. Questionnaires
- Have you felt stress during the past year? (Severe/Moderate/Mild/None)
- Are you a smoker? (Yes/Past/No)
- Do you take at least one medication per week to lower blood sugar levels? (Yes/No)
2.5. Salivary Microbiome Analysis
2.6. Genotyping
2.7. Assessment of Other Factors
2.8. Statistical Analysis
2.9. Data Availability
3. Results
3.1. Participants’ Characteristics
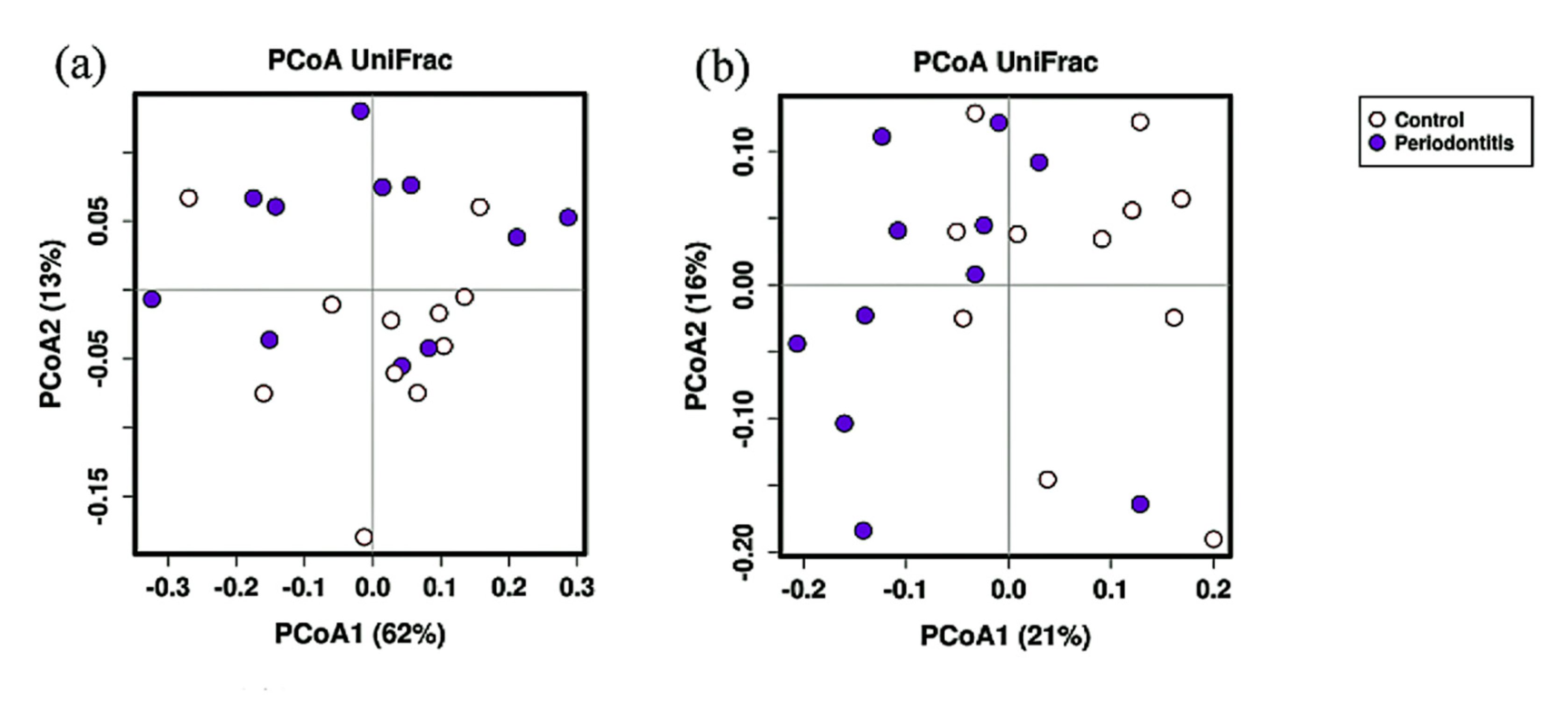
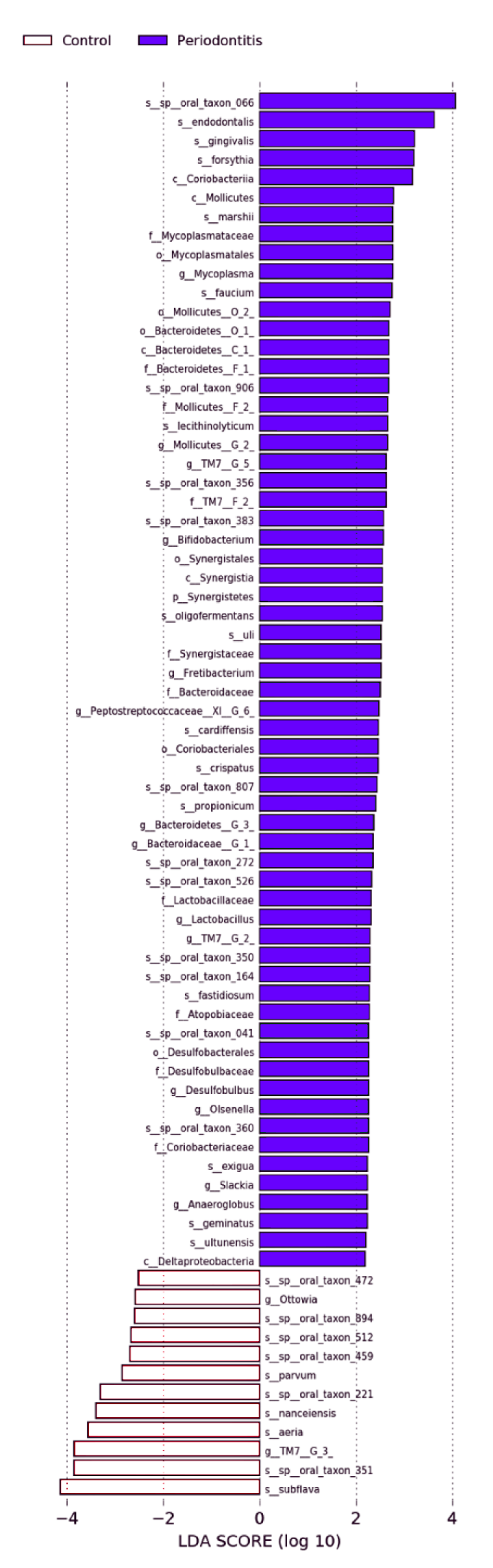
3.2. Salivary Microbiome Analysis
3.3. Genotyping
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Petersen, P.E. The World Oral Health Report 2003: Continuous Improvement of Oral Health in the 21st Century—The Approach of the WHO Global Oral Health Programme. Commun. Dent. Oral Epidemiol. 2003, 31, 3–24. [Google Scholar] [CrossRef] [PubMed]
- JSP Clinical Practice Guideline for the Periodontal Treatment. 2015. Available online: file:///C:/Users/Toyama/Zotero/storage/9KLV5QTF/guideline_perio_plan2015.pdf (accessed on 8 June 2020).
- Vieira Colombo, A.P.; Magalhães, C.B.; Hartenbach, F.A.R.R.; Martins do Souto, R.; Maciel da Silva-Boghossian, C. Periodontal-Disease-Associated Biofilm: A Reservoir for Pathogens of Medical Importance. Microb. Pathog. 2016, 94, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal Diseases. Nat. Rev. Dis. Primers 2017, 3, 1–14. [Google Scholar] [CrossRef]
- Marsh, P.D.; Moter, A.; Devine, D.A. Dental Plaque Biofilms: Communities, Conflict and Control. Periodontology 2000 2011, 55, 16–35. [Google Scholar] [CrossRef]
- Guerra, F.; Mazur, M.; Ndokaj, A.; Corridore, D.; La Torre, G.; Polimeni, A.; Ottolenghi, L. Periodontitis and the Microbiome: A Systematic Review and Meta-Analysis. Minerva Stomatol. 2018, 67, 250–258. [Google Scholar] [CrossRef]
- Munz, M.; Richter, G.M.; Loos, B.G.; Jepsen, S.; Divaris, K.; Offenbacher, S.; Teumer, A.; Holtfreter, B.; Kocher, T.; Bruckmann, C.; et al. Meta-Analysis of Genome-Wide Association Studies of Aggressive and Chronic Periodontitis Identifies Two Novel Risk Loci. Eur. J. Hum. Genet. 2019, 27, 102–113. [Google Scholar] [CrossRef] [Green Version]
- Shastry, B.S. SNPs: Impact on Gene Function and Phenotype. In Single Nucleotide Polymorphisms: Methods and Protocols; Komar, A.A., Ed.; Methods in Molecular BiologyTM; Humana Press: Totowa, NJ, USA, 2009; pp. 3–22. ISBN 978-1-60327-411-1. [Google Scholar]
- 16S Metagenomic Sequencing Library Preparation. Available online: https://support.illumina.com/documents/documentation/chemistry_documentation/16s/16s-metagenomic-library-prep-guide-15044223-b.pdf (accessed on 8 June 2020).
- Edgar, R.C. UPARSE: Highly Accurate OTU Sequences from Microbial Amplicon Reads. Nat. Methods 2013, 10, 996–998. [Google Scholar] [CrossRef]
- Edgar, R.C. Search and Clustering Orders of Magnitude Faster than BLAST. Bioinformatics 2010, 26, 2460–2461. [Google Scholar] [CrossRef] [Green Version]
- Koyama, T.; Kuriyama, N.; Ozaki, E.; Matsui, D.; Watanabe, I.; Takeshita, W.; Iwai, K.; Watanabe, Y.; Nakatochi, M.; Shimanoe, C.; et al. Genetic Variants of RAMP2 and CLR Are Associated with Stroke. J. Atheroscler. Thromb. 2017, 24, 1267–1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delaneau, O.; Marchini, J.; Zagury, J.-F. A Linear Complexity Phasing Method for Thousands of Genomes. Nat. Methods 2012, 9, 179–181. [Google Scholar] [CrossRef]
- Das, S.; Forer, L.; Schönherr, S.; Sidore, C.; Locke, A.E.; Kwong, A.; Vrieze, S.I.; Chew, E.Y.; Levy, S.; McGue, M.; et al. Next-Generation Genotype Imputation Service and Methods. Nat. Genet. 2016, 48, 1284–1287. [Google Scholar] [CrossRef] [Green Version]
- Brodzikowska, A.; Górska, R.; Kowalski, J. Interleukin-1 Genotype in Periodontitis. Arch. Immunol. Ther. Exp. 2019, 67, 367–373. [Google Scholar] [CrossRef] [Green Version]
- Lin, W.; Xu, H.; Wu, Y.; Wang, J.; Yuan, Q. In Silico Genome-Wide Identification of M6A-Associated SNPs as Potential Functional Variants for Periodontitis. J. Cell. Physiol. 2020, 235, 900–908. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.; Liu, F.; Pan, Y.; Jin, X.; Wang, H.; Cao, J. BsmI, TaqI, ApaI, and FokI Polymorphisms in the Vitamin D Receptor Gene and Periodontitis: A Meta-Analysis of 15 Studies Including 1338 Cases and 1302 Controls. J. Clin. Periodontol. 2011, 38, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, A.S.; Bochenek, G.; Manke, T.; Nothnagel, M.; Graetz, C.; Thien, A.; Jockel-Schneider, Y.; Harks, I.; Staufenbiel, I.; Wijmenga, C.; et al. Validation of Reported Genetic Risk Factors for Periodontitis in a Large-Scale Replication Study. J. Clin. Periodontol. 2013, 40, 563–572. [Google Scholar] [CrossRef]
- Taiete, T.; Casati, M.Z.; Stolf, C.S.; Corrêa, M.G.; Santamaria, M.P.; Andere, N.M.R.B.; Coletta, R.D.; Sallum, E.A.; Júnior, F.H.N.; Silvério, K.G.; et al. Validation of Reported GLT6D1 (Rs1537415), IL10 (Rs6667202), and ANRIL (Rs1333048) Single Nucleotide Polymorphisms for Aggressive Periodontitis in a Brazilian Population. J. Periodontol. 2019, 90, 44–51. [Google Scholar] [CrossRef] [Green Version]
- Leite, F.R.M.; Enevold, C.; Bendtzen, K.; Baelum, V.; López, R. Pattern Recognition Receptor Polymorphisms in Early Periodontitis. J. Periodontol. 2019, 90, 647–654. [Google Scholar] [CrossRef]
- Marchesan, J.T.; Jiao, Y.; Moss, K.; Divaris, K.; Seaman, W.; Webster-Cyriaque, J.; Zhang, S.; Yu, N.; Song, C.; Bencharit, S.; et al. Common Polymorphisms in IFI16 and AIM2 Genes Are Associated With Periodontal Disease. J. Periodontol. 2017, 88, 663–672. [Google Scholar] [CrossRef] [PubMed]
- Zupin, L.; Robino, A.; Navarra, C.O.; Pirastu, N.; Lenarda, R.D.; Gasparini, P.; Crovella, S.; Bevilacqua, L. LTF and DEFB1 Polymorphisms Are Associated with Susceptibility toward Chronic Periodontitis Development. Oral Dis. 2017, 23, 1001–1008. [Google Scholar] [CrossRef]
- Fernandez, R.; Tufanaru, C. Understanding Propensity Scores. Int. J. Evid. Based Healthc. 2017, 15, 142–143. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.-R.; Shin, J.; Guevarra, R.B.; Lee, J.H.; Kim, D.W.; Seol, K.-H.; Lee, J.-H.; Kim, H.B.; Isaacson, R.E. Deciphering Diversity Indices for a Better Understanding of Microbial Communities. J. Microbiol. Biotechnol. 2017, 27, 2089–2093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodrich, J.K.; Di Rienzi, S.C.; Poole, A.C.; Koren, O.; Walters, W.A.; Caporaso, J.G.; Knight, R.; Ley, R.E. Conducting a Microbiome Study. Cell 2014, 158, 250–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Bittinger, K.; Charlson, E.S.; Hoffmann, C.; Lewis, J.; Wu, G.D.; Collman, R.G.; Bushman, F.D.; Li, H. Associating Microbiome Composition with Environmental Covariates Using Generalized UniFrac Distances. Bioinformatics 2012, 28, 2106–2113. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Damgaard, C.; Danielsen, A.K.; Enevold, C.; Massarenti, L.; Nielsen, C.H.; Holmstrup, P.; Belstrøm, D. Porphyromonas Gingivalis in Saliva Associates with Chronic and Aggressive Periodontitis. J. Oral Microbiol. 2019, 11, 1653123. [Google Scholar] [CrossRef] [Green Version]
- Spinler, J.K. Human Microbiome, Lactobacillaceae in the. In Encyclopedia of Metagenomics; Nelson, K.E., Ed.; Springer: New York, NY, USA, 2014; pp. 1–8. ISBN 978-1-4614-6418-1. [Google Scholar]
- van der Hoeven, J.S.; van den Kieboom, C.W.; Schaeken, M.J. Sulfate-Reducing Bacteria in the Periodontal Pocket. Oral Microbiol. Immunol. 1995, 10, 288–290. [Google Scholar] [CrossRef] [PubMed]
- Schulz, S.; Porsch, M.; Grosse, I.; Hoffmann, K.; Schaller, H.-G.; Reichert, S. Comparison of the Oral Microbiome of Patients with Generalized Aggressive Periodontitis and Periodontitis-Free Subjects. Arch. Oral Biol. 2019, 99, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Acharya, A.; Chen, T.; Chan, Y.; Watt, R.M.; Jin, L.; Mattheos, N. Species-Level Salivary Microbial Indicators of Well-Resolved Periodontitis: A Preliminary Investigation. Front. Cell. Infect. Microbiol. 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Takeshita, T.; Kageyama, S.; Furuta, M.; Tsuboi, H.; Takeuchi, K.; Shibata, Y.; Shimazaki, Y.; Akifusa, S.; Ninomiya, T.; Kiyohara, Y.; et al. Bacterial Diversity in Saliva and Oral Health-Related Conditions: The Hisayama Study. Sci. Rep. 2016, 6, 22164. [Google Scholar] [CrossRef] [Green Version]
- Takayasu, L.; Suda, W.; Takanashi, K.; Iioka, E.; Kurokawa, R.; Shindo, C.; Hattori, Y.; Yamashita, N.; Nishijima, S.; Oshima, K.; et al. Circadian Oscillations of Microbial and Functional Composition in the Human Salivary Microbiome. DNA Res. 2017, 24, 261–270. [Google Scholar] [CrossRef]
- Shimizu, S.; Nagasawa, T.; Furuichi, Y. A genome-wide association study of periodontitis. Nihon Shishubyo Gakkai Kaishi (J. Jpn. Soc. Periodontol.) 2019, 61, 127–135. [Google Scholar] [CrossRef]
- Cornejo Ulloa, P.; van der Veen, M.H.; Krom, B.P. Review: Modulation of the Oral Microbiome by the Host to Promote Ecological Balance. Odontology 2019, 107, 437–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Periodontal Disease Group | Control Group | p | ||
|---|---|---|---|---|
| N = 11 | N = 11 | |||
| Gender | Male | 6 (54.5) a | 5 (45.5) | 1.000 b |
| Female | 5 (45.5) | 6 (54.5) | ||
| Passive stress | Negative | 5 (45.5) | 2 (18.2) | 0.361 |
| Positive | 6 (54.5) | 9 (81.8) | ||
| Smoking status | No | 3 (27.3) | 7 (63.6) | 0.061 c |
| Past | 4 (36.4) | 4 (36.4) | ||
| Current | 4 (36.4) | 0 (0) | ||
| Diabetes | No | 9 (81.8) | 11 (100) | 0.333 |
| Past | 1 (9.1) | 0 (0) | ||
| Current | 1 (9.1) | 0 (0) | ||
| Age | 64.3 ± 7.6 d | 57.1 ± 11.0 | 0.091 e | |
| Body mass index | 23.9 ± 3.3 | 21.3 ± 2.7 | 0.051 | |
| Triglyceride (mg/dL) | 102.5 ± 34.7 | 89.2 ± 48.8 | 0.470 | |
| HbA1c (%) | 5.8 ± 0.3 | 5.0 ± 0.3 | 0.065 | |
| Blood glucose (mg/dL) | 100.8 ± 19.3 | 92.7 ± 13.0 | 0.263 |
| OTU | Periodontitis | Control | pa | qb | ||||
|---|---|---|---|---|---|---|---|---|
| Species | Median | 25th Percentiles | 75th Percentiles | Median | 25th Percentiles | 75th Percentiles | ||
| Actinomyces cardiffensis | 1.31 × 10−4 | 0 | 2.48 × 10−4 | 0 | 0 | 0 | 0.047 | 0.074 |
| Rothia aeria | 1.20 × 10−3 | 9.45 × 10−5 | 1.15 × 10−2 | 8.36 × 10−3 | 2.28 × 10−3 | 2.16 × 10−2 | 0.047 | 0.071 |
| Propionibacterium propionicum | 0 | 0 | 2.74 × 10−5 | 4.58 × 10−5 | 2.51 × 10−5 | 8.32 × 10−5 | 0.023 | 0.075 |
| Olsenella sp. oral taxon 807 | 4.87 × 10−5 | 0 | 1.29 × 10−4 | 0 | 0 | 0 | 0.065 | 0.087 |
| Olsenella uli | 5.47 × 10−5 | 0 | 1.31 × 10−4 | 0 | 0 | 2.13 × 10−5 | 0.040 | 0.076 |
| Slackia exigua | 2.25 × 10−4 | 2.75 × 10−5 | 6.58 × 10−4 | 3.02 × 10−5 | 0 | 5.12 × 10−5 | 0.040 | 0.072 |
| Bacteroidaceae [G-1] sp. oral taxon 272 | 3.56 × 10−4 | 2.19 × 10−5 | 7.54 × 10−4 | 2.48 × 10−5 | 0 | 1.07 × 10−4 | 0.047 | 0.068 |
| Porphyromonas endodontalis | 7.06 × 10−3 | 1.14 × 10−3 | 2.50 × 10−2 | 1.12 × 10−3 | 0 | 3.69 × 10−3 | 0.034 | 0.068 |
| Porphyromonas gingivalis | 6.61 × 10−4 | 4.96 × 10−4 | 2.79 × 10−3 | 0 | 0 | 0 | <0.001 | 0.007 |
| Tannerella forsythia | 1.73 × 10−3 | 1.05 × 10−3 | 8.62 × 10−3 | 4.29 × 10−4 | 4.22 × 10−5 | 1.29 × 10−3 | 0.028 | 0.072 |
| Prevotella marshii | 2.36 × 10−5 | 0 | 8.26 × 10−5 | 0 | 0 | 0 | 0.028 | 0.067 |
| Prevotella nanceiensis | 8.27 × 10−4 | 1.26 × 10−4 | 6.66 × 10−3 | 8.12 × 10−3 | 2.73 × 10−3 | 1.60 × 10−2 | 0.023 | 0.069 |
| Prevotella sp. oral taxon 472 | 0 | 0 | 2.75 × 10−5 | 1.02 × 10−4 | 6.45 × 10−5 | 1.49 × 10−4 | 0.007 | 0.084 |
| Prevotella sp. oral taxon 526 | 1.31 × 10−4 | 0 | 6.76 × 10−4 | 0 | 0 | 0 | 0.019 | 0.086 |
| Lactobacillus crispatus | 0 | 0 | 1.08 × 10−4 | 0 | 0 | 0 | 0.151 | 0.160 |
| Lactobacillus ultunensis | 5.90 × 10−5 | 0 | 1.44 × 10−4 | 0 | 0 | 0 | 0.065 | 0.084 |
| Streptococcus oligofermentans | 8.05 × 10−5 | 2.53 × 10−5 | 9.74 × 10−5 | 2.13 × 10−5 | 0 | 2.77 × 10−5 | 0.005 | 0.090 |
| Streptococcus sp. oral taxon 066 | 3.28 × 10−2 | 1.34 × 10−2 | 5.78 × 10−2 | 1.28 × 10−2 | 9.79 × 10−3 | 2.09 × 10−2 | 0.013 | 0.078 |
| Catonella sp. oral taxon 164 | 2.74 × 10−5 | 0 | 1.31 × 10−4 | 0 | 0 | 0 | 0.076 | 0.094 |
| Oribacterium parvum | 0 | 0 | 0 | 2.29 × 10−5 | 0 | 4.30 × 10−5 | 0.101 | 0.121 |
| Peptostreptococcaceae [XI][G-1] sp. oral taxon 383 | 0 | 0 | 7.18 × 10−5 | 0 | 0 | 0 | 0.151 | 0.151 |
| Mollicutes [G-2] sp. oral taxon 906 | 1.61 × 10−5 | 0 | 1.10 × 10−4 | 0 | 0 | 0 | 0.101 | 0.117 |
| Mycoplasma faucium | 6.68 × 10−4 | 0 | 1.26 × 10−3 | 0 | 0 | 2.15 × 10−5 | 0.013 | 0.067 |
| Anaeroglobus geminatus | 3.59 × 10−5 | 0 | 3.14 × 10−4 | 0 | 0 | 0 | 0.019 | 0.076 |
| Leptotrichia sp. oral taxon 221 | 4.87 × 10−5 | 0 | 7.67 × 10−4 | 7.46 × 10−4 | 1.37 × 10−4 | 5.99 × 10−3 | 0.040 | 0.069 |
| Ottowia sp. oral taxon 894 | 0 | 0 | 2.74 × 10−5 | 1.07 × 10−4 | 2.56 × 10−5 | 1.60 × 10−4 | 0.047 | 0.065 |
| Kingella sp. oral taxon 459 | 0 | 0 | 0 | 0 | 0 | 1.51 × 10−4 | 0.151 | 0.151 |
| Neisseria subflava | 1.89 × 10−4 | 1.61 × 10−5 | 3.02 × 10−3 | 5.72 × 10−2 | 2.60 × 10−2 | 7.43 × 10−2 | 0.008 | 0.058 |
| Desulfobulbus sp. oral taxon 041 | 5.51 × 10−5 | 0 | 2.51 × 10−4 | 0 | 0 | 0 | 0.028 | 0.063 |
| Aggregatibacter sp. oral taxon 512 | 2.36 × 10−5 | 0 | 1.45 × 10−4 | 1.54 × 10−4 | 2.51 × 10−5 | 1.26 × 10−3 | 0.040 | 0.065 |
| TM7 [G-2] sp. oral taxon 350 | 0 | 0 | 2.20 × 10−4 | 0 | 0 | 0 | 0.133 | 0.150 |
| TM7 [G-3] sp. oral taxon 351 | 1.04 × 10−2 | 2.38 × 10−3 | 1.90 × 10−2 | 2.18 × 10−2 | 1.36 × 10−2 | 3.79 × 10−2 | 0.023 | 0.064 |
| TM7 [G-5] sp. oral taxon 356 | 3.58 × 10−4 | 1.77 × 10−4 | 1.13 × 10−3 | 1.26 × 10−4 | 0 | 3.05 × 10−4 | 0.019 | 0.068 |
| Treponema lecithinolyticum | 0 | 0 | 1.09 × 10−4 | 0 | 0 | 0 | 0.133 | 0.145 |
| Fretibacterium fastidiosum | 8.75 × 10−5 | 4.87 × 10−5 | 1.89 × 10−4 | 1.79 × 10−5 | 0 | 6.04 × 10−5 | 0.028 | 0.059 |
| Fretibacterium sp. oral taxon 360 | 2.92 × 10−4 | 5.90 × 10−5 | 7.66 × 10−4 | 2.56 × 10−5 | 0 | 9.16 × 10−5 | 0.007 | 0.063 |
| Genus | ||||||||
| Bifidobacterium | 0 | 0 | 3.03 × 10−4 | 0 | 0 | 0 | 0.133 | 0.142 |
| Olsenella | 1.75 × 10−4 | 2.75 × 10−5 | 3.29 × 10−4 | 0 | 0 | 3.57 × 10−5 | 0.002 | 0.032 |
| Slackia | 2.25 × 10−4 | 2.75 × 10−5 | 6.58 × 10−4 | 3.02 × 10−5 | 0 | 5.12 × 10−5 | 0.040 | 0.058 |
| Bacteroidetes [G-3] | 2.87 × 10−4 | 4.38 × 10−5 | 1.02 × 10−3 | 0 | 0 | 1.83 × 10−4 | 0.034 | 0.060 |
| Bacteroidaceae [G-3] | 3.56 × 10−4 | 2.19 × 10−5 | 7.54 × 10−4 | 2.48 × 10−5 | 0 | 1.07 × 10−4 | 0.047 | 0.063 |
| Lactobacillus | 6.56 × 10−5 | 0 | 2.51 × 10−4 | 0 | 0 | 0 | 0.034 | 0.054 |
| Peptostreptococcaceae [XI][G-6] | 1.64 × 10−4 | 1.09 × 10−4 | 1.47 × 10−3 | 4.26 × 10−5 | 0 | 1.25 × 10−4 | 0.010 | 0.053 |
| Mollicutes [G-2] | 1.61 × 10−5 | 0 | 1.10 × 10−4 | 0 | 0 | 0 | 0.101 | 0.115 |
| Mycoplasma | 1.05 × 10−3 | 1.31 × 10−4 | 1.51 × 10−3 | 1.24 × 10−4 | 2.77 × 10−5 | 5.63 × 10−4 | 0.023 | 0.061 |
| Anaeroglobus | 3.59 × 10−5 | 0 | 3.14 × 10−4 | 0 | 0 | 0 | 0.019 | 0.076 |
| Ottowia | 0 | 0 | 2.74 × 10−5 | 1.07 × 10−4 | 2.56 × 10−5 | 1.60 × 10−4 | 0.047 | 0.058 |
| Desulfobulbus | 5.51 × 10−5 | 0 | 2.51 × 10−4 | 0 | 0 | 0 | 0.028 | 0.056 |
| TM7 [G-2] | 0 | 0 | 2.20 × 10−4 | 0 | 0 | 0 | 0.133 | 0.133 |
| TM7 [G-3] | 1.04 × 10−2 | 2.38 × 10−3 | 1.90 × 10−2 | 2.18 × 10−2 | 1.36 × 10−2 | 3.79 × 10−2 | 0.023 | 0.053 |
| TM7 [G-5] | 3.58 × 10−4 | 1.77 × 10−4 | 1.13 × 10−3 | 1.26 × 10−4 | 0 | 3.05 × 10−4 | 0.019 | 0.061 |
| Fretibacterium | 4.14 × 10−4 | 1.97 × 10−4 | 1.65 × 10−3 | 5.02 × 10−5 | 1.79 × 10−5 | 1.81 × 10−4 | 0.004 | 0.032 |
| Family | ||||||||
| Atopobiaceae | 1.75 × 10−4 | 2.75 × 10−5 | 3.29 × 10−4 | 0 | 0 | 3.57 × 10−5 | 0.002 | 0.020 |
| Coriobacteriaceae | 2.46 × 10−4 | 2.75 × 10−5 | 6.58 × 10−4 | 3.02 × 10−5 | 1.79 × 10−5 | 5.12 × 10−5 | 0.047 | 0.052 |
| Bacteroidetes [F-1] | 8.77 × 10−4 | 1.61 × 10−4 | 2.55 × 10−3 | 1.07 × 10−4 | 0 | 2.77 × 10−4 | 0.034 | 0.049 |
| Bacteroidaceae | 7.09 × 10−4 | 1.38 × 10−4 | 1.21 × 10−3 | 9.14 × 10−5 | 0 | 1.83 × 10−4 | 0.019 | 0.063 |
| Lactobacillaceae | 6.56 × 10−5 | 0 | 2.51 × 10−4 | 0 | 0 | 0 | 0.034 | 0.043 |
| Mollicutes [F-1] | 1.61 × 10−5 | 0 | 1.10 × 10−4 | 0 | 0 | 0 | 0.101 | 0.101 |
| Mycoplasmataceae | 1.05 × 10−3 | 1.31 × 10−4 | 1.51 × 10−3 | 1.24 × 10−4 | 2.77 × 10−5 | 5.63 × 10−4 | 0.023 | 0.046 |
| Desulfobulbaceae | 5.51 × 10−5 | 0 | 2.51 × 10−4 | 0 | 0 | 0 | 0.028 | 0.047 |
| TM7 [F-2] | 3.58 × 10−4 | 1.77 × 10−4 | 1.13 × 10−3 | 1.26 × 10−4 | 0 | 3.05 × 10−4 | 0.019 | 0.048 |
| Synergistaceae | 4.14 × 10−4 | 1.97 × 10−4 | 1.65 × 10−3 | 5.02 × 10−5 | 1.79 × 10−5 | 1.81 × 10−4 | 0.004 | 0.020 |
| Order | ||||||||
| Coriobacteriales | 4.18 × 10−4 | 1.65 × 10−4 | 7.51 × 10−4 | 5.02 × 10−5 | 2.15 × 10−5 | 7.45 × 10−5 | 0.005 | 0.015 |
| Bacteroidetes [O-1] | 8.77 × 10−4 | 1.61 × 10−4 | 2.55 × 10−3 | 1.07 × 10−4 | 0 | 2.77 × 10−4 | 0.034 | 0.041 |
| Mollicutes [O-2] | 1.61 × 10−5 | 0 | 1.10 × 10−4 | 0 | 0 | 0 | 0.101 | 0.101 |
| Mycoplasmatales | 1.05 × 10−3 | 1.31 × 10−4 | 1.51 × 10−3 | 1.24 × 10−4 | 2.77 × 10−5 | 5.63 × 10−4 | 0.023 | 0.046 |
| Desulfobacterales | 5.51 × 10−5 | 0 | 2.51 × 10−4 | 0 | 0 | 0 | 0.028 | 0.042 |
| Synergistales | 4.14 × 10−4 | 1.97 × 10−4 | 2.23 × 10−3 | 5.02 × 10−5 | 1.79 × 10−5 | 1.81 × 10−4 | 0.002 | 0.012 |
| Class | ||||||||
| Coriobacteriia | 9.98 × 10−4 | 1.97 × 10−4 | 5.06 × 10−3 | 5.02 × 10−5 | 0 | 5.02 × 10−5 | 0.005 | 0.013 |
| Bacteroidetes [C-1] | 8.77 × 10−4 | 1.61 × 10−4 | 2.55 × 10−3 | 3.02 × 10−5 | 0 | 1.81 × 10−4 | 0.034 | 0.034 |
| Mollicutes | 1.17 × 10−3 | 1.65 × 10−4 | 1.51 × 10−3 | 4.96 × 10−5 | 0 | 1.74 × 10−4 | 0.016 | 0.020 |
| Deltaproteobacteria | 8.26 × 10−5 | 0 | 2.51 × 10−4 | 5.54 × 10−4 | 2.13 × 10−5 | 1.13 × 10−3 | 0.007 | 0.012 |
| Synergistia | 4.14 × 10−4 | 1.97 × 10−4 | 2.23 × 10−3 | 9.14 × 10−4 | 3.05 × 10−5 | 9.90 × 10−4 | 0.002 | 0.010 |
| Phylum | ||||||||
| Synergistetes | 4.14 × 10−4 | 1.97 × 10−4 | 2.23 × 10−3 | 5.02 × 10−5 | 1.79 × 10−5 | 1.81 × 10−4 | 0.002 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toyama, N.; Ekuni, D.; Matsui, D.; Koyama, T.; Nakatochi, M.; Momozawa, Y.; Kubo, M.; Morita, M. Comprehensive Analysis of Risk Factors for Periodontitis Focusing on the Saliva Microbiome and Polymorphism. Int. J. Environ. Res. Public Health 2021, 18, 6430. https://doi.org/10.3390/ijerph18126430
Toyama N, Ekuni D, Matsui D, Koyama T, Nakatochi M, Momozawa Y, Kubo M, Morita M. Comprehensive Analysis of Risk Factors for Periodontitis Focusing on the Saliva Microbiome and Polymorphism. International Journal of Environmental Research and Public Health. 2021; 18(12):6430. https://doi.org/10.3390/ijerph18126430
Chicago/Turabian StyleToyama, Naoki, Daisuke Ekuni, Daisuke Matsui, Teruhide Koyama, Masahiro Nakatochi, Yukihide Momozawa, Michiaki Kubo, and Manabu Morita. 2021. "Comprehensive Analysis of Risk Factors for Periodontitis Focusing on the Saliva Microbiome and Polymorphism" International Journal of Environmental Research and Public Health 18, no. 12: 6430. https://doi.org/10.3390/ijerph18126430
APA StyleToyama, N., Ekuni, D., Matsui, D., Koyama, T., Nakatochi, M., Momozawa, Y., Kubo, M., & Morita, M. (2021). Comprehensive Analysis of Risk Factors for Periodontitis Focusing on the Saliva Microbiome and Polymorphism. International Journal of Environmental Research and Public Health, 18(12), 6430. https://doi.org/10.3390/ijerph18126430